
Abstract
Building on eHealth literacy and mental health literacy, this cross-sectional survey study examined associations between eMental health literacy (the degree to which individuals obtain, process, and understand basic mental health information online to inform mental health-related decisions), perceived barriers to mental healthcare, and psychological distress. Data were collected online for 247 older adults in the United States. Higher eMental health literacy was associated with fewer perceived barriers to mental healthcare, in models conceptualizing psychological distress as an outcome of eMental health literacy and barriers to care (intrinsic, β = −0.36, p < .001; extrinsic, β = −0.24, p = .002) and as a covariate of eMental health literacy (intrinsic, β = −0.33, p = .001; extrinsic, β = −0.24, p = .003). Continued research and replication of findings are needed to better understand the potential role of eMental health literacy in reducing barriers to mental health services in later life.
• This study is the first to examine eMental health literacy in later life, which expands the field’s understanding of how online literacy is associated with barriers to mental health services for older adults. • During a cultural shift towards more online healthcare, eMental health literacy and psychological distress are crucial areas of focus for researchers and clinicians working to dismantle barriers to mental healthcare in later life.
• These findings inform future interventions aimed at improving access to mental healthcare in older adults and urge the field to view technology not as a limitation but rather as a tool that can reduce barriers to services in later life. • As the healthcare system transitions into a more digital world, older adults deserve special attention. Beyond considering mere access to technology, the degree of literacy older adults possess regarding obtaining and understanding mental health information online must be considered.What this paper adds
Applications of study findings
Introduction
By 2034, older adults (65+ years) will outnumber children for the first time in United States (U.S.) history (U.S. Census Bureau, 2018). This population shift will increase the proportion of older adults among those experiencing mental health concerns, resulting in increasingly more individuals in later life navigating the mental healthcare system (SAMSHA, 2019). During the COVID-19 pandemic, the mental healthcare system relied heavily on technology to provide therapeutic services (APA, 2021). However, research has not examined older adults’ literacy in accessing online information related to mental healthcare (i.e., their eMental health literacy), which is a new construct that builds upon prior eHealth literacy and mental health literacy constructs. The current study examined whether eMental health literacy was associated with older adults’ perceived barriers to mental health services and to their psychological distress.
Technology’s Role in Older Adults’ Mental Healthcare
A significant shift in telehealth utilization occurred during the COVID-19 pandemic. Among adults aged 50–80, those participating in any telehealth visit raised from 4% in 2019 to 30% in 2020; notably, 18% engaged in telehealth for mental healthcare (Buis, 2020). Fifty-percent of psychologists adopted a hybrid approach (mix of telehealth and in-person) in 2021 compared to 33% in 2020, and 93% planned to continue providing telehealth care (APA, 2021). To ensure that mental health services are accessible to older adults, more information is needed regarding how online literacy may factor into older adults’ perceived barriers to the mental healthcare system.
In addition to receiving mental healthcare online, individuals use online resources to assist with health and mental health decisions. Most (72%) internet users (18 + years) in the U.S. reported searching for health information online; however, fewer older adults (13%) researched a medical condition online than 18–29 year-olds (47%) and 30–49 year-olds (43%) (Fox & Duggan, 2013; Watkins & Xie, 2014). Unfortunately, investigations of online literacy in healthcare have focused on physical health (i.e., eHealth literacy). Given fundamental differences in how health concerns are viewed in our society relative to mental health concerns, especially in later life, understanding the unique aspects of accessing mental health information online is critical to supporting older adults’ mental health, maintaining quality of life, and promoting successful aging.
eMental Health Literacy and Psychological Distress
Prior research established the constructs of eHealth literacy (EHL) and mental health literacy (MHL). EHL was defined as “the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem” (Norman & Skinner, 2006, p. e9). MHL represents “knowledge and beliefs about mental disorders which aid their recognition, management or prevention” (Jorm et al., 1997, p. 182). Individuals with greater EHL were more likely to engage in physical exercise and have a balanced diet (Mitsutake et al., 2016). Similarly, higher MHL was associated with lower rates of depression, anxiety, and stress (Tambling et al., 2021). Low MHL can serve as a barrier to treatment, prolonging psychological distress (Coles & Coleman, 2010).
Building on the EHL and MHL constructs, we defined eMental health literacy as the degree to which individuals obtain, process, and understand basic mental health information online that informs mental health-related decisions such as when and how to seek services. Although older age has been associated with both lower EHL (Neter & Brainin, 2012; Tennant et al., 2015) and poorer MHL (Piper et al., 2018; Reavley et al., 2014; Wetherell et al., 2009), older adults’ literacy regarding mental health information online is unknown. Thus, based on research linking MHL with psychological distress, the current study hypothesized that higher eMental health literacy would be associated with lower psychological distress.
