
Abstract
A greater number of studies have examined the impact of social engagement on cognitive function rather than the other way around, leaving their reciprocal association underexplored. Furthermore, formal and informal social engagement are not differentiated, although they may have independent relationships with cognitive function. This study aims to identify (1) whether informal and formal social engagements are effective in maintaining cognitive health and (2) if cognitive function has a bidirectional effect on social engagement. The study applies a dynamic panel data structural equation modeling with a maximum likelihood estimator (ML-SEM) to the Korean Longitudinal Study of Aging (KLoSA) data. The results confirm that frequent participation in organizational activities is more robustly associated with cognitive function than memberships or informal social contact. Concerning the bidirectional relationship, the cognitive function increases the degrees of informal and formal engagement. The study thus validates a reciprocal association between social engagement and cognitive function.
• The paper identifies a reciprocal association between social engagement and cognitive function in South Korea. • The article highlights the distinct role of formal associational activities in maintaining cognitive health.
• Study findings necessitate future studies that examine a reciprocal association between social engagement and cognitive function in other countries. • Study findings affirm the need to devise policies that encourage the active social engagement of older adults.What this paper adds
Applications of study findings
Introduction
Older adults tend to lose principal roles, such as worker, parent, or spouse, that have stimulated their cognitive function to resolve complex problems regularly. To compensate for this loss, they need interpersonal (informal) or organizational (formal) engagement that provides opportunities to use the cognitive function to meet challenges (Scott et al., 2020). Specifically, social support, a type of informal social engagement, is positively related to better cognitive abilities, while lacking it is associated with slower processing speed (Gow et al., 2013; Kelly et al., 2017). Relevant studies report that older adults’ informal engagement with persons around them effectively keeps cognitive function intact (Saito et al., 2018). Also, the formal engagement that denotes either membership in or activities through voluntary organizations preserves cognitive function (Yang et al., 2020).
Nonetheless, it is less clear whether both informal and formal social engagements protect cognitive function. Relevant studies mostly checked the effect of either informal or formal engagement on the cognitive function of older adults (Evans et al., 2019; Lee & Yeung, 2019). Further, many studies presume a unidirectional impact of social engagement on cognitive function without examining whether cognitive function facilitates social engagement. Also, these studies rarely account for past cognitive status and unmeasured time-invariant individual characteristics such as personality traits and genetic predisposition, which may predetermine the association between social engagement and cognitive function. This study applies a dynamic panel model with fixed effects (Allison et al., 2017) to the seven waves of data from the Korean Longitudinal Study of Aging (KLoSA) to rigorously examine a reciprocal relationship between informal/formal social engagements and cognitive function over time. It is crucial to understand the relationship between social engagement and cognitive function in the country because the prevalence of dementia increased almost thirty times between 2003 and 2015 (J.-W. Jang et al., 2021).
Social Engagement and Cognitive Function
The relationship between social engagement and cognitive function has attracted considerable research attention in the past two decades. Bassuk, Glass, and Berkman’s seminal work defines social engagement as “the maintenance of many social connections and a high level of participation in social activities” (1999, p. 165) and suggests three plausible reasons why social engagement is associated with cognitive function. First, social engagement invites older adults into complex interpersonal exchanges that demand the use of mental capacities (Pan & Chee, 2020). Second, social engagement brings older adults to a broader community where more opportunities to activate cognitive functions arise. These positive interpersonal and communal ramifications of an active lifestyle on cognitive function align with the cognitive reserve hypothesis (Beyer et al., 2021). In particular, Hultsch et al. (1999) find that increases and decreases in intellectually engaging activities were associated with changes in cognitive function over time. These engaging activities may offer chances for older adults to develop cognitive reserve, “the ability to optimize or maximize performance through differential recruitment of brain networks” (Stern, 2002: p. 451). Third, social engagement enables older adults to draw emotional support when needed, which may provide a buffer against experiencing cognitive decline. Specifically, emotional support may help reduce depressive symptoms, improve quality of life, and increase self-esteem, preventing cognitive deterioration (Leung et al., 2015).
Numerous studies have documented the cognitive benefits of social engagement; however, most do not differentiate between informal and formal engagements and their respective associations with cognitive function (e.g., Pugh et al., 2021). Presumably, informal engagement with personal contacts provides instrumental and emotional support. On the other hand, formal engagement with various groups renders an organized lifestyle stimulating cognitive reserve through regular participation in physical and mental activities.
Informal Engagement and Cognitive Function
Empirical studies generally support the effect of informal engagement on cognitive function. The relevant research primarily concentrates on the engagement with close and intimate ties such as a spouse, children, relatives, or friends. For example, Fratiglioni et al. (2000) find that the lack of intimate ties put Swedish older adults at a heightened risk of developing dementia. Another Swedish study reports that weekly contact with friends and acquaintances generated a lower chance of developing dementia (Sörman et al., 2015). Frequent contact with friends and relatives also produced a lower risk of dementia or cognitive decline for older adults in the United Kingdom (Hackett et al., 2019), Spain (Zunzunegui et al., 2003), and Japan (Saito et al., 2018). Specifically, Pugh et al. (2021) show that a higher level of interpersonal activity was related to higher degrees of global cognition, semantic memory, and word memory.
