
Abstract
Wearable activity trackers (WAT) have shown high potential to improve health in the aging population. Evidence links various social factors with WAT use in older adults, but mainly within small samples and the prevalence of their WAT use during the COVID-19 is unknown. We reported WAT use prevalence before and during the first wave of COVID-19 and examined social factors associated with WAT use frequency using a nationally representative sample of 3302 U.S. older adults. We used Multinomial Logistic Regression to identify social factors associated with WAT use frequency. Only 10.3% of pre-COVID-19 and 10.9% of first-wave subsamples were frequent WAT users. Older adults aged 75 and above and those with low incomes were less likely to frequently use WATs. Our findings suggest socioeconomic and age disparities in WAT use among older Americans. Future studies should focus on enhancing low-income older adults’ WAT adoption to enable equal access to WAT-related health benefits.
• This research describes the pattern of wearable activity trackers (WAT) use in American older adults, which was understudied in the U.S. older adult population. • This research describes prevalence of WAT use before and during the first wave of the COVID-19 pandemic among American older adults, which provides essential information on older adults’ health monitoring behavior responding to COVID-19 and related policy. • This research adds to the current literature on social disparities in WAT use among older Americans, which needs to be addressed in future research.
• To help close the digital divide, policies are needed to improve the accessibility of WATs among socially disadvantaged older Americans. • Detailed WAT instructions should be provided to older adults and the health benefits of using WATs frequently should be emphasized. • Future WAT-related research needs to focus on interventions designed for socially disadvantaged older adults, considering the long-term impact of the COVID-19 pandemic.What this paper adds
Applications of study findings
Introduction
Wearable activity trackers (WATs) refer to smart electronic devices—often wrist-worn—that detect, analyze, and transmit information on body signals such as vital signs, physical activity, or ambient data to provide real-time biofeedback to the wearer (Düking et al., 2016; O’Donoghue & Herbert, 2012). WATs have been increasingly adopted for health self-monitoring in the last few years. Commercial WATs, such as Fitbit, Apple Watch, Garmin, etc., are accessible and may promote health outcomes through self-monitoring of health parameters (e.g., physical activity, heart rate, and sleep), safety alerts (e.g., fall risk detection), stress reduction (e.g., breathing techniques), and symptom tracking and management (e.g., reporting COVID-19 or other symptoms) (Tedesco et al., 2017; Zhang et al., 2022).
Several qualitative studies have found that older adults reported positive feedback regarding the ease of use, usefulness, and acceptability, and showed a willingness to learn how to operate WATs (Li et al., 2022; Zhang et al., 2022; Zytnick et al., 2023), but also noted issues including low familiarity or limited access to the technology, lack of available training and assistance, privacy issues (Fischer et al., 2014; Li et al., 2022), and design challenges (Fang & Chang, 2016; Puri et al., 2017) among older adults. Quantitative studies have focused mainly on the effectiveness of WAT-facilitated interventions that often incorporate the use of WATs with behavioral change techniques including goal setting, providing positive feedback, providing social support, and improving self-efficacy towards activity goals (Olander et al., 2013; Western et al., 2021). WATs and WAT-based interventions have demonstrated effectiveness in improving physical activity levels in older adults including step counts (Liu et al., 2020; Stockwell et al., 2019) which results in improvement of cardiovascular health (Myers, 2003), prevention of type 2 diabetes (Colberg et al., 2010), a decreased risk for obesity (Ringeval et al., 2020), and better sleep and mental health (Kline, 2014; Sharma et al., 2006). In addition, recent research has linked increased step counts with a significant decrease in the risk of developing dementia (Del Pozo Cruz et al., 2022).
