
Abstract
This study compared a sample of Australian drivers aged 77 years and older to participants from an older driver longitudinal cohort study (Ozcandrive) and examined the relationship between resilience and self-reported driving measures within these samples. Using a survey with a subset of questions from Ozcandrive, data were collected from 237 older drivers throughout Australia. The two samples were analyzed for differences in demographics, health, resilience, and self-reported driving behavior. A series of multiple regression models were fit for each driving outcome measure for both samples. The two samples had both similarities and differences, with the largest difference observed for resilience. Strong and consistent associations were found between resilience and driving comfort, abilities, and frequency for the Australian sample. Across samples, resilience remained a significant variable in seven of 10 regression models, more than any other independent variable.
• The findings extend and confirm previous research exploring the role of resilience in aging drivers. • The strong and consistent association of resilience to several driving-related measures underscores the importance of this psychological variable in the context of aging and driving. • First insight into the resilience levels of a large sample of older adults across Australia.
• The dynamic nature of resilience, and the ability to support its development in individuals, could lend itself to inclusion in transport-related behavioral change programs or interventions intended to increase appropriate decision making about driving. • Increasing resilience among older drivers has the potential to extend safe community mobility, alleviating the negative impacts of driving cessation.What this paper adds
Applications of study findings
In the coming decades, there will be a marked increase in the number and proportion of adults aged 75 and older in most industrialized countries (United Nations, Department of Economic and Social Affairs, Population Division, 2019). This demographic shift has brought increased attention to the issues of older driver safety and mobility. Mobility is often inextricably linked to the ability to drive a personal vehicle, enabling individuals to engage within the community and stay socially connected (Oxley & Whelan, 2008). Research shows that many older adults are dependent on personal vehicles to maintain mobility and consider them their primary mode of transport (Newbold & Scott, 2017).
Driving is a complex activity that requires coordination and integration of visual, cognitive, and psychomotor abilities (Boot et al., 2014). Older adults experience declines in these abilities due to the normal aging process, medical conditions that are more common in older age, and medications used to treat these conditions (Eby et al., 2019). To compensate for functional declines, older adults adopt coping mechanisms, including changing the way they think or feel about their declines or adapting their driving behavior (Choi et al., 2012). The latter may include self-regulation, the process by which individuals modify or adjust their driving patterns by driving less or intentionally avoiding situations considered challenging (Molnar et al., 2015). Such behaviors may allow older adults to meet their mobility needs for a longer time.
Many studies have highlighted the importance of driver perceptions (particularly confidence or comfort) and their impact on driving practices of older adults (Blanchard & Myers, 2010; MacDonald et al., 2008; Molnar et al., 2015; Myers et al., 2008). Psychological resilience is another factor recently examined in relation to aging driver behavior (St Louis et al., 2020). Resilience is a multifaceted concept that has been defined in myriad ways across disciplines. A synthesis of 271 research articles resulted in defining psychological resilience as, “the process of effectively negotiating, adapting to, or managing significant sources of stress or trauma” (Windle, 2011, p. 163). Challenges faced in early life differ from those in later life, with older people managing age-related declines in physical and cognitive functioning as well as other external factors that have an influence on health and well-being. Key characteristics of resilient older adults generally fall into three categories: mental, physical, and social (MacLeod et al., 2016). For example, greater resilience is associated with optimism, adaptive coping skills, lower rates of depression, increased physical activity, greater independence on Activities of Daily Living, and higher levels of social support and connectedness with others.
A unique aspect of resilience is that it is modifiable, naturally evolving throughout an individual’s lifespan (Kinsel, 2005), and can also be learned or promoted through appropriate intervention (Resnick et al., 2018). A systematic review of interventions for increasing resilience identified several potentially modifiable psychosocial factors associated with resilience, such as self-esteem, active coping, self-efficacy, optimism, and positive reappraisal (Helmreich et al., 2017). Interventions have been designed to target and strengthen these psychosocial factors, thereby increasing resilience.
As people age into older adulthood, they are likely to experience changes, such as health issues or disability, that can significantly impact their driving and mobility. The process of driving modification, reduction, and cessation can be characterized as an age-related life transition. Research suggests that even when older adults plan to cease driving, they are not confident in their ability to adapt to life without driving (Liddle et al., 2014), and this feeling can impact judgment and decision-making regarding mobility. Resilience can moderate the impacts of stressful life events or transitions (Clark et al., 2010), such as the process of driving reduction and transitioning to non-driving.
Previous studies using data from Ozcandrive, a longitudinal older driver cohort study in Australia (Marshall et al., 2013), have shown significant associations between resilience and self-reported and naturalistic driving behaviors (St Louis et al., 2020). Higher levels of resilience were associated with greater driving comfort, positive perceptions of driving abilities, frequent driving in complex scenarios, and shorter trips. However, it is unclear if the findings would hold for a more general cohort of older drivers not bound by the comprehensive eligibility requirements of participating in Ozcandrive, or the potential self-selection bias of an in-depth, longitudinal study of driving and health.