Formal Engagement and Cognitive Function
Likewise, formal engagement exhibits a positive relationship with cognitive function in the literature. For instance, Oh et al. (2021) report that a consistent engagement with religious, sports, alumni, political, and voluntary associations over time helped maintain the cognitive function of older Korean adults. Further, James et al. (2011) find that the interaction between such organized activities and the observation period of up to 12 years produced a reduced rate of global cognitive decline, suggesting a protective effect of formal engagement. Hughes et al. (2013) also observe that frequent engagement in and the slower reduction of organizational activities over time decreased the risk of cognitive impairment. By contrast, Saczynski et al. (2006) report that Japanese American men recorded a higher risk of dementia if their level of organizational activities declined from mid to late life.
The Reciprocal Effect of Cognitive Function on Social Engagement
It is crucial to examine the bidirectional effect of cognitive health on informal and formal engagements apart from the well-documented impact of social engagement on cognitive function. The cognitive health selection mechanism may predispose a minority of older adults to become active social engagers. If this is the case, we would be left with an incorrect conclusion that overemphasizes the effect of social engagement even when no such impact exists. For example, Liao et al. (2018) use the White Hall II study sample of about 7000 London civil servants who were 56 years old on average at the baseline year of 1997 to track the reciprocal associations between social support and cognitive function over the next 10 years. They find that cognitive function in the past affected the degree of social support but not vice versa, supporting the health selection mechanism.
However, few studies scrutinize the bidirectional association between social engagement and cognitive function. Dyer et al. (2020) observe that a greater dementia severity at baseline was associated with a poorer social network over time. However, James et al. (2011) report that global cognition was not longitudinally related to changes in social activities. Empirical evidence regarding the effect of cognitive function on social engagement is thus inconclusive. This study aims to fill this gap in the literature by (1) using a suitable method to examine the reciprocal relationship and (2) providing a distinct comparison between informal and formal social engagements in their associations with cognitive function.
We propose two hypotheses that suggest a reciprocal relationship between social engagement and cognitive function.
Methods
Data
We used the KLoSA data set. The initial survey was administered in 2006 and gathered information regarding socioeconomic conditions, health and well-being, and family and social lives from a nationally representative sample of 10,254 adults aged 45 years and above. It employed a face-to-face Computer Assisted Personal Interviewing (CAPI) that facilitates logic checks and validations of answers during the interview and reduces errors in data entry (S.-N. Jang et al., 2009). The baseline survey recorded a response rate of 75.4% based on a multistage stratified probability sampling. The KLoSA continued the biannual survey, reaching its seventh wave in 2018 with an overall sample retention rate of 78%. For further details on the data such as the research design, sampling, and specific protocols, refer to the study website (https://survey.keis.or.kr/eng/klosa/klosa01.jsp).