Despite older adults’ acceptance and WATs’ potential health benefits, use of WATs among U.S. older adults remains unknown. First, although it has been reported that about 25% of adults between 18 and 49 years of age and 17% of adults over 50 years of age used a WAT in 2019 (Vogels, 2020), there is a lack of evidence showing the prevalence of WAT use among older adults aged 65 years and above. Older adults aged 65 years and above may significantly differ from those aged between 50–65 years in multiple social and behavioral aspects including retirement status, daily activities and routines, social behaviors, health conditions, and healthcare needs (Isaacowitz et al., 2021; Noftle & Fleeson, 2010). As a result, older adults aged 65 years and above may have different needs or purposes of using technology than those who are younger, leading to different prevalence of use (Faverio, 2022). Therefore, it is necessary to separately investigate WAT use prevalence of those 65 years and above. Second, frequency of WAT use may be linked to users’ physical activity levels and health but only 47.3% American adult WAT users use WATs every day (Chandrasekaran et al., 2020), and no study has investigated frequency of U.S. older adults’ use of WATs. Third, the public’s use of digital technology has significantly increased during the COVID-19 pandemic (De’ et al., 2020), yet no study has specifically investigated use of WATs since the COVID-19 pandemic among older adults.
The digital divide is the gulf between those who have ready access to technology and those who do not (Lai & Widmar, 2021). Older adults are considered to be on the disadvantaged side of the digital divide as they have lower technology adoption (Faverio, 2022) and lower digital literacy (Hargittai & Dobransky, 2017; Hargittai et al., 2019; van Deursen & van Dijk, 2011) compared to other age groups. Since COVID-19 was announced as a global pandemic by the World Health Organization in March 2020, in-person activities significantly decreased and reliance on digital technology drastically increased (De’ et al., 2020; Lai & Widmar, 2021). The older adult population has been shown to have less access to technology and less opportunities to utilize online exercise programs during the pandemic (Füzéki et al., 2022; Haase et al., 2021). Similar to other digital devices, WATs often require a connection to smartphones and the Internet, and the digital divide may result in low WAT use rates among those with less access and low digital literacy.
The digital divide is also closely related to social factors (Mubarak et al., 2020). Social factors are social, demographic, and economic characteristics of a population, including age, sex, race and ethnicity, income, education, and neighborhood environments. Different social factors have been found to be associated with the use of WATs in older adults: older adults who are female, White, younger than 75 years, have higher education levels, more income, and are healthier have higher rates of WAT use (Kakulla, 2020; Li et al., 2020; Macridis et al., 2018). However, most of these findings were reported through studies with small samples (5–49 participants) who participated in an intervention (Brickwood et al., 2019; Cadmus-Bertram et al., 2015; Fausset et al., 2013; Preusse et al., 2017; Puri et al., 2017; Rosales et al., 2018). With the three studies investigating older adults’ WAT use, two of them (Kakulla, 2020; Vogels, 2020) only examined basic social factors (age, race, sex, education level, and income), the other study (Schuster et al., 2023) used data only collected online which may result in sampling bias. There is still a need to examine social factors including age, sex, race, education, income, and area factors associated with older adults aged 65 years and above with large representative U.S. older adult data.
Study Aims and Hypotheses
Aim 1
Examine the prevalence of WAT use among U.S. older adults aged 65 years and above before and during the first wave of the COVID-19 pandemic.
Aim 2
Identify social factors (age, gender, race/ethnicity, education, income, and area factors) associated with the use of WATs among U.S. older adults aged 65 years and above.
Hypothesis
Older adults aged 65–74 years, who are female, White, have higher education and income, and live in large metro areas are more likely to use WATs than their counterparts.
Exploratory Aim
Explore social factors associated with the use of WATs among U.S. older adults aged 65 years and above before and during the first wave of the COVID-19 pandemic.
The results of this study will provide important guidance to WAT-related or technology-related clinical practice and interventions, research directions, and policy changes to benefit the older adult population.
Methods
Conceptual Framework
The conceptual framework was adapted from the Fundamental Cause Theory developed by Link and Phelan in 1995 (Link & Phelan, 1995). Fundamental Cause Theory describes the way that social adversity may influence resource access through multiple replicating and interacting pathways. In Fundamental Cause Theory, socioeconomic status and other social factors are considered as a “fundamental cause” of various health outcomes. This theory posits that variations in social factors may cause health inequity by different levels of resources an individual may utilize to promote health and avoid disease. In this study, the use of WATs can be considered as an important resource, a technological tool, that may promote physical activity and other health outcomes, and avoid chronic illness (see Figure 1). Conceptual Framework, adapted from Fundamental Cause Theory by Link and Phelan.