No study to date has investigated resilience in a broader sample of older drivers to examine its relationship with driving-related measures. This study aimed to: 1) compare resilience, health, and self-reported driving behaviors of a broad sample of older drivers across Australia (referred to as the “Australian sample”) with the Ozcandrive sample and 2) determine if resilience is associated with driving-related outcomes in the Australian sample. While it is important to recognize where the samples converge, it is also important to understand divergences and particularly, implications for the consideration of resilience in aging and driving translational research. Given the eligibility requirements and longitudinal nature of the Ozcandrive study, we hypothesize that: 1) the Ozcandrive sample will report significantly higher scores on health, resilience, and driving-related measures compared to the Australian sample and 2) based on previous Ozcandrive results, resilience will be a significant variable in explaining the variance in self-reported driving behaviors in the Australian sample.
Method
Participants
The Candrive/Ozcandrive Study
The Candrive/Ozcandrive prospective cohort study was a multicenter, international research program comprised of 1230 participants from Canada (n = 928), Australia (n = 257), and New Zealand (n = 45). Ozcandrive participants in Australia were recruited through membership of the Royal Automobile Club of Victoria (RACV) and previous participants who had indicated willingness to be contacted for future studies. Additional recruitment efforts included advertisement in newspapers, newsletters, posters, and presentations to senior-related associations. Recruitment occurred from June 2010 to June 2011. Inclusion criteria included: being 75 years or older, having a valid driver’s license, driving a vehicle model year 2002 or newer, driving at least four times a week, and residing in local regions of Melbourne. Participants were not eligible if they: planned to move out of the local region, had a medical contraindication to driving within the previous 6 months (Austroads, 2017), or had been diagnosed with a progressive medical condition that could affect driving (e.g., macular degeneration). Participants were enrolled for up to 8 years and completed annual in-person assessments to document physical and cognitive performance, and to collect information on demographics, health and functioning, and driving behavior. Additionally, psychosocial questionnaires regarding driving and well-being were completed by participants at home and returned by mail (Marshall et al., 2013). The current study utilized Ozcandrive data from Year 3; the first year in which resilience data were collected (n = 183).
The Driving, Health, and Well-being Study
The Driving, Health, and Well-being study used a cross-sectional survey design to gather information on resilience, health, and driving behaviors of adults across Australia. This study provided a broader opportunity to examine resilience and driving throughout adulthood, although the focus of the current study is older adults. The survey was pilot tested with 10 volunteers representing a range of ages and balanced by sex. Based on feedback, changes were made to the layout and instructions to provide clarity and ease of understanding. Several recruitment strategies were employed to gain access to older age groups, including partnering with University of the Third Age, National Council on the Aging, and the RACV. Recruitment efforts included newsletters, direct email to organization membership, word-of-mouth, and online advertisement. Potential participants were directed to an online survey link and provided contact information to request a paper copy. Upon completion, participants were invited to opt into a draw to win one of five $100 gift vouchers.
The survey took approximately 20 minutes to complete, was approved by the Monash University Human Research Ethics Committee (MUHREC 18977), and made available online (Qualtrics, https://www.qualtrics.com) and in paper format. Participants were eligible to complete the survey if they: were 18 years or older, lived in Australia, had a valid driver’s license, and drove at least once per week. The current study was limited to participants aged 77 years and older to be more comparable to Ozcandrive participants. The survey was administered from May 2019 through March 2020.
Measures
The Driving, Health, and Well-being survey contained questions from the existing Ozcandrive data collection protocol related to sociodemographic information, health, resilience, and driving behavior.
Sociodemographics
Participants provided information on: age (continuous variable), highest level of education, relationship status (multilevel categorical variables), location of residence, and employment status (dichotomous variables: urban/rural and yes/no, respectively).
Health
Self-rated health was measured by asking participants: “In general, would you say your health is excellent, very good, good, fair, or poor?” (Ware & Sherbourne, 1992). Due to low numbers of participants reporting ‘poor’ health, fair and poor were collapsed into one category.
Resilience
Participants’ resilience was measured using the 14-item Resilience Scale (Wagnild, 2009). The scale was developed using grounded theory research which identified five underlying characteristics of resilience that serve as the conceptual foundation: self-reliance, purpose, equanimity, perseverance, and authenticity. Participants were asked to rate their agreement on each item (e.g., “I am determined”) on a 7-point scale from strongly disagree to strongly agree; a valid total score required completion of all items. Total scores range from 14 to 98, with higher scores indicating greater resilience.
Driving Characteristics
Driving frequency and distance were assessed with two questions. Participants were asked “How frequently do you drive?” Response options were: daily, 4–6 times per week, 2–3 times per week, and once per week. Participants then estimated the number of kilometers driven in the previous year, with categories ranging from 0–1000 km to greater than 25,000 km.
Five self-reported measures examined participants’ level of comfort while driving in various situations during the day and night, perceptions of their driving ability, and driving frequency and avoidance. These were the outcome measures in the analyses.
