
Abstract
Cognitive stimulation is essential for successful aging. The influence of sex and socio-occupational elements on this area remains unknown. This study aimed to analyze the possible mediation of those elements in the effectiveness of a cognitive stimulation program in primary care. A randomized clinical trial was conducted with 232 adults aged 65 years or older without cognitive impairment. The intervention produced significant cognitive improvements. Women improved independently of social and occupational factors, while men’s improvement occurred at a low role level (zero to one), a medium level of interests (two to three), with a medium level of mental occupation (neither high nor low), and with marked personal values. The mediating variables were the intervention group in both sexes and, also in men, a low and medium role level. Therefore, the intervention and roles appear as mediating variables moderated by sex. In conclusion, cognitive stimulation programs should be adapted.
• The cognitive effect achieved after the application of a cognitive stimulation program is different according to sex. • Women’s cognitive abilities improve regardless of their roles, interests, values, or mental occupation. • Men’s improvement is marked by roles, interests, values, and mental occupation.
• It is necessary to contemplate occupational elements by sex to adapt cognitive stimulation programs for older adults. • The activities designed must be meaningful and add value and purpose, particularly for the male participants. • Equality in educational and social tasks must be guaranteed, particularly for female participants.What this paper adds
Applications of study findings
Increased life expectancy brings with it the challenge of promoting healthy, meaningful, and participatory aging in the community (Freak-Poli et al., 2021). Social isolation and reduced participation in social roles could indicate a prodromal stage of dementia (Joyce et al., 2022; Kuiper et al., 2015, 2016). The risk of cognitive decline is lower in individuals with greater participation in leisure activities during adulthood and greater prior occupational complexity due to the improved cognitive reserve produced (Gatz et al., 2006; Tan et al., 2019).
According to Gary Kielhofner’s (2007) model of human occupation (MOHO), social participation is based on the choice of meaningful activities (interests) that, according to the value system, allow adequate cognitive and social performance through role development. Interests are those activities which one enjoys or finds satisfaction in performing. Values are the coherent set of convictions that imply a commitment and oblige one to act in a socially accepted manner, generating a sense of belonging to a group. Finally, roles represent a social position defined socially and/or personally, as well as a set of related attitudes and behaviors, such as the role of parents, spouses, grandparents, workers, and students, ranging from productive to leisure activities (Kielhofner, 2007; Oakley et al., 1986).
Participation in multiple roles is related to greater psychological and cognitive well-being (Adelmann, 1994; Ahrens & Ryff, 2006). Paradoxically, in old age the loss of roles (widowhood, retirement) is frequent (Cohen-Mansfield et al., 2016; Jonsson et al., 1997; Kielhofner, 1980), and therefore it is necessary to compensate for these with new roles or activities to prevent cognitive deterioration (Gyasi et al., 2019; Tan et al., 2019). In addition, there are sex differences in role performance, interests, and values (Hayes et al., 2018). The socialization and acquisition of traditional roles differ in men (who are more dedicated to the role of worker) and women (role of wife and mother) (Smith et al., 2018) in addition to carrying different associated values in their performance (instrumental type in men and personal type in women) (Mausz et al., 2022).
Cognitive stimulation is a nonpharmacological intervention that consists of participating in a series of group activities and discussions (typically in a group) aimed at improving cognitive and social functioning in general (Clare & Woods, 2004). Cognitive stimulation increases social participation (Lee et al., 2019; Tan et al., 2019) and cognitive function (Carballo-García et al., 2013; Fernández-Prado et al., 2012; Gonzalez-Moreno et al., 2022; Jung et al., 2021), thus increasing the number of roles and the cognitive reserve (Clare et al., 2017; Mao et al., 2020; Zhu et al., 2017). Cognitive stimulation programs are cost-effective in older adults; however, they need to be incorporated more into practice (Turcotte et al., 2018; Zubatsky et al., 2022), for example, by attempting to incorporate social participation interventions. These interventions improve social and leisure activity participation, self-efficacy and self-confidence, social interactions, participation in outdoor activities, self-assessment of health, and healthcare cost reduction (Turcotte et al., 2018). Therefore, this study aims to analyze through a randomized clinical trial whether roles, values, interests, and mental work occupation could mediate the effectiveness of a cognitive stimulation program in older adults in primary care and whether this mediation could be different according to sex.
