
Abstract
Cognitive vulnerability, that is, clinically significant symptoms of dementia, depression, or delirium, puts older adults at high risk for physical inactivity and falls. Programs addressing activity and falls are needed. The purpose was to determine feasibility of an in-home, modified, Otago Exercise Program (OEP) for those with cognitive vulnerability, based on acceptability (retention and adherence), safety (pain intensity and falls), and potential positive effects (change in short physical performance battery (SPPB)). This secondary analysis of a randomized controlled trial included 80 participants who received the OEP; 64 completed it, 48% had depression, 22% had dementia, and 30% had a combination dementia/depression/delirium. Adherence to home exercise was low to moderate; pain was stable over 16 weeks; 31% of participants reported falls unrelated to OEP. SPPB increased from 6.95 to 7.74 (p < .01); age by time and diagnosis by time interactions were not significant. The modified OEP shows promising feasibility for older adults with cognitive vulnerability.
• Older adults with dementia, depression, or delirium improve physical performance similarly; regardless of age, after completing a 16-week in-home exercise program. • Participating in an in-home exercise program did not increase pain in older adults with cognitive vulnerability. • Older adults with cognitive vulnerability have modest adherence to unsupervised exercise in a modified Otago exercise program.
• The modified Otago exercise program should be more widely introduced and tested in this target population. • Adherence to the home exercises was done through manual logging which may not be the most effective way to monitor adherence; other technologies should be explored. • Families and older adults with depression, dementia, or delirium should be educated that performance of exercise, such as those in the modified Otago exercise program, did not cause pain or falls and can potentially increase physical performance.What this paper adds
Applications of study findings
Introduction
Cognitive vulnerability has been defined as living with clinically significant symptoms of dementia, depression, or delirium (Fortinsky et al., 2020). Two out of every three Americans 70 years and older experience some level of cognitive vulnerability (Hale et al., 2020). Additionally, these older adults are at greater risk for inactivity and falls as dementia doubles the risk of falls; untreated depression is associated with 37% greater risk of falls, and delirium is an independent risk factor for falls (Montero-Odasso et al., 2022).
Exercise improves strength, balance, and mobility and decreases fall risk in persons with dementia (de Souto Barreto et al., 2021; Forbes et al., 2015; Lam et al., 2018). However, trials examining similar features of balance, mobility, and falls risk in older adults with depression and delirium are rare (Porter et al., 2011). While exercise and physical activity are beneficial for all older adults, we do not know if balance, mobility, and falls risk improves similarly among older adults with cognitive vulnerability.
The Otago Exercise Program (OEP) is an evidence-based exercise program designed to prevent falls (Campbell et al., 1997). The original OEP was a year-long program delivered by physical therapists who focused on improving lower extremity strength, balance, and physical activity through in-home visits, phone calls, and home exercise(Campbell et al., 1997); although many modifications have been reported (Martins et al., 2018; Shubert et al., 2018). For older adults, adherence is cited as a barrier to effectiveness with adherence rates ranging from 37% to 55% (Thomas et al., 2010); greater variability is reported among those with cognitive vulnerability (consistently below 50%) and for those who perform unsupervised home exercise (Di Lorito et al., 2020; Katon et al., 2010).
However, OEP has not been adequately studied in older adults with cognitive vulnerability. For example, various functional gains were reported from: retrospective data from 34 patients with dementia receiving the OEP over 6 weeks, (Trapuzzano et al., 2020); 15 adults with developmental disabilities receiving weekly group OEP sessions (Renfro et al., 2016); and a randomized controlled trial (RCT) of 40 participants with Alzheimer disease, but a 42% drop-out rate. (Suttanon et al., 2012) The limited trials have small sample sizes, retrospective design, high drop-out rates, institutionalized participants, and undescribed modifications to the OEP (Chen et al., 2021; Kovács et al., 2013; Renfro et al., 2016; Suttanon et al., 2012; Trapuzzano et al., 2020). These factors limit the understanding and ultimately the adoption of a potentially useful program for persons with cognitive vulnerability.