Study Design and Recruitment
This is a cross-sectional secondary data analysis using the Health Information National Trends Survey (HINTS) dataset with data collected from January to April in 2019 (Cycle 3) and February to June in 2020 (Cycle 4). Launched by NIH’s National Cancer Institute (NCI) in 2003, HINTS regularly collects nationally representative data about the American public’s understanding of, attitudes toward, and utilization of cancer-related and other health-related information. To recruit participants, HINTS sent postal mail to random samples of non-vacant U.S. residential addresses for both 2019 and 2020 cohorts. More details about the HINTS study are available through HINTS briefs and reports (National Institute of Health n.d.). The present study includes 3302 participants aged 65 and above from both Cycles 3 and 4. All data collected in HINTS are self-reported on paper and sent back by mail.
Measures
Independent Variables
Sociodemographic factors included age, sex, annual household income, education, race/ethnicity, and area factors. Participants’ sex was self-reported, including “Male” and “Female.” Based on previous literature and data distribution, the age variable was dichotomized into 65–74 years and 75 years and above (Lee et al., 2018). Annual household income was categorized into (1) low income (less than $35,000), (2) intermediate income ($35,000–$75,000), and (3) high income ($75,000 and above) (Xie et al., 2020). The educational variable was categorized into (1) high school or less, (2) some college, and (3) college degree or higher. Race and ethnicity were categorized into three categories: (1) Non-Hispanic White, (2) non-Hispanic Black, and (3) Hispanic, non-Hispanic Asians, and others. Due to the small number of participants reporting to be Hispanic, non-Hispanic Asians, and others, we combined these race and ethnic groups as one group, to reach a comparative balance with the other two groups. Area factors included region and area minority percentage. Region population was a variable created to reflect the USDA 2013 rural-urban continuum codes in which a classification scheme was used to distinguish metropolitan counties by population size of the metro area. For the present study, region population was dichotomized into (1) Large Metro Area: Counties in metro areas of at least 250,000 population; and (2) Small/Non-Metro Area: Counties in metro areas of fewer than 250,000 population or non-metro areas. The area minority level was formed using the census tract-level characteristics from the 2014–2018 American Community Survey data file. According to HINTS 5, addresses in census tracts with a population proportion of Hispanics or African Americans that equaled or exceeded 34% were assigned to the high minority level category, and the remaining addresses were assigned to low minority level category.
Dependent Variable: WAT Use
WAT use is based on the subject’s self-reported WAT use over the prior 12 months and the frequency of use over the past month of data collection. Two questions were asked regarding WAT use: (1) “In the last 12 months, have you used an electronic wearable device to monitor or track your health or activity? For example, a Fitbit, Apple Watch, or Garmin Vivofit.” (2) “In the past month, how often did you use a wearable device to track your health?” For those who answered “Yes” in the previous question, options included “Every day,” “Almost every day,” “1–2 times per week,” “Less than once per week,” or “I did not use a wearable device in the past month.”
Based on these questions, we categorized the participants into three categories: (1) Frequent WAT use: those who reported using a WAT “Every day” or “Almost every day” in the past month; (2) Infrequent use: those who reported using a WAT “1–2 times per week,” “Less than once per week,” or “I did not use a wearable device in the past month (but used one in the past year)”; and (3) No use: those who did not use a WAT in the past month and those who did not use a WAT over the past 12 months.
COVID-19 Pandemic
A “Pandemic” variable was made available in the HINTS Cycle 4 (2020) to flag households whose survey was received after the World Health Organization declared COVID-19 to be a pandemic on March 11, 2020. For this analysis, all data collected in 2019 and before March 11, 2020, were categorized as “Before COVID-19,” and data collected after March 11 before June (end of data collection) were categorized as “During the first wave of COVID-19” to reflect the period during the first wave of the COVID-19 pandemic.