Materials and Methods
Design and Participants
This study is a randomized clinical trial that follows consort guidelines (Albert Cobos-Carbo & Augustovski, 2011). The study populations are the people seen in primary care consultations who receive regular medical and nursing care at the San José Norte-Centro de Zaragoza health center and who have agreed to participate in this study. Participants were recruited in two ways: by referral from family physicians (who had previously received a clinical information session on the study), and by employing information posters placed at the doors of the medical offices.
To detect the proportion of individuals with a certain level of cognitive impairment, according to the scores obtained in the Spanish version of the Mini-Mental State Examination (MEC-35) (Lobo et al., 1979), between 32 and 35 points was the normal cognition group (NC), between 28 and 31 points was the subtle cognitive impairment group (SCD), and between 24 and 27 points was the level impairment group (LD) (Friedman et al., 2012; Vinyoles Bargalló et al., 2002) (as a three-category qualitative variable). The sample size was calculated for an expected proportion of 30%, with a 6% error and a confidence level of 95%. For this calculation, we used an algorithm implemented in WinEpi 2, and an unknowing reference population has been assumed (Vallejo et al., 2013). This algorithm is based on a binomial distribution and the Wilson score method to calculate the sample size required to determine a proportion avoiding misestimation of the traditional method based on a normal distribution. The sample size required was between 225 and 242 individuals depending on the distribution assumed (from normal to binomial). Finally, 232 individuals participated, thus reaching the calculated sample size.
The inclusion criteria were ≥65 years with a score of ≥24 on the MEC-35. The exclusion criteria were institutionalization, deafness, blindness, neuropsychiatric disorders, motor difficulties, and having participated in a formal structured program of cognitive stimulation at any time in the past 12 months. All participants were informed of the nature of the study, its objectives, and their voluntary participation, and they could leave the study at any time.
Treatment Allocation
Participants were randomized into two groups: the intervention group (IG) and control group (CG), performing stratified randomization according to the scores obtained on the MEC-35 (Lobo et al., 1979): between 32 and 35 points was the NC group, between 28 and 31 points was the SCD group, and between 24 and 27 points was the LD group (Friedman et al., 2012; Vinyoles Bargalló et al., 2002). Randomization was performed by an anonymous independent therapist, using an opaque box containing the participants' file numbers once the first author verified the inclusion criteria; the sequence was blinded.
Intervention
The intervention was carried out in a day center for older adults. All participants were blinded to subgroup assignment on account of randomization (NC, SCD, and LD). The treatment using mental activation notebooks was carried out by two qualified occupational therapists. The program consisted of 10 sessions of 45 min/week for 10 weeks, where the different cognitive aspects—“memory,” “orientation,” “language,” “praxis,” “gnosis,” “calculation,” “perception,” “reasoning,” “visual attention,” “executive functions”—were worked on, and a group correction of practical exercises was carried out (Arilla Viartola et al., 2010). The intervention was carried out in small groups, although each participant had an individual mental activation notebook. In the design of these notebooks, not only have the cognitive elements been taken into account but also the MOHO (i.e., the different occupations and the hobbies and roles played were taken into account). In each session, a single cognitive aspect of those mentioned above was worked on, with a theoretical explanation of it that contained theoretical-practical strategies, then individually each participant performed four exercises of this cognitive aspect, with a final group sharing as reinforcement. The number of sessions performed was registered. They needed to carry out at least 80% of the intervention, although it was necessary that if they could not attend a session, it was explained to them another day so they had time to carry it out later. Further details about the intervention have already been published (Calatayud et al., 2020).
Outcome Measures and Instruments
Study participants were assessed on all outcome measures at baseline (pre-) and at 10 weeks (post-intervention) by different blinded occupational therapists. The evaluators received a 20-hour theoretical-practical training to guarantee the homogeneous application of the tests. The sociodemographic variables studied were age and sex. As a clinical variable, the diagnosis of “anxiety” and “depression” was studied by a psychiatrist.
The primary outcomes were changes in cognitive level, assessed with the MEC-35 (Lobo et al., 1979) Spanish version of the Mini-Mental State Examination (MMSE) (Folstein et al., 1975). It evaluates eight components: temporal and spatial orientation (10 points), fixation memory (3 points), attention (3 points), calculation (5 points), short-term memory (3 points), language and praxis (11 points). Its sensitivity is 85–90%, and its specificity is 69%. As secondary outcome variables, the list of roles, interests, values, and mental occupation status have been evaluated.