Barriers to Mental Healthcare
Mental health concerns in later life are associated with an increased risk of suicide, lower cognitive functioning, and decreased quality of life (Blazer, 2003; Sivertsen et al., 2015); however, older adults under-utilize mental health services (WHO, 2017). Delayed mental health treatment for older adults increases severity of symptoms, prolongs personal suffering, and decreases psychological health (Thompson et al., 2008). Understanding older adults’ perceptions of barriers to mental healthcare is important to improve delivery of services. Barriers to mental healthcare have been conceptualized as intrinsic or extrinsic (Pepin et al., 2015). Intrinsic barriers represent processes internal to an individual (e.g., help-seeking behaviors and stigma); extrinsic barriers represent processes external to an individual (e.g., cost and transportation).
Association of eMental Health Literacy with Barriers to Care
Higher EHL and MHL are associated with fewer intrinsic and extrinsic barriers to care. Higher EHL skills lessened barriers to adhering with COVID-19 quarantine restrictions given that this information was often shared online (Brørs et al., 2020). Furthermore, higher EHL facilitated patient-centered communication, which not only reduced barriers but also improved satisfaction, interactions with physicians, and self-management of healthcare needs (Mitsutake et al., 2016; Neter & Brainin, 2012; Rathert et al., 2013; Tennant et al., 2015; Xiang & Stanley, 2017). Low MHL delayed use of mental health services and treatments for older adults (Spiranovic et al., 2014), and higher MHL has been associated with less stigma towards mental illness and increased help-seeking behavior (Reavley et al., 2014). Thus, in the current study, we hypothesized that higher eMental health literacy would be related to fewer reported intrinsic and extrinsic barriers to mental healthcare.
Association of Barriers to Care with Psychological Distress
In addition to mental healthcare barriers noted for diverse samples (Britt et al., 2008; Thompson et al., 2008), older adults also experience unique barriers such as stigma, complex comorbidities, and the myth that depression is a normal part of aging (Pepin et al., 2015; Polacsek et al., 2019). Such barriers decrease older adults’ help-seeking behaviors, resulting in delayed care and prolonged distress (Polacsek et al., 2019). Thus, in the current study, we hypothesized that perceiving more intrinsic and extrinsic barriers would be related to higher psychological distress.
