
Abstract
COVID-19 regulations have posed challenges for long-term care (LTC). However, few studies have examined how such regulations influenced the care of residents living with dementia. Our objective was to gain an understanding of LTC administrative leaders’ perceptions regarding the impact of the COVID-19 response on this population. Using the convoys of care framework, we conducted a qualitative descriptive study. Forty-three participants, representing 60 LTC facilities, completed one interview where they described how COVID-19 policies shaped care for residents living with dementia. Results from deductive thematic analysis revealed that participants believed the care convoys of residents living with dementia were strained. Participants emphasized how diminished family involvement, increased staff responsibilities, and the industry’s heightened regulatory climate contributed to disrupted care. Further, they highlighted how pandemic-focused safety guidelines did not always consider the unique needs of those living with dementia. Consequently, this study may inform policy by outlining considerations for future emergencies.
• Support for the convoys of care framework • Insight about how policies impact the care of residents living with dementia in LTC
• Policymakers may draw from the study’s findings when drafting LTC regulations for future emergencies • Educates regulators and practitioners about care strategies that support residents living with dementia during emergenciesWhat this paper adds
Applications of study findings
Introduction
COVID-19 has had a devastating impact on the health of residents in long-term care (LTC) (Vipperman et al., 2021), to include nursing homes (NH), assisted living communities (ALC), and family care homes (FCH) where providers reside with a small number of residents and provide direct care. There are 15,600 NH and 28,900 ALC in the U.S. serving approximately 1.3 million and 810,000 residents (National Center for Health Statistics, 2019). The risks of hospitalization and mortality for these residents are elevated because of their medical conditions, the transmissibility of the virus, and the congregate nature of LTC (Thomas et al., 2021).
Federal and state governments limited visitation from individuals considered to be nonessential early in the pandemic (Chen et al., 2020). Although this response aimed to minimize exposure, scholars warned of the risks of isolating LTC residents from family and friends given the support they provide (Kemp, 2021). Families play a particularly important role for residents living with dementia, highlighting the need to include dementia in studies examining responses to the pandemic (Curelaru et al., 2021).
Approximately 48% of NH and 42% of ALC residents have been diagnosed with dementia (Harris-Kojetin et al., 2019; Sengupta & Caffrey, 2020). Although several studies (e.g., Thomas et al., 2021) have examined the clinical effects of COVID-19 on LTC residents, data are more limited concerning the effect of restrictions in the U.S. that limited residents’ social contact. Nash and colleagues (2021) found high levels of frustration and anxiety among families who perceived declines in their loved ones and poor care delivery in LTC. International studies describe similar LTC visitation restrictions and the negative effects it had on residents living with dementia, as reported by family members and residents (Avidor & Ayalon, 2021; Giebel et al., 2022; Ickert et al., 2021) and staff (Giebel et al., 2022; Leontjevas et al., 2021; Smaling et al., 2022).
The present study adds to this literature in its use of the convoys of care model (Kemp et al., 2013) to investigate the effect of the COVID-19 pandemic and related policies on residents living with dementia at the individual/interpersonal, facility, and industry levels. The well-known model (Figure 1), adapted from Kemp and colleagues (2013) appears below. Convoys of Care Model.
The convoys of care model extends Kahn and Antonucci’s (1980) convoy model of social relations, which proposes that individuals exist within evolving networks through which they give and/or receive support. It addresses the intersection of formal and informal care and how the interplay of the varied relationships affects caregiver and care recipient outcomes (Kemp et al., 2013).
The purpose of our study was to explore LTC administrative leaders’ perceptions of whether and how the pandemic and the associated response, impacted the care convoys of residents living with dementia. Administrative leaders were selected due to their broad view of care convoys (i.e., individual/interpersonal, facility, industry). We used this framework to interpret our qualitative findings, with the overall goal of gaining knowledge to inform public policy concerning the range of individuals who play critical roles in care delivery in LTC.
Methods
We chose a qualitative descriptive approach because we aimed to better understand LTC administrative leaders’ perceptions of whether and how COVID-19 policies impacted the care convoys of residents living with dementia. Qualitative descriptive studies are ideal for exploring the “who, what, and where of events or experiences” (Kim et al., 2017, p. 2). Our research team consisted of three doctoral level researchers with expertise in qualitative methods and one doctoral candidate. The study was approved by our Institutional Review Board (STUDY001803_MOD000003).