Covariates
Other covariates were included in the analyses. Body Mass Index (BMI) was calculated using the respondents’ self-reported heights and weights and was dichotomized into (1) non-obesity: under 30, and (2) obesity: 30 and above. Smoking status was a variable derived from two questions on past smoking experience and current smoking frequency and was categorized into current, former, and never smoker. The marital status question was included in the questionnaire and dichotomized into two categories: (1) married or living with a partner, and (2) divorced, widowed, separated, or never married. Comorbidity was measured by the sum of reported medical conditions reported by respondents and categorized into: (1) one or no comorbidity and (2) multiple comorbidities. General health status was assessed by the item: “In general, would you say your health is …” with the choices of “Excellent, Very good, Good, Fair, or Poor.” Depression was assessed by the item: “Has a doctor or other health professional ever told you that you had depression or anxiety disorder?” Health insurance coverage was a variable derived from several health insurance-related items from the HINTS survey and dichotomized into “Yes” and “No.”
Statistical Analyses
Since 14.6% of data were missing on the variable “annual household income,” an imputation of this variable generated by HINTS was used for this data analysis. Full-sample weights were provided by HINTS dataset and were used in the analyses to provide population estimates. We described sample characteristics of the three groups with different WAT use frequency (no use, infrequent use, and frequent use) using Pearson’s chi-square. Variables with a p-value of less than .10 in bivariate analyses were considered in further analyses; corresponding variables (sex, age, education, race and ethnicity, smoking status, marital status, comorbidity, depression, and area minority level) were then included in the regression analyses. Multinomial logistic regression models were conducted to examine the social factors associated with older adults’ WAT use in the total sample and before COVID-19 and during COVID-19 subgroups. A test with a p-value of less than .05 was considered statistically significant for multivariable regression. In addition, we adjusted for multiple testing in the multinomial regression models following a Bonferroni’s correction for the number of social factors tested (9) and the number of subgroup tests (2), and a p-value less than .0028 was considered as statistically significant in the new set of multivariable analyses. Both results with and without Bonferroni’s correction were presented as varying levels of evidence. The social factors that are significant after the correction are considered as the strongest evidence of social factors associated with older adults’ use of WATs.
Results
Sample Characteristics
Sample Characteristics Based on WAT Use Frequency (Weighted Analysis).

The Pattern of WAT Use
In the study sample, 2812 older adults reported no WAT use, 169 reported infrequent use of WATs, and 321 used WAT frequently in the past month (65.5% of WAT users frequently used WATs). The weighted analysis showed small but non-significant differences in WAT use were observed during versus before the COVID-19 pandemic: 14.4% older adults were WAT users (frequent users: 10.3%) before COVID-19 and 16.9% (frequent users: 10.9%) during the first wave of COVID-19.
Bivariate Associations Between Social Factors and WAT Use
In bivariate analysis, older adults with younger age (65–74 years), higher education, higher annual household income, smoking status of “former” or “never” smoker, a “good” self-rated general health status, one or no comorbidity, and no depression diagnosis reported frequent use of WATs (all p < .05; see Table 1).
Associations Between Social Factors and Frequent WAT Use
Associations Between Social Factors and Electronic Wearable Device Use (Weighted Analysis).
