
Abstract
Annual Wellness Visits (AWV) promote preventive care for older adults, yet uptake remains low. To increase AWVs, a Medicare Advantage (MA) plan in Puerto Rico contracted a medical group to provide home-based AWVs during the last quarter of 2020. Using data from 464 visits, we conducted descriptive and multivariable analysis to profile patient characteristics and identify predictors of mental health referrals. We found that 87% of patients had multiple chronic conditions, 75% were taking more than 5 medications, and the odds of a mental health referral were higher for those who also had a nutrition-related condition (AOR = 5.05, CI95: 1.76–11.88), diabetes (AOR = 3.34, CI95: 1.18–7.58), or an additional reported uncontrolled health issue (AOR = 28.18, CI95: 8.96–70.59). This strategy helped one MA plan reach high-need patients, but coordination of follow-up care is needed to ensure patients receive recommended services.
• The study is the first to explore contracting with a private medical group to provide home-based Medicare Annual Wellness Visits. • Patients visited at home had high rates of multimorbidity and polypharmacy and those with a nutrition-related condition or diabetes were more likely to receive a mental health referral. • This study responds to the limited research literature on Medicare services in Puerto Rico by documenting the health needs of beneficiaries with limited access to care and the efforts used by managed care to reach them.
• Offering in-person or telehealth visits in patients’ homes may help Medicare Advantage plans reach older adults with clinical and social risks. • Interventions that include ongoing coordination of follow-up care should be considered to ensure patients receive needed services. • Future research should investigate whether home-based Annual Wellness Visits improve the quality of preventive care and linkages to specialty care.What this paper adds
Applications of study findings
Introduction
Medicare Advantage (MA) plans in Puerto Rico enroll the highest percentage of Medicare beneficiaries of any U.S. state or territory (Ochieng et al., 2023). Yet, Puerto Rican enrollees have higher rates of chronic disease and depression than those on the mainland (Matos-Moreno et al., 2022; Ng et al., 2017; Rivera-Hernandez et al., 2016). Meanwhile, providers receive lower reimbursement from the Centers for Medicare and Medicaid Services (CMS) and natural disasters like 2017’s Hurricane Maria have led to widespread provider shortages, particularly in primary and mental health care (Assistant Secretary for Planning and Evaluation, 2017; Health Resources and Service Administration, 2023).
Annual wellness visits (AWV), introduced as part of the Affordable Care Act, have the potential to help Puerto Rican MA plans promote healthy aging while compensating for lower funding from CMS. AWVs include the key components of a geriatric assessment, a depression screening, and a wholistic discussion of patients’ conditions, providers, risk factors, and needs for preventive or follow-up care in a single visit (Tatum et al., 2018; Annual Wellness Visits, 2011). To encourage AWVs, CMS allows visits to occur in patients’ homes, and since COVID-19 via telehealth. For MA plans, completing AWVs can also help them meet quality-based metrics used to calculate pay-for-performance bonuses, and offset lower payments from CMS (Roberts & Song, 2022). However, despite these incentives and evidence that AWVs increase access to preventive services, uptake remains low (Farford et al., 2021; Ganguli et al., 2017).
In this descriptive study, we examine one strategy used by an MA plan operating in Puerto Rico to increase AWVs: contracting with a private medical group to conduct in-person or telemedicine visits in enrollees’ homes during the first year of the COVID-19 pandemic. We profile the enrollees reached through this strategy, with a focus on chronic conditions and their risk factors. Also, given the unmet need for mental health services on the island (Canino et al., 2016) and that referrals from a health care provider encourages use of mental health services (Ledoux et al., 2009), we examine potential predictors of receiving a mental health referral during the AWV.
Methods
An MA plan operating in Puerto Rico identified 1363 enrollees who had not had an AWV by the start of the last quarter of 2020. Identified enrollees were located across the island, but notably 844 (62%) lived in the Southern or Western regions, which contain many rural communities in mountainous and remote areas characterized by geographic isolation, limited transportation, and provider shortages. The MA plan contracted with a private medical group to try to complete home-based AWVs with these enrollees. The group contacted 601 and completed visits with 464. Reasons for declining the AWV among those contacted included being off the island at the time, wanting to be seen by their regular primary care provider, and discomfort with technology or having clinical personnel in their home. We extracted demographic and health data from deidentified, scanned copies of health assessment forms filled-out by the physician or physician assistant who conducted the visit. Data on health conditions included condition type (diabetes, kidney, cancer, nutrition, cardiovascular, mental health, or respiratory), whether the patient had any other controlled or uncontrolled health issues, and the treatment plan for each condition or issue identified. We coded treatment plans that included follow-up care for the condition as a referral. The research protocol was approved by the New York University Institutional Review Board (# FY2021-5612).