Feasibility has been defined as the “extent to which an intervention was plausible in a given agency or setting” (Ojo et al., 2019). Feasibility studies are described by design, recruitment, adherence, safety, retention, randomization, adverse events, average exercise intensity, attrition rates, and improvements in physical performance (Baker et al., 2007; Borges-Machado et al., 2018; Callisaya et al., 2017). We adapted a feasibility model to study the OEP (Barker et al., 2016) (Figure 1). The objective of this study was to describe the feasibility of a modified OEP in terms of acceptability, safety, and potential positive effects in a group of home-dwelling older adults with cognitive vulnerabilities. Our hypothesis was that participants, regardless of age or diagnosis, will demonstrate similar improvement in Short Physical Performance Battery (SPPB) scores from start to finish of OEP participation. Feasibility model. The feasibility model used in this study was adapted from the framework presented by Barker et al., 2016.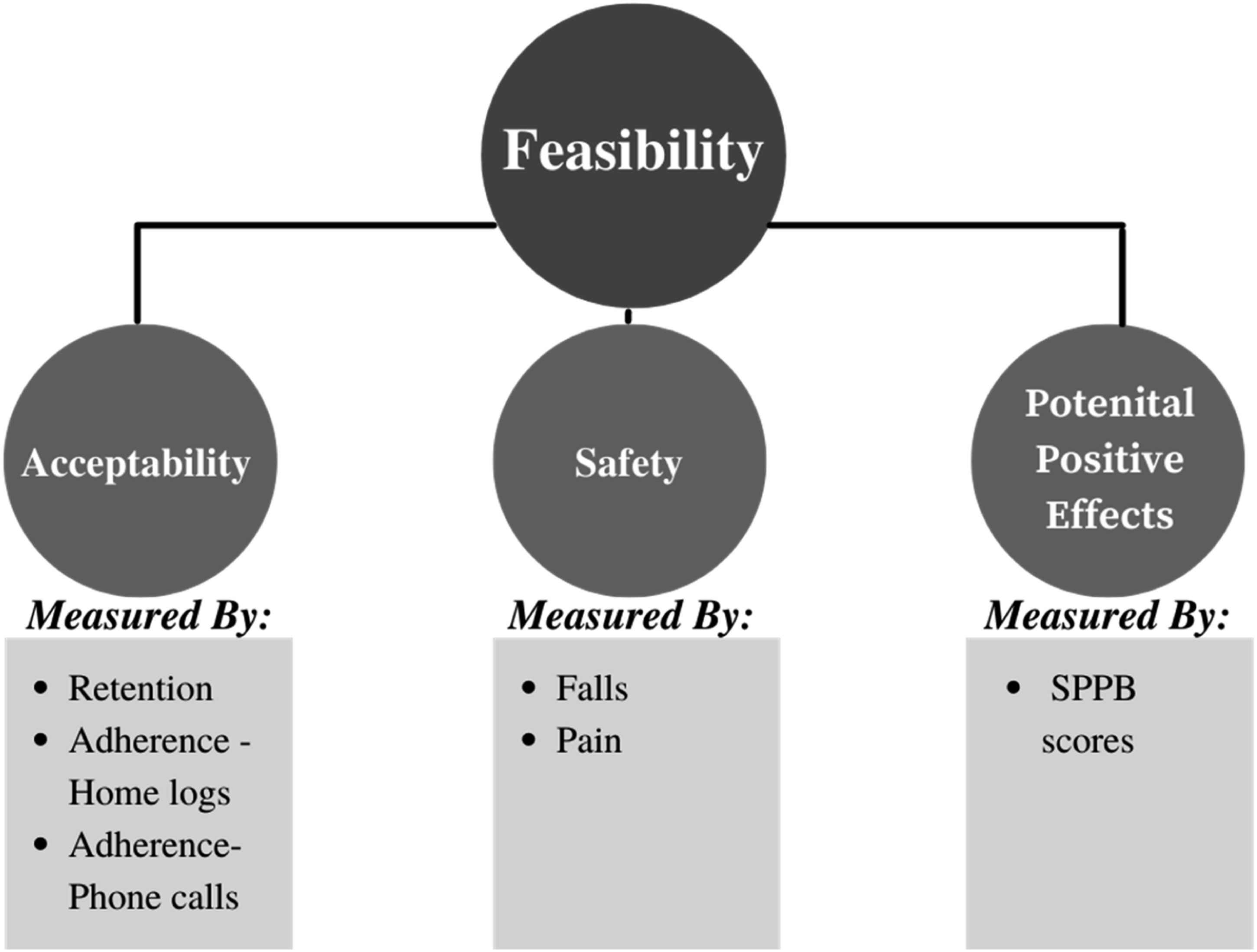
Methods
Study Design
This feasibility study is a secondary analysis of participants who received the modified OEP as part of a larger RCT. The parent trial’s randomization and study procedures have been reported elsewhere (Fortinsky et al., 2020) and compared multidisciplinary, home-based care team (HBCT) for older adults (age >65) with cognitive vulnerability with routine telephone-based care management (Fortinsky et al., 2020). The cohort for the secondary analysis was limited to those participants randomized to the HBCT and further qualified for the OEP by being ambulatory with a Timed Up and Go (TUG) (Podsiadlo & Richardson, 1991) time of >12 seconds and ≥1 reported fall in the past 12 months; or TUG time >20 seconds and fall or balance concerns as noted by the HBCT nurse practitioner (Kojima et al., 2015)
Recruitment of participants for the parent trial was initially based on ICD-10 diagnostic codes for dementia, depression, and delirium found in medical claims from a collaborating Medicare Advantage plan. In a second screening phase, classification of cognitive variability was confirmed by scores on validated tools. The Center for Epidemiologic Studies Depression scale (Radloff, 1977) was used, those who scored ≥16 were considered eligible for depression. For the Telephone Interview for Cognitive Status (Seo et al., 2011), those who scored <31 (range 0–41) were considered eligible for dementia. The FAM-CAM was used to determine if the member had a recent episode of delirium (Steis et al., 2012). Participants provided informed consent; proxy-consent was provided for individuals who did not pass the initial “capacity to consent” procedure. Proxies were family members, the large majority being spouses, followed by adult children.
Modified OEP Intervention