The “role checklist” was used for measurement. This is a checklist of roles suitable for older people that evaluates along a time continuum the roles that have been most useful in organizing the individual’s daily life into a satisfactory routine. These roles contain a brief definition and include student, worker, caregiver, landlord, friend, family member, religious participant, hobbyist, organizational participant, and “other” if the role is not specified in the list. The list shows the definition of each role and the frequency of its performance. For example, the family member role refers to spending time doing something at least once in the past week with a family member, such as a spouse, parent, or another relative. The key phrase is “once a week” (Oakley et al., 1986). Roles were assessed using the Spanish version of the role checklist, whose test-retest reliability, measured by weighted Kappa, is 0.74. Roles were divided into low (0–1 role), medium (two to three roles), and high (more than three roles) (Scott et al., 2017).
To determine the interests of the participants, the Matsutsuyu (1969) interest list was administered, which collects the interest patterns of the older adults. This list asks the respondent for a summary of their history of interests corresponding to leisure time, indicating their most pleasurable activities. The reliability of the test is 0.92. As for validity, it is based on three criteria: the universality and comprehensibility of the items and their relevance to the clinic. The items and their categorization appear to have form validity. The interests were subdivided into three categories (one interest, two to three interests, more than three interests).
Values were divided into two categories: non-personal (including health, happiness, peace, tranquility, family, love, and friendship) and social (including human values, culture, hope and religion, and independence) based on a quantitative ranking according to participants’ responses, in line with the MOHO (Kielhofner, 2007). The subdivision of mental occupational status was done according to three levels: low, medium, and high for each, according to the classification of Grotz et al. (2018).
Ethical considerations
