
Abstract
Ageism is a global challenge and a public health concern that the recent COVID-19 pandemic has further exacerbated. Existing research has mainly focused on individual factors, overlooking the association between the neighborhood-built environment and ageism. This study examined this association and whether its effect varied among areas possessing different socioeconomic characteristics. We conducted a cross-sectional survey of 1278 older people in Hong Kong and merged this with the built environment factors derived from geographical information system data. We used multivariable linear regression to examine the association. Findings revealed that more parks were significantly associated with a lower level of ageism, an impact that remained significant in low-income or low-education areas. Conversely, more libraries in high-income areas were associated with a lower level of ageism. Our findings provide urban planners and policymakers insight into planning for the built environment that reduces ageism enabling older people to achieve a better life.
Keywords
• This study sheds light on the importance of the built environment in association with ageism among older people • Parks and libraries in a locality were associated with a lower level of ageism • The association of the built environment and ageism differs in areas with different socio-economical characteristics
• This study indicates the need for future research to investigate the relationship and interaction between individual-level, social environment, and the built environment determinants of ageism • Policymakers and urban planners can incorporate our findings in future city planning to combat ageismWhat this paper adds
Applications of study findings
Introduction
Ageism, defined as “the stereotypes, prejudice, and discrimination directed towards others or oneself based on age” (World Health Organization, 2021, 2), has been widely recognized as a major threat to healthy aging, damaging older people’s health, well-being, and quality of life (Levy et al., 2012). The Covid-19 pandemic has further exacerbated ageism by characterizing older people as a homogeneous and vulnerable group (Previtali et al., 2020). Given these circumstances, combating ageism is a major action area in the United Nations’ Decade of Healthy Aging in 2021–2030 (World Health Organization, 2020).
Determinants of Ageism Against Older People
Following Butler’s (1969) introduction of the ageism concept, researchers have since identified factors associated with ageism against older people. Existing studies show that certain sociodemographic factors such as being female (Allan et al., 2014), older (Officer et al., 2020), more highly educated (Officer et al., 2020), and knowledge about aging (Cooney et al., 2021) were associated with a lower level of ageism. In addition, other studies have found that certain interpersonal factors, including presenting older people positively (Marques et al., 2020) and having better quality contact with older people (Hale, 1998), were associated with a lower level of ageism.
Recently, studies have focused on the contextual determinants and social environment of ageism. For example, Vitman et al. (2014) found that higher levels of social integration in a neighborhood were negatively associated with ageism. Moreover, studies consistently report a negative association between ageism and countries with a higher proportion of older people participating in paid and volunteer work (Bowen & Skirbekk, 2013) or with more available economic resources (Marques et al., 2020). However, the proportion of the older population in a country has yielded inconsistent results due to the difference in ageism measurements and definitions of older people (e.g., Löckenhoff et al., 2009; Officer et al., 2020).
The neighborhood-built environment is crucial for older people because they tend to spend more time in their immediate neighborhoods (Besser et al., 2017) due to lifestyle changes and age-related mobility decline (Yen et al., 2009a). Therefore, a growing number of studies have focused on the association between the built environment and ageism. For example, Van Hoof et al. (2020) studied the manifestation of ageism in the built environment from the age-friendly city framework and found that poor accessibility in buildings and public transport reflected the explicit form of ageism. In addition, Gamliel (2000) found that older people living in sheltered housing exhibit ageism against their own age group. Noon and Ayalon (2018) found age and gender segregation in public open spaces. From a macro perspective, Phillipson and Grenier (2021) investigated the relationship between urbanization and ageism, and found that privatizing land and public assets (e.g., public space, leisure centers, parks, etc.) in an urbanized society may intensify ageism. Although extensive efforts have been made to identify different determinants of ageism, existing studies on ageism are limited in two ways (Noon & Ayalon, 2018).
Firstly, we know very little about ageism among older people themselves (John, 2013). Most empirical studies on ageism focused on young people (Minichiello et al., 2000), students (Wang & Chonody, 2013), healthcare professionals, and social workers (Levy & Macdonald, 2016). As life experience affects ageism (Marques et al., 2020), we cannot extend the existing findings from these populations to understand ageism among older people.