Sampling and Recruitment
Participants were recruited through an online survey generated via Qualtrics and distributed to LTC facilities in Florida from October 2020 to March 2021. Respondents who expressed interest in providing further details about their experiences throughout the pandemic in a focus group or interview and provided their contact information were sent an email for scheduling and a copy of the interview guide. We used a purposive sampling maximum variation approach to ensure that participants represented different types of facilities in varied regions across Florida (Sandelowski, 1995).
Interviews
Participants completed one interview between April and November 2021, providing verbal informed consent beforehand. We originally intended to conduct focus groups but determined after conducting one focus group that individual interviews would give participants more time to discuss their unique experiences. Interviews lasted approximately 60 minutes and were conducted via Zoom or telephone, based on preference. Interviews were audio recorded with permission and professionally transcribed verbatim. Pseudonyms were used to protect participants’ identities.
We asked a series of questions centered on participants’ experiences throughout the pandemic, focusing on their perceptions regarding how residents living with dementia and their care convoys were impacted by pandemic policies. Questions included: can you discuss how COVID-19 has affected residents living with dementia? What have you done to encourage/facilitate resident communication with family?; and how have you managed resident and staff contact within your facility? Participants also had the opportunity to share additional details or schedule a subsequent interview. Additionally, they received a $75 Amazon gift card as a token of appreciation. After each interview, our team met to discuss takeaways and to refine our questions.
Analysis
We uploaded the transcripts to ATLAS.ti 9. We utilized a thematic analysis approach to discern patterns in participants’ responses (Nowell et al., 2017) along with a deductive coding approach wherein our codes were drawn from concepts in our interview guide (Azungah, 2018). As a first analytic step, following the creation of our a priori codebook, one member of our team carefully read through one transcript to look for additional codes. Based on their reading, they revised the codebook and shared it with the team to ensure its clarity and prompt the analysis. Next, each team member independently coded the same five interview transcripts, reading the data line by line and assigning the appropriate codes. Following, we met to read through the transcripts line by line, talk about the codes we independently applied for each line of data, discuss interpretive differences to reach team consensus, and reconcile codes. As new ideas emerged, we refined the codebook and recoded previously coded transcripts. For example, one initial code was called “communication.” However, we refined this code to distinguish communication between different groups of people (e.g., families, staff).
We coded in pairs for the next 20 transcripts, with each member of these two-member teams independently coding their assigned transcripts and meeting to discuss their interpretations of the data. Modifications were shared with the full team to ensure everyone was using the same codebook and to signal the recoding of previously coded transcripts. The remaining 18 transcripts were divided among team members to be independently coded. Our team continued to meet throughout this process to discuss the codes we applied. No new codes emerged during the single coder process.
Once all data were coded, we utilized the code frequency and code co-occurrence tools in ATLAS.ti 9 to examine which codes routinely appeared in the data and more importantly, how the codes overlapped to form overarching ideas that spoke to the levels (e.g., individual/interpersonal) in the convoys of care model (Kemp et al., 2013). Using these outputs and the model as a guide, we pinpointed the ideas that transcended the individual codes and gave meaning to participants’ shared experiences.
Trustworthiness
We engaged in numerous activities to ensure rigor and trustworthiness. First, we utilized team and paired coding processes which ensured our codebook was accurate and understood by each member of our team. Second, we wrote memo notes to document our reflections of the data, modify our codebook, and refine our themes (Richards & Morse, 2002). Last, we actively looked for disconfirming evidence to confirm that our findings reflected participants’ perceptions (Booth et al., 2013).
Results
Participant and Facility Characteristics
Nursing Home and Assisted Living Community Characteristics (N= 59).