Driving comfort: Driving comfort was measured using the 13-item daytime and 16-item nighttime Driving Comfort Scales (DCS-D and DCS-N, respectively). Self-efficacy, as defined by Social Cognitive Theory (Bandura, 1986), serves as the basis for these scales which were developed with older drivers and subjected to rigorous psychometric examination using Rasch analysis (Blanchard & Myers, 2010; MacDonald et al., 2008; Myers et al., 2008). Each driving scenario (e.g., “How comfortable are you driving at night in light rain?”) was rated on a 5-point scale from 0% (not at all comfortable) to 100% (completely comfortable). Total scores range from 0% to 100%, with higher scores indicating greater driving comfort.
Perceived driving abilities: Driving abilities were measured with the 15-item Perceived Driving Abilities (PDA) scale, which was also developed with older drivers and found to have strong psychometric properties (Blanchard & Myers, 2010; MacDonald et al., 2008; Myers et al., 2008). Driving abilities (e.g., to reverse) were rated on a 4-point scale (0 = poor to 3 = very good). Total scores range from 0 to 45, with higher scores indicating more positive perceptions of driving abilities.
Situational driving frequency and avoidance: Driving frequency and avoidance were assessed using the Situational Driving Frequency (SDF) and Avoidance (SDA) scales. Participants reported how often they drive, on average, in 14 different driving scenarios (e.g., in new/unfamiliar areas) on a 5-point scale from never (0) to very often (4 = 4 to 7 days a week). Total scores range from 0 to 56, with higher scores indicating driving more often in challenging situations. The SDA scale is a list of 19 driving situations and participants were asked to select all situations they try to avoid. Scores range from 0 to 19, with higher scores indicating greater avoidance (MacDonald et al., 2008; Myers et al., 2008).
Data Management and Analysis
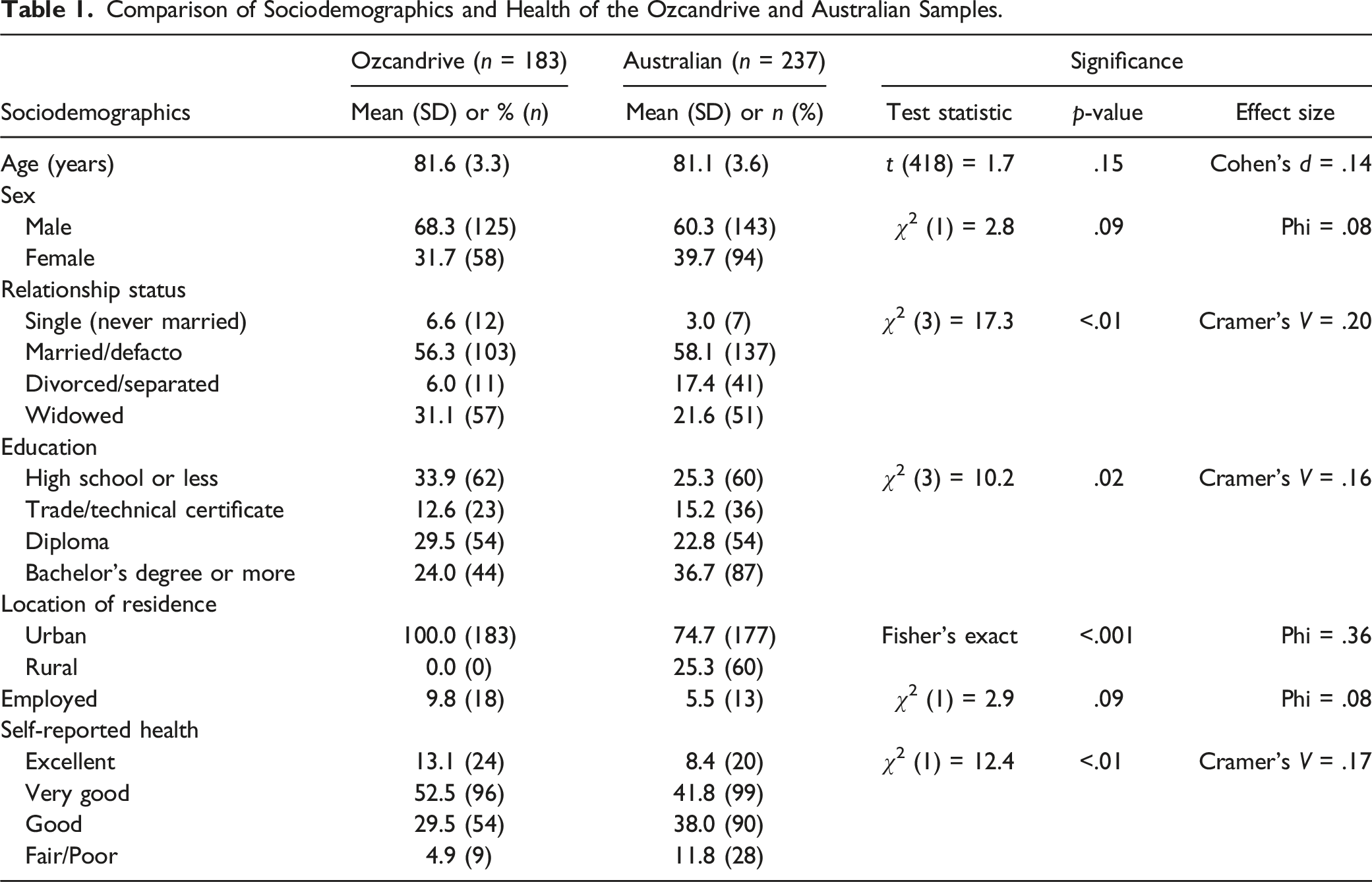
Comparison of Sociodemographics and Health of the Ozcandrive and Australian Samples.