Moreover, most existing studies on the built environment and ageism were focused on the theoretical association supported by qualitative evidence. For example, some adopted the age-friendly city framework proposed by the World Health Organization to examine the manifestation of ageism through environmental design or facilities (e.g., Chui et al., 2019; Van Hoof et al., 2020). Other researchers explored ageism through the lens of urbanization (e.g., Phillipson & Grenier, 2021). Only limited studies provided quantitative evidence on the association between the built environment and ageism. For instance, Zhong et al.’s (2022) study on the community-built environment found that the presence of religious destinations is positively associated with older people’s intra-generational interaction, which could reduce ageism. Therefore, more quantitative studies are needed to understand ageism’s determinants comprehensively.
Theoretical Rationale of this Study
A community-built environment can be associated with ageism through two pathways. Firstly, a well-designed built environment can enable higher levels of social interactions, which in turn, can reduce ageism by increasing perspective-taking and empathy, as suggested by the intergroup contact theory (Pettigrew et al., 2011). Intergroup contact theory could be applied to study intra-generation ageism, where older people disassociate themselves from being old and declining by perceiving the frail, retired, and inactive older people as an outgroup (Kydd et al., 2018). For example, Kwong and Yan (2021) found that people with quality face-to-face contact with older people displayed lower levels of ageism.
From this perspective, a built environment that facilitates social interaction in the community can help reduce ageism. For example, public parks have been identified as places with frequent intergroup contact (Neal et al., 2015). Public parks in Hong Kong are open to people of any age group with no specific restriction. Therefore, visiting public parks could bring people together and facilitate repeated social interaction (Neal et al., 2015; Peters et al., 2010). Similarly, community centers provide activity spaces for older people to engage in various hobbies or volunteer activities, promoting healthy behavior, and facilitating social participation and interactions (Hosokawa et al., 2019). Finally, older people are frequent users of public libraries in Hong Kong (Leisure & Cultural Services Department, 2015). The universal design with barrier-free facilities in Hong Kong public libraries ensures older people easy access (Leisure & Cultural Services Department, 2022), which creates opportunities for them to interact with others and offers opportunities for intergenerational activity (Institute of Museum and Library Services, 2012). As a result, the built environments which promote positive social interactions could be associated with lower ageism (Zhong et al., 2022).
Secondly, the stereotype embodiment theory proposes that individuals internalize ageism by repeatedly being exposed to negative stereotypes of older people in their life course (Levy, 2009). These stereotypes could be reinforced by the negative presentation of older people in daily life (Donlon et al., 2005). Previous research has confirmed that negative representation of older people generates a poor impression of older people and increases ageism (Gekoski & Knox, 1990), whereas positively presenting older people can lower ageism (Marques et al., 2020).
People may be exposed to different environmental features that promote negative aging stereotypes in their community. For example, nursing homes were perceived as a place of abandonment and a stop before death (Gamliel, 2000; Villeneuve et al., 2022). Furthermore, nursing home residents are often portrayed as frail, dependent, desperate, and lonely (Villeneuve et al., 2022). Similarly, clinics and geriatric wards represent the ill and sickness in aging. Thus, it is plausible that individuals who have continuous exposure to these built environments may develop a higher level of ageism (Davidovic et al., 2007).