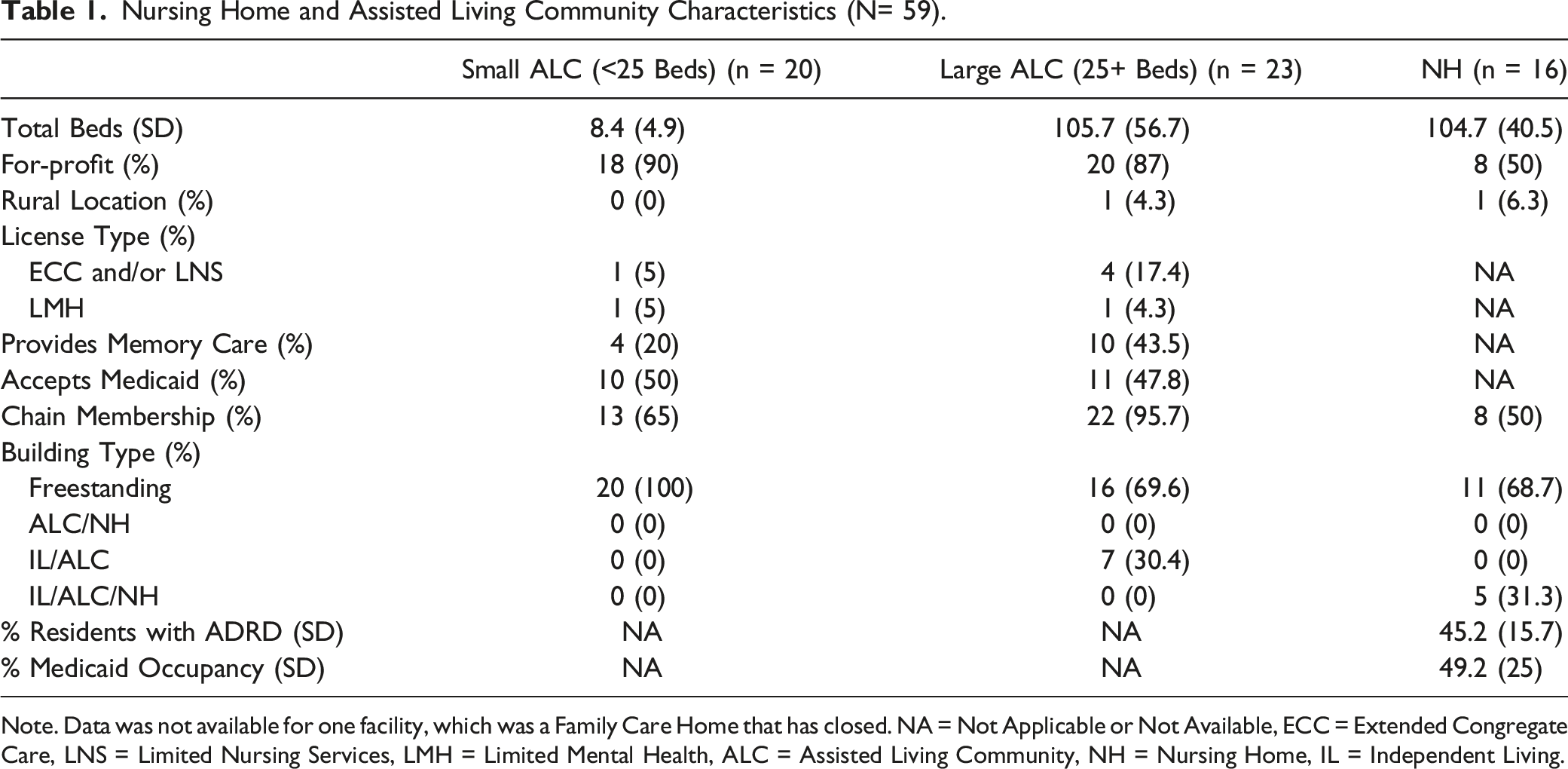
Note. Data was not available for one facility, which was a Family Care Home that has closed. NA = Not Applicable or Not Available, ECC = Extended Congregate Care, LNS = Limited Nursing Services, LMH = Limited Mental Health, ALC = Assisted Living Community, NH = Nursing Home, IL = Independent Living.
Theme and Subthemes
“It Was a Struggle to Make It As Home Like As Possible, but Also Try to Keep Them Safe”
The overarching theme of our study concerned participants’ perceptions of how care convoys for LTC residents living with dementia were challenged by pandemic policies. This theme, addressing the difficult balance between mitigating risk and maintaining residents’ quality of life, manifested into three distinct subthemes that mapped onto the individual/interpersonal, facility, and industry levels of the convoys of care model (Kemp et al., 2013). These subthemes illuminated how decreased family involvement, increased staff responsibilities of staff, and the heightened LTC regulatory climate disrupted care convoys for persons living with dementia.
Individual/Interpersonal Level: “There’s No Substitute for Family”
This subtheme explores participants’ attitudes about the impact of reduced family visitation on the care convoys of residents living with dementia. Further, it addresses participants’ perceptions regarding the helpfulness of visitation innovations (e.g., video technology, window visits).