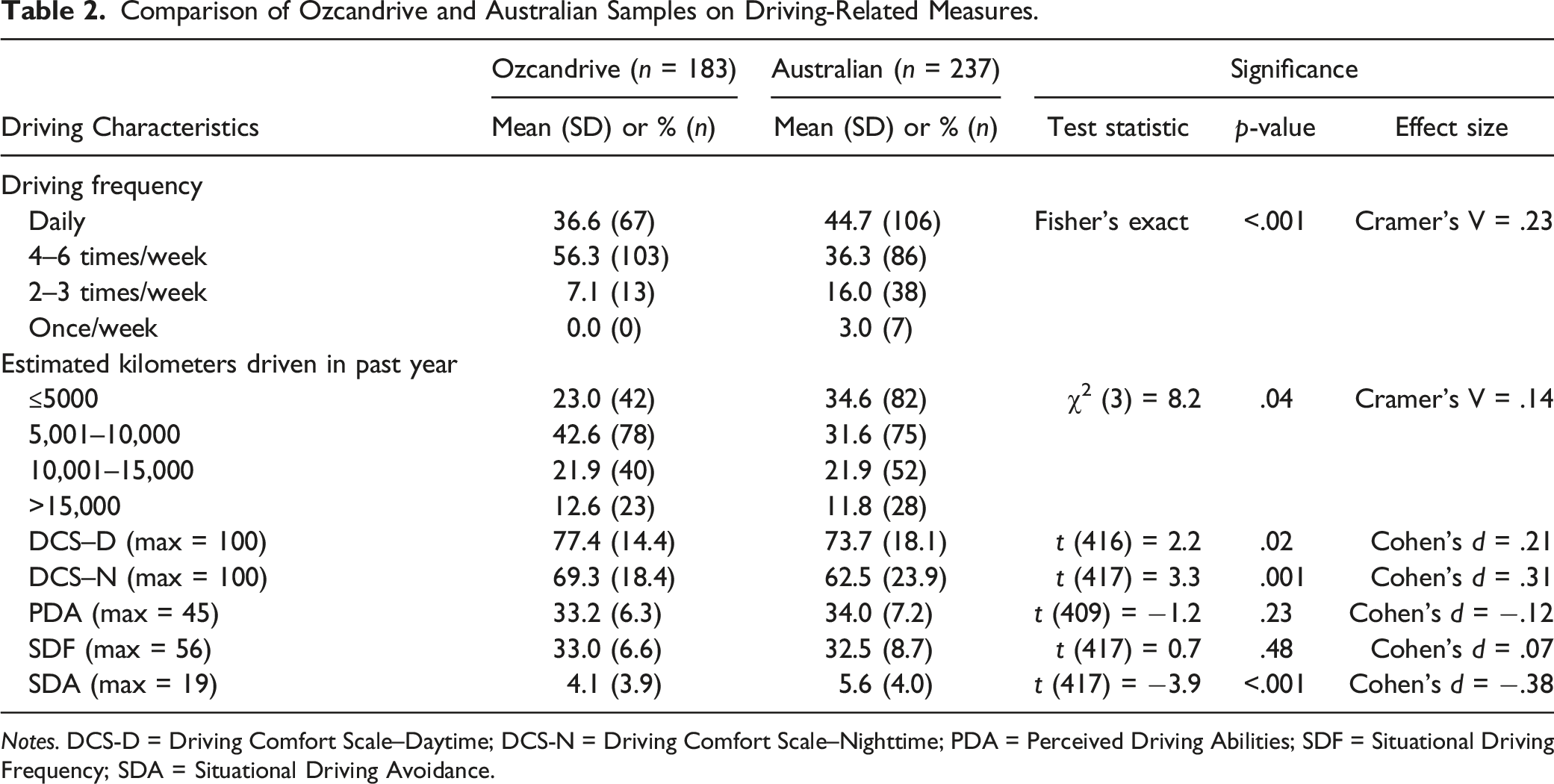
Comparison of Ozcandrive and Australian Samples on Driving-Related Measures.
Notes. DCS-D = Driving Comfort Scale–Daytime; DCS-N = Driving Comfort Scale–Nighttime; PDA = Perceived Driving Abilities; SDF = Situational Driving Frequency; SDA = Situational Driving Avoidance.