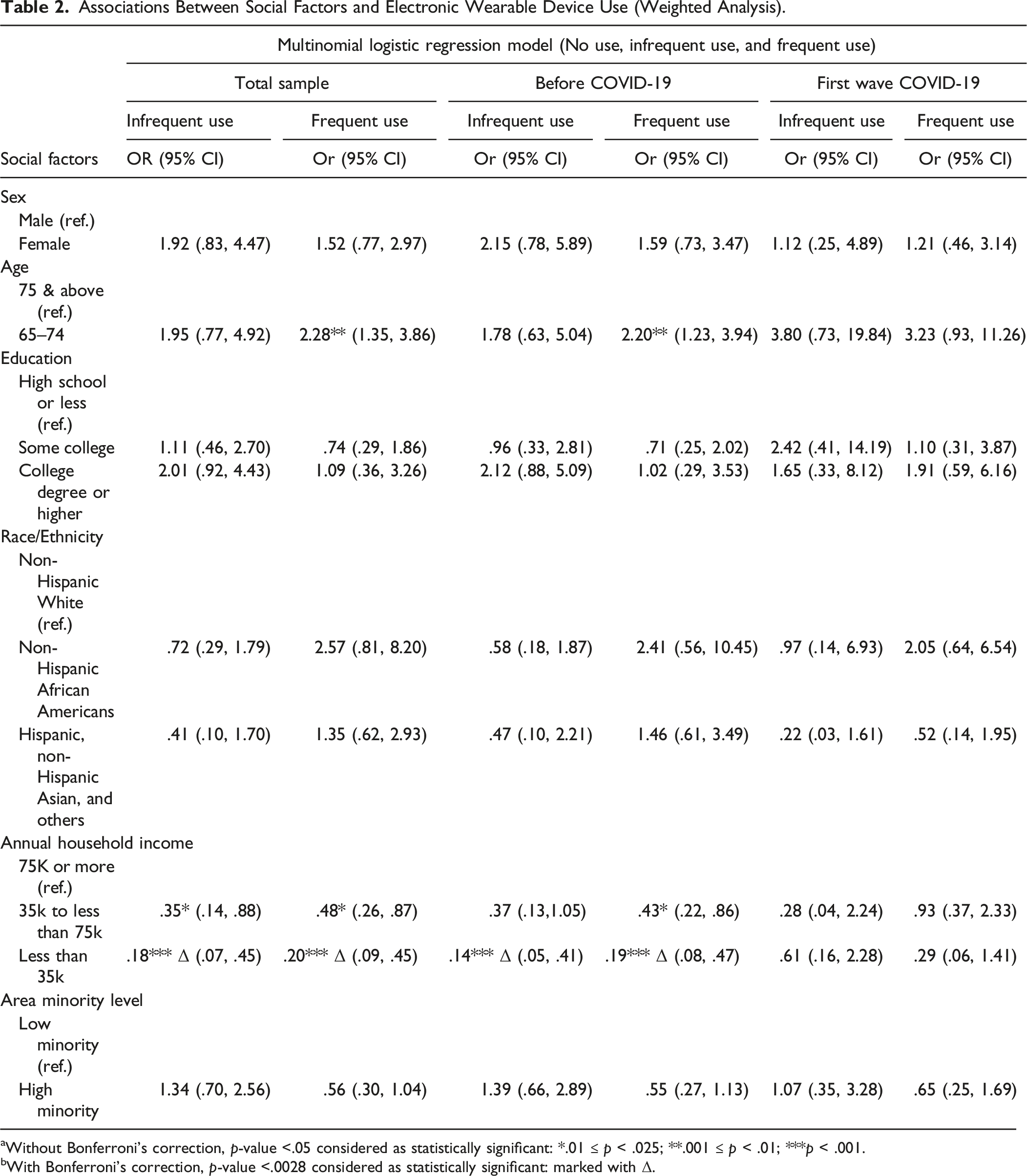
aWithout Bonferroni’s correction, p-value <.05 considered as statistically significant: *.01 ≤ p < .025; **.001 ≤ p < .01; ***p < .001.
bWith Bonferroni’s correction, p-value <.0028 considered as statistically significant: marked with Δ.