Statistical Analysis
We calculated descriptive statistics for all variables and used independent t, Mann Whitney U, and chi square tests to compare enrollees with and without a mental health condition. We used multiple logistic regression to estimate associations between potential predictors and the odds of having a documented mental health condition and, for the sub-sample with a mental health condition, the odds of having a referral. To address high homogeneity within clusters (patients with the same provider) in the odds of having a mental health referral and the small size of several of the clusters, we fit a Bayesian multilevel model for the sub-group analysis using the bayes and melogit commands in STATA 15.1 (Stata Corp, 2017).
Results
Characteristics of all Enrollees who Received an AWV and Enrollees With and Without a Diagnosed Mental Health Condition Who Received an AWV.
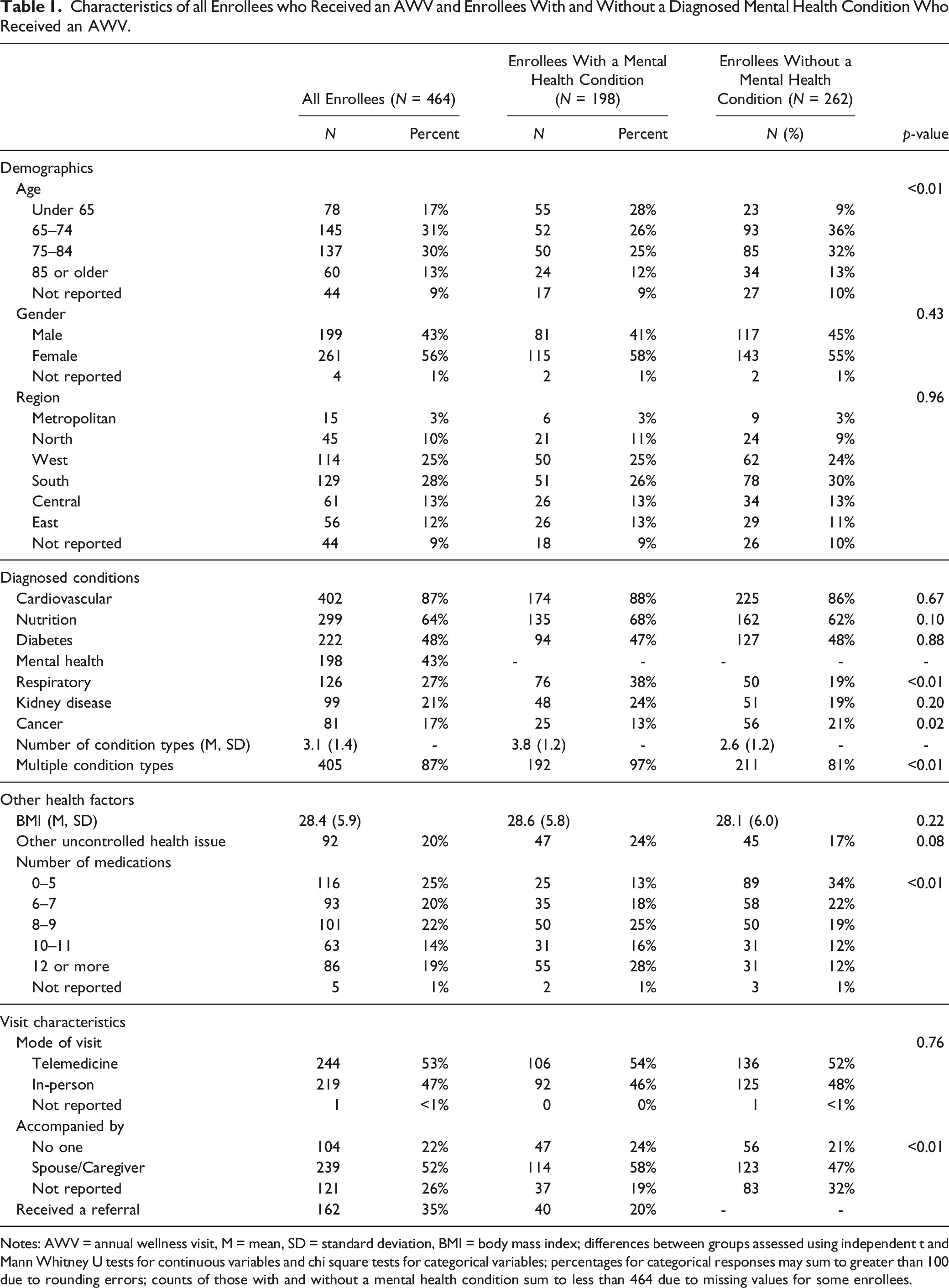
Notes: AWV = annual wellness visit, M = mean, SD = standard deviation, BMI = body mass index; differences between groups assessed using independent t and Mann Whitney U tests for continuous variables and chi square tests for categorical variables; percentages for categorical responses may sum to greater than 100 due to rounding errors; counts of those with and without a mental health condition sum to less than 464 due to missing values for some enrollees.
