
Abstract
Individuals with intellectual and developmental disabilities (IDD) face several barriers to healthcare, making them less likely to receive numerous routine preventive health screenings. Preventive healthcare is a critical aspect to maintaining health and wellness, particularly for people with complex health needs. This study examines individual
• Adults with IDD living with family are less likely to receive breast and colon cancer screenings in mid- and later-life. • Transportation access and community inclusion may be important factors for completion of preventive health screenings for adults with IDD. • Medicaid expansion may reduce barriers to preventive healthcare usage among adults with IDD who are under the age of Medicare eligibility.
• Interventions to improve participation in preventive health screenings for adults with IDD should target those living with parents or other family as a population at particularly high risk of low health service utilization. • Interventions designed to improve transportation access among adults with intellectual and developmental disabilities may assist efforts to improve health and longevity among this population. • Interventions to increase community involvement among the population with IDD may have benefits for health service utilization as well.What this paper adds
Applications of study findings
Introduction
Preventive screening is critical to early diagnosis and treatment for both breast and colon cancers, yet, individuals aging (i.e., age 40+) with intellectual and developmental disabilities (IDD) face a number of barriers to healthcare access (Williamson et al., 2017; Willis et al., 2018). IDD refers to conditions that affect intellectual functioning and adaptive behaviors throughout the lifespan, such as Down syndrome and Autism Spectrums Disorders (NIH, 2021). Overall adults with IDD receive fewer preventive health screenings than the general population (Havercamp and Scott, 2015). As people with IDD age this lack of preventive healthcare puts them at risk of experiencing further health disadvantages in late life (Haveman et al., 2010).
Individual Risk Factors and Preventive Health Screenings Among Adults with IDD
Adults with IDD are less likely to receive mammograms, pap smears, and prostate exams than those without disabilities, but are more likely to receive a routine physical exam (Havercamp and Scott, 2015). Havercamp and Scott (2015) reported that 43.4% of women with developmental disabilities had not received a mammogram in the past 2 years, compared with 23.4% among those with no disability. Both individual- and system-level factors contribute to the lower rates of mammogram uptake among the population with IDD (Wilkinson et al., 2011; Williamson et al., 2017), which suggests the need for efforts at multiple levels to improve preventive health screening completion.
Although research indicates comparable or higher risk of gastrointestinal cancer in adults with intellectual disabilities, colorectal screening rates for adults with IDD remain well behind the general population (Willis et al., 2018). Individuals with IDD may be at heightened risk for colon cancer because of a generally higher prevalence of obesity and lack of physical activity, which are two key risk factors for colon cancer (Koritsas and Iacono, 2016).
Recent scholarship has noted the importance of social inclusion and community involvement for healthy aging among the population with IDD (Heller & Sorensen, 2013). Moreover, access to transportation may not only facilitate such inclusion and involvement, but can have additional benefits for those with IDD as well (Heller and Sorensen, 2013). Yet, most research concerning individual factors associated with health risks and healthcare usage among this population has focused on comorbidities and health behaviors (see Bershadsky et al., 2012; Haveman et al., 2010). Our study aims to examine not only demographic and health factors associated with preventive health screening completion, but community inclusion and engagement and transportation access as well.
State-Level Factors
Beyond individual factors there is also significant variation in screening completion by state (e.g., Bershadsky et al., 2012). Yet, the healthcare landscape has changed substantially since much of this research was conducted. In particular, passage of the Affordable Care Act (ACA) in 2010 ushered in numerous changes to the American healthcare system, including a broad expansion of healthcare insurance uptake as well as expansion of Medicaid to help fund preventive healthcare services among the poorest Americans. However, implementation of Medicaid expansion varied by state, as well. Adults with IDD living in states without Medicaid expansion may be at greater risk of failing to receive important preventive measures such as mammograms and colonoscopies, especially before reaching the age for Medicare eligibility. Recent evidence suggests that Medicaid expansion was associated with a reduction in emergency department visits among the population with IDD, a potential sign of better preventive care (Horner-Johnson et al., 2022). In addition to examining individual factors associated with mammogram and colonoscopy screening completion among the population aging with IDD, we aim to explore (1) state-level variation in screening completion, and (2) whether Medicaid expansion is associated with screening completion, particularly at younger ages before individuals reach the age of Medicare eligibility (65+) or Medicare/Medicaid dual-eligibility.