Participants emphasized the challenge of managing family visitation guidelines. Though most reported having minimal conflict with families, they perceived that residents living with dementia were severely affected by reduced contact with family. Summer (ALC) reported that her residents were devastated by the isolation they experienced. She said, “They weren’t having the interaction with the family. [They were not] able to get that physical hug and that hand touch. You could see the severe decline.” Her statement highlights how crucial socioemotional support is for residents living with dementia, arguing that the lack of such support and physical touch is detrimental for this population.
Iris (ALC) also described how the mental health of her residents worsened due to decreased family involvement, though with a much more dire consequence. She remarked: I'm a firm believer, we did more damage isolating residents than we did keeping them from COVID. So, all of it, not being able to see family, not being touched, the fear, all of that, did tremendous damage to their mental health. And I truly believe it killed quite a few of our residents because the depression was so severe, that they just completely lost hope, especially as it just continued on and on and on.
Several participants also spoke about the duration of the visitor restrictions and the strain this placed on residents and their families. The loss of precious time together was particularly troubling. Some participants explained that this resulted in increased agitation and anxiety among residents. Darlene (NH) recalled an interaction she witnessed between a resident and her spouse. She said, “She got to the window and saw her husband and was mad. And [she] was like, ‘Why haven’t you come to see me? Where have you been? What were you doing?’." She explained that even though this resident was living with dementia, she deeply felt his absence.
Other participants talked about the impact of the pandemic’s duration on family members. Felicia (NH) reported, “Sadly, a lot of our residents forgot who their loved ones were.” She went on to discuss the grief this caused families. She perceived that the long separation uniquely impacted persons living with dementia and their families because it appeared to exacerbate the progression of the disease. Visitation restrictions prevented families from observing the changes that took place in their loved ones as closely as they could before the pandemic.
Participants also discussed innovations which were used as alternatives to visitation (e.g., window visits). Though participants acknowledged a certain level of success in using these methods for residents living without cognitive impairment, they believed that they posed many challenges for residents living with dementia. Derek (NH) said, “… it was very difficult for dementia residents to understand what a Zoom phone call and seeing a family member was. I’m not sure it helped as much as we thought it was going to help.” He explained that although he hoped that video technology would mitigate loneliness, it proved to be an unfeasible solution for this population. Evelyn (NH) provided additional insight on why video technology failed, saying, “Even to see them on a computer monitor was not enough, especially if they had poor eyesight. How do they know that’s their daughter? Their speech is not as clear on electronic devices as it is in person.” Her comment implies that the technology’s shortcomings extended beyond residents’ cognitive abilities. She perceived that the video technology’s design did not meet the needs of those with visual or auditory limitations.
Participants explained that window visits were facilitated with mixed success. Isabel (ALC) said, “The window visits were helpful, but they had to be continually reminded why they couldn’t come in and give them a hug or sit by their side, that we were trying to protect everybody, make sure nobody gets sick.” Her reflection suggests that while window visits enabled families to see their loved ones, they prevented residents from interacting in their preferred way—being physically near and comforted by their relative. Further, she noted that not being able to touch their family members confused the residents living with dementia. Similarly, William (ALC) reported: Not having interaction that they needed, that one-on-one, close-up, hand-to-hand, talking to them. That was tough. Trying to talk to them through a glass didn't go over well with many of them. There were a couple banging on the glass looking out, and they just didn't understand. They seemed to be confused about what that meant...They needed some contact with family members or loved ones, just to kind of hold on to some level of reality.
Similar to others, William perceived that window visits were helpful for family members who longed to see how their loved ones were doing but seemed to be damaging for residents living with dementia. As he observed, their pain from being separated manifested in physical outbursts that seemed to suggest that “There’s no substitute for family.”
Facility Level: “It’s Been More on the Caregiver”
This subtheme speaks to the increased demands placed on formal caregivers and staff during the pandemic and how the care convoys of residents living with dementia were affected by these changes. Participants also shared how residents responded to staff during this time.
Multiple participants addressed how and why relationships between their staff and residents changed during the pandemic. Participants suggested that a residents’ ability to understand COVID-19 and how to keep themselves safe contributed to their care delivery. Participants commented that while the residents had personal protective equipment (PPE) available to them, the residents struggled to recognize what purpose it served. Celeste (ALC) shared: Yeah, so really, I don't think they understand the whole thing of it. They don't understand what to do with their mask. I've got some gentlemen that used it as a slingshot. They wear the mask on their heads, on their ears, on their elbows. They have various uses for the mask. They really don't understand why they have to wear them.