The analytic sample excluded (1) 3296 respondents aged less than 55 at Wave 1, (2) 2099 respondents who passed away in the 12-year observation period, and (3) 128 respondents who reported a formal diagnosis of dementia by the time of the final wave. The latter was done because the outcome measure, a Korean version of the Mini-Mental State Examination (K-MMSE), is not a formal diagnostic instrument to confirm dementia cases (Kang et al., 1997). Those excluded from the analytic sample were likely to be unmarried, less religious, more educated, and have a higher household income than others. Regarding health-related indicators, the excluded were more likely to smoke and drink, suffer from functional limitations and depressive symptoms, and exercise irregularly. The sample also does not include 920 respondents replenished at Wave 5. Figure 1 shows the sample composition over time, detailing the total eligible cases, number of nonresponses, and deaths at each wave. Sample composition.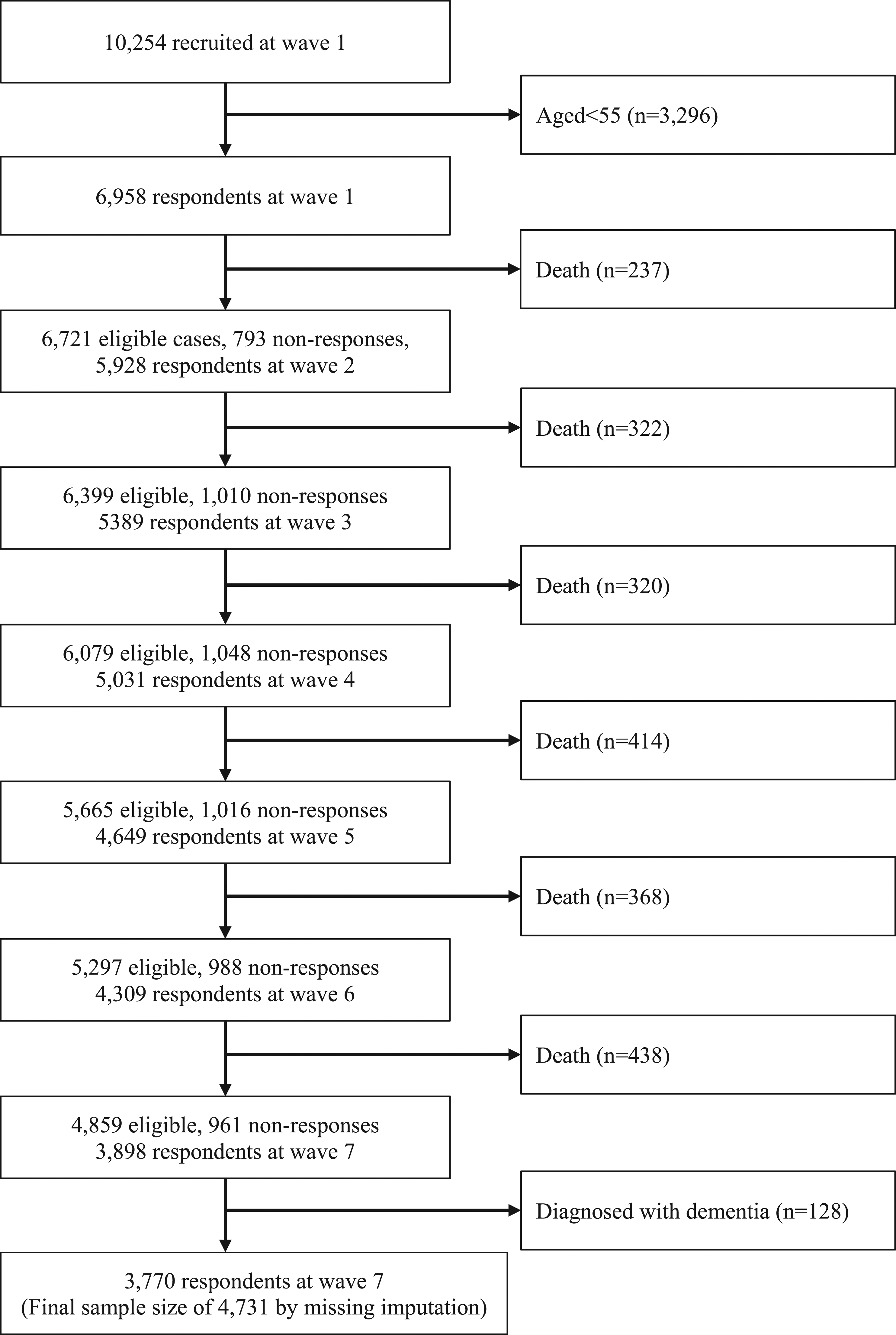
The study employed the Full Information Maximum Likelihood (FIML) estimator to account for missing data and item nonresponses. The imputed sample comprises 4731 respondents without a formal dementia diagnosis.
Measures
Social Engagement
Although incomplete, the KLoSA offers informal and formal social engagement measures that have been used in many studies (e.g., Min et al., 2016; Oh et al., 2021). A variable of contact frequency indicates informal engagement.
Frequency of contact with familiar persons measures how often a respondent met friends, relatives, or neighbors. It ranges from 1 = almost never to 10 = almost every day. Next, formal engagement is measured by two indicators.
Number of association memberships sums the memberships a respondent held in (1) a religious group, (2) older adults’ club or rotating-credit association among friends and neighbors, (3) a leisure/culture/sports group, (4) alumni association, hometown alliance, clan gathering, (5) a volunteer group, (6) political party, NGO, interest group, or (7) other organization. It may range between 0 and 7.
Frequency of organizational activities measures how frequently a respondent engaged in each of the seven associational activities. It ranges from “1. Almost never” to “10. Almost every day.” The maximal frequency of activity among the seven types of associations was assigned to a respondent.
Cognitive Function
Cognitive function is assessed by 19 items from a Korean version of the Mini-Mental State Examination (K-MMSE). It is a translated and modified version of the original MMSE that evaluates various cognitive health domains such as orientation to time and place, short-term and long-term memory, arithmetic ability, language, and visual construction (Han et al., 2008). The study uses a summated scale that ranges from 0 to 30. The higher the score, the better the cognitive function.
Time-Varying Controls
This study considers confounders that are known to be associated with social engagement or cognitive function (Sörman et al., 2015). Among them, the time-varying covariates are as follows:
Functional limitation is evaluated by the number of difficulties in instrumental activities of daily living (IADL) (Graf, 2008; Lawton & Brody, 1969). The ten-item scale probes whether a respondent experienced difficulty performing various activities such as grooming, cleaning, preparing meals, shopping, managing finance, or making phone calls (Cronbach’s α = .89 at Wave 1).