The Current Study
eMental health literacy skills may be more salient than ever due to the COVID-19 pandemic, particularly for older adults. Older adults’ internet use and the mental health issues faced by this population point to a clear need to examine their ability to obtain and understand mental health information online as a potential pathway to reduce barriers to mental healthcare and subsequently support their mental health. However, older adults’ literacy with online information related to mental healthcare has not been previously assessed. Building on EHL and MHL, the current study sought to fill this gap by examining the concept of eMental health literacy.
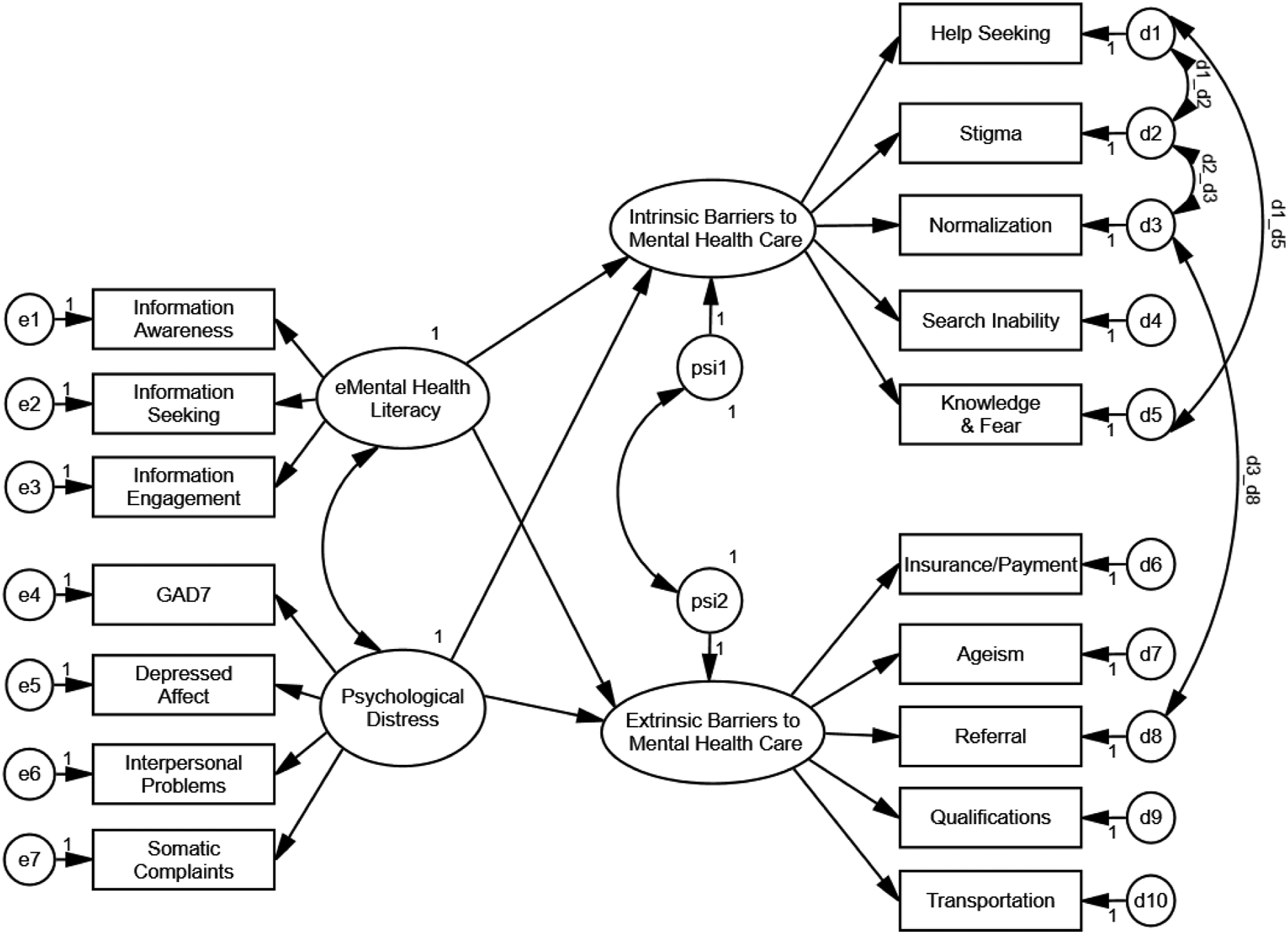
The current study tested two models of the association of eMental health literacy with intrinsic and extrinsic barriers to mental healthcare and psychological distress in older adults. Model 1 tested the following hypotheses: (1) higher eMental health literacy is associated with fewer perceived intrinsic and extrinsic barriers to seeking mental health services as well as lower psychological distress, and (2) fewer perceived intrinsic and extrinsic barriers is associated with lower psychological distress (Figure 1). Following best practices for structural equation models, an alternative model was also examined (Figure 2). Model 2 tested the following hypotheses: (1) higher eMental health literacy and less psychological distress are associated with fewer intrinsic and extrinsic barriers, and (2) psychological distress covaries with eMental health literacy, given that individuals experiencing psychological distress may have greater exposure to the mental healthcare system and more opportunities to experience barriers to accessing care and to seek information online about mental health. Hypothesized structural equation model assessing eMental health literacy as a predictor of barriers to care and psychological distress. Alternative structural equation model assessing eMental health literacy as a predictor of barriers to care, controlling for psychological distress as a covariate.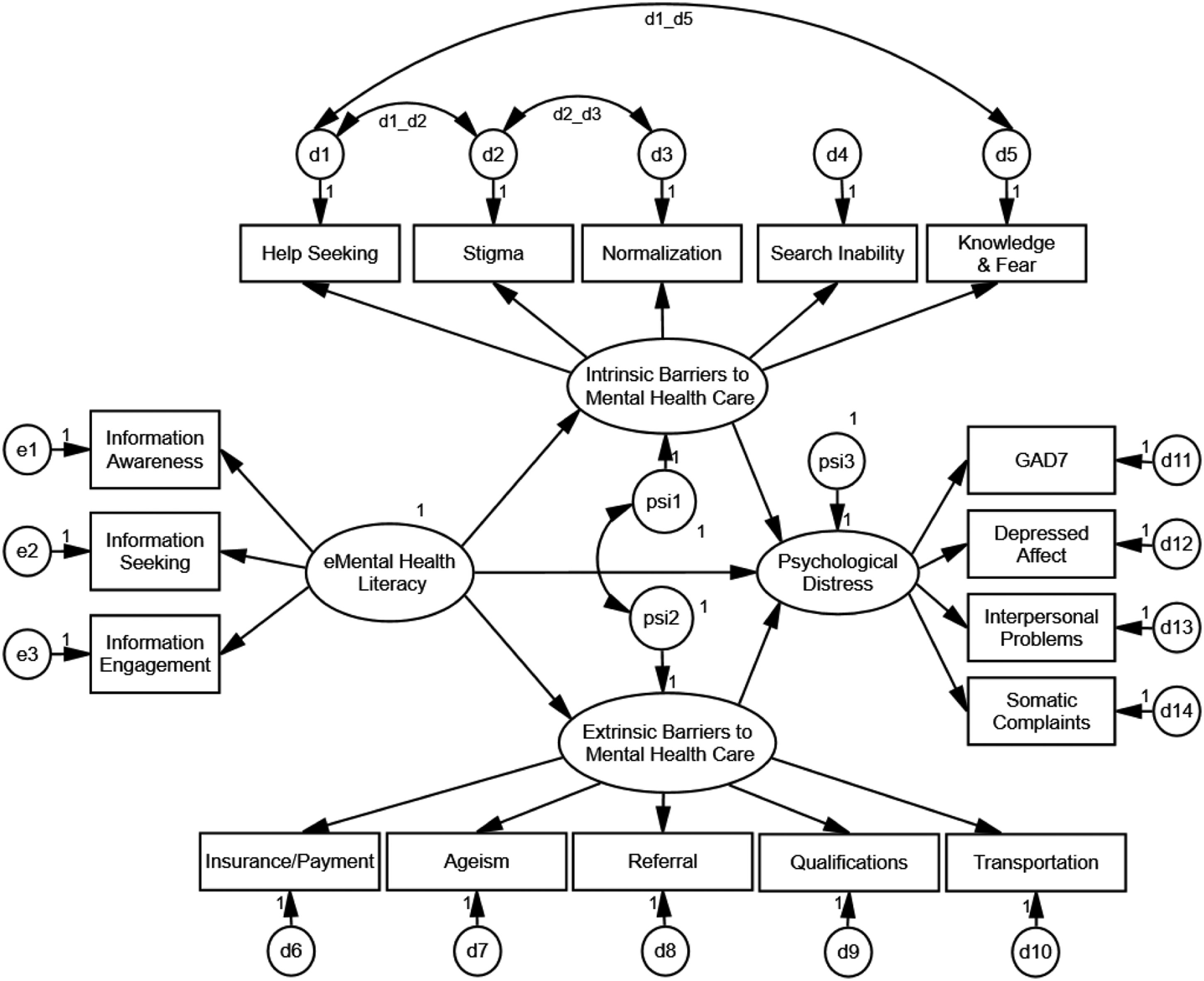
Method
Participants
Demographic Characteristics of Sample (N = 247).