The 16-week OEP consisted of four home visits and two telephone calls. (Figure 2). Physical therapists (PTs) were trained in-person using standardized manuals and conducted each home visit by history taking (falls and pain), vital sign monitoring, and assessment and education in proper exercises. Warm-up exercises, strength and balance exercises, and the walking program were reviewed and progressed each visit, if appropriate, on an individualized basis. (Supplementary Appendix- Tiedier Checklist). The modifications from the original OEP included (1) decreasing the duration of the program from 52 to 16 weeks, (2) decreasing the number of home visits from 6 to 4, (3) decreasing the phone calls from 8 to 2, and (4) eliminating leg weights for the strengthening exercises to limit burden for the caregiver. Participants with dementia were required to have a caregiver present at each home visit, but caregivers were optional for the depression subgroup. Schedule of study contacts. The figure represents the 6-week duration of the program and the six study contacts. The shaded areas represent time windows in which the visit or call could occur.
Measurements
Participant Characteristic Measures
Demographic variables included age, gender, race, marital status, education level, and comorbidities were collected in the parent trial. Additional measures of cognitive vulnerability included the Montreal Cognitive Assessment (MOCA) to measure the level of cognitive impairment, (Nasreddine et al., 2005) and the Grid-Hamilton Depression Rating Scale (G-HAMD) to measure the severity of depressive symptoms (Williams et al., 2008). A fall history was also obtained; all additional measures were collected by the HBCT nurse practitioner before referral to the OEP.
Acceptability
Acceptability was measured by intervention adherence and program retention. Intervention adherence was monitored by PTs with logs and phone calls. Home exercise logs were completed daily by study participants or by the caregiver in cases of more severe dementia where the caregiver was needed for performance of exercise. During the two phone calls, participants (or caregivers) were queried about the frequency and duration of exercises and walking program. We used a threshold of ≥50% adherence to assist in the interpretation of our results based on reported adherence (45%) for older adults performing unsupervised exercise(Taylor et al., 2017). Program retention was the number of participants who completed OEP visit 4 divided by the total number of participants who had visit 1. We used 80% as the threshold for acceptable retention (Di Lorito et al., 2020).
Safety
Safety was assessed by inquiring about presence and intensity of pain and the number of falls. In the first 19 participants, pain intensity reporting was open ended; in the remaining participants, pain intensity was reported as none, mild, moderate, severe, very severe, or horrible (Mutebi et al., 2016). The PTs asked the participant or caregiver (if the subject was unable to recall) about fall history at each home visit and telephone call.
Potential Positive Effects
We examined the magnitude of change (first to final visit) in the SPPB to inform future trials using the OEP in home-dwelling older adults with cognitive vulnerabilities. The SPPB evaluates lower extremity physical performance and mobility disability in older adults and is globally recommended for assessment of falls risk (Guralnik et al., 1994; Montero-Odasso et al., 2022) It consists of balance, self-selected gait speed, and chair stand tests which were timed and rank ordered from 0 to 4, for a total score from 0 to 12 with 12 indicating highest function.