Based on the intergroup group contact theory and the stereotype embodiment theory, we hypothesize that older people’s ageism against their own age group is negatively associated with the number of public facilities that enhances social interactions. Therefore, parks, libraries, and community centers, which allow interactions, would associate with lower ageism. We further hypothesize that ageism is positively associated with the number of clinics and nursing homes, which present older people as frail, weak, and dependent (Figure 1). Theoretical model and hypotheses of this study. Note: H: Hypothesis; (+): positive relationship; (−): negative relationship.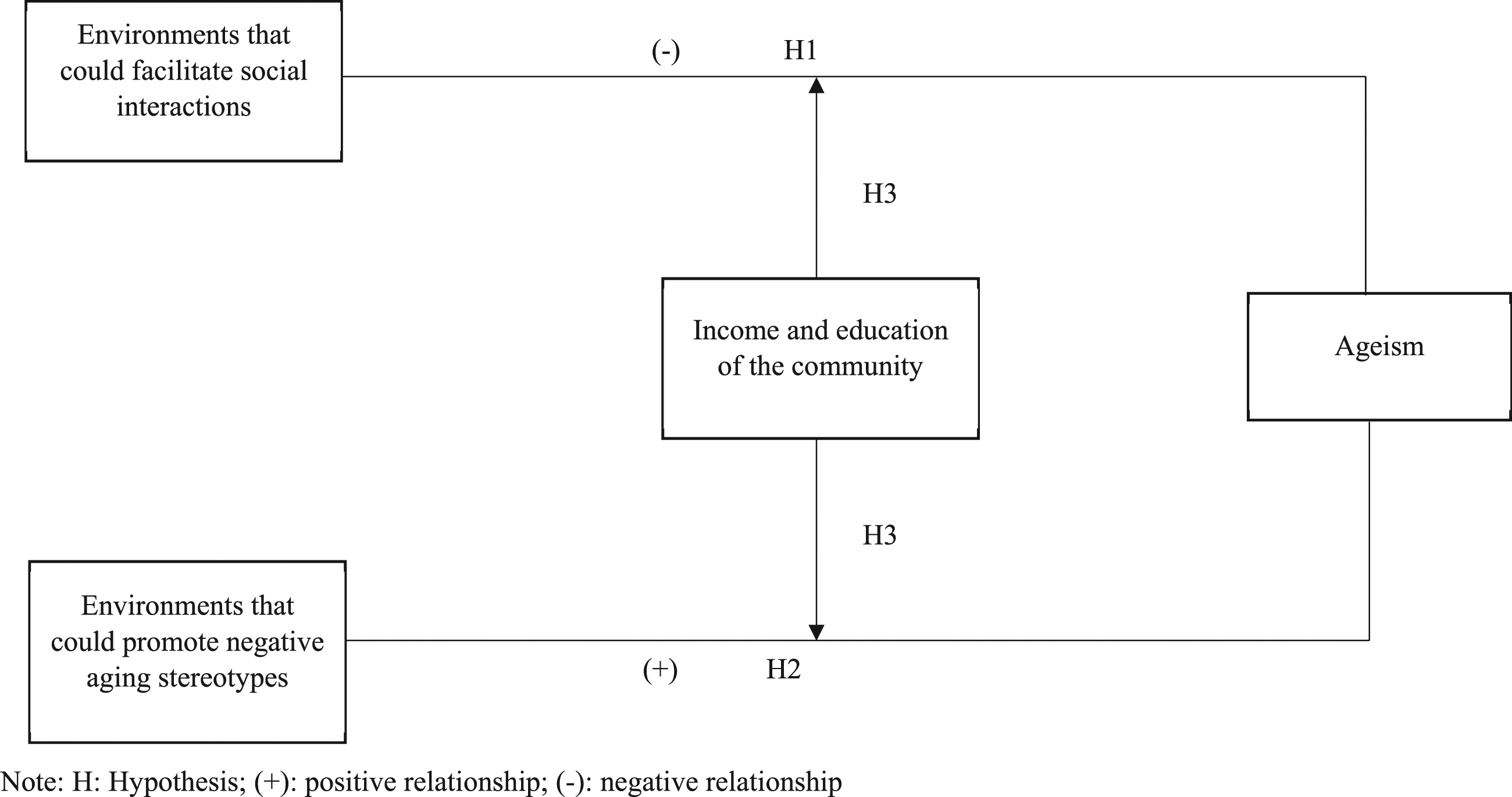
Finally, different socioeconomic status (SES) groups might have different interaction patterns with the environment and be affected differently by environmental attributes. For example, some studies show that lower SES groups may rely more on their immediate environment because they tend to travel across a smaller area, walk shorter distances for recreation, and visit fewer activity places than people with higher income (Tao et al., 2020). More importantly, a small but growing number of studies have found that the SES of a community is associated with ageism. For example, Marques et al. (2020) found that communities with more available economic resources recorded lower levels of ageism among their residents. In addition, despite no existing research on the impact of community-level education on ageism, the strong linkage between an individual’s education and ageism (e.g., Chopik & Giasson, 2017; Maurya et al., 2022) may hint at the potential association between community-level education and ageism. As a result, the impact of the community’s SES (e.g., income and education) on ageism warrants further examination.
To fulfill the knowledge gaps mentioned above, the objectives of this study were to examine: (1) the association between the objectively measured built environment features and ageism among community-dwelling older people; and (2) variations in such associations between neighborhoods with different levels of income or education.