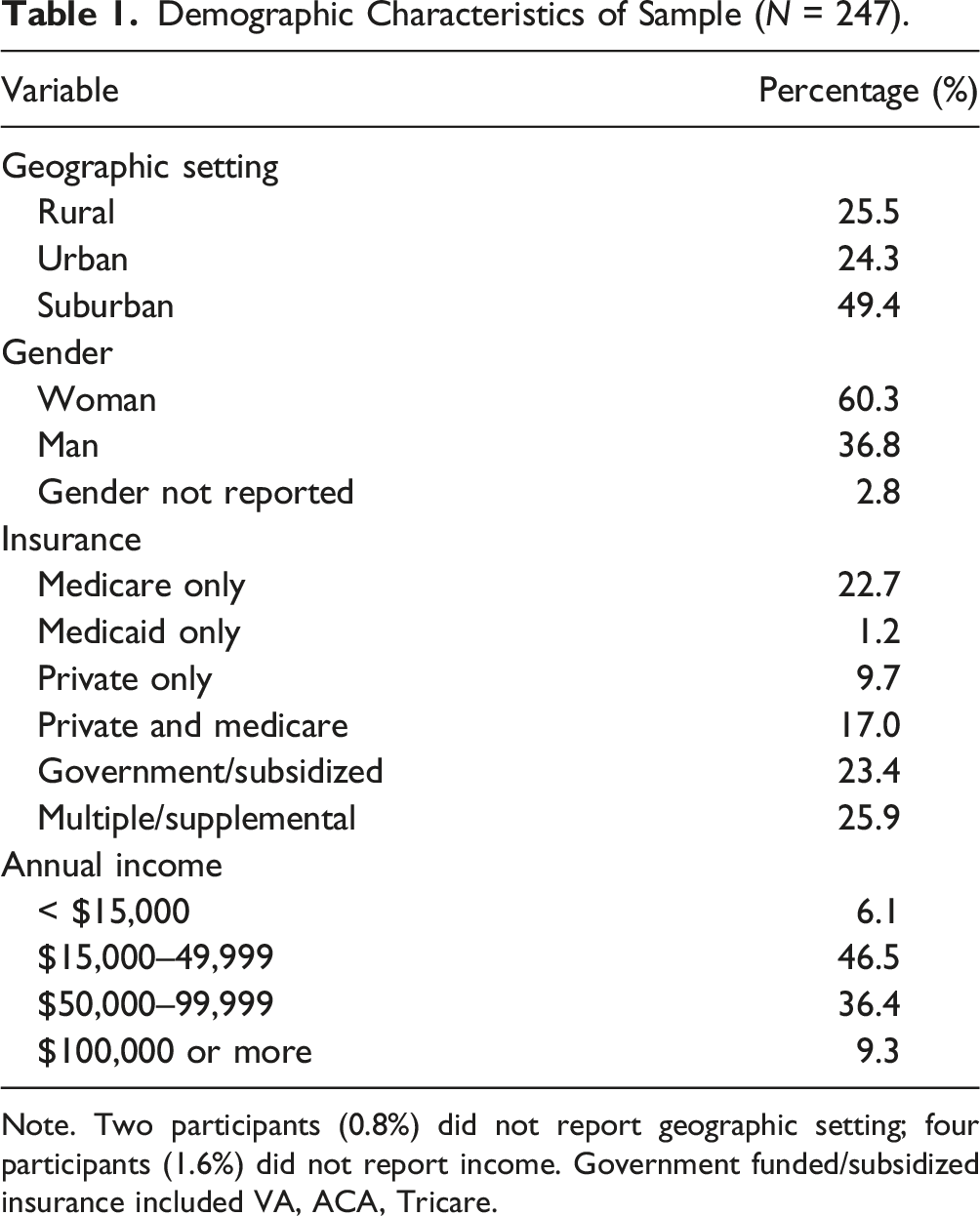
Note. Two participants (0.8%) did not report geographic setting; four participants (1.6%) did not report income. Government funded/subsidized insurance included VA, ACA, Tricare.