Associations Between Enrollee and Visit Characteristics and the Odds of Having a Documented Mental Health Condition and With the Odds of Having a Mental Health Care Referral.
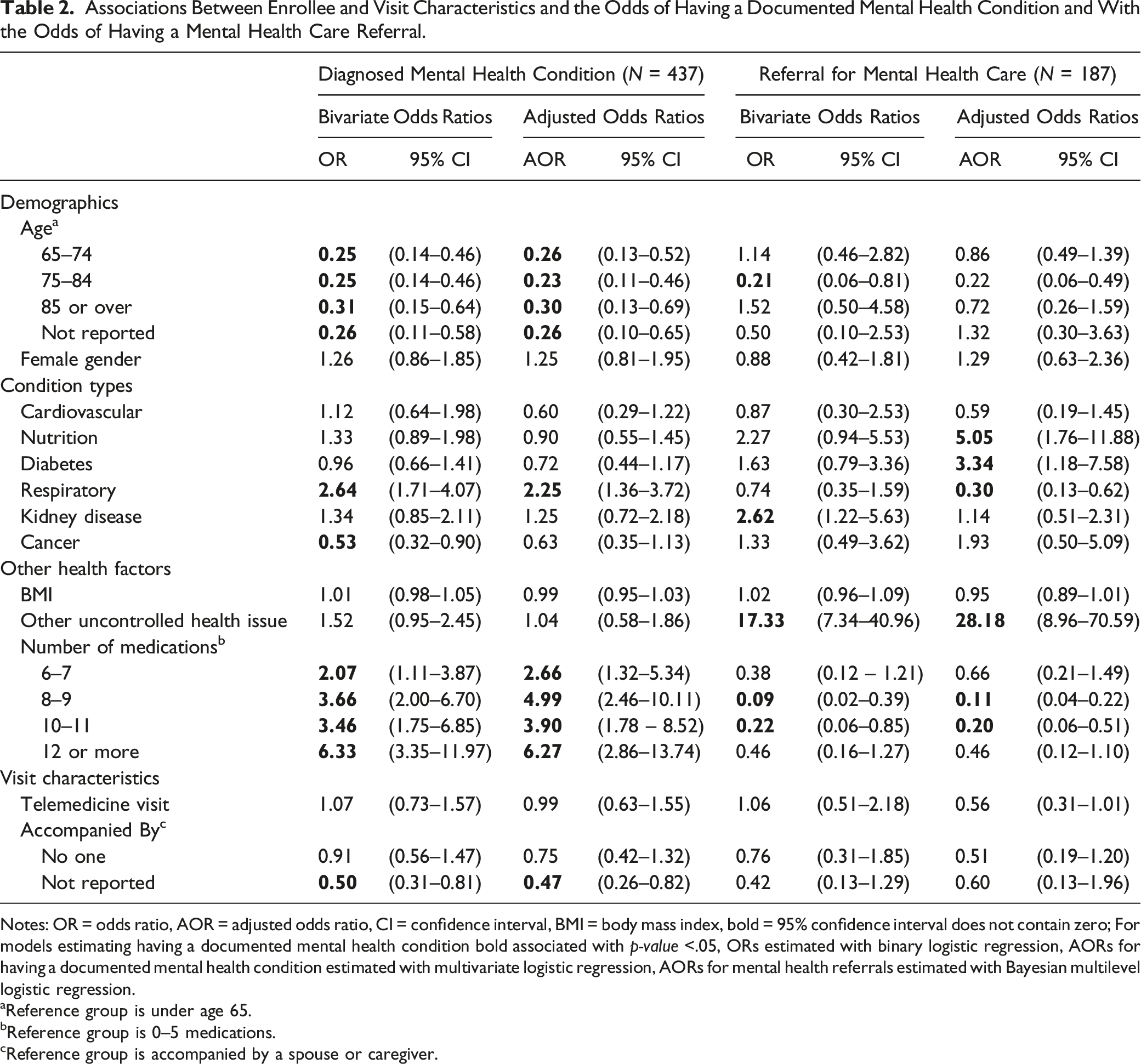
Notes: OR = odds ratio, AOR = adjusted odds ratio, CI = confidence interval, BMI = body mass index, bold = 95% confidence interval does not contain zero; For models estimating having a documented mental health condition bold associated with p-value <.05, ORs estimated with binary logistic regression, AORs for having a documented mental health condition estimated with multivariate logistic regression, AORs for mental health referrals estimated with Bayesian multilevel logistic regression.
aReference group is under age 65.
bReference group is 0–5 medications.
cReference group is accompanied by a spouse or caregiver.