The Study Site: Hong Kong, China
Hong Kong is a Chinese city with high levels of economic development, urbanization, and population density. In 2021, 20% of its population were 65 years or older and the figure will increase to about 33% by 2039 (Census and Statistics Department, 2020; 2022b). Although many believe that Hong Kong people share the traditional filial culture that respects older people and have a more positive attitude toward them, studies found otherwise (Lou & Dai, 2017). In fact, a recent study found higher ageism in Hong Kong than in other Western countries (Löckenhoff et al., 2015). With this context, Hong Kong provides a suitable place to understand ageism in rapidly developing Asian cities.
Research Design and Methods
Study Design and Respondents
This cross-sectional study comprised 1333 people aged 60 years and above recruited by purposive and snowball sampling. We recruited participants from 44 centers for older people in three districts of Hong Kong. These centers are funded by the Government and provide healthy aging and leisure activities to older residents in the district (Social Welfare Department, 2022). Although membership is open to all district residents, most members were from the lower to middle socioeconomic classes. We therefore supplemented the sample by snowball sampling to increase the number of participants from upper middle socioeconomic status. The snowball participants came from volunteers in aging programs of the center-on-aging of the university. We successfully recruited a minimum of 400 participants in each district. Most older people were members of multiple centers, and we were not able to associate them with a specific center. Therefore, we did not use center characteristics as control variables in our multivariate analysis.
The inclusion criteria were (1) people aged 60 or above; and (2) able to understand and communicate in Cantonese. Domestic helpers or individuals with a medical history of dementia diagnosed by medical professionals were excluded. Domestic workers were excluded as they were not permanent residents of Hong Kong. People with a diagnosis of dementia by a medical professional were excluded because of their memory challenge as we asked participants to answer survey questions retrospectively. Data were collected via self-administered questionnaires with the assistance of trained research assistants. Face-to-face interviews using the same questionnaire were conducted with respondents who were illiterate. Participants had given informed written consent before the interview began. A total of 55 (4.0%) people were excluded from the statistical analysis because of missing data. The final sample comprised 1278 individuals. The study was approved by the Human Research Ethics Committee of The University of Hong Kong [Reference Number: EA1510033].
Dependent Variable—Ageism
Our study focused on older people’s ageism against their age group (intra-generation ageism) and we used the short version of Kogan’s Attitudes towards Older People Scale (KAOP) to measure it (Kogan, 1961b). KAOP has been used in various ageism studies to assess older people’s ageism against their own age group (e.g., Kogan, 1961a; Salguero et al., 2019).
The original KAOP has 34-items consisting of 17 matched pairs. Each pair has one negatively phased statement (KAOP-) and one positively phased statement (KAOP+) on older people (see Kogan, 1961b). Respondents are asked to rate their agreement with the statement using a six-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). To obtain the total score, the 17 KAOP-items are reverse coded and summed with the KAOP + score. The possible scores range from 34 to 204, and a higher score indicates a more positive attitude toward older people (i.e., a lower level of ageism) (Kogan, 1961b). The scale has been validated in a Chinese population (Yen et al., 2009a). The short version of KAOP used in this study included 10 items selected from the original KAOP based on a factor analysis conducted by a team with another larger dataset (Sun et al., 2019). Cronbach’s alpha of the short-version scale was 0.80 in this dataset, demonstrating good reliability. The first nine negative items were reverse coded, and the score of these 10 items was summed to generate the total scores. The possible score ranged from 10 to 60, with a higher total score indicating a lower level of ageism.
Independent Variable—Neighborhood-Built Environment
The neighborhood-built environment variables included the number of (1) community centers, (2) libraries, (3) parks, (4) nursing homes, and (5) clinics within the 200-meter buffer area of the respondent’s residential address. They were selected because they could facilitate social interactions (from the intergroup group contact theory) or promote negative aging stereotypes in the community (the stereotype embodiment theory). Although public transportation affects older people’s well-being and opportunity for social interaction (Van Hoof et al., 2020), we did not include it in our study as all districts were served by extensive public transportation services and older people enjoy a significantly discount on bus ($0.25 US dollar per trip) and on subway (half priced) services in Hong Kong.