Statistical Methods
Descriptive statistics were used to describe the sample, adherence, program retention, and measures of safety. Intervention adherence was calculated by adding the total number of check marks performed for a given 4-week period and then calculating the average number of times the exercise was performed in a given week. Average time spent walking each week was calculated by the total minutes walked in a 4-week period divided by the total number of walks.
Sixty-four participants completed the program, but due to restrictions of COVID-19, the final home visit was converted to a phone call for six participants. Fifty-eight participants had completed SPPB scores that were used for the comparative analysis. SPPB data were analyzed using an ANOVA model with one repeated measure factor: Time (baseline-to post-treatment SPPB scores) and two between-subjects factors: Age Group and Diagnosis. Age groups were classified into 65–74; 75–84; 85+. The diagnosis groups were the screening diagnosis of depression and dementia. No patients screened for delirium alone, so those with delirium and dementia were termed—Dementia; those with delirium and depression were termed—Depression, and those with depression, dementia, and delirium were termed—Mixed. The Main effects of Time, Diagnosis, and Age Group were tested along with Diagnosis*Time and Age*Time interaction effects. Absence of outliers and assumptions of normality, homogeneity of variance, and sphericity were checked and verified. Bonferonni corrections were employed for post-hoc analyses. A ninety percent confidence interval (90% CI) for partial eta-squared (η2 p ) was computed to investigate the magnitude of the time effect (Steiger, 2004). All reported p-values are 2-sided. Analyses were performed using IBM SPSS Statistics version 27.
Results
Demographics.
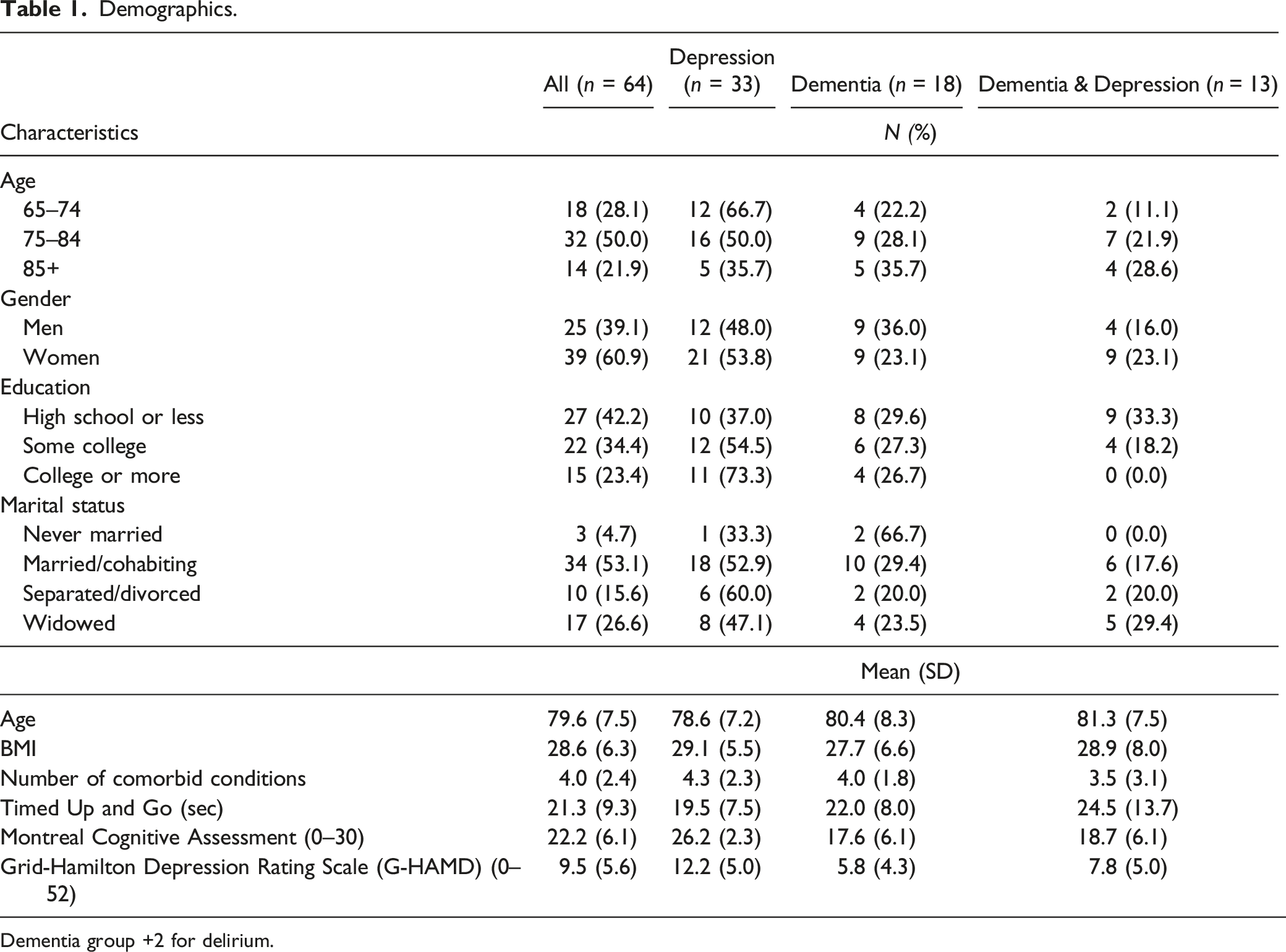
Dementia group +2 for delirium.