Depression is measured by a ten-item short form of the Center for Epidemiologic Studies Depression Scale (CES-D 10) (Kohout et al., 1993). It identifies whether a respondent experienced depression in the past week: for example, “I felt depressed,” “I felt that everything I did was an effort,” or “My sleep was restless.” Each has four response categories ranging from “0. Rarely or none of the time (less than 1 day)” to “3. Most or all of the time (5 to 7 days)” (Cronbach’s α = .81 at Wave 1). The summated scale ranges from 0 to 30. The higher the score, the greater the number of depressive symptoms.
In addition, health behaviors, marital status, income, working status, and place of residence are considered.
Smoking is a dichotomous variable where 1 = current smoker, 0 = nonsmoker.
Drinking is a dichotomous variable where 1 = current drinker, 0 = non-drinker.
Exercise is a dichotomous variable where 1 = regular exercise (more than once a week), 0 = no regular exercise.
Married is a dichotomous variable where 1 = married, 0 = unmarried.
Household income denotes logged total household income.
Working is a dichotomous variable where 1 = currently working, 0 = not working.
Urban is a dichotomous variable where 1 = urban residence, 0 = rural residence.
Time-Invariant Controls
Time-invariant controls are considered because the analytic method (ML-SEM) allows them to be estimated along with time-varying covariates (Williams et al., 2018).
Age ranges between 55 and 90 at the baseline survey. It is treated as time-invariant because all the respondents experience the same extent of increase in age over time, producing no variation in terms of within-person changes across individuals.
Sex is a dichotomous variable where 1 = woman, 0 = man.
Education indicates the highest level of education a respondent completed: 1 = less than primary school, 2 = middle school, 3 = high school, and 4 = university or above.
Religious affiliation has four dummy variables, Protestant (1 = Protestant, 0 = non-Protestant), Catholic (1 = Catholic, 0 = non-Catholic), Buddhist (1 = Buddhist, 0 = non-Buddhist), and other (1 = other religion, 0 = nonother religion). The reference category is comprised of respondents of no religion.
Analysis