Each respondent’s residential address was geocoded to latitude and longitude automatically using Map Location (https://maplocation.sjfkai.com/). We used Google Map to geocode the addresses manually should the address could not be geocoded automatically using Map Location. The neighborhood-built environment was assessed within a 200-meter road network and slope-adjusted buffer area of the respondent’s residential address to ensure maximum closeness to reality, thus significantly improving the precision of objective measurement. The 200-meter buffer area was chosen to capture the neighborhood-built environment within a five-minute walk of older people’s residences (Gehl, 2010). The 2014 GeoReference Database (scale 1:1000) (including the road network data), the 2014 digital topographic data (Scale 1:1000) (showing the topography of terrain), and the 2014 GeoCommunity Database (including exact location points of various types of facilities) provided by the Hong Kong Government’s Lands Department were used to create the objective measures. ArcGIS version 10.7.1 was used for processing the geographical data.
Covariates
Control variables included age (years), gender (male and female), education (no education, primary school, junior high school, senior high school, and post-secondary education), individual monthly income (HKD <$2000, $2000-3,999, $4000-5,999, $6000-$7,999, $8000-$9,999, and ≥$10,000) 1 , physical health, mental health, and percentage of older people in the sub-district. Physical health and mental health were measured by the Physical Component Summary (PCS) and Mental Component Summary (MCS) scale of the 12-item Short-form Health Survey (SF-12). The SF-12 is a shortened version of the 36-item Short-form Health Survey (SF-36). It extracted 12 questions from the SF-36 with the same eight domains in physical health (i.e., physical functioning, role-physical, bodily pain, and general health) and mental health (i.e., vitality, social functioning, role-emotional, and mental health) (Ware et al., 1996). Twelve items were weighted separately and summated to generate the standardized PCS-12 and MCS-12 scores (Ware et al., 1996). The norm-based standardized PCS and MCS score were used in this study, in which higher scores indicated better physical and mental health. The SF-12 has been validated in a Chinese population (Lam et al., 2005). The percentage of older people in the sub-district was retrieved from the district profiles generated by the Hong Kong Census Department based on the Hong Kong Population By-census 2016 (https://www.bycensus2016.gov.hk/en/bc-dp.html).
Statistical Analysis
Firstly, we divided each sub-district based on whether their average income/education level was higher or lower than the district median income/educational level (from 74 sub-districts in this study). The division of the sub-district allowed us to test the potential moderation effect of district-level socioeconomic status on the association between environmental variables and ageism. The district and sub-district median incomes and educational levels were obtained from the Census and Statistics Department of the Government (Census and Statistics Department, 2017).
Secondly, we reported sample characteristics and examined the differences between groups using chi-square and t-test. Moreover, we used the intra-class correlation coefficient (ICC) to test the clustering effect between different sub-districts. The result of ICC was close to zero (<0.001), indicating that no significant clustering effect was found among sub-districts. Therefore, we used multivariable linear regression modeling to examine the association of our environmental variables with ageism after controlling for the covariates (including individuals’ income and education). The variance inflation factor (VIF) ranged from 1.04 to 1.62, and all were lower than 10, indicating that multicollinearity was not a concern (Hair et al., 1995). Finally, we repeated the main regression in each subgroup of income and education to identify the moderation effect of district-level income and education on the association between environmental variables and ageism. Statistical analysis was undertaken using SPSS 26.
Results
Respondents’ Characteristics by Sub-District Income and Education Levels.