This study was approved by the Research Ethics Committee of the Autonomous Community of Aragón, protocol number (CEICA PI11/90 and PI11/00091) and registered on ClinicalTrials.gov Identifier (NCT03831061 and NCT04648670). All personal data protection regulations were respected. Participants were informed of the study objectives, and they signed written informed consent. The deontological norms recognized by the Declaration of Helsinki (World Medical Association, 2013) and good clinical practice norms were followed, and current legislation was complied with.
Statistical analysis
Statistical analysis was performed with IBM SPSS Statistics Package, v.22. The descriptive statistics are shown according to the nature of each variable. Then, for quantitative variables, the mean (
The Pearson chi-square test was used to determine associations between qualitative variables. Differences between groups in the cognitive measurements were evaluated using the nonparametric Mann–Whitney U and paired samples Wilcoxon tests. Moreover, Spearman correlation coefficients between the cognitive measurements were calculated, and using the ANOVA analysis some predictive multiple linear regression models are given.
Results
This study included 232 older adults with MEC-35 scores ≥24 points randomly distributed, 130 IG and 102 CG. The flow of participants and dropouts in the different phases of the study is shown in Figure 1. Flowchart of participants and dropouts in the different phases of the study. Note. Non-localized: one of the reasons for abandonment, it means that the participants could not be located (i.e., the researchers could not contact them by telephone, even after trying 10 times).
Socio-Demographic, Clinical, and Occupational Characteristics of the Participants by Protocol (Pre-Test and Post-Test Participation).
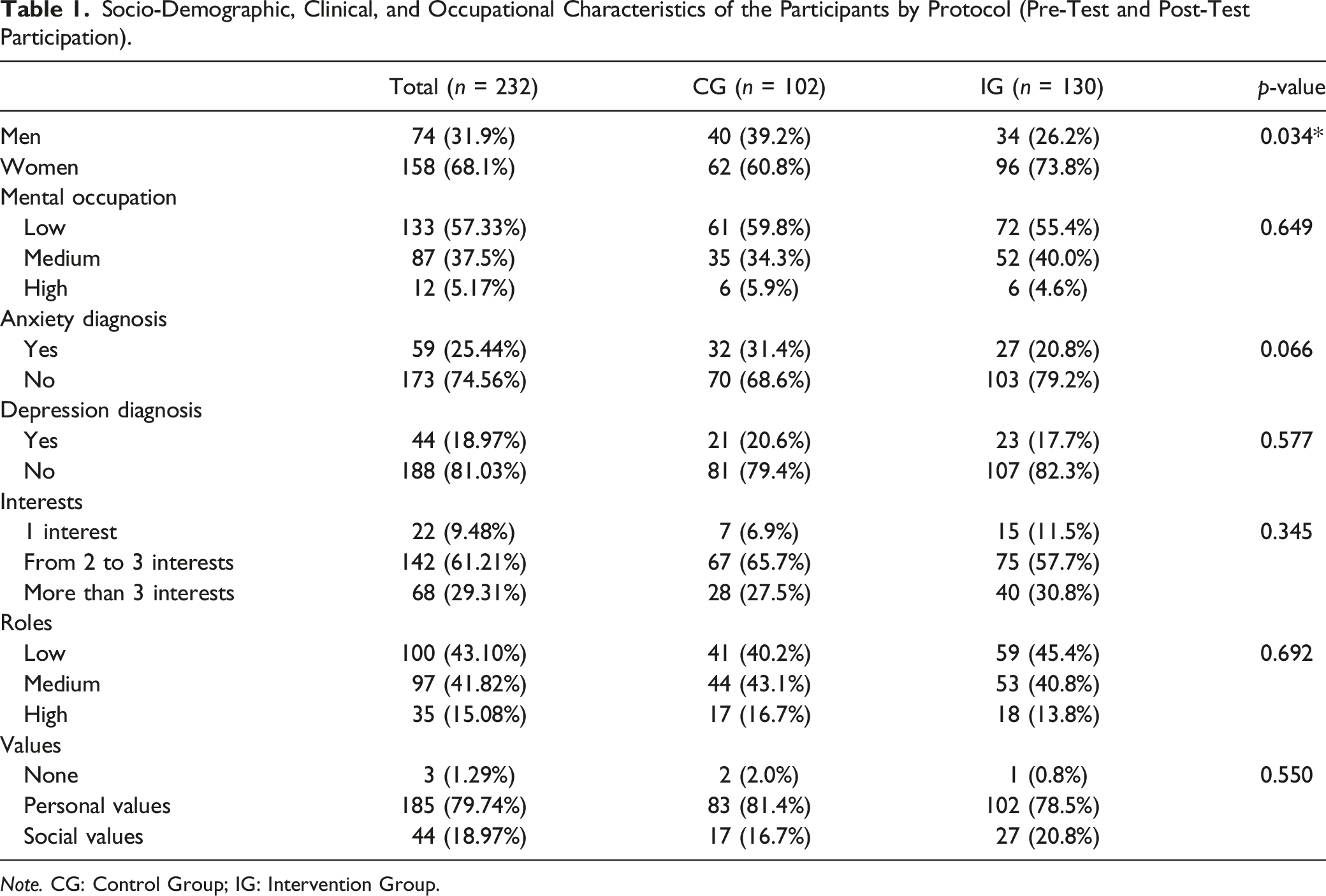
Note. CG: Control Group; IG: Intervention Group.
Mean Differences Tests Between Age and Main Variable of Cognitive Impairment (MEC-35).
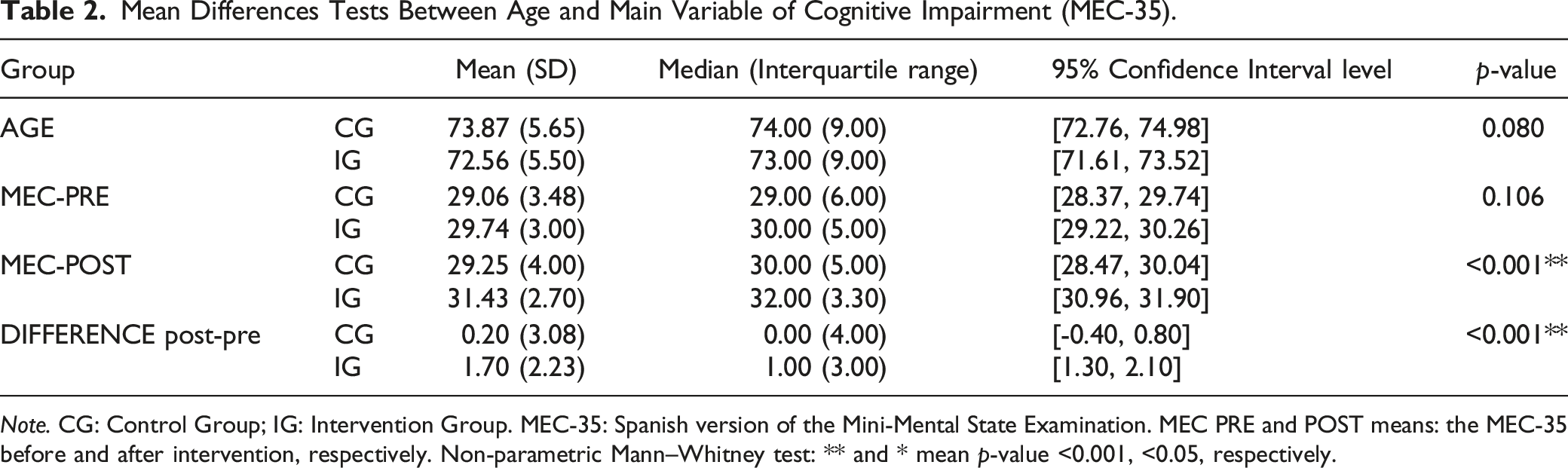
Note. CG: Control Group; IG: Intervention Group. MEC-35: Spanish version of the Mini-Mental State Examination. MEC PRE and POST means: the MEC-35 before and after intervention, respectively. Non-parametric Mann–Whitney test: ** and * mean p-value <0.001, <0.05, respectively.