Measures
Demographic Questionnaire
Participants were asked questions regarding age, gender, sexual orientation, race/ethnicity, insurance coverage, internet access, and comfort with the internet.
eMental Health Literacy
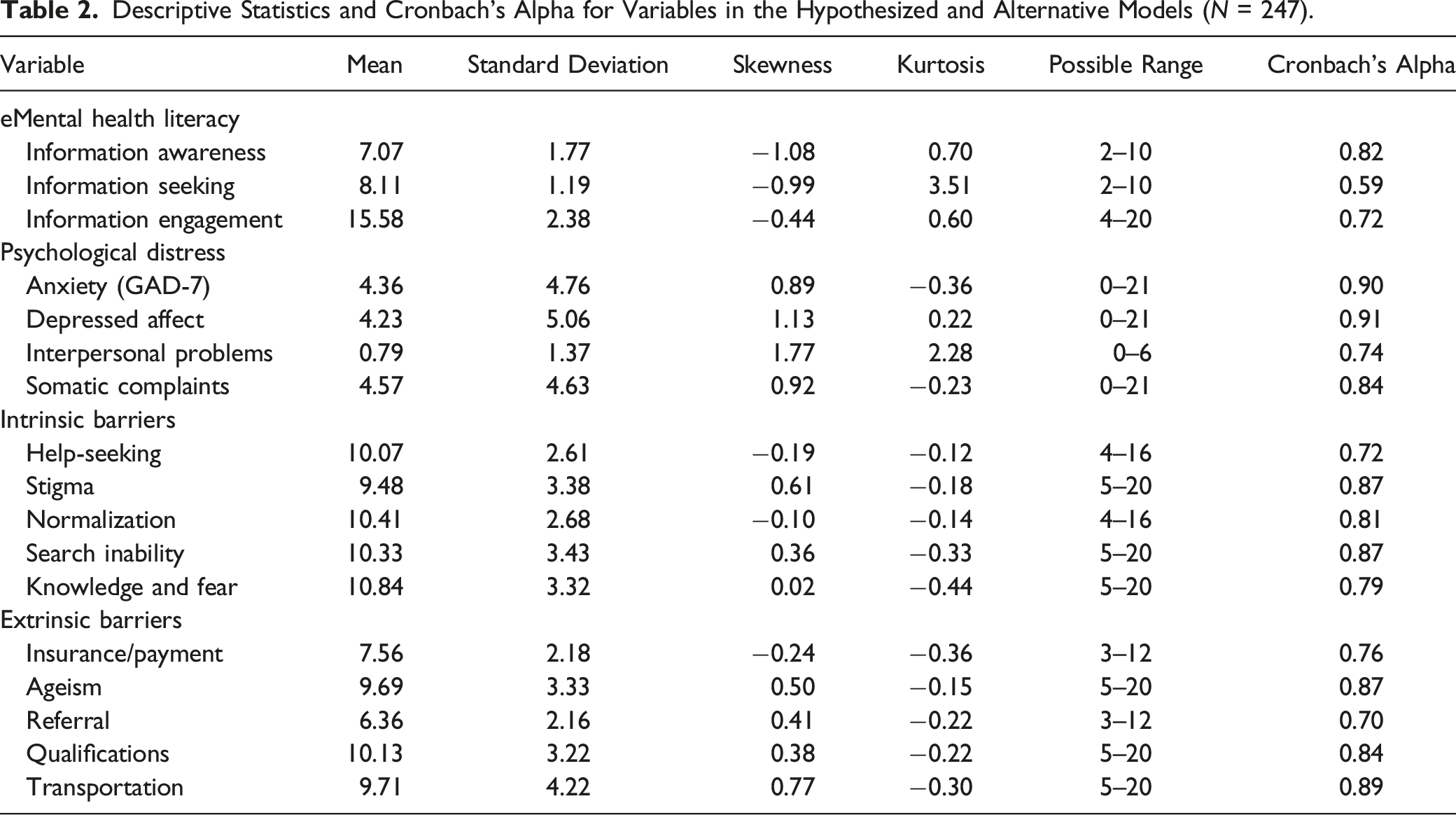
Descriptive Statistics and Cronbach’s Alpha for Variables in the Hypothesized and Alternative Models (N = 247).