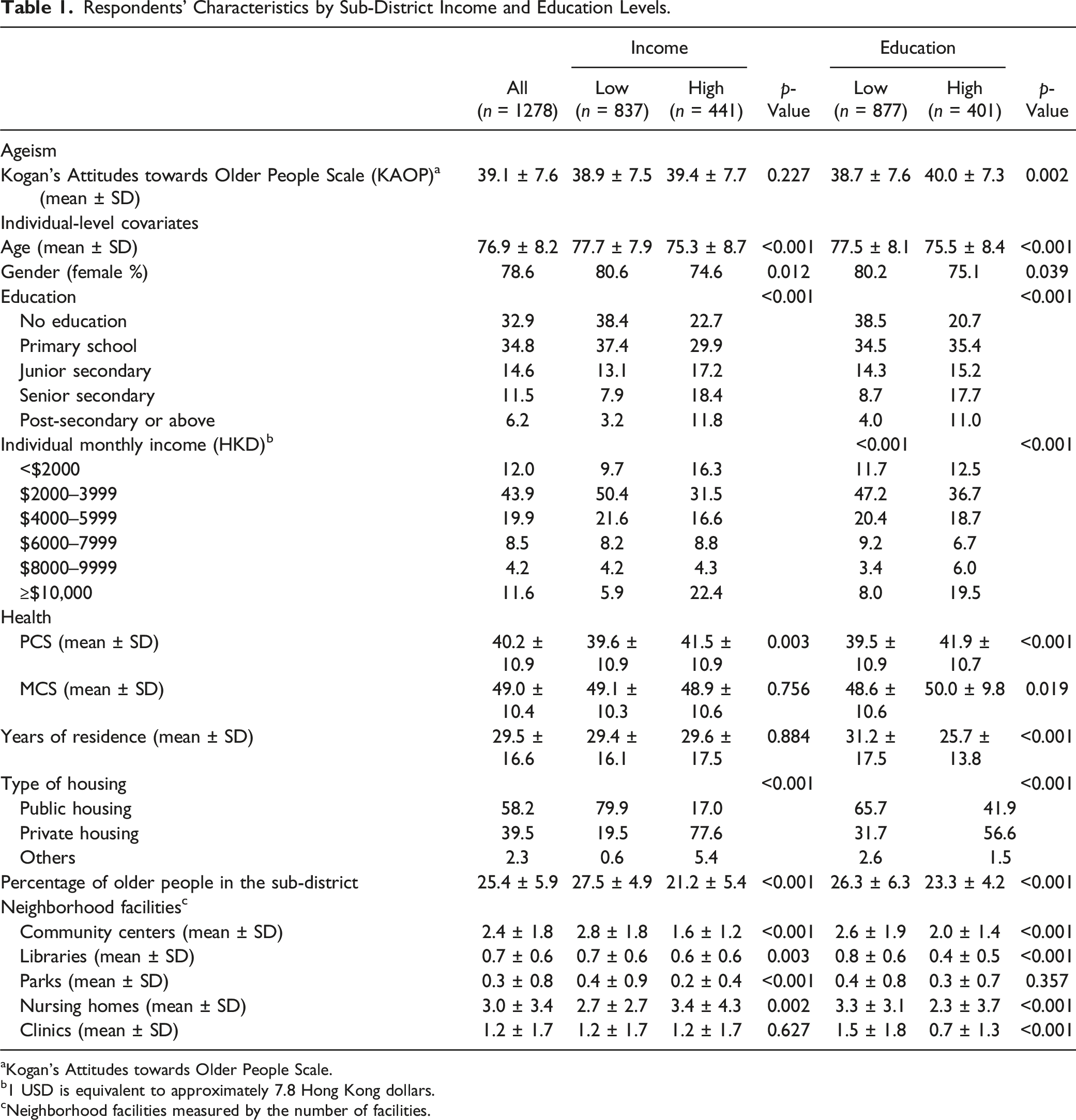
aKogan’s Attitudes towards Older People Scale.
b1 USD is equivalent to approximately 7.8 Hong Kong dollars.
cNeighborhood facilities measured by the number of facilities.
Table 1 also shows the characteristic of people living in areas with different incomes and education. People living in low-income or low-education areas were older, more likely female, and had poorer physical health than those in high-income or high-education areas. Regarding the built environment in the area, low-income or education areas had more community centers and libraries. However, low-income areas had more parks, and low-education areas had more nursing homes and clinics. The Hong Kong Government used a population-based planning ratio to decide the number of public facilities, such as public libraries and parks, in each district (Department Planning, 2022). Since low-income districts have a higher concentration of public housing and, therefore, higher population density (Census and Statistics Department, 2022a), they end up having higher numbers of libraries and parks.
Unstandardized Regression Coefficients (β) and 95% Confidence Intervals (CI) for Ageist Attitude in Old Age by Sub-District Income and Education Levels.