Difference between the MEC after the intervention and the baseline MEC, for IG and CG according to sex.
Effect by Sex on MEC-35 After Intervention According to Occupational Variables, Roles, Interests, Values, and Mental Occupation in the Work Stage.
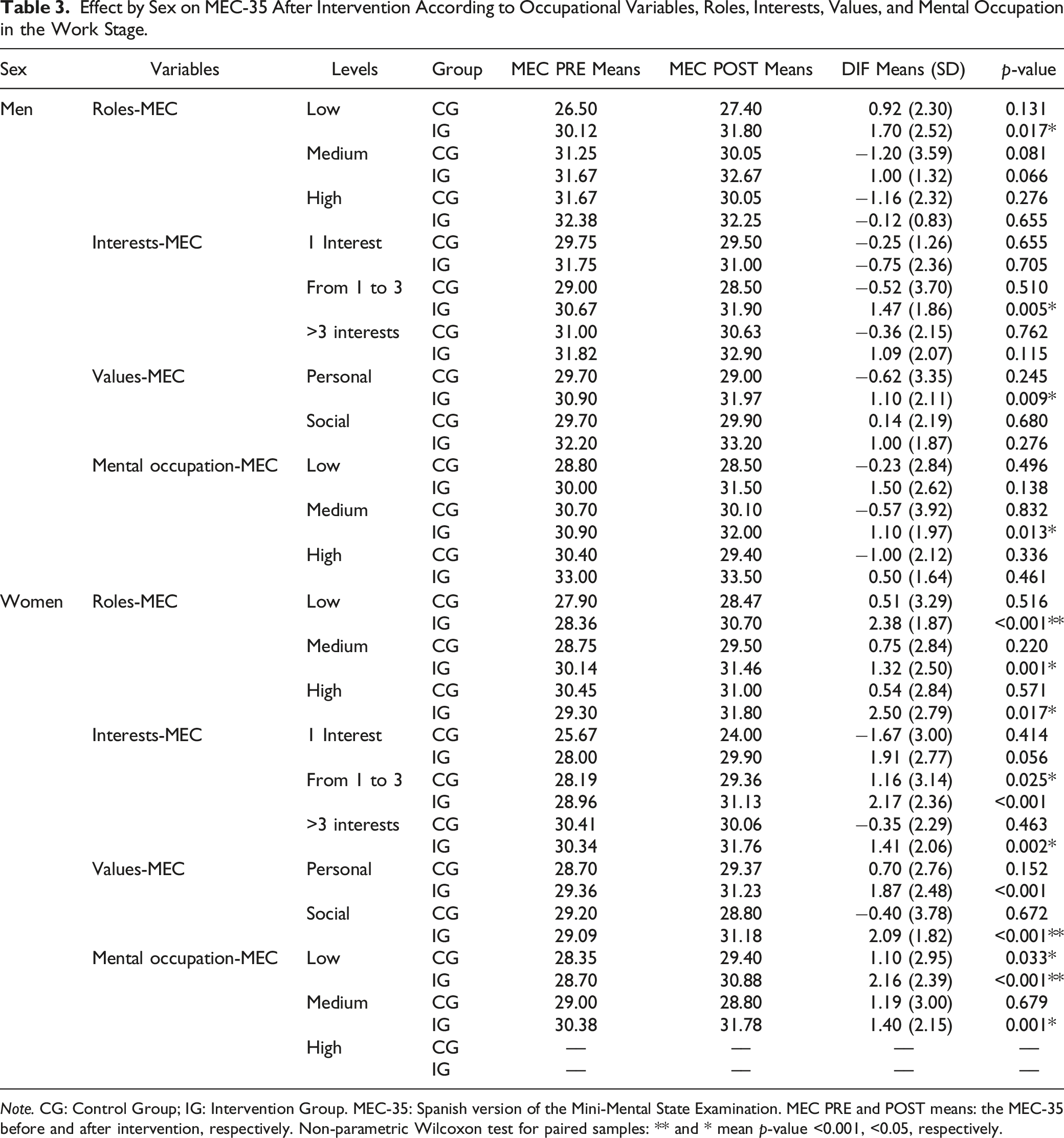
Note. CG: Control Group; IG: Intervention Group. MEC-35: Spanish version of the Mini-Mental State Examination. MEC PRE and POST means: the MEC-35 before and after intervention, respectively. Non-parametric Wilcoxon test for paired samples: ** and * mean p-value <0.001, <0.05, respectively.