The study employs a dynamic panel model with fixed effects fitted using structural equation modeling (Allison et al., 2017). Because it uses Moral-Benito’s (2013) maximum likelihood estimator, it is called ML-SEM. A merit of the ML-SEM is its unbiased estimates of cross-lagged time-varying predictors on an outcome measure controlling for the lagged effect of the outcome on itself. Cross-lagged means the causal impact of a past independent variable on the future realization of an outcome variable (see Figure 2). The lagged effect of an outcome variable is called autoregression, where a current state depends on its past state. These features distinguish dynamic models from static or cross-sectional models. Cross-lagged reciprocal relationship between social engagement (“soceng”) and cognitive function (“mmse”), taking both lagged and proximal effects into account.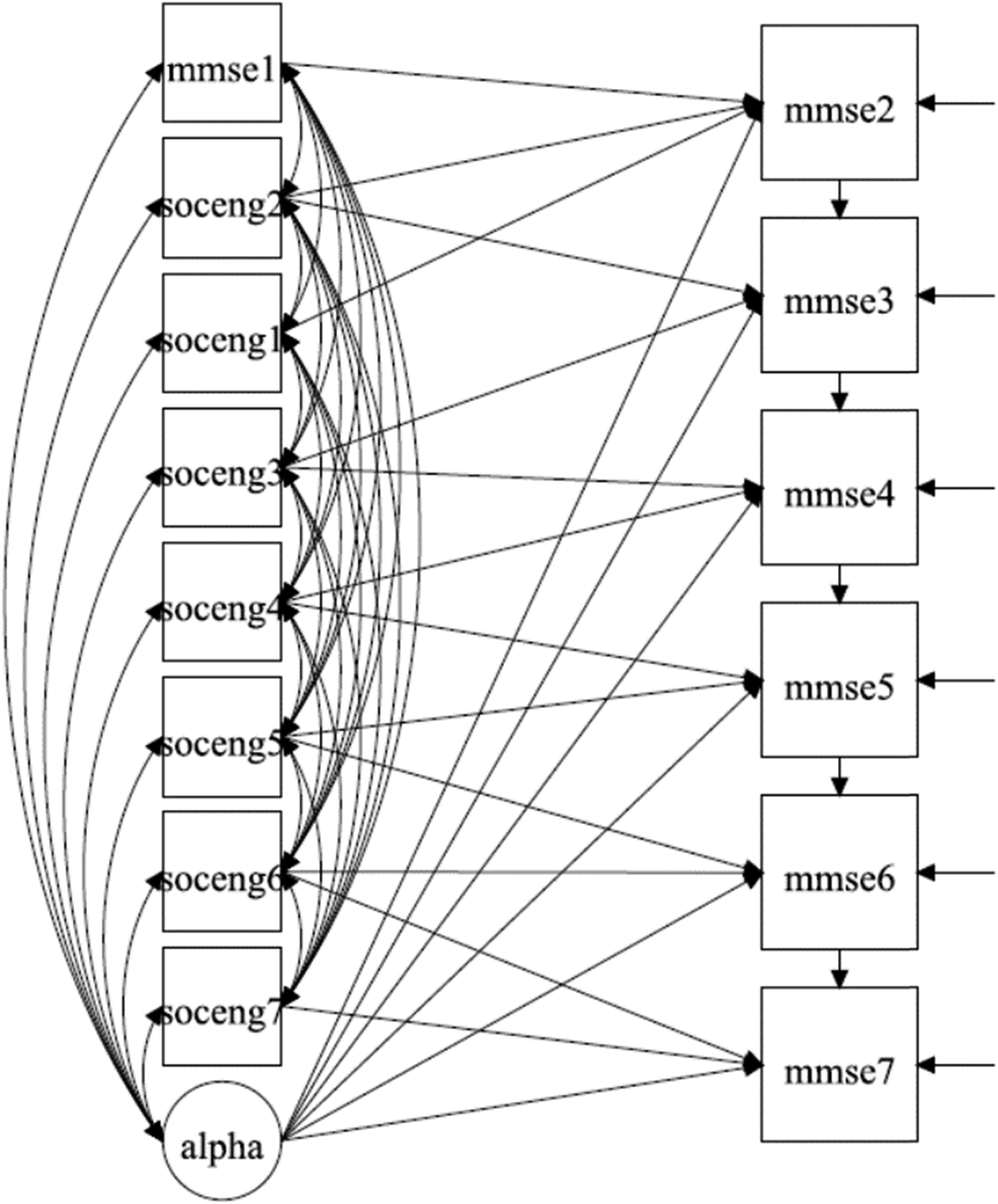
Further, ML-SEM differs from traditional cross-lagged SEMs because it accounts for unmeasured time-invariant individual traits by a latent construct that absorbs unmeasured unit-specific fixed effects. In short, ML-SEM uses within-individual variation over time to estimate the relationship between time-varying predictors and an outcome, accounting for all stable individual characteristics (Allison, 2009).
The ML-SEM models are specified as follows:


The two equations stipulate the cross-lagged relationship between x (social engagement) and y (cognitive function). Specifically,
Figure 2 displays how social engagement (“soceng”) predicts cognitive function (“mmse”), considering both the proximal and cross-lagged effects of engagement and the autoregressive effects of cognitive function. “Alpha,” the unit-specific fixed effects, predicts “mmse2-mmse7” after considering its correlations with “soceng1-soceng7” (the exogenous variable across waves) and “mmse1” (the endogenous variable at baseline).
Additionally, the time-varying predictor (e.g., “soceng”) is predetermined and thus sequentially exogenous to the outcome; the current degree of engagement may be affected by the past cognitive function level. Robust standard errors are applied to adjust for the non-normality of outcome variables. It is executed by the MLR (maximum likelihood parameter estimates with robust standard errors) estimator in Mplus (Lai, 2018). A Supplementary File presents the relevant Stata and Mplus scripts.
Results
Variables in the Analyses.
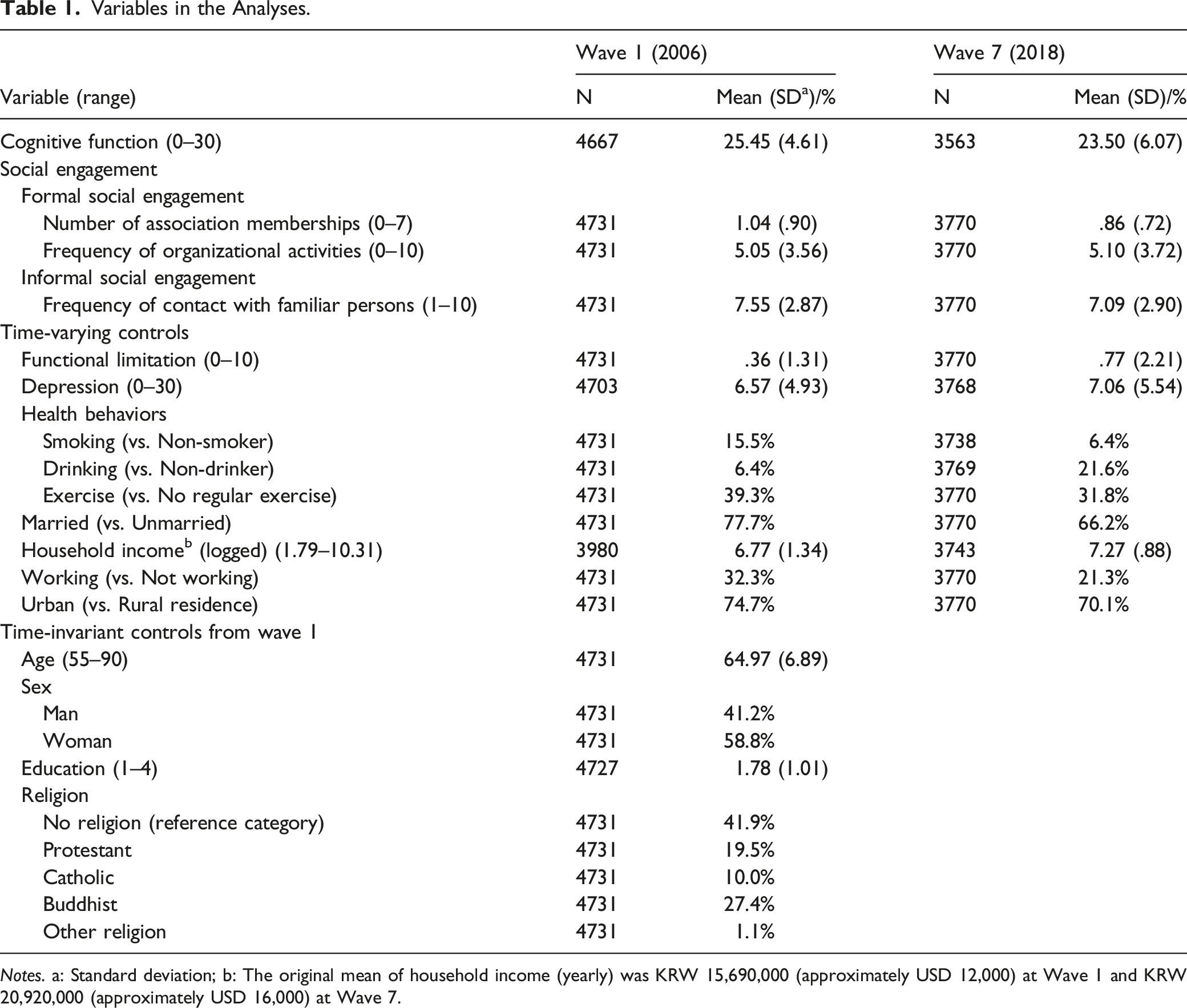