Acceptability
There was 80% retention- 64/80 completed both the first and final home visit. Reasons for discontinued participation included changes in health (e.g., new medical conditions or placement into LTC) (n = 5), study window in parent trial closed (n = 2), death (n = 2), unwilling to perform exercises (n = 4), and no reason provided (n = 3).
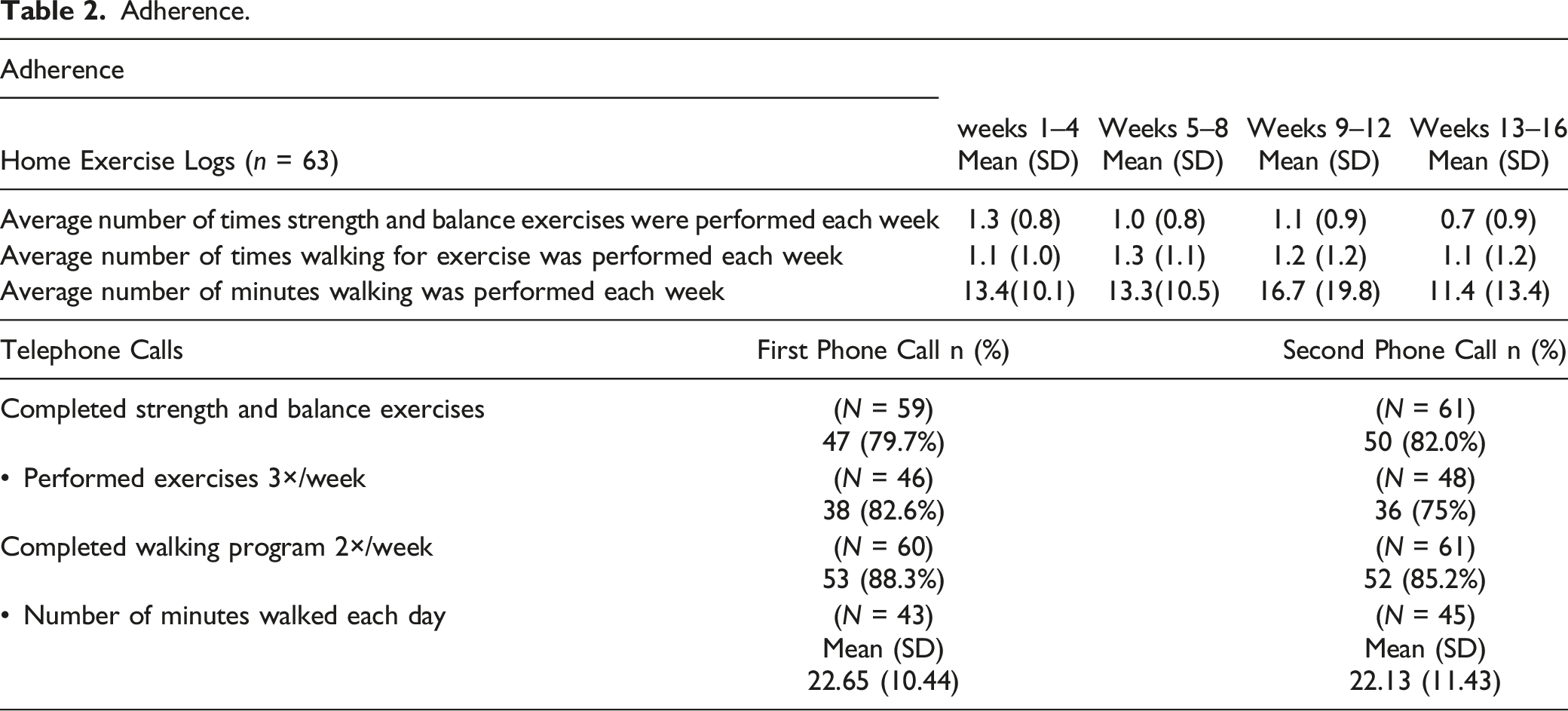
Adherence.