With respect to interests, in women we found statistically significant differences in the IG in practically all three cases (for one interest, it is on the borderline). For men, we only found significant differences in the IG at the intermediate level (from one to three interests p = 0.005). Interestingly, we should note that there are also statistically significant differences in the CG at this level for women (p = 0.025).
As far as values are concerned, we found statistically significant differences in women in the IG in the two types of values (personal and social, both of them p < 0.001). In the case of men, these differences have only been found in the IG of those referring to personal values (p = 0.009).
Regarding mental occupation, women showed statistically significant differences in the IG in the two levels analyzed (low p < 0.001 and medium p = 0.001), while men showed this difference only in the medium level of mental occupation (p = 0.013). Moreover, these differences are significant in CG in women with a low level of mental occupation (p = 0.033). We note also that no woman in the study worked in an occupationally complex job (i.e., occupations that are characterized by highly sophisticated work) during her lifetime.
Predictive Linear Regression Model in Relation to the MEC POST-MEC PRE, Only With the Significant Coefficients by Sex (Rmen2 = 0.198*, Rwomen2 = 0.130*).
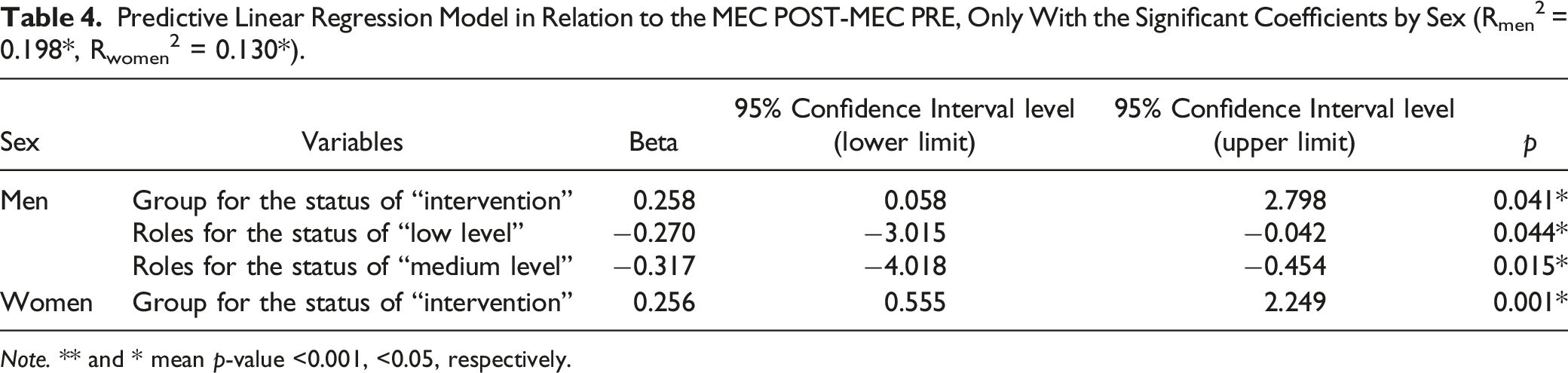
Note. ** and * mean p-value <0.001, <0.05, respectively.