Associations Before and During the First Wave of COVID-19
Subgroup analyses were conducted as an additional exploration of the sociodemographic and area factors associated with older adults’ WAT use in both models before and during the first wave of the COVID-19 pandemic, with detailed data shown in Table 2. Before COVID-19, we found similar results as in the total sample: Older adults aged between 65 and 74 years had higher odds of being WAT frequent users compared to older adults aged 75 and above (OR: 2.20, 95% Confidence Interval [CI]: 1.23, 3.94). Compared to older adults who reported annual household income higher than $75,000, those reported middle income ($35,000–$75,000) had lower odds of being WAT frequent users (OR: .43, 95% CI: .22, 0.86), and those reported low income (less than $35,000) had lower odds of being WAT infrequent users (OR: .14, 95% CI: .05, 0.41) and frequent users (OR: .19, 95% CI: .08, .47). During the first wave of COVID-19, no significant associations were found between social factors and WAT use frequency.
Association Between Social Factors and WAT Use (with Bonferroni’s Correction)
After Bonferroni’s correction, only annual household income was significantly associated with older adults’ use of WAT. In the total sample, compared to older adults who reported annual household income higher than $75,000, those who reported low income (less than $35,000) had lower odds of being WAT infrequent (OR: .18, 99.997% CI: .03, 1.14) and frequent (OR: .20, 99.997% CI: .04, .98) users. In the before COVID-19 subgroup, compared to older adults who reported annual household income higher than $75,000, those reported low income (less than $35,000) had lower odds of being WAT infrequent (OR: .14, 99.997% CI: .02, 1.18) and frequent (OR: .19, 99.997% CI: .03, 1.13) users. No statistically significant association was detected in the first wave of COVID-19 subgroup.
Discussion
In the present study, we examined the prevalence of WAT use in older adults before and during the first wave of the COVID-19 pandemic and examined sociodemographic factors associated with older adults’ use of WATs. The prevalence of WATs use was low in this sample of older adults in the U.S. We found that only 10.3% of older adults pre-COVID-19 and 10.9% of older adults during first wave of COVID-19 were frequent WAT users. In the total sample and pre-COVID-19 subsample, older adults aged between 65 and 74 years were more likely to be frequent WAT users after adjusting for covariates. Lower income was associated with lower odds of frequent WAT use. No significance was found between social factors and older adults frequent use of WATs in the first wave of COVID-19 subsample. After Bonferroni’s correction, income remained to be the only social factor statistically significantly associated with frequency of WAT use.
Currently, there is limited understanding of WAT use in the aging population. However, the use of WATs is especially important in the older adult population as WATs and WAT-based interventions have demonstrated the ability to significantly improve physical activity levels which can further help users achieve better health through lowering of risks for cardiovascular disease, cancer, insomnia, poor mental health, type 2 diabetes, and dementia (Colberg et al., 2010; Del Pozo Cruz et al., 2022; Kline, 2014; Myers, 2003; Ringeval et al., 2020; Sharma et al., 2006). The findings of this study provided valuable insight into social factors associated with older adults’ use of WATs. We found that annual household income and age were the two factors statistically significantly associated with U.S. older adults’ frequent use of WATs.
First, annual household income was statistically significantly associated with older adults’ WAT use frequency. Previous research has reported that the adoption of digital tools and applications was associated with the users’ income in the adult population (Chandrasekaran et al., 2020; Sheon, 2018) and a previous article demonstrated that financial cost was a key factor that influences older adults’ willingness to purchase a WAT device (Rosales et al., 2018). Like other commercially available digital devices, most WATs require an Internet connection and other digital tools such as smartphones for data synchronization. Therefore, users need to afford the Internet, a smartphone, and a WAT device to utilize a WAT device (Tedesco et al., 2017). It has been reported that seniors who are older, less affluent, or with lower levels of educational attainment are expected to have less experience using digital technology, including WATs (Alley et al., 2016; Macridis et al., 2018). In addition, after Bonferroni’s correction, annual household income remained to be the only social factor statistically significantly associated with frequent WAT use. The findings of this study further emphasized the importance of enhancing WAT access and adoption in older adults, especially those with lower income to prevent further perpetuating health disparities. Currently, limited research examines the health benefits of WAT-facilitated interventions in low socioeconomic status populations. It is unclear whether current WAT-facilitated interventions among older adults with lower socioeconomic status may achieve the same level of effectiveness as in the general older adult population. Therefore, future research should focus on finding effective ways to promote both WAT utilization and WAT-based intervention effectiveness among low socioeconomic status older adults to help promote beneficial health outcomes in this population.