Barriers to Mental Health Services
The Barriers to Mental Health Services Scale Revised (BMHSS-R) assessed perceived barriers to mental health services using 44 items rated from 1 (strongly disagree) to 4 (strongly agree). Intrinsic domain subscales included: help-seeking (4 items), stigma (5 items), belief that depression is normal (4 items), belief about inability to find a therapist (5 items), and knowledge and fear of psychotherapy (5 items). Extrinsic domain subscales included: insurance/payment concerns (3 items), ageism (5 items), physician referral (3 items), confidence in therapist’s qualifications (5 items), and transportation concerns (5 items). Items for each subscale were summed; higher scores indicated more perceived barriers. Pepin et al. (2015) found convergent validity for the BMHSS-R and good internal consistency for its 10 subscales (0.63–0.87), with eight of the ten values greater than .70 (Pepin et al., 2015). Cronbach’s alphas for BMHSS-R subscales were strong in our sample (see Table 2).
Psychological Distress
Center for Epidemiological Studies Depression Scale (CES-D)
The CES-D (Radloff, 1977) assessed depressive symptoms with 20 items with possible responses from 0 (rarely or none of the time/<1 day) to 3 (all of the time/5-7 days). Three of the four CES-D subscales were used: Depressed Affect (7 items), Interpersonal Problems (2 items), and Somatic Complaints (7 items). Items for each subscale were summed; higher scores indicated more depressive symptoms. Cronbach’s alphas were strong in our sample (see Table 2).
Generalized Anxiety Disorder 7 (GAD-7)
The GAD-7 (Spitzer et al., 2006) assessed generalized anxiety symptoms using the sum of seven items with possible responses from 0 (not at all) to 3 (nearly every day). Higher scores indicated more anxiety symptoms. Cronbach’s alpha in our sample was .90.
Attention-Check Items
Seven attention-check items (e.g., “If you’re reading this, please choose Undecided”) were interspersed throughout the online survey. Only participants who responded correctly to at least five attention-check items were retained for analysis.
Procedure
From mid-June to mid-July of 2020, a study advertisement was posted on the Amazon MTurk worker platform with a link to the online survey. Potential participants (n = 297) reviewed the written informed consent, and those who clicked “I agree to participate in this study” (n = 295) moved forward. Next, two questions screened for study inclusion criteria. Only individuals who were 65+ years old and residing in the US moved forward to the study measures (n = 269). At least five of seven attention-check items were answered correctly by 250 participants, of whom 247 had complete data on our 17 analysis variables. Participants were compensated $1. The Institutional Review Board at Lehigh University waived approval for this cross-sectional survey study. We aimed to recruit N ≥200 participants based on typical recommendations for structural equation models (Weston & Gore, 2006) and a power analysis indicating that N = 201 would produce power of .80 for our model (i.e., DF = 113; Hancock & French, 2013). Our sample of 247 had a power of ≥.90 to detect a well-fitting model (ε = 0.02; Hancock & French, 2013).
Data Analysis
Study hypotheses were tested via structural equation modeling (SEM). Table 2 lists the observed indicators used for each of the four latent variables. Following recommendations regarding SEM with N < 500 (Weston & Gore, 2006), a priori fit criteria for global model fit were ≥.90 for the Tucker-Lewis index (TLI) and the comparative fit index (CFI) and ≤.10 for the Root Mean Square Error of Approximation (RMSEA) and for the Standardized Root Mean Square Residual (SRMR). The chi-square test is also reported; however, good model fit was not contingent on obtaining a statistically non-significant value, given the well-known sensitivity of the chi-square test (Weston & Gore, 2006). Specific fit was assessed by examining the direction and statistical significance of the hypothesized paths in the model. Amos 28 software and maximum likelihood estimation were used (Arbuckle, 2022).
Results
Preliminary Analyses
Cronbach’s alphas and descriptive statistics for the observed indicators are given in Table 2. All indicators demonstrated univariate normality (Curran et al., 1996). The normalized Mardia’s coefficient was 17.76, indicating some multivariate non-normality (Bentler, 2006).
Structural Equation Modeling
Hypothesized Model
Standardized Parameter Estimates and Confidence Intervals for Weights of Observed Indicator Variables with their Corresponding Latent Variables in the Hypothesized and Alternative Models (N = 247).

***p ≤ .001.
Standardized Parameter Estimates and Confidence Intervals for Structural Paths in the Hypothesized and Alternative Models (N = 247).

aIn the alternative model, this parameter was operationalized as a correlation. In all other cases, the → symbol indicates a unidirectional path as depicted in Figures 1 and 2.
**p < .01; ***p < .001.
Alternative Model
The alternative model had adequate fit (χ2 (113) = 411.77, p < .001, TLI = 0.88, CFI = 0.90, RMSEA = 0.10, SRMR = 0.09). To improve model fit, three correlated measurement errors were added sequentially, reflecting shared method variance between help-seeking and stigma, between help-seeking and knowledge/fear, and between normalization and referral. Model fit significantly improved (Δχ2 (3) = 52.73, p < .001), and the modified alternative model achieved acceptable fit (χ2 (110) = 359.04, p < .001, TLI = 0.90, CFI = .92, RMSEA = 0.10, SRMR = 0.08). All indicators were significantly related to their latent construct (p ≤ .001). Standardized estimates and confidence intervals for these weights are provided in Table 3.