Methods
Data and Sample
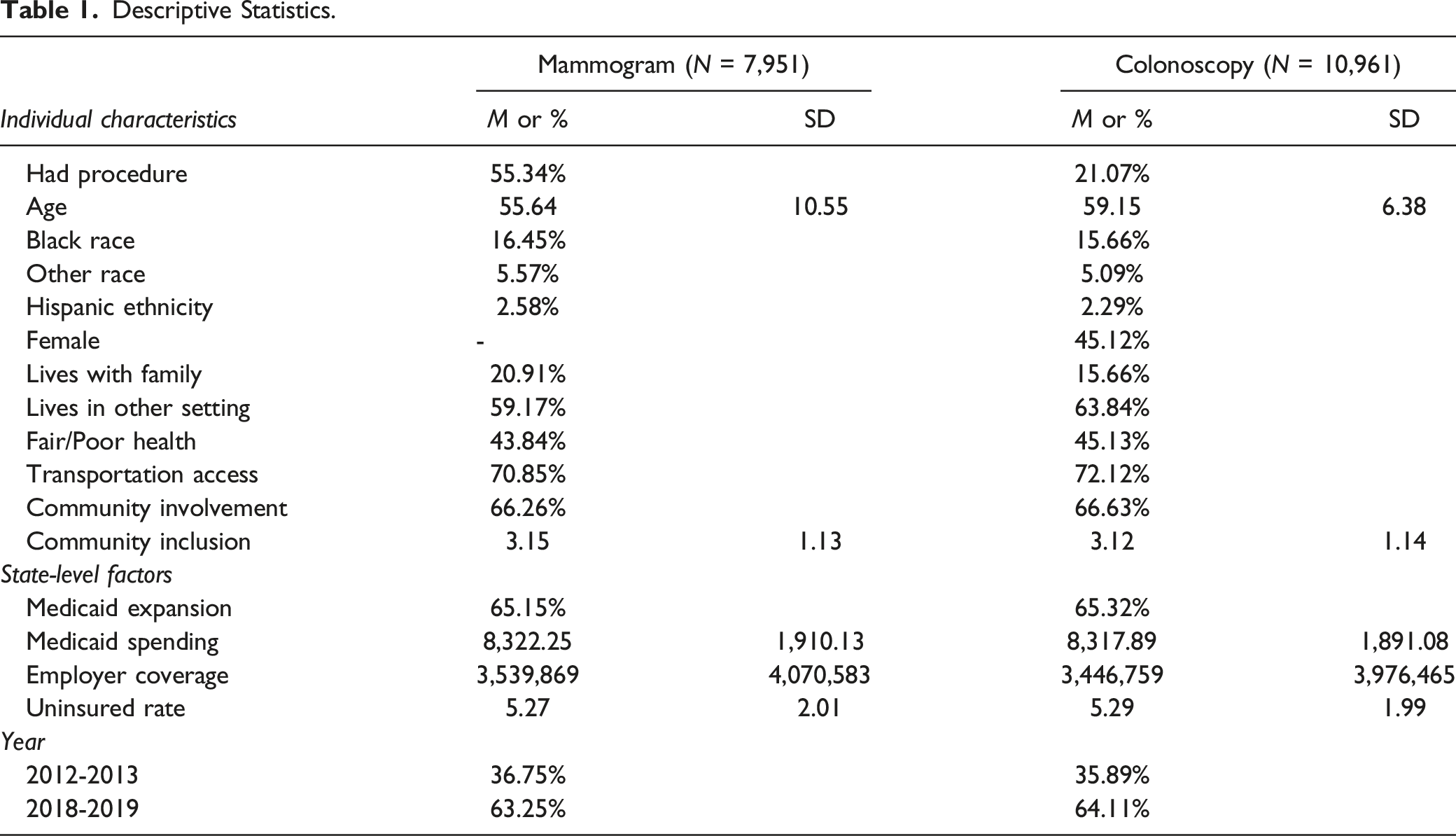
Data came from two recent waves of the National Core Indicators In-Person Survey (NCI-IPS). Due to the panel-design of the study, observations from the 2012-2013 and 2018-2019 waves were pooled. These dates include the most recent data before Medicaid expansion and the most recent data available at the start of analyses. The NCI-IPS collects information from individuals with IDD receiving state services—such as employment and day program supports or skills training—in participating states (n = 37 states in this study). While the definition of IDD varies by state, the NCI-IPS includes a minimum random sample of 400 adults per state (18+ years). Qualifying individuals must meet the state’s definition of IDD services and receive at least one state service besides case management for inclusion in the study (NCI-IPS, 2018). Analyses concerning mammogram completion were limited to women age 40 or older (maximum: 107) at the time of data collection (n = 7,951 individuals from 37 states). Analyses concerning colonoscopy completion were limited to participants age 50–75 at the time of data collection (n = 10,961 individuals from 37 states).
Measures
Outcomes
Mammogram completion was generated as a dichotomous indicator (1 = yes, 0 = no) of whether an eligible female participant (age 40+) had received a mammogram within the last calendar year. Colonoscopy completion was generated as a dichotomous indicator (1 = yes, 0 = no) of whether an eligible participant (age 50–75) had ever received a colonoscopy.