Consistent with previous evidence, we found that a relatively younger age was associated with greater WAT use among older adults. Generally, age is negatively associated with the use of WATs: a survey in 2019 estimated that 25% of U.S. adults between 18–49 years of age reported using a WAT regularly; 17% of those 50 years of age and older reported using a WAT regularly (Vogels, 2020). In addition, current WAT studies often compare young adults with older adults (Xie et al., 2020), but no study has investigated WAT use within different subgroups of older adults. The present study focuses on WAT use among U.S. older adults, specifically comparing older adults between 65 and 74 years of age and older adults aged 75 and above (Lee et al., 2018; Little & Little, 2014). We compared these subgroups in that it is necessary to acknowledge the differences among each age group considering the development of technology in the past few decades. For example, the “Baby Boomers,” born between 1946 and 1964 (Hogan et al., 2008), are currently between the ages of 60 and 74 years. Reports have shown that this population embraces digital life and are more likely to adopt technology such as smartphones, social media, and use tablet computers than older adults 75 years and above (Vogels, 2019). This finding provides important guidance for future research and practice with an emphasis on meeting the needs of different age subgroups among older adults. For example, age-related capability of technology use should be considered, and more technological guidance may be provided for those aged 75 and above to avoid technology-related frustration; future interventions may be developed to meet health needs of different age groups.
In this study, the results of several social factors did not reach statistical significance in the association with WAT use, yet still provided important information. First, female sex has a higher odds ratio compared to male in both frequent (OR: 1.52) and infrequent (OR: 1.92) WAT use. This shows a potential trend of higher use of WAT in female older adults. Li et al. (Li et al., 2020) found that among an online panel of older adults, females were more likely to be long-term WAT users. Population-based surveys from both Canada and Australia report that, among general adults, females use physical activity-tracking devices more than males (Alley et al., 2016; Macridis et al., 2018), although males are more likely to use advanced trackers (Alley et al., 2016). A similar finding in terms of e-health utilization indicated that female adults were more likely than male adults to have ever looked for health information online or owned a mobile app for health (Escoffery, 2018). Findings from a national survey in the United States also showed that females were significantly more likely to report health information technology use than males (Hung et al., 2020). This could be related to the fact that women are more likely than men to actively seek health care. Another national survey in the US found that female older adults were more likely than male older adults to use mental health services (Karlin et al., 2008). A study focusing on health information-seeking behaviors in older adults found that females were inclined to have more control in health information retrieval and favorable attitudes toward self-directed or informed treatment (Chaudhuri et al., 2013).
Although race and ethnicity were not statistically significantly associated with frequency of WAT use, in the total sample, non-Hispanic African American older adults had a higher odd’s ratio compared to non-Hispanic White older adults of being WAT frequent users (OR: 2.57, 97.5% CI: .68, 9.69). In accordance with this result, Pew Research Center reported higher WAT use among African Americans: approximately 23% of Black U.S. adults and 20% of White U.S. adults reported regular use of a WAT in 2019 (Vogels, 2020). Evidence suggests that the trend in differences between race and ethnicity in WATs could be explained by different acceptance of data sharing: White adults are more likely than Black and Hispanic adults to find it unacceptable to share WAT data for research (Vogels, 2020). Other underlying explanations of racial and ethnic differences in WAT use among U.S. older adults should be explored in future studies.