As hypothesized (see Table 4), greater eMental health literacy was associated with fewer intrinsic (β = −0.33, p = .001) and extrinsic (β = −0.25, p = .003) barriers to mental health services. Greater psychological distress were associated with more intrinsic (β = 0.48, p < .001) and extrinsic (β = 0.50, p = .001) barriers to mental healthcare services. Squared multiple correlations (R2) indicated the model explained 33.6% of the variance in extrinsic barriers to mental healthcare and 36.4% of intrinsic barriers to mental healthcare.
Discussion
This study introduced the construct of eMental health literacy and examined two potential models describing its associations with perceived barriers to mental healthcare and psychological distress for a sample of older adults. Our focus on the older adult population aimed to position eMental health literacy as a new tool with the potential to reduce barriers to mental healthcare. As hypothesized, higher eMental health literacy had a strong association with fewer reported intrinsic and extrinsic barriers to mental healthcare. Although our study was the first to examine eMental health literacy, this finding was consistent with prior literature examining the association of EHL and MHL to perceived barriers (Meltzer et al., 2003; Mitsutake et al., 2016; Neter & Brainin, 2012; Spiranovic et al., 2014; Tennant et al., 2015).
Similar to how greater health literacy and mental health literacy can reduce barriers to care, eMental health literacy may play an essential role in how older adults perceive and navigate mental healthcare in an online setting. eMental health literacy represents a potential opportunity for facilitating and improving older adults’ experiences with online mental health information and services. Given the aging population and changing landscape of healthcare towards a more digital system, in part due to the demands of COVID-19, better eMental health literacy skills are crucial to ensuring older adults’ access to mental healthcare and, thus, represent a potential point of intervention that warrants further exploration.
The hypothesis that greater eMental health literacy would be associated with less psychological distress was not supported in the current study. This finding contradicted previous literature indicating significant associations between EHL and health (Mitsutake et al., 2016) as well as between MHL and mental health (Tambling et al., 2021). High eMental health literacy may have developed as a result of experiencing prior or current symptoms of anxiety and depression, rendering the association non-significant in this sample. Additionally, psychological distress may have been elevated due to data collection occurring during the early months of the COVID-19 pandemic. Future research should consider assessing individuals’ engagement in mental healthcare treatment as another way to parse out the ways that eMental health literacy may relate to psychological well-being.
It is also important to contrast the findings for the association between barriers and psychological distress across the two models we tested. In the hypothesized model, the hypothesis that more perceived barriers would be associated with greater psychological distress was not supported. However, in the alternative model, when covaried with eMental Health literacy, greater psychological distress was significantly associated with more perceived intrinsic and extrinsic barriers to care. Thus, when older adults had similar levels of online literacy with mental health resources, their psychological well-being was more strongly associated with their perception of barriers to mental healthcare. Determining whether having experienced barriers to mental healthcare influenced the sample’s anxiety and depression symptoms was not possible in a cross-sectional study such as the present investigation. However, this finding implied that assessments of psychological distress may be useful for elucidating older adults’ perceptions of the accessibility of the mental healthcare system. Longitudinal data collection and inclusion of outcomes directly related to use of mental healthcare, such as coping strategies or emotional regulation, may help to flesh out our understanding of how perceived barriers relate to psychological well-being and eMental health literacy.
Finally, we noted that the hypothesized model explained a large percentage (i.e., 31.9%) of the variance in psychological distress despite finding non-significant individual associations with eMental health literacy, extrinsic barriers, and intrinsic barriers. Thus, as a whole, older adults’ literacy was associated with accessing mental health information online and how accessible the mental healthcare system was perceived are important to understanding interindividual variability in psychological distress. Similarly, in the alternative model, 33.6% of the variance in extrinsic barriers and 36.4% of variance in intrinsic barriers were explained (compared to 8.5% and 12.2% in the hypothesized model). These values provided evidence that psychological distress may be more important to consider as a covariate rather than an outcome when examining the association between eMental health literacy and barriers to care.
Limitations
Some limitations of the current study should be acknowledged. All participants were recruited from an online platform (MTurk) during the early months of a global pandemic. Our sample’s average eMental Health literacy subscale scores were relatively high (Awareness: 7.07 out of 10; Information Seeking: 8.11 out of 10; Information Engagement: 15.6 out of 20), and participants were likely more comfortable with the internet than the average older adult. Thus, generalizability to older adults with less technological experience is limited, and these relationships should be explored in older adults with broader ranges of eMental health literacy, including community-based samples. However, finding a significant association between eMental health literacy and fewer perceived barriers to mental health services, even in this sample with high average literacy, may suggest that an even stronger association could be found when samples with a wider range of eMental health literacy scores are examined. Another limitation was that most participants identified as White, non-Hispanic, cis-gender, and heterosexual, indicating that these results may not generalize to diverse older adult populations; further intersectional investigation of eMental health literacy is imperative to understanding barriers to care given disparities in the U.S. health and mental healthcare systems (Sorkin et al., 2016). Because our data were cross-sectional, the causal direction of the associations demonstrated in this could not be established. Finally, some multivariate non-normality was noted in the data; however, establishing univariate normality with continuous indicators mitigated its influence on standard errors and model fit indices (Finney & DiStefano, 2006).