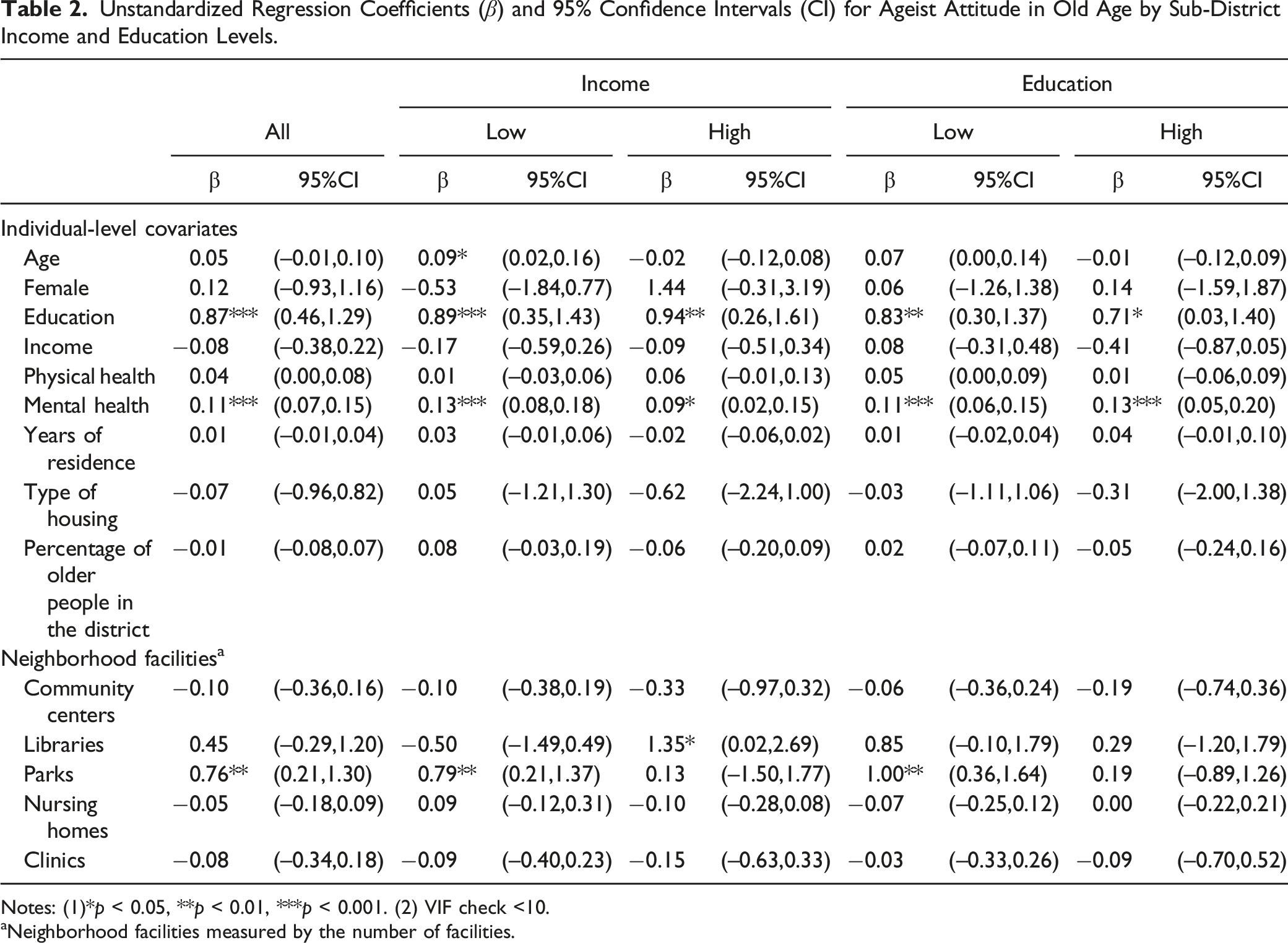
Notes: (1)*p < 0.05, **p < 0.01, ***p < 0.001. (2) VIF check <10.
aNeighborhood facilities measured by the number of facilities.
A different association was found when dividing the sub-districts into two income groups. Older people with higher educational levels and better mental health were associated with a lower level of ageism in both districts, similar to the overall model. However, older people (β = 0.09, p < 0.05) were associated with a lower level of ageism in the low-income area only. Two neighborhood-built environments, which facilitate social interactions, were associated with ageism. We found that a greater number of parks (β = 0.79, p < 0.01) in the low-income area was associated with a lower level of ageism but not in the high-income area. A greater number of libraries (β = 1.35, p < 0.05) in the high-income area were associated with a lower level of ageism. No significant association was found between ageism and the neighborhood-built environments that promote negative aging stereotypes.