Nearly all participants noted that their staff had to take on additional roles to ensure adherence to safety precautions throughout the pandemic. Fara (NH) recalled a conversation with her staff where she said, “It doesn’t matter what department you work in. If you see a member who isn’t able to follow infection control practices and they’re supposed to, gently remind them...It just takes a village.” In her statement, she addressed the need to reorient her staff toward a shared mission. Whereas before, staff members could focus on their own job duties, the pandemic shifted facility operations as well as her expectations. Participants remarked that during the pandemic, everyone, regardless of their position or training, became accountable for maintaining residents’ health and safety through efforts to prevent the virus’ spread. Beyond reminding residents about safety guidelines, staff were also tasked with disinfecting areas, rearranging furniture, and monitoring social distancing.
In addition to staff having to wear multiple hats, participants also described how they had to overcompensate for residents’ lack of understanding and adherence to pandemic procedures. Hazel (NH) said, “We had such strict protocols in place because they could not wear their masks and we could not keep them in their rooms. So, full PPE on the staff as far as N-95s, eye goggles, gowns, gloves.” Although the PPE precautions were designed to keep residents safe, and staff readily complied, participants discussed how the PPE interfered with staff members’ interactions and rapport with the residents living with dementia. For example, Kristen (ALC) observed that the PPE impeded interactions between her residents and her staff. She stated, “[they] rely a lot on body language. And so, it was really difficult. A lot of times we would just have to stand back… pull our mask down so that they could understand.” Kristen’s observation reveals that while the PPE was intended to be a barrier to prevent the spread of COVID-19, it also became a barrier to interacting with residents, requiring staff to break protocol so residents could understand what they were telling them.
Several participants perceived that residents living with dementia responded negatively to staff wearing PPE, with many feeling that residents became fearful. Ethan (NH) explained, “How scary is it for a dementia resident to see everybody in mask in such a clinical, cold environment? I think it’s very alarming to these residents.” His comment alludes to the culture change facilities experienced as a result of COVID-19, whereby they steered from a social model of health toward a more medical model of care. As he noted, the residents living with dementia not only noticed the changes that took place but may have been disturbed by them. Oliver (ALC) also spoke of these challenges, saying: So, I'm sure it was very traumatic at times. We couldn't necessarily explain fully to them what it was about because of their cognitive ability. All we could do was reassure. At the time, obviously touch was very limited because of the safeguards in place, in terms of COVID-19. But a gentle hand on the shoulder, making sure that you were smiling so that there wasn't a panic. But with masks, obviously smiling, they can't necessarily see that, so touch was very important. Touch and reassurance, and soft language to try and help them through the process.
Oliver’s statement underscores staff members’ efforts to maintain the safety of residents living with dementia throughout the pandemic. As the residents grappled with the new normal, staff were charged with finding multiple ways to alleviate residents’ fears. His comment concerning the staff exemplifies the opinion of many that the care dynamics shifted during the pandemic such that “It’s been more on the caregiver.”
Industry Level: “This Guidance Has Got to Change”
This subtheme reflects participants’ perspectives about how the guidance on managing COVID-19 affected care delivery. It further reflects the perceived dissonance between participants’ views and the policies of regulating bodies (e.g., CMS, Department of Health).
Although residents living without cognitive impairment were typically quick to follow protocols, residents living with dementia were not. As Noel (ALC) explained, this gap in adherence made it difficult to consistently follow mandated safety guidelines.
We had to step into their world of reality, and we could not create combative situations. We obviously tried to encourage, but if they took the mask off, we couldn’t make a big deal out of it. That’s why we control the narrative of who was there, how many people, and how far apart they were. Because you can’t do that. There’s just no way. They don’t comprehend to do that.
Her statement stresses the importance of meeting residents where they are. She talked about creating an environment where residents felt comfortable and not threatened, rather than focusing on their limitations.