Implications and Future Directions
With a shortage of trained mental health professionals specializing in geropsychology, the development of new programming and interventions aimed to ensure the well-being of the aging population is vital to prepare for the increasing number of older adults who will likely require mental healthcare (Flaherty & Bartels, 2019). The current study suggested that eMental health literacy may be a target area for intervention given its association with fewer barriers perceived by older adults. The skills included in eMental health literacy are simple, yet can be integral to meeting older adults’ mental health needs. Like EHL, eMental health literacy is conceived of as a skill that can evolve and change (Brørs et al., 2020). Therefore, future research could examine whether individual or community efforts to increase eMental health literacy would reduce barriers older adults experience in accessing mental healthcare, which could ultimately lead to more positive psychological outcomes. It may also be helpful to investigate how eMental health literacy relates to specific perceived barriers (e.g., stigma, cost) in addition to overall intrinsic and extrinsic barriers in future studies.
The extension of the concepts of EHL and MHL into an online environment via eMental health literacy adds a useful tool to support and facilitate older adults’ use of the internet for mental health information, especially as cohorts more familiar with the internet age into this group. A strength of our study is being the first to measure eMental health literacy. Future studies should further examine the psychometric properties of the eMHEALS, including its reliability, factorial invariance across diverse and community-based samples, and construct validity relative to MHL and EHL (Norman & Skinner, 2006; O’Connor & Casey, 2015).
The role of psychological distress in regard to eMental health literacy and barriers to care requires further exploration. Our finding that more psychological distress was significantly associated with older adults’ perceptions of more extrinsic and intrinsic barriers to mental healthcare may indicate that individuals endorsing more symptoms of anxiety and depression face additional barriers. In addition to increasing older adults’ online literacy for mental health research and decisions, how to remove their barriers to mental healthcare also may need to be addressed. eMental health literacy may also function differently across clinical populations (i.e., with individuals who meet clinical criteria for mental health diagnoses) and community samples. Given the non-significant association in this study between eMental health literacy and psychological distress, longitudinal research may be needed to better understand this association and its directionality. The current study lays a foundation to expand our understanding of eMental health literacy and its association with psychological distress and barriers to care.
Future directions should also include examining the role of eMental health literacy in diverse populations. Cultural context and minority status can influence individuals’ experiences with barriers to mental healthcare in the older adult population. For example, discomfort speaking to professionals and fear of someone finding out were barriers to mental health services reported by Hispanic participants and older adults of color, respectively, more than their non-Hispanic white counterparts (Sorkin et al., 2016). Due to systemic barriers and racial inequities that currently exist in the health and mental healthcare system, it is imperative to develop eMental health literacy as a culturally informed construct.
Considering recent events such as the COVID-19 global pandemic, services such as tele-psychotherapy have become the new normal; therefore, more information on the way older adults interact with information online regarding their mental health, or their eMental health literacy, is crucial. Mental health providers have begun to shift the way mental health services are provided, significantly increasing the availability of telehealth opportunities (APA, 2021). Greater availability of tele-psychotherapy may help further reduce barriers to mental healthcare due to flexibility regarding travel or transportation and reduction of stigma concern due to a lack of physical waiting-rooms (Rosen & Glassman, 2020). However, it is possible that older individuals with lower eMental health literacy may have additional barriers in finding information on tele-psychotherapy and appropriate providers online. As a strength-based concept, promoting eMental health literacy may help to empower older adults to adapt to the digital shift occurring in mental healthcare services and reduce barriers.
Despite the surge of mental healthcare professionals moving their services to an online environment, our understanding of the online social space is still limited, particularly for older adults. A recent study examining treatment engagement and conversion to telehealth during the COVID-19 pandemic found that older adults were less likely to receive services online (Miu et al., 2021). However, our study highlighted that online literacy may improve navigation through the current mental healthcare system. Therefore, it is imperative for researchers and clinicians to do a better job at facilitating and helping to develop skills that empower older adults to use technology to aid in supporting their mental health. We believe eMental health literacy is one possible solution.
The current study posited that greater literacy with online mental health information may facilitate older adults’ engagement with the mental healthcare system given its association with fewer perceived intrinsic and extrinsic barriers. Rather than viewing the transition towards a more digital healthcare system as a barrier for older adults, technology could be viewed as a tool for older adults to overcome existing barriers to accessing mental health services. Individual and systemic level attention should consider solutions fostering higher eMental health literacy skills in later life. In sum, the current study introduced eMental health literacy as an essential skill and demonstrated its association with the ease with which older adults navigate the mental healthcare system. Expanding our understanding of eMental health literacy is one avenue to increasing support older adults’ healthy aging.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Review Board at Lehigh University waived approval for this study (Protocol 1598322–1).