Safety
Pain
Forty participants (62.6%) reported some degree of pain at the first home visit. Mild pain was reported by 6 (15%) participants, moderate pain by 14 (35%), severe pain by 9 (22.5%), and very severe pain was noted in a single participant. The numbers varied minimally, and at the final visit, pain was relatively unchanged as 36 participants (56%) continued to report some degree of pain. Intensity of pain improved slightly overall; notably, reporting of severe pain was decreased from 22.5% to 8%, while mild and moderate pain both increased (19% and 44%, respectively. Intensity of pain was unable to be determined in 25% of participants due to the change in method for pain questions.
Falls
Of the 64 participants, 73% reported one or more falls in the year prior to OEP start. During their 16 weeks of OEP participation, 31% reported one or more falls; no falls occurred directly as a result of the OEP.
Potential Positive Effects
Short Physical Performance Battery Scores by Diagnosis Group and Age Group.

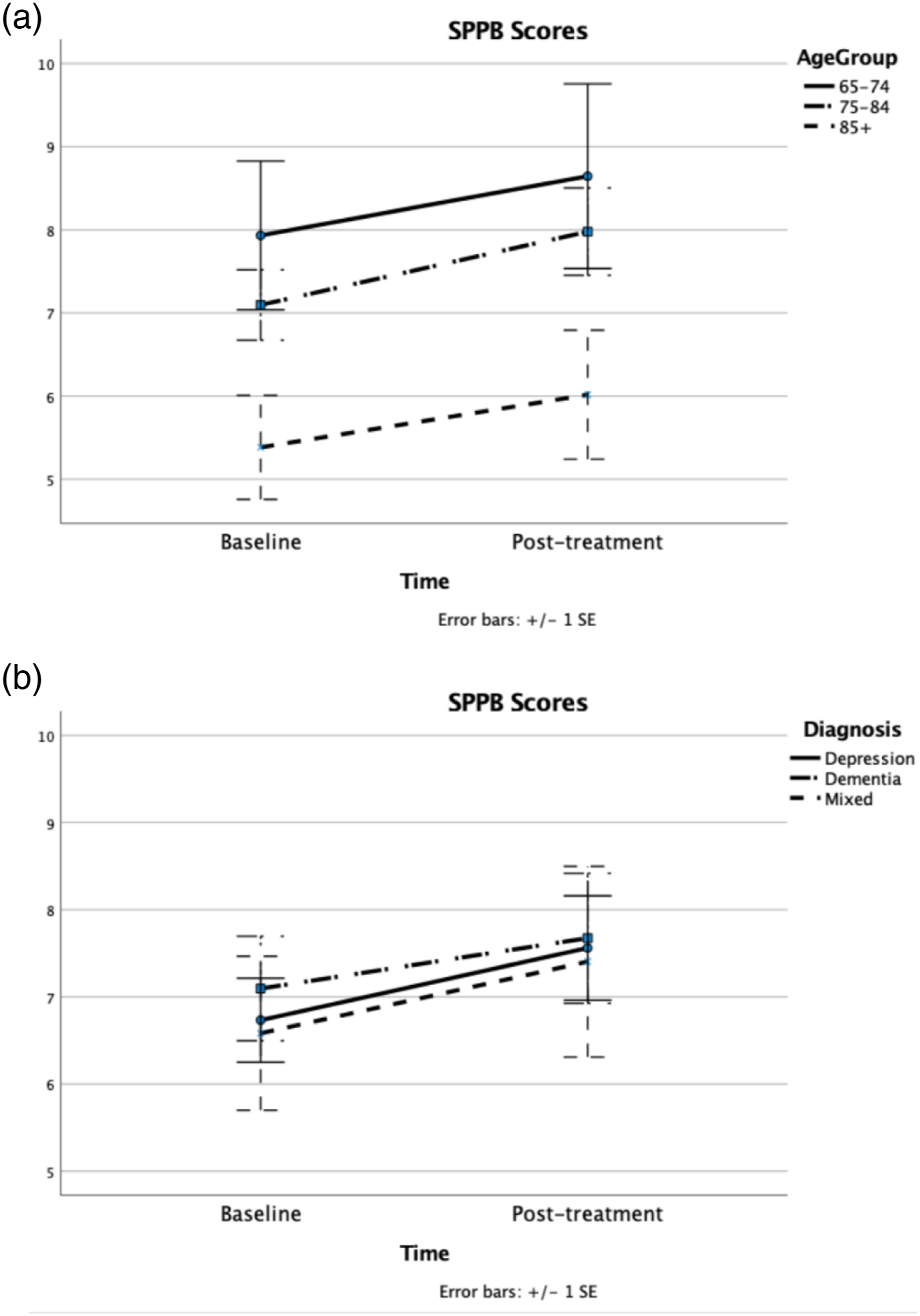
(a) and (b): Participants’ mean baseline and post-treatment SPPB scores by age and by diagnosis. Figure (a) lists measurement time on the x axis and SPPB scores on the y axis. The solid line represents participants 65–74 years old, the dot and dash line represents participants 74–84 years old, and the dashed line represents participants 85 years and older. Means are represented with open circles and 1 standard error is depicted around the mean. Figure (b) Figure (a) lists measurement time on the x axis and SPPB scores on the y axis. The solid line represents participants with a diagnosis of depression, the dot and dash line represents participants with dementia, and the dashed line represents those with both depression and dementia. Means are represented with open circles and 1 standard error is depicted around the mean.
Discussion
We described the feasibility of the OEP in home-dwelling older adults with cognitive vulnerability. Acceptability was demonstrated by program retention and self-reported adherence to home exercises via phone calls. Adherence to home exercise measured by exercise logs was low. Pain and falls did not increase and trended lower over the 16 weeks of the program. Mean SPPB scores increased from baseline to post-treatment across age groups and diagnoses. We believe this information about an understudied population adds to the applicability of the OEP.