Sub-districts with different education levels had similar results to the overall model. Better education and mental health were associated with a lower level of ageism in low- and high-education areas. Regarding the neighborhood-built environments that promote social interactions, only a greater number of parks was associated with a lower level of ageism (β = 1.00, p < 0.01) in the low-education area. No significant association was found between neighborhood environment and ageism in the high-education area.
Discussion and Implications
This study provided empirical evidence on the association between the built environment and ageism. Concerning the neighborhood-built environments, which could facilitate social interactions, a greater number of parks was associated with a lower level of ageism in the overall model and in low-income and low-education areas. A greater number of libraries was associated with a lower level of ageism among older people in the high-income area after controlling for individual-level covariates. However, no significant association was found between ageism and the neighborhood-built environments that promote negative aging stereotypes in all models. Higher education and better mental health were consistent individual factors, which were found to be associated with a lower level of ageism. Several additional insights can be generated from this study.
This study sheds light on the importance of the built environment in association with ageism. The availability of parks and libraries in the community was associated with a lower level of ageism. This association could be explained by enhancing intergroup contact. Parks and libraries provide a platform to facilitate positive social interaction among people (Peters et al., 2010). As posited by intergroup contact theory, increased interaction may enhance mutual understanding, empathy, perspective-taking, and knowledge between groups (Pettigrew et al., 2011). Even though older people have sufficient knowledge of aging, intergroup contact with other older people may reduce ageism.
A greater number of parks was significantly associated with a lower level of ageism, an impact that remained significant in low-income and low-education areas. Parks may be particularly important for less affluent older people who are highly reliant on their neighborhood living environment (Tao et al., 2020) and less educated older people who exhibit disproportionately less social participation (Minhat & Mohd Amin, 2012). However, a significant association between ageism and libraries was found only in the high-income area. Different library usage habits among people with different household incomes may explain this result (Sin & Kim, 2008). People with higher median household incomes have higher library usage (Meyer, 2018). Therefore, the availability of a library may exert more impact on people with higher median household incomes. However, such an association warrants further investigation.
Contrary to our second hypothesis, environments that may intensify negative aging stereotypes (e.g., nursing homes and clinics) were not associated with ageism. This may be because existing studies on aging stereotypes were conducted in the laboratory setting (e.g., Gekoski & Knox, 1990). The stimulant in our living environment that promote aging stereotypes may be insufficient to influence people’s ageism. Therefore, further research on stereotypes in the community setting is warranted to enhance our understanding.
This study has several limitations. First, most respondents were recruited from centers for older people, which could limit the generalizability of the findings to older people who are less active and are not members of centers for older people. Moreover, the centers’ level characteristic was not considered in our model, so we may overlook the impact of the centers on our model.
Second, we used 200 m buffer area GIS data, preventing us from generalizing our findings to a larger buffer area. Although a 200m buffer is an appropriate area to capture an older adult’s daily life because older people rely more on their immediate community environment (Lu et al., 2021), there is some variation across cultures regarding walking distance and the walking behavior of older adults. Such factors may affect the utilization of public facilities and may influence the study results.
Moreover, due to the cross-sectional nature of this study, a causal relationship between the built environment and ageism cannot be established. Therefore, future research could address these limitations by adopting longitudinal designs with a larger buffer area and recruiting older people from diverse sources in the community.
Finally, we separately tested the moderation effect of community-level income and education on the association between the built environment and ageism. Future research may incorporate different SES components (e.g., income, education, age) of a community into a community SES index to reflect the community SES as a whole.
Despite these limitations, this study is one of the few which provides empirical evidence on the neighborhood-built environment attributes and ageism among older people. Our results ascertain that the built environment is one of the determinants of ageism, which has been overlooked in previous studies. This finding enhances our understanding of ageism and indicates the need for future research to investigate further the relationship and interaction between individual-level, social environment, and the built environment determinants of ageism. Policymakers and urban planners could also incorporate these findings in future city planning to combat ageism in practice by providing more parks and libraries to promote positive interaction between community residents.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hong Kong Jockey Club Charities Trust under grant number 2017-0032-002.
Ethical approval
The study was approved by the Human Research Ethics Committee of The University of Hong Kong [Reference Number: EA1510033].