Notes. a: Standard deviation; b: The original mean of household income (yearly) was KRW 15,690,000 (approximately USD 12,000) at Wave 1 and KRW 20,920,000 (approximately USD 16,000) at Wave 7.
Concerning time-varying controls, both physical and mental health deteriorated somewhat. The number of functional limitations (IADL) increased from .4 to .8, while the number of depressive symptoms grew from 6.6 to 7.1. Regarding health behaviors, smokers in the sample decreased from 16% to 6%, whereas drinkers increased from 6% to 22%. Those who regularly exercised decreased from 39% to 32%. The married diminished from 78% to 66%. Household income increased over time, although working older adults shrank from 32% to 21%. The percentage of urban residents decreased slightly from 75% to 70%.
Regarding time-invariant controls, the average respondent was 65 years old at the baseline. Fifty-nine percent of the sample were women. The average respondent completed middle school. The largest religious category was Buddhists (27%), followed by Protestants and Catholics, while 42% had no religion.
The Reciprocal Relationship Between Social Engagement and Cognitive Function
ML-SEM of Cognitive Function on Social Engagement (N = 4731).

Notes. Standardized coefficient reported; FIML (Full Information Maximum Likelihood) estimator applied; CFI = Comparative Fit Index, TLI = Tucker-Lewis Index, RMSEA = Root Mean Square Error of Approximation, SRMR = Standardized Root Mean Squared Residual; *p < .05; **p < .01; ***p < .001 (two-tailed).
As to time-varying controls, none of them was related to cognitive function. Among time-invariant controls, being younger, educated, and man was associated with better cognitive function. Those with any religious affiliation recorded a higher MMSE than the nonreligious. The model fit is satisfactory, with the CFI (Comparative Fit Index) and TLI close to 1, while the RMSEA (Root Mean Square Error of Approximation) and SRMR (Standardized Root Mean Squared Residual) are close to 0. The ML-SEMs explained about 58% of the outcome measure.
ML-SEM of Social Engagement on Cognitive Function (N = 4731).

Notes. Standardized coefficient reported; FIML (Full Information Maximum Likelihood) estimator applied; CFI = Comparative Fit Index, TLI = Tucker-Lewis Index, RMSEA = Root Mean Square Error of Approximation, SRMR = Standardized Root Mean Squared Residual; *p < .05; **p < .01; ***p < .001 (two-tailed).