Results
Two-hundred thirty-seven participants aged 77 years and older completed the Driving, Health, and Well-being survey. Table 1 shows the sociodemographic characteristics of the two samples, along with group comparisons. Both samples had a mean age of approximately 81 years (Range 77–96 years) and a higher proportion of males. Most participants were in a married/defacto relationship. However, post-hoc pairwise comparisons with adjusted p-values revealed a significantly larger proportion of the Australian sample reported being divorced/separated compared to the Ozcandrive sample. There was no significant difference in education, with over half of both samples reporting having achieved at least a diploma. All Ozcandrive participants resided in urban areas of Victoria. The majority of the Australian sample also lived in the state of Victoria (80.1%), and one-quarter reported living in a rural area. There was no significant difference in employment status. The sample differed significantly on self-reported health, with a larger proportion of Ozcandrive participants reporting “excellent” or “very good” health compared to the Australian sample. While there were some statistically significant differences across the two samples, the effect sizes were small.
Driving-related characteristics are shown in Table 2. Most participants drove four or more times per week. Pairwise comparisons showed that a significantly larger proportion of Ozcandrive participants drove 4–6 times per week than the Australian sample. Approximately 65% of both samples drove 10,000 km or less in the previous year. Ozcandrive participants reported significantly higher scores for comfort while driving at night, and no statistical difference in driving comfort during the day. The samples were similar in reporting positive perceptions of their driving abilities. Frequency of driving in challenging situations did not differ by group; however, the Australian sample reported avoiding more driving scenarios than the Ozcandrive sample. Overall, effect sizes for group differences in driving characteristics were small.
Comparison of Resilience Scores for the Ozcandrive and Australian Samples.

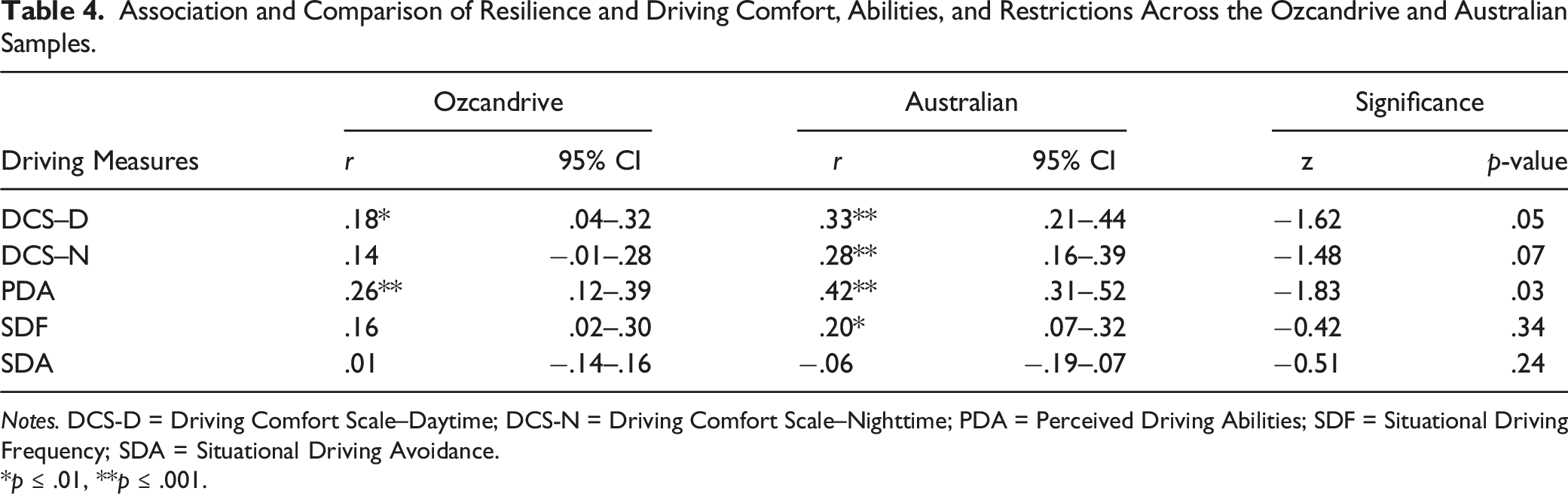
Association and Comparison of Resilience and Driving Comfort, Abilities, and Restrictions Across the Ozcandrive and Australian Samples.
Notes. DCS-D = Driving Comfort Scale–Daytime; DCS-N = Driving Comfort Scale–Nighttime; PDA = Perceived Driving Abilities; SDF = Situational Driving Frequency; SDA = Situational Driving Avoidance.
*p ≤ .01, **p ≤ .001.