Individual-level factors
Age was measured in years. We also included a quadratic age term to examine whether uptake was reduced among the oldest participants (e.g., 70+) following increases through their 40s–60s. Race was measured using dichotomous indicators for White (reference), Black, and Other race. Hispanic ethnicity was measured with a dichotomous indicator (1 = yes, 0 = no). Gender was measured using a dichotomous indicator (1 = female, 0 = male). Living situation was measured using dichotomous indicators for lives independently (reference), lives with family, and other living situation. Poor self-rated health was measured as a dichotomous indicator (1 = fair/poor, 0 = excellent/very good/good). Transportation access was measured as a dichotomous indicator of whether one has access to transportation when needed (1 = yes, 0 = no). Community involvement was measured as a dichotomous indicator of whether a participant was involved in any community activity in the past month (1 = yes, 0 = no) and Community inclusion was measured as a sum-score (0-4) scale concerning whether participants have gone out for errands or appointments, shopping, entertainment, and/or to eat in the past month.
State-level characteristics
Medicaid expansion was measured as a dichotomous indicator of whether a state approved expansion of Medicaid following passage of the American Care Act (1 = yes, 0 = no). To avoid spurious results for Medicaid expansion we also included state-level characteristics associated with both participants’ healthcare access and the likelihood of Medicaid expansion. These included continuous measures for total state Medicaid expenditures, number of residents with employer-based healthcare, and state uninsured rate.
Interactions
We expect expanded access to Medicaid to be most strongly associated with healthcare usage among participants under the age of 65 required for dual Medicare/Medicaid eligibility. Therefore, interactions were tested between state-level Medicaid expansion and the individual age and age-squared terms.
Analytic Strategy
Multilevel logistic regression models were estimated to address our research questions, whereby individuals were nested within states. Multiple imputation was used to address missing data at the individual level. There was no missing data at the state level.
Results
Descriptive Statistics.
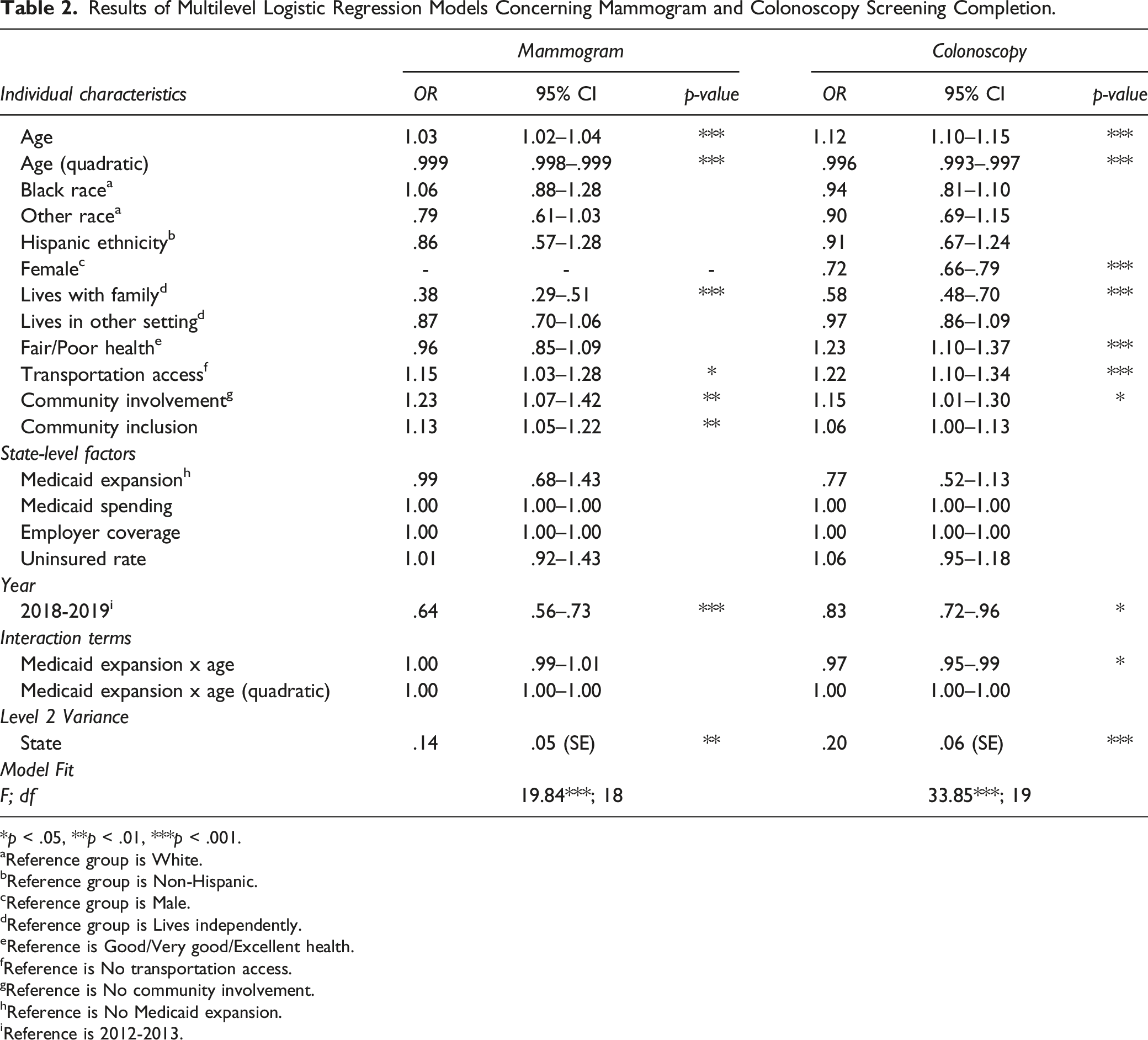
Results of Multilevel Logistic Regression Models Concerning Mammogram and Colonoscopy Screening Completion.