Acceptability of the OEP met the threshold of 80% for program retention. A 58% retention rate for OEP was reported in a 6-month RCT of older adults with Alzheimer’s disease, (Suttanon et al., 2012) while an 18% attrition rate was reported in a systematic review of generalized exercise programs for those with dementia (Di Lorito et al., 2020). Cognitively healthy individuals demonstrated similar retention rates to the OEP to ours suggesting adequate feasibility of this intervention (Kyrdalen et al., 2014; Liston et al., 2014; Pitkälä et al., 2013). Adherence to the unsupervised home exercises differed based on the collection method. Exercise logs revealed less than 50% adherence for the strength and balance exercises and slightly greater than 50% for the walking component. Adherence was greatest during the first 4-weeks and tapered during the following weeks. In contrast, adherence obtained during phone calls was approximately 80%. Anecdotally, some participants reported doing the exercises more frequently, but failed to complete the logs. However, this is unlikely to explain the large discrepancy. Additionally, we cannot rule out whether the phone calls were subject to a social desirability bias (Adams et al., 2005).
Adherence to unsupervised exercise in persons with cognitive vulnerabilities is complex. In a secondary analysis, adherence to the OEP was higher in those with lower mobility, poorer attention and short-term memory (Davis et al., 2021). While this may seem counterintuitive, caregivers may take a larger role when cognition is impaired. While a caregiver was present during all visits for participants with dementia, caregiver involvement with the exercises was not recorded. An RCT of participants with dementia reported 82% adherence to the OEP, but had >40% drop-out rate, and 33% missing logs (Suttanon et al., 2012). Although motivational interviewing during the calls is associated with adherence, (Arkkukangas et al., 2018) the long term benefits of motivational interviewing on adherence and performance outcomes have not been substantiated. (Tuvemo Johnson et al., 2021).
A systematic review reported that 63% of studies did not report how adherence was monitored or recorded in persons with dementia. The few studies conducted in the home setting and monitored by a caregiver or participant showed adherence rates from 15% to 45% (Di Lorito et al., 2020), similar to our logbooks. In contrast, phone call monitoring of adherence in a large multicenter pragmatic trial, reported that 88% of participants with dementia were performing exercises as recommended (Lamb et al., 2018). We reported a slightly lower (80%) rate. Adherence to unsupervised exercise among those with cognitive vulnerability remains unclear, but the pre-specified structure of the OEP makes it reasonable to use with older adults with cognitive vulnerabilities.