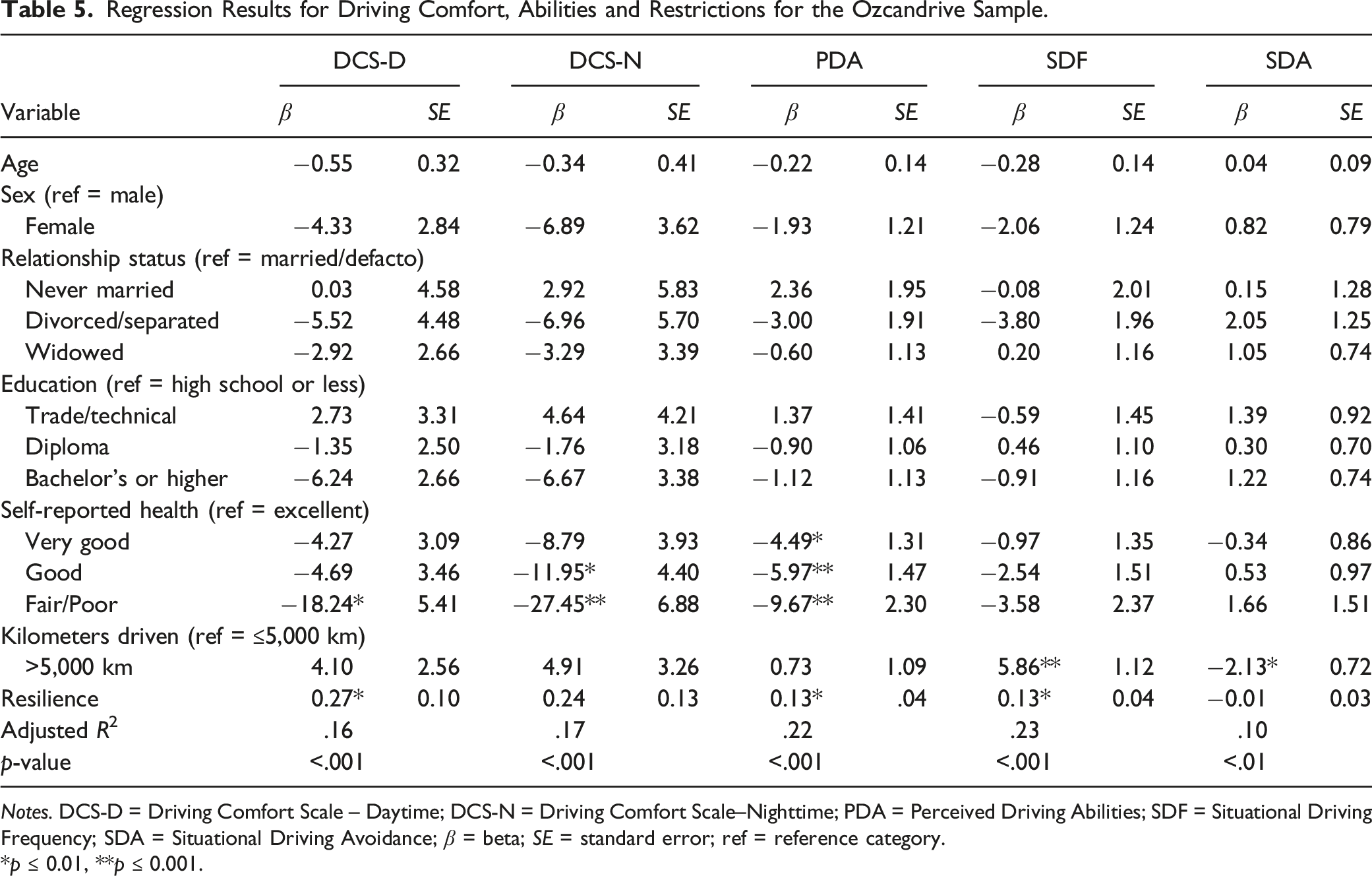
Regression Results for Driving Comfort, Abilities and Restrictions for the Ozcandrive Sample.
Notes. DCS-D = Driving Comfort Scale – Daytime; DCS-N = Driving Comfort Scale–Nighttime; PDA = Perceived Driving Abilities; SDF = Situational Driving Frequency; SDA = Situational Driving Avoidance; β = beta; SE = standard error; ref = reference category.
*p ≤ 0.01, **p ≤ 0.001.
Regression Results for Driving Comfort, Abilities and Restrictions for the Australian Sample.

Notes. DCS-D = Driving Comfort Scale – Daytime; DCS-N = Driving Comfort Scale – Nighttime; PDA = Perceived Driving Abilities; SDF = Situational Driving Frequency; SDA = Situational Driving Avoidance; β = beta; SE = standard error; ref = reference category.
*p ≤ 0.01, **p ≤ 0.001.
Ozcandrive
In the Ozcandrive sample, driving comfort during the day was associated with self-reported health and resilience. Specifically, those reporting fair/poor health had lower driving comfort scores than those reporting excellent health, and increasing resilience corresponded to greater daytime driving comfort. Nighttime driving comfort was associated only with self-reported health. Compared to excellent health, participants reporting good and fair/poor had lower nighttime driving comfort scores.
Perceived driving ability was associated with self-reported health and resilience. Compared to those reporting excellent health, successively lower health ratings were associated with lower perceived driving abilities. Higher resilience was associated with more positive perceptions of abilities.
Frequency of driving in challenging situations was associated with kilometers driven and resilience. Compared to low mileage drivers, participants who drove more than 5000 km drove more frequently in challenging scenarios. Higher resilience scores were associated with more frequent driving in complex driving situations. Avoidance of driving situations was associated only with kilometers driven; that is, higher mileage drivers avoided fewer challenging driving scenarios compared to low mileage drivers.