The present study is one of the first studies to additionally observe frequency of WAT use in a nationally representative dataset. Studies have investigated older adults’ adherence to using WATs as part of a study in which participants were provided devices and asked to wear them (Junxin Li et al., 2021; Li et al., 2022; Paolillo et al., 2022). Few studies that focused on older adults’ WAT use considered user frequency (Li et al., 2019). A survey in Japan estimated that about 58% of female and 68% male users used a WAT every day, 14% of female users in Japan used WATs only once a week (Statista, 2022). No studies have been found to present U.S. older adults’ frequency of WAT use based on national data. In the present study, we found that, among older adults who do use WATs, only 65.5% used WATs frequently and about one-third of WAT users used the technology only occasionally, which could lead to decreased health benefits from using WATs. The reasons for low adherence to WAT use could include forgetting to wear the device, forgetting to charge the device, and having difficulties with synchronizing the device or operating the device (Li et al., 2022). Therefore, training demonstrating the health benefits of using WATs, with detailed instructions on WAT operation, charging, and synchronization designed for the aging populations should be included in future research.
Several limitations exist in the present study. First, in the HINTS survey, Cycle 4 data were collected between February and June 2020. The COVID-19 pandemic started in March in the U.S.; therefore, the data reflecting the COVID-19 pandemic were available only from March to June. This means that the data represent the start and first wave of COVID-19 and do not provide changes in WAT use patterns throughout the pandemic. Additional studies are needed to explore the WAT use changes considering the entire COVID-19 progression. Second, because of the short period of data collection during COVID-19, limited subgroup data (627 participants since the start of COVID-19) made it difficult to conduct statistical analyses. Therefore, we did not aim to compare changes in WAT use before and during COVID-19, but instead presented the available data to show the within-sample prevalence of WAT use. Additionally, other factors that may impact the frequency of WAT use, such as cognitive function, perceived ease of use, interest/acceptance of technology, etc. (Adapa et al., 2018; Dai et al., 2020; Wang et al., 2020), were not assessed in the HINTS data.
The findings of the present study provide important implications for future WAT-related research and policy. The inequality of WAT use among older Americans needs to be addressed to foster equal access to WATs among older Americans. As Sieck et al. stated (Sieck et al., 2021), improved access to digital devices in diverse communities with different socioeconomic levels is needed to avoid the risk of digital technologies becoming another social determinant of health. Future WAT-based interventions should focus on the inclusion of low-income older adults and tackle health disparities among older Americans.
Conclusion
In this study, we examined the prevalence of WAT use before and during the first wave of COVID-19, and explored social factors associated with WAT use frequency among older adults in the U.S. Our findings suggest disparities in WAT use among older adults aged 75 and above and with low income. The study highlights the importance of promoting WAT use among the aging population with a focus on socioeconomic status. Future study directions include understanding the feasibility and preliminary efficacy of WAT-based interventions in low-income older adults and further understanding the impact of the COVID-19 pandemic on WAT use among older adults.
Supplemental Material
Supplemental Material - Social Factors and Older Adults’ Use of Wearable Activity Trackers: Before and During the First Wave of the COVID-19 Pandemic
Supplemental Material for Social Factors and Older Adults’ Use of Wearable Activity Trackers: Before and During the First Wave of the COVID-19 Pandemic by Mengchi Li, Jing Huang, Chakra Budhathoki, Qiwei Li, Laura Samuel, Sarah L. Szanton, Jennifer A. Schrack, and Junxin Li in Journal of Applied Gerontology
Footnotes
Acknowledgment
We would like to express our special thanks of gratitude to Johns Hopkins University School of Nursing Center of Innovative Care Pilot Grant Program for supporting this work. We would like to thank the National Cancer Institute for providing the Health Information National Trends Survey data.
Author Contributions
Junxin Li provided mentorship for Mengchi Li on this manuscript. Mengchi Li, Jing Huang, MPhil; Chakra Budhathoki, and Qiwei Li analyzed and interpreted the data. Mengchi Li and Jing Huang wrote the first draft of the manuscript and structured the tables. Junxin Li, Laura Samuel, Sarah L. Szanton, and Jennifer A. Schrack provided additional guidance on revisions after the first draft. All authors reviewed the draft, contributed on the revisions, and approved the final version of the report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Johns Hopkins University School of Nursing Center of Innovative Care Pilot Grant Program and National Institute of Nursing Research R00NR016484.
IRB Approval
This study was exempted for the Protection of Human Subjects because we only used public-available and de-identified data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.