Approximately 60% reported pain at the first home visit. Pain is common and is under-reported among those with cognitive vulnerabilities (van Dalen-Kok et al., 2015). While some variation in the severity of pain was noted over the 16 weeks, the percentage remained relatively stable. The small decrease in reported pain intensity (from severe pain to moderate or mild pain), may be related to increased physical activity associated with the OEP (Cederbom & Arkkukangas, 2019). Interestingly, 48% of the participants reported arthritis; and arthritis pain has been reported to decrease with exercise (van Dalen-Kok et al., 2015). The underlying physiologic rationale is not well understood for why exercise decreases pain, but our finding may be relevant for patients arthritis and cognitive vulnerabilities. Importantly, severity and the number experiencing pain did not increase. Twenty participants (31%) reported falls over 16 weeks of participation, similar to fall rates reported in OEP-based studies (Campbell et al., 1997; Kovács et al., 2013; Liu-Ambrose et al., 2008; Renfro et al., 2016). Interestingly, 73% of participants reported a fall in the year prior to participation. While comparing fall rates over 16 weeks of participation to the year prior to the study is not optimal, this line of inquiry for those with cognitive vulnerability could be studied in a future trial.
SPPB scores increased 0.8 points, on average, suggesting moderate improvement and clinically important change (Kwon et al., 2009; Perera et al., 2006). A 0.8-point change in SPPB was reported for a modified OEP for cognitively healthy older adults (Benavent-Caballer et al., 2016), but we did not find the SPPB reported for those with cognitive vulnerabilities. The improvement in SPPB scores was similar when comparing age groups and diagnoses. While the oldest group had lower baseline values than the younger participants, the improvement was similar. Our data suggest that older adults with cognitive vulnerabilities, regardless of age, can improve physical performance measures associated with fall risk.
A unique strength of this study was the inclusion of older adults with depressive symptoms. The majority of participants had depressive symptoms, alone or in combination with dementia and delirium. The combination of dementia and depressive symptoms in older age is common, but under-detected (van Dalen-Kok et al., 2015). Relationships between depression and poor adherence to exercise or physical activity have been reported (Allan et al., 2007; Katon et al., 2010) but studies for improving physical function with exercise in older adults with depression are rare. In depressed and socially vulnerable participants, SPPB scores after a group exercise program (Porter et al., 2011). Our findings support Porter and taken together may encourage clinicians to consider offering exercise programs (OEP or Steady As You Go) for home-dwelling older adults with cognitive vulnerabilities (Robson et al., 2003)
Limitations
There are several limitations, the therapists who delivered the OEP also collected the feasibility data. The lack of a control group limits our ability state that the OEP improved participants’ performance on the SPPB. Adherence measures were subject to recall bias of those with cognitive impairment as well as potential bias of proxies completing the forms on participants’ behalf. The conflicting results with the two adherence measures suggest that different measures, for example, actigraphy, may be a more valid representation of performance. The pain severity data should be interpreted cautiously due to our inability to have data for the entire sample. Lastly, weights were not used in the OEP which may have limited the effect size.
Conclusions
This study describes the feasibility of an OEP in home-dwelling older adults with cognitive vulnerabilities. The data suggest the OEP was acceptable in terms of retention, but equivocal in terms of adherence to home exercise. Initial indicators of safety by pain measurements and falls suggest no harmful effects. Participants, regardless of age group or cognitive diagnosis, showed clinically important gains in SPPB scores. Initial feasibility data suggest clinical use and further controlled trials of older adults with cognitive vulnerability.
Supplemental Material
Supplemental Material - Feasibility of a Modified Otago Exercise Program for Older Adults With Cognitive Vulnerability
Supplementary Material for Feasibility of a Modified Otago Exercise Program for Older Adults With Cognitive Vulnerability by Kathleen K. Mangione, Hope Darreff, McKenna Welsh, Weihong Ni, Edward Wolff, Julie T. Booth, Susan S. Glenney, and Richard H. Fortinsky in Journal of Applied Gerontology.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this manuscript was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award (IHS-1502-27171). The views expressed in this manuscript are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee. Supported also, in part, by the National Institutes of Health, National Institute on Aging (P30AG067988). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Approval
The parent clinical trial (Care Management for Cognitively Vulnerable Older Adults) is reviewed for continuation annually by the IRB at UCONN Health, IRB # 17-02-1, and was approved for continuation most recently in May 2022.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.