Australian Sample
In the Australian sample, daytime driving comfort was associated with sex, driving exposure, and resilience. Females and those who drove less than 5000 km had lower daytime driving comfort scores. Higher resilience scores were associated with increased comfort. The same significant associations were also found for nighttime driving comfort; however, the beta coefficients were larger.
Perceived driving ability was associated with kilometers driven and resilience. Compared to low mileage drivers, those who drove more than 5000 km had more positive perceptions of their driving abilities. Higher resilience was also related to more positive perceptions of abilities.
Higher resilience and driving more than 5000 km were related to more frequent driving in challenging scenarios. Avoidance of driving situations was associated with older age, being female, and never married compared to married/defacto.
Discussion
This study had two aims: to compare the Ozcandrive sample to a broader sample of older adults in Australia on resilience, health and driving measures, and to determine if there was a significant association between resilience and driving-related outcome measures. We hypothesized that the Ozcandrive sample would rate themselves as healthier, have higher resilience scores, and have more positive scores on driving outcome measures. We also hypothesized that resilience would be a significant variable in the regression models for the Australian sample.
There were more similarities than differences between the two samples on sociodemographic, health, and driving characteristics, and as noted, the magnitude of the differences was small. The samples were similar on age, sex, education, and employment and differed by relationship status and location of residence. As predicted, the Ozcandrive sample had higher ratings on health. With respect to driving characteristics, our hypothesis was only partially supported as the samples did not differ on kilometers driven in the previous year, daytime driving comfort, perceived driving abilities, or frequency of driving in challenging situations. However, the Ozcandrive sample drove more often each week, had higher nighttime driving comfort scores, and avoided fewer driving situations.
Due to the eligibility requirements for Ozcandrive, some of the differences are understandable, particularly regarding driving frequency and location of residence. Ozcandrive participants were required to drive at least four times per week upon recruitment (compared to once per week for the Australian sample), generating a very active group of drivers. Ozcandrive participants were also required to attend in-person assessments in the southeast suburbs of Melbourne, and therefore resided in urban areas convenient to the testing location. The Australian sample was spread nationwide and could fill out the survey in their home. Gagnon et al. (2016) compared the Candrive cohort to a representative sample of older drivers in Canada and found similar results. That is, the Candrive sample reported driving significantly more frequently than the Canadian sample and a higher proportion of Candrive participants lived in urban areas.
Higher health ratings for Ozcandrive may also be explained by other eligibility requirements, such as not having been diagnosed with a progressive disease which may impact driving. Furthermore, the Ozcandrive sample had to make an extensive time commitment to participate in a study that monitored their health and driving for several years. This may have led to self-selection bias with an overrepresentation of older adults reporting higher health status.
Where the samples differed more strongly was with respect to resilience, and results were counter to our hypothesis. The Australian sample exhibited significantly higher resilience scores than the Ozcandrive sample. The small differences in sociodemographics and health are not sufficient to explain this difference. The multifaceted nature of resilience coupled with the data available do not allow for an explicit explanation for why the Australian sample had higher resilience scores. Gathering more information about the antecedents of resilience would help to explain this difference. Higher resilience in the Australian sample corresponded to moderate associations with several driving outcome measures. Although resilience was significantly associated with daytime comfort and perceived abilities for the Ozcandrive sample, these correlations were small.
Regression modeling revealed different significant associations between independent and dependent variables for each sample, with congruence for situational driving frequency. Overall, resilience remained a significant variable in seven of the 10 regression models, more than any other independent variable. The hypothesis was supported as resilience was significant in all regression models for the Australian sample except driving avoidance. Across samples, resilience was a common significant variable for daytime comfort, perceived driving abilities, and frequency of driving in challenging situations, with positive associations within each model. As previously discussed, driving comfort is closely related to self-regulation; therefore, resilience may act as a moderator between driving comfort and self-regulatory behaviors. This link between resilience and comfort points to a new approach for understanding driving decisions. Previous research found a relationship between resilience and positive adaptation, well-being, and quality of life, and protective factors to cope with challenges of the aging process (Windle et al., 2011). Resilience in the context of aging and driving does not necessarily translate into continued driving, irrespective of declines in abilities and potential safety issues. Rather, higher resilience may help to extend safe mobility by allowing individuals to be more adaptable and willing to modify their driving behavior in response to declines in health or comfort, or to explore other forms of transportation to facilitate the transition to non-driving. The results regarding resilience in the Australian sample are especially encouraging given that they extend this significant association beyond the more tightly-constrained Ozcandrive sample.
Driving exposure played a significant role in the regression models, particularly for the Australian sample. The associations were consistent with previous findings that driving comfort scores were lower for those driving fewer than 5000 km (Hua et al., 2018; Langford et al., 2013). Resilience and driving exposure were significant variables in the models for situational driving frequency for both samples. This combination of variables helped explain approximately one-quarter of the variance in these models. Although it was important to control for distance driven, we recognize that motivations for driving and the specific situations in which participants drove were not known. Understanding the reasons for driving would allow for a more thorough explanation of these results and future research should attempt to more clearly delineate motivations for driving decisions.