However, this approach often conflicted with the expectations of government officials, causing many participants to feel unsupported and frustrated. Owen (NH) recalled an interaction with a local health department official. He said, “[they] questioned why we weren’t requiring them to wear face masks. And I’m like, we are requiring them to wear it, but you try to keep demented residents with their face masks on...sometimes we catch them and sometimes we don’t!” His experience speaks to a core element of this subtheme, the discourse between participants and regulators regarding what is pragmatic. Each party had separate assumptions about what could be reasonably expected of staff and residents. Similar to Noel, Owen acknowledged the importance of the pandemic protocols, however, he accepted that residents living with dementia were not always able to comply. However, the regulators did not appear to share his beliefs and seemed to expect that all residents, regardless of ability, adhere to the rules. Participants appeared to be particularly irritated by interactions that highlighted regulators’ lack of knowledge about the unique behaviors and needs of persons living with dementia.
Participants also reported differing with regulators in their philosophies of resident care. Most participants described viewing their facilities as their residents’ homes. Consequently, Taylor (ALC) recalled advocating for his residents to maintain their routines and social activities. He said, “When they came in, we were still doing communal dining. A lot of people had already stopped. [Regulator] came in and said, ‘you can’t do that.’ We said, ‘it’s better for the residents.’” Taylor emphasized the important role of socialization for residents living with dementia and the risk of it being overlooked by regulators. Kara (ALC) described a similar situation where she tried to explain to regulators that because her facility is a home, her residents should not be isolated in their rooms. She stated, “I went ‘well, so when you’re at home, do you lock everybody in their bedrooms?… You wouldn’t like to be locked in your room!’” Her comment illustrates the essence of what makes a place feel like home. For her, home is a space where one can freely move about and to restrict residents is to deny them their home. While some participants negotiated with regulators, others remained fearful of potential consequences. Ellen (ALC) said: It was hard. [The residents] didn't understand why they couldn't come out. They didn't understand. And when they did come out, we were like, “Oh, here, let me take you back to your room. Let's go see what we can find.” They did not understand. But the thing is that if the state were to walk in, and I have a resident or two walking around, am I going to get cited? Am I going to get fined? It's like, nobody knew. Nobody knew what to expect.
Ellen’s experience points to the complexities and uncertainties that participants faced throughout the pandemic. Further, her comment reveals the unique concerns of small ALC that may not have had the financial ability to pay a regulatory fine and pay for basic resident care. She also highlights the role of power dynamics and the power of position, suggesting that the regulators placed her in the precarious position of being unable to care for her residents the way she preferred.
Several participants expressed that their worlds were filled with ambiguity because limited information existed about how to manage the pandemic while caring for persons living with dementia. Patricia (FCH) discussed the shortcomings of the available resources and the lack of dementia specific guidance provided. She reported, “Oh, no, not at all. Nothing towards dementia. That was just general COVID information.” Patricia’s experience highlights the importance of tailoring messages. Instead of offering a one-size-fits-all approach, she said that LTC would benefit from resources that provide strategies for successfully managing the virus while also caring for persons living with dementia.
Some participants argued that strategies for managing COVID-19 missed the mark completely. Greta (NH) communicated her dismay with the guidance provided to participants throughout the pandemic, offering a series of pointed directives to illustrate how a person living with dementia might have felt—oppressed. She said: What is so bad with COVID is our guidance was to shut down! And to “go to your room” and “shut the door” and “go to your room” and “stay in your room” and “put your mask on” and “don't come out of your room!” And for someone with dementia, it was horrible!
In her comments, she suggests that the guidance may have been developed too hurriedly. She expressed an urgent plea that echoed those of other participants who saw the pandemic response as disruptive to the care of those living with dementia, “This guidance has got to change.”
Discussion
This study explored the perceptions of LTC administrative leaders concerning the effects of COVID-19 policies on residents living with dementia. Our findings highlight the profound ways that care convoys in LTC settings were disrupted, with serious implications for residents living with dementia.
Concerning the care that families provide, most participants perceived that the visitation restrictions precipitated residents’ physical and cognitive decline. This finding supports prior research on family involvement in LTC and aligns with early-pandemic scholarship on the potentially damaging effects of such restrictions (Kemp, 2021). It additionally provides evidence of the key position of families in care convoys. What emerged distinctly from our interviews was the emotional toll that losing physical contact with family had on residents living with dementia. Similar results about residents’ anxieties emerged internationally, in the Netherlands (Smaling et al., 2022), U.K. (Giebel et al., 2022), Canada (Hindmarch et al., 2021), and Israel (Avidor & Ayalon, 2021) and stressed the importance of connections between residents and family members.