Among the time-varying controls, marital status predicted less-frequent organizational activities and informal contact over time, which may denote that an active lifestyle becomes a viable option for nonmarried older adults to make up for their lack of a marital tie. Living in urban areas reduced contact with familiar persons. According to the time-invariant controls, younger respondents with a higher level of education held a greater number of group memberships, while educated women engaged in organizational activities more frequently. By contrast, it was less-educated women who frequently engaged with familiar persons. Being a Protestant was related to formal and informal engagements, while being a Catholic was related to formal engagement alone. However, Buddhism was related to less-frequent organizational activities.
The model fit is satisfactory. The ML-SEMs explained about 23–34% of social engagement variation.
ML-SEM Between Types of Associations and Cognitive Function (N = 4731).
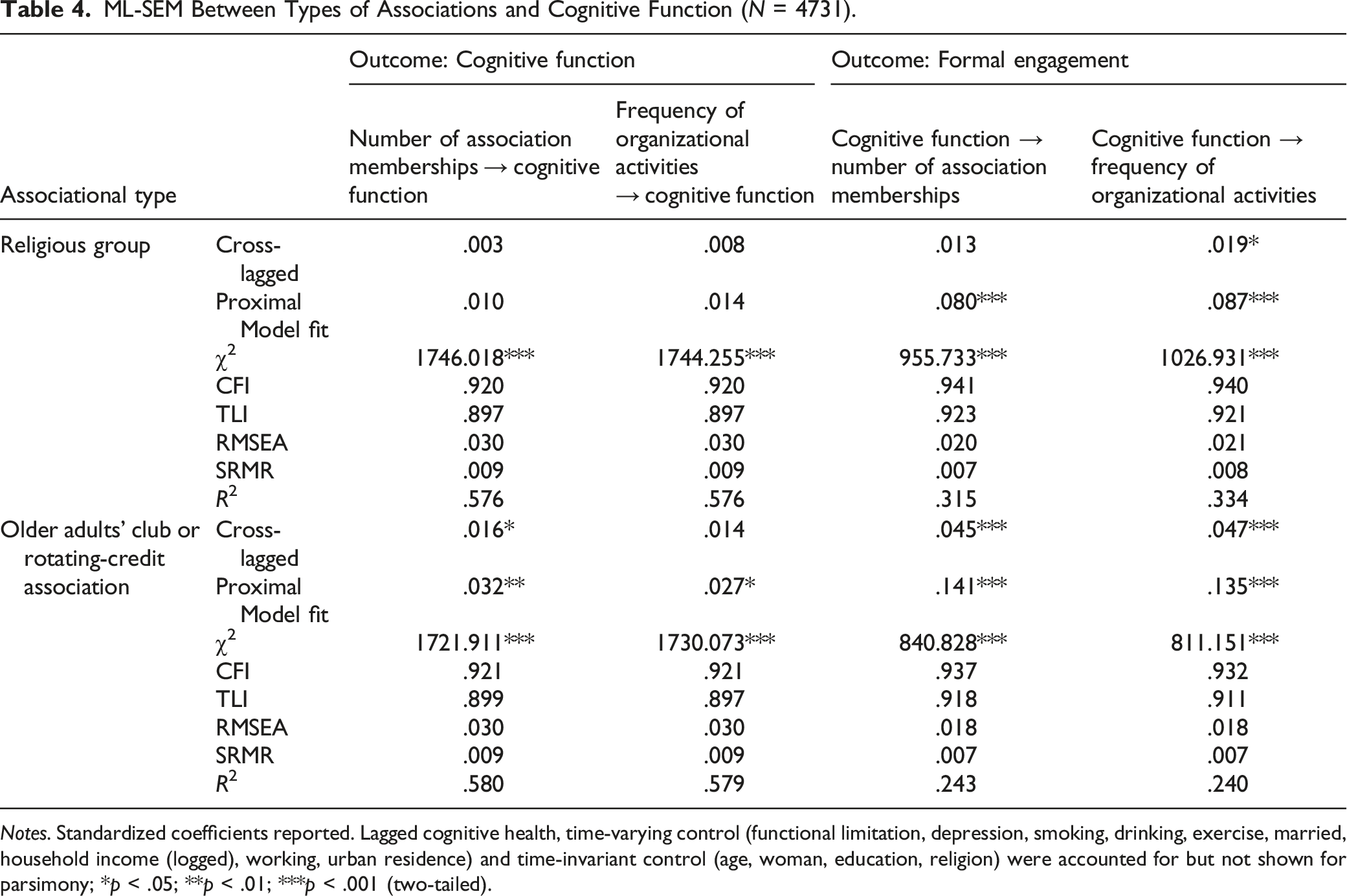
Notes. Standardized coefficients reported. Lagged cognitive health, time-varying control (functional limitation, depression, smoking, drinking, exercise, married, household income (logged), working, urban residence) and time-invariant control (age, woman, education, religion) were accounted for but not shown for parsimony; *p < .05; **p < .01; ***p < .001 (two-tailed).