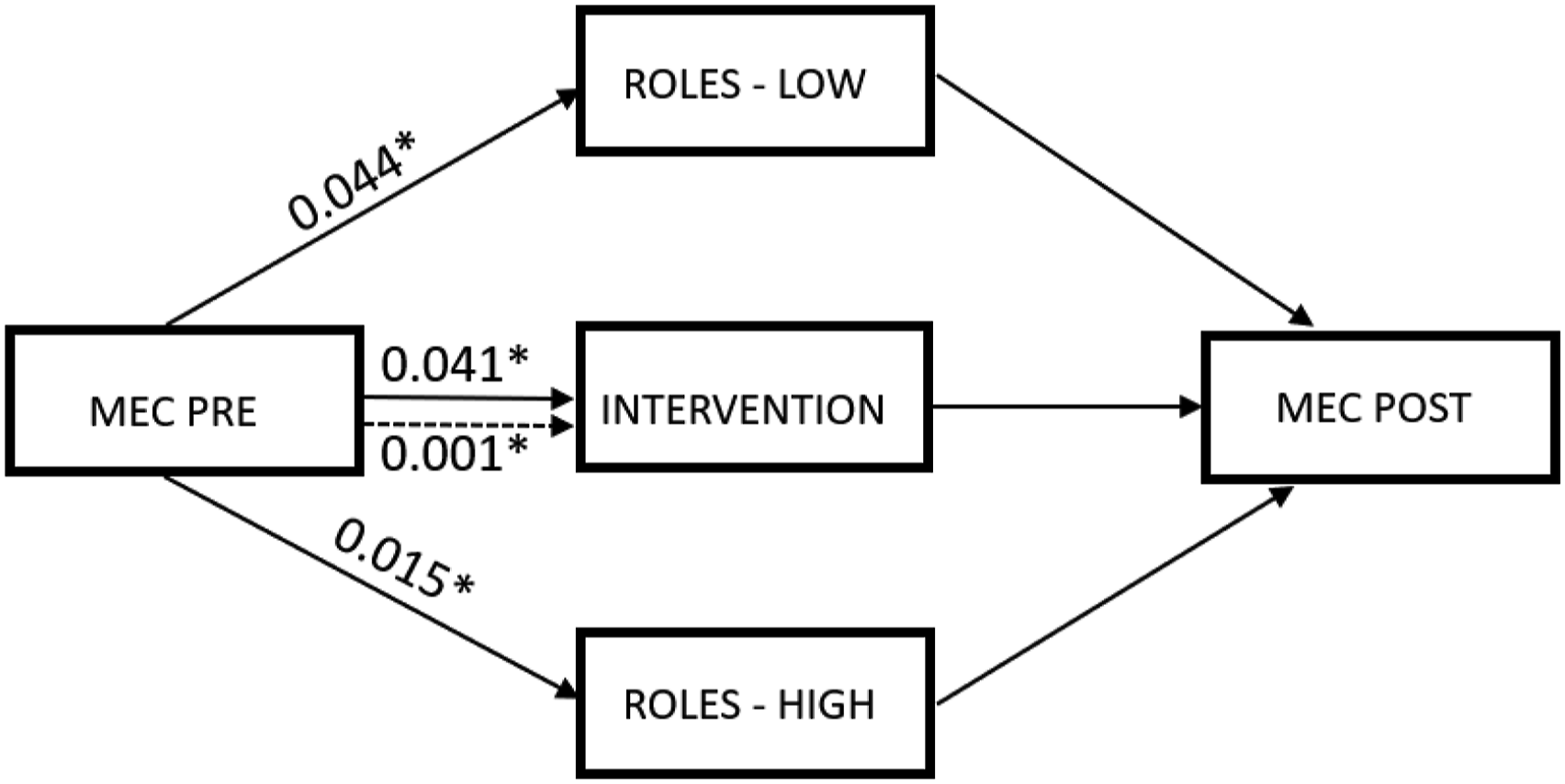
Representation of the predictive linear regression model for MEC post-intervention. The p-values in the continuous lines correspond to the significant variables in the model by men, and the p-values in the dashed line correspond to the significant variable in the model by women.
Discussion
In this randomized clinical trial, we have analyzed whether roles, values, interests, and the state of mental occupation could mediate cognitive effects by sex after the application of a cognitive stimulation program in 232 older adults. At baseline, a significant difference was observed between the percentage of men and women. In the region where the study was conducted, and in Spain in general, the percentage of women over 75 years of age is 60% higher than that of men. Our program has increased the cognitive level of the participants (Table 2, rows 4–5). The literature highlights that these programs optimize cognitive functioning in older adults (Fernández-Prado et al., 2012; Hong et al., 2021; Jung et al., 2021) in both men and women (Whitley et al., 2020), although the cognitive areas of improvement are different by sex. While men perform better on working memory, sustained attention, and verbal fluency, women perform above men with respect to verbal memory and verbal learning tasks (Navarro et al., 2014). In the present study, the cognitive effect achieved is different according to sex, and also according to roles, interests, values, and occupational mood. It is highlighted that women improve their cognitive level regardless of these aspects, but in men, this improvement is clearly marked by these factors (Table 3).