*p < .05, **p < .01, ***p < .001.
aReference group is White.
bReference group is Non-Hispanic.
cReference group is Male.
dReference group is Lives independently.
eReference is Good/Very good/Excellent health.
fReference is No transportation access.
gReference is No community involvement.
hReference is No Medicaid expansion.
iReference is 2012-2013.
Concerning colonoscopy completion, significant individual-level factors included age (OR = 1.12, 95% CI = 1.10–1.15) and age-squared (OR = .996, 95% CI = .994–.998); female gender (OR = .72, 95% CI = .66–.79), living with family rather than independently (OR = .58, 95% CI = .48–.70); poor self-rated health (OR = 1.23, 95% CI = 1.10–1.37); transportation access (OR = 1.22, 95% CI = 1.10–1.34); and community involvement (OR = 1.15, 95% CI = 1.01–1.30). Likelihood of colonoscopy completion was lower in 2018-2019 than in 2012-2013 (OR = .83, 95% CI = .72–.96). None of the state-level characteristics has significant main effects; however, the effect of Medicaid expansion varied significantly by individuals’ age (OR = .97, 95% CI = .95–.99), such that Medicaid expansion was associated with colonoscopy completion at younger ages only. Even after accounting for individual-level factors, colonoscopy completion still varied significantly by state (p < .001).
Discussion
This study identified several factors associated with the likelihood of midlife and older adults with IDD receiving mammogram and colonoscopy screenings. Notably, individual-level factors appeared more influential than state-level factors. Foremost among these were living situation, access to transportation, and community involvement. Importantly, our study is the first we are aware of to examine the roles of transportation access and community involvement alongside other individual- and state-level characteristics of adults with IDD. Results suggest that both factors reduce barriers to healthcare access and may be related with improved health behaviors—including screening uptake—among adults with IDD (Heller and Sorensen, 2013).
Our findings are consistent with previous research on mammograms which also found women living with parents or family were least likely to receive mammograms (Bershadsky et al., 2012). Unlike prior research we also found that those living with parents or family were significantly less likely than those living independently to have received colorectal screening (Bershadsky et al., 2012). Families may be fearful of cancer screenings and may even infantilize their adult child with IDD, believing they do not need adult services. These views impose barriers to screening and may explain why adults with IDD who live with parents and family have lower rates of screening completion (Greenwood et al., 2014).
Among state-level factors we found only that state Medicaid expansion was significantly associated with an increased likelihood of completing a colonoscopy screening among younger persons in the sample (e.g., in their 50s). This coheres with recent research concerning Medicaid expansion and emergency department visits among adults with IDD (Horner-Johnson et al., 2022). However, significant variation at the state level remained, indicating that unmeasured state-level factors are likely associated with healthcare screenings as well.
Limitations
The sample was drawn from adults with IDD receiving state services in states participating in the NCI-IPS. Thus the sample is likely not representative of all adults aging with IDD in the U.S. Moreover, it is possible that individuals were receiving state services at multiple timepoints. Because participants were not tracked longitudinally, we lack a pre/post design for Medicaid expansion. Further, we cannot determine whether Medicaid expansion directly affected sample participants or their families. Numerous items were also limited to dichotomous measurement (e.g., self-rated health), which masks variability within dichotomous groups.
Conclusion
We found that community involvement and transportation access were associated with a greater likelihood of preventive health screening completion, while living with family was associated with a lower likelihood of screening completion. Moreover, results identify significant variation in screening completion by state, which is partly—but not completely—explained by Medicaid expansion. Future research should build on these insights to improve healthcare access and uptake among the population aging with IDD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from The Patrick and Catherine Weldon Donaghue Medical Research Foundation.
Ethical Approval
The present research involves the use of de-identified secondary data and does not meet the definition of Human Subjects Research. Therefore no Institutional Review Board review was required.