Enrollees with a mental health condition (n = 198) were nested within 11 providers from the contracted medical group. An initial single-level logistic regression model with no predictors had an intraclass correlation of .513 and cluster sizes ranging from 1 to 50. To accommodate some small cluster sizes and high homogeneity within clusters, we then fit a multilevel Bayesian model using an analytic sample of 187 observations with complete data on all predictors (see Table 2). The analytic sample contained 10 clusters ranging from 2 to 43 patients, with a mean size of 18.7. In the final model, the estimated odds of referral were higher among those who also had a nutrition-related condition (AOR= 5.05, CI95 = 1.76–11.88), diabetes (AOR= 3.34, CI95 = 1.18–7.58), or another uncontrolled health issue (AOR= 28.18, CI95 = 8.96–70.59). The estimated odds were lower among those ages 75–84 (AOR = .22, CI95 = .06–.49), those with a respiratory illness (AOR = .30, CI95 = .13–.62), and those taking six to seven or eight to nine medications (AOR = .11, CI95 = .04–.22; AOR = .20, CI95 = .06–.51, respectively). Readers should note the large confidence intervals for some coefficient estimates, particularly having another uncontrolled health issue, and use caution when interpreting results.
Discussion
In Puerto Rico, COVID-19 exacerbated pre-pandemic health and socioeconomic disparities caused by the cumulative effects of repeated natural disasters, income inequality, outmigration, government austerity policies, and underfunded health care systems (García et al., 2021). For older adults, these structural factors have led to nearly 40% of them living in poverty (U.S. Census Bureau, 2021), reduced social and caregiving support due to outmigration of working-age children and other adults, and reduced access to primary care providers (Matos-Moreno et al., 2022). Older adults on the island continue to be at risk of social isolation, cognitive decline, and increased functional limitations (Matos-Moreno et al., 2022) and health care strategies are urgently needed to help older patients traverse aging-related barriers to care. Our study finds that one MA plan’s strategy of contracting a medical group to reach patients at home connected vulnerable older adults to a primary care service they likely would not have gotten otherwise. Expanding or adapting home-based models such as this has the potential to improve the responsiveness of the island’s health care system to the needs of a rapidly aging population, particularly patients without sufficient social or financial resources to travel to appointments or adhere to treatment plans.
Our study extends prior research on in-person home and telemedicine visits which find they can benefit older adults who are underserved, homebound, or have debilitating conditions (De Jonge et al., 2014; Han et al., 2017), although, to our knowledge, this is the first study to examine contracted providers and home visits with patients in Puerto Rico. However, unlike other programs that include coordination of follow-up visits, our study could not confirm whether enrollees referred for additional services actually received them. Our findings also align with studies suggesting AWVs may assist MA plans with revenue generation as documenting chronic conditions during AWVs can increase risk scores for enrollees and therefore future payment rates (Cuenca & Kapsner, 2019; Jacobs & Kronick, 2021). Future research should examine how using home-based AWVs impacts receipt of follow-up care and if documentation of health conditions during AWVs results in better management of those conditions.
Study Limitations
Our study does not include data on follow-up visits, nor were we able to determine whether conditions recorded as part of the AWV reflect coding intensity. We also did not have access to data to determine if visited enrollees were systematically different from other enrollees in the plan. Lastly, our study was conducted during 2020 when the COVID-19 pandemic may have limited access to medical appointments for MA beneficiaries. Still, given the scant data available on health care and MA plans in Puerto Rico (Medicaid and Medicare Advantage Products Association of Puerto Rico, 2022), this study provides valuable insight into the needs of these patients and strategies used to address them.
Conclusion
High-need MA enrollees with multiple chronic conditions may benefit from flexible outreach strategies that offer home-based AWVs. However, additional and ongoing coordination of follow-up care may be required to ensure patients receive the care they need.
Footnotes
Acknowledgments
Sofia Palacios received support for this research from a grant from the New York Academy of Medicine. We wish to thank Dr. Reynaldo Pezzotti, MD, and Madeleine Cruz of Solutions Medical Group, PSC for sharing the data that served as the basis for this study. The research presented in this paper is that of the authors and does not reflect the opinions of the funders or other organizations acknowledged here.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Sofia Palacios received support for this research from a New York Academy of Medicine Margaret E. Mahoney Fellowship grant.
IRB Approval
New York University Institutional Review Board (FY2021-5612).