Concerning formal caregivers, we found that the absence of family from the care convoy and the difficulties of working in PPE among residents living with dementia created an enormous strain on staff. They faced increasing expectations to attend to residents’ socioemotional needs. Some participants spoke of staff becoming pseudo family members for residents whose families could not visit or were hesitant to visit after restrictions ceased, though this seemed to be the case more so with small ALC. Among participants overall, we found that the pandemic created an almost untenable situation in which residents’ personalized care needs were increasing amid increasing care provision challenges. The difficulties described highlight the need for all staff to be trained in how emergencies disrupt care convoys and create new responsibilities throughout LTC settings. This training should be dementia specific and include how to interpret residents’ expressions of fear or distress and how to manage those emotions (Alzheimer’s Association, 2021).
Throughout our interviews we heard about the challenges of following regulatory mandates that were presented as protection measures, but potentially increased residents’ risks (e.g., falling). Many participants reported receiving little help from regulatory officials in navigating these circumstances, with comments alluding to the tension that normally exists between providers and regulators. These tensions appeared to breed a defensiveness that may have inhibited discussion of operational shortcomings worsened by the pandemic. Studies from multiple countries have identified “lessons learned” in LTC from the pandemic (Martínez-Payá et al., 2022). However, gleaning lessons from LTC leaders concerning management of a pandemic or any other emergency will require greater trust and collaboration between providers and regulators. Some providers openly described their struggles and decisions to not strictly follow the requirements, emphasizing the perspective that their buildings are the residents’ homes. This was the case more so with ALC, particularly those with long-time owner operators who likely had developed a rapport with regulatory officials. By contrast, many others from ALC and NH described imposing the rules in fear of regulatory repercussions, which suggests there were gaps in collaboration between providers and health and safety officials in the management of the pandemic. These experiences highlight the critical importance of emergency response collaboration between providers and health and safety officials that prioritizes residents’ needs, particularly residents living with dementia, and accounts for the damage of disruptions and social isolation. Furthermore, they show that LTC care convoys extend beyond facility levels (e.g., NH, ALC) to include industry-level operations and relationships.
Limitations and Future Directions
Although our study offers previously unreported insights about how care convoys were disrupted by COVID-19, the perceptions of our participants cannot be applied to all LTC administrative leaders. There is the potential, however, that findings for specific types of LTC settings are transferrable to similar settings. Further, interviews were conducted over eight months, so timing may have influenced participants’ perceptions. Last, this study only addresses the beliefs of administrative leaders who may have been reluctant to discuss issues concerning any shortcomings and who do not represent the beliefs of other staff, residents, families, or regulators. We also note that our analyses relied on the perceptions of LTC leaders and did not reveal any differing effects of the pandemic based on resident-level sociodemographic factors (e.g., race, education). However, given the rich insight provided by our participants who were well positioned to comment holistically on care convoys, future research may build on this work to gather the perceptions of these other populations in order to gain further understanding. Additionally, future studies could extend this work by learning if and how distinct factors (e.g., facility type, bed size) contribute to or mitigate disrupted care during emergencies.
Conclusion
While safety precautions aimed to protect LTC residents from COVID-19 and certainly did save lives, our use of the convoys of care model reveals that the precautions critically disrupted care practices by shutting out family caregivers and heightening staff challenges. These disruptions appear to have had a cumulative effect, particularly on residents living with dementia who depend on regularity and personal contact and have difficulty adapting to sudden changes. Our study may help inform policy and practice in identifying which care strategies worked, the implications of care strategies that did not work, and considerations for moving forward when faced with another emergency in LTC.
Supplemental Material
Supplemental Material - “We Did More Damage”: How COVID-19 Collapsed the Care Convoys of Residents Living With Dementia
Supplemental Material for “We Did More Damage”: How COVID-19 Collapsed the Care Convoys of Residents Living With Dementia by Sara E. Hackett, Lindsay J. Peterson, Carlyn E. Vogel, and Debra Dobbs in Journal of Applied Gerontology
Footnotes
Acknowledgments
Thank you to Dr. Sweta Patel of Brown University for helping to collect the data used in the Nursing Home and Assisted Living Community Characteristics table.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging of the National Institutes of Health (NIH; R01AG060581-01). The content is solely the responsibility of the authors and does not represent the official views of the NIH.
IRB Approval
Our study was approved by the University of South Florida Institutional Review Board (approval no. STUDY001803_MOD000003). All participants provided verbal informed consent prior to enrollment in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.