Self-reported health was a significant variable in the models for driving comfort and abilities for the Ozcandrive sample, consistent with Tuokko et al. (2013) who used Candrive data. Results showed that after controlling for age and sex, daytime and nighttime comfort were significantly associated with perceived health status. Indeed, health was the sole significant variable in the model for driving comfort at night. Participants with good or fair/poor health ratings compared to excellent ratings had vastly lower scores on nighttime driving comfort, indicating the importance of perceived heath for driving in a condition commonly avoided by older drivers. While health was a significant factor for the Ozcandrive sample, it failed to reach significance for the Australian sample. Research has shown that self-reported health is a significant predictor of driving cessation in older adults (Anstey et al., 2006); however, the measure used in this study may not have been sensitive enough to capture more specific dimensions of health (e.g., vision) and subsequent impacts on driving.
Associations between driving measures and sociodemographic variables were only partially consistent with previous findings in the literature (see Dickerson et al., 2019). Age, sex, relationship status, and education were not related to any outcome measures examined in the Ozcandrive sample. Where these variables were significant in the models for the Australian sample, they were largely consistent with the direction of association found in previous studies. For example, research has shown that females report lower driving comfort and avoid more driving situations than males (Blanchard & Myers, 2010), consistent with the findings for the Australian sample.
The proportion of variance explained in the models was much higher for the Australian sample. Demographic factors shown to be associated with driving were not significant in the models for Ozcandrive, which may partially explain this difference. The modest R-square values indicate that there are other factors influencing driving behavior not considered in these analyses.
This study’s focus on resilience in older drivers helps to fill a significant gap in the literature, as there is limited research on resilience in individuals of more advanced age (Hayman et al., 2017). Moreover, resilience in the context of aging and driving has never been studied in a general sample of older drivers. The regression models show that resilience is an important factor in aging and driving behavior, even after accounting for other factors known to impact driving reduction and cessation.
Some limitations should be noted. For a true generalizability study, the Ozcandrive sample should be compared to the general population of older drivers across demographic, health, resilience, and driving-related variables. These data are not currently available. As comfort and resilience have been found to be significantly associated with driving behavior, inclusion of these measures into a study with a population-based sample would yield valuable insights. Additionally, as these data were cross-sectional, it is difficult to establish a causal relationship between resilience and driving outcomes. Previous research analyzed Ozcandrive data across 5 years and found a statistically significant increase in resilience as well as reduced driving over time (St Louis et al., 2022). As resilience is associated with adaptive coping skills, this study concluded that older adults with higher resilience may be able to more effectively engage in appropriate coping behaviors with regard to driving behavior. To help clarify causality, future research would benefit from utilizing a longitudinal research design or use of an experimental design to increase resilience.
While objective measures of health and driving would eliminate biases associated with self-reported data, previous research on older drivers has shown the utility of self-reported data. For example, Anstey et al. (2006) found that subjective feelings of health and well-being were better predictors of positive outcomes for maintaining driving in older age than chronic medical conditions and sensory impairment. Additionally, as noted, the driving outcome measures were developed with older adults, have undergone rigorous psychometric examination, and have been used in previous studies examining older driver behavior. Finally, driving frequency and avoidance were assessed via self-report, but the reasons for avoidance are not known. The reported driving behaviors may result from self-regulation or may simply reflect changes in preferences or lifestyle choices.
Conclusion
The current findings confirm and extend previous research that explored the role of resilience in relation to driving behavior in the Ozcandrive study. The strong and consistent association of resilience to several driving-related measures in a broader population of older drivers underscores the importance of this psychological variable in the context of aging and driving. The dynamic nature of resilience, and the ability to support its development in individuals, could lend itself to inclusion in transport-related behavior change programs or interventions intended to increase appropriate decision-making about driving, thereby extending safe community mobility and ultimately alleviating the impacts of driving cessation on psychosocial and health outcomes.
Footnotes
Acknowledgments
The authors thank Lorraine Atkinson, Ozcandrive Program Manager, for her role in managing and operationalizing the study for the Australian and New Zealand sites. The authors gratefully acknowledge the invaluable contribution of the Ozcandrive team, including: Amy Allen, Louise Beasley, Russ Boag, Matthew Catchlove, Cara Dawson, Johan Davydov, Lei Gryffydd, Yik-Xiang Hue, Elizabeth Jacobs, Duncan Joiner, Phuong Hua, Flora Le, Peter Liu, Jason Manakis, Kevin Mascarenhas, Rachel Osborne, Emma Owen, Hiep Pham, Glenys Smith, Jarrod Verity, Zefi Vlahodimitrakou, and Chenghao Yu. The authors also thank the Ozcandrive cohort study older drivers for their dedication. Without their commitment, this research would not have been possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a graduate research scholarship from Monash University; the Australian Research Council [grant number LP 100100078]; and the Canadian Institutes of Health Research [grant number 90429].
Human Subjects Approval Number
Monash University Human Research Ethics Committee, Project Approval Number 18977.