About the roles, we interpret from our clinical experience that the program in men may have added a new interest and significant role related to its instrumental values. The literature explains that differences in the meaning assigned to occupational roles could be partially responsible for the cognitive advantage of men over women (Ahrens & Ryff, 2006; Andrieu et al., 2015) (Table 3, rows 2–4).
Women, who are apparently better suited to multiple roles than men, may not adequately buffer lost roles after retirement (Gyasi et al., 2019; Rafael et al., 2021; Tan et al., 2019) and focus on those in which they feel more responsibility (such as grandmothers and caregivers), which could cause opposite effects on cognitive health (Burn & Szoeke, 2015; Jutras & Veilleux, 1991) (Table 3, rows 13–15). Participating in more activities and interests is related to a better adaptation to the aging process due to the increase in cognitive reserve that each new activity and role produces (Clare et al., 2017; Gulley et al., 2011; Kielhofner, 2007; Kim et al., 2021; Mao et al., 2020; Oakley et al., 1986; Zhu et al., 2017). Our results are congruent with the multirole theory and MOHO (Ahrens & Ryff, 2006).
Regarding values, our study only found differences in men, possibly because they identify with more personal values, such as being ambitious, intellectual, capable, and responsible (Antonovsky & Sagy, 1990). Women, on the other hand, benefited from the program regardless of their values. In contrast, the literature shows that women with more social and spiritual values benefit from better mental health (Hybels et al., 2018) (Table 3, rows 8–9, 19–20). With respect to mental occupation, our study demonstrates similarly to other studies that cognitive performance is higher if the cognitive level involved in the occupation developed in adulthood is high (Vemuri et al., 2014), which lowers the risk of dementia in old age (Kivimäki et al., 2021). Educational and occupational differences by sex could determine these cognitive differences in men and women in old age (Hyun et al., 2022) (Table 3, rows 10–12, 21–23).
Regarding the loss of roles, retirement is an event with different meanings from the escape from hard work and the opportunity to dedicate time to other interests, studies, or family to the loss of social contact and the interruption of a source of value and personal meaning (Jonsson et al., 1997). Although retirement is associated with poorer mental health in both sexes, it is more marked in men (Milner et al., 2021). Understanding these sex differences in the transition to retirement process will help occupational therapists make the necessary adaptations for healthy aging (Eagers et al., 2018, 2020). However, health promotion in retirement is an area which needs scientific and economic investment as there is a lack of evidence that describes programs directed toward retirees and their families and that measure the meaningfulness and appropriateness of what concerns their health status (Loureiro et al., 2015).
Finally, upon analysis of the mediation effects, it is clear that the predictive linear regression model for the improvement of the cognitive function can validate the mediation effects of the IG group and the low and medium level of roles. Moreover, these effects are moderated by sex. Therefore, in men, they mediate both IG and roles, whereas for women, only IG produces a mediation effect (Table 4). In conclusion, it is necessary to contemplate occupational elements by sex to adapt cognitive stimulation programs for older adults, and the activities designed must be significant and add value and purpose, especially in the case of men so that they increase their roles. In the case of women, equality in educational and social tasks must be provided.
Limitations
The first limitation of the study is the greater participation of women in the program. On the other hand, it is a cultural fact that Spanish women tend to be more participative and more consistent in their participation when collaborating on these types of studies. Men tend to refuse to participate, and they are much less consistent. Therefore, it is difficult to obtain a larger male sample. The second limitation is the fact that women generally have a lower educational and occupational level and a lower level of education. Another limitation of the study is the differential dropout rate between the IG and the CG, which has occurred for three reasons: the greater number of people in the CG who suffered from diseases, greater rejection of the program on account of not having received the intervention, and a greater number of people who were not located. All this is also related to the fact that the primary care services do not have an occupational therapy professional, and the follow-up of the participants was more difficult, especially in the CG since they did not receive the intervention.
Lines of Future Research
It will be necessary to further investigate these data with a population of a balanced number of men and women with similar occupational characteristics in order to extrapolate the results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.