Both cross-lagged and proximal reciprocities were established between the membership in older adults’ clubs or rotating-credit associations and cognitive function. Regarding religious associations, cognitive function was associated with a greater frequency of group activities.
Discussion
Although numerous studies concur that social engagement helps protect cognitive function, it is yet unclear (1) whether informal and formal engagements are protective against cognitive decline and (2) if cognitive function also exercises a bidirectional effect on sociality. For a rigorous empirical examination, the study applied the ML-SEM to a seven-wave panel data set of older Korean adults.
Regarding the effect of social engagement on cognitive function, the fixed-effect estimates confirmed that regularly conducting organizational activities mattered more than merely holding a membership. Additionally, informal engagement—frequent contact with familiar persons—had a proximal effect on cognitive function when the formal engagement was considered concurrently. In sum, regular organizational activities were more robust in protecting cognitive function.
Then what makes the effect of organizational activities significant in their association with cognitive function? Independent of the direct impact of organizational activities that stimulate cognitive function, these activities may offer chances to mingle with distant social ties. Active engagement at the organizational level may reflect an unmeasured social bridging effect of expansive and diverse informal ties on cognitive reserve. For instance, Perry et al. (2021, p. 7) maintain that “contact with a larger and more diverse group of peripheral others” increases cognitive reserve that may protect global cognitive function, episodic memory, and executive function. Frequent organizational activities may afford a way to socialize with such peripheral ties. Therefore it is likely that organizational activities increase cognitive function by enabling older adults to associate with diverse persons, which suggests a logical linkage between formal and informal engagement.
Further, we checked if each type of membership/activity was related to cognitive function (Table 4). In this regard, Fancourt et al. (2020) identify that in the U.K. regular community cultural engagement (e.g., visiting museums, art galleries, or theaters) reduced the risk of dementia over time. We found that older adults’ clubs or rotating-credit associations in Korea formed a significant reciprocal association with cognitive function. Specifically, it is not only that more than half of the sampled respondents belonged to this associational type but also that they participated in the activities about three or four times a year on average, indicating its local embeddedness (Supplementary Appendix Table 1). Coleman (1988, p. S102) clarifies that in Asia the rotating-credit associations are a “case that illustrates the value of the trustworthiness of the environment … These associations are groups of friends and neighbors who typically meet monthly, each person contributing to a central fund that is then given to one of the members … until … each of the n persons has made n contributions and received one payout.” This particular associational activity provides regular experiences that encourage older adults to activate their cognitive function.
Concerning the bidirectional relationship, cognitive function increased the degree of both formal and informal engagements over time. In conclusion, ML-SEMs supported the social causation and health selection mechanisms. It should be duly noted that the impact of cognitive function on social engagement seems more considerable than the other way around, according to their respective standardized coefficients in Tables 2–4. Nonetheless, we should aim to increase social engagement to protect cognitive health because relevant policies cannot tackle cognitive health problems directly.
This study has several limitations. First, we employed only a single indicator of informal engagement. In particular, due to the lack of data, we could not consider other crucial aspects of informal engagement such as the size of networks, intimacy with network members, or social support. Despite the weak measurement, the study confirms that the proximal effect of informal social ties was strong even when the formal engagement was concurrently considered. Second, the study used the maximal frequency of organizational activities to measure formal engagement. This is because those who engaged in multiple organizational activities tended to get a lower average score than others who frequently participated in only one type of activity. We thus employed the mean frequency of organizational activities in a Supplementary Analysis. We found that the ML-SEM estimates did not differ from the results when the maximal frequency was used (a table available upon request). Third, the study dropped respondents who died during the observation period and those who received a formal diagnosis of dementia by the final wave. The inevitable omission of these respondents from the analyses may have influenced the ML-SEM estimates.
Conclusion
This study identifies a reciprocal association between formal social engagement and cognitive function over time, using a longitudinal data set of older Korean adults. In sum, frequent engagement at the organizational level protects older adults’ cognitive function. In particular, older adults’ involvement in a type of association more culturally embedded in the local sociocultural context matters significantly in maintaining cognitive health.
This study suggests that it is critical to develop policies ensuring that older adults engage in organizational activities that activate their cognitive function. Future studies may explore whether such a reciprocal association applies to other countries. When examining the reciprocal association, more specific dimensions of informal and formal engagements should be considered. Further, empirical verification regarding if various types of organizations form a bidirectional relationship with cognitive function across countries would enrich policy implications tailored to promoting the cognitive health of older adults.
Supplemental Material
Supplemental Material - The Reciprocal Relationship Between Social Engagement and Cognitive Function Among Older Adults in South Korea
Supplemental Material for The Reciprocal Relationship Between Social Engagement and Cognitive Function Among Older Adults in South Korea by Joonmo Son and Pildoo Sung in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.