
Abstract
• This paper provides administrators’ perspectives on the process of PDPM implementation in skilled nursing facilities (SNFs). More thorough patient assessment and documentation were emphasized • Administrators reported instituting staffing changes to better match patient needs; reductions in therapists seemed concentrated among contract employees • SNF administrators considered the role of increased incentives to admit patients with more complex needs in their preparation for the PDPM
• In implementing the PDPM, SNFs focused on assessment and documentation to identify patient acuity and maximize associated reimbursement levels. Policy makers should proactively consider how payment methods best compensate the actual cost of providing enhanced services • The effect of the PDPM on therapy staff levels in SNFs should continue to be examined as group therapy is encouraged under the PDPM. Incentives for SNFs should be modified accordingly • The PDPM increased incentives to admit patients with more complex needs. Policy makers should monitor SNF admission criteria closely to ensure the range of acuity in patients continues to be matched with appropriate careWhat this paper adds
Applications of study findings
Introduction
In addition to providing long-term services to residents typically funded by Medicaid, skilled nursing facilities (SNFs) provide short-term skilled nursing and rehabilitation services to patients after a stay in an acute care hospital. In 2019, 15,000 SNFs in the United States (U.S.) provided services for 4% of Medicare’s fee-for-service (FFS) beneficiaries, at a cost of US$27.8 billion (MedPAC, 2021). From July 1998 to September 2019, SNFs were reimbursed by Medicare using the Resource Utilization Group (RUG) system, with reimbursement largely based on the amount of therapy provided, rather than on the level of illness or special care needs of patients. This created an increased financial incentive for SNFs to provide more therapy to patients. In 2011, a Medicare Payment Advisory Commission (MedPAC) report identified a series of inefficiencies under the RUG system for SNFs. One of these inefficiencies included a lack of adequate adjustments to reflect variation in provider costs for services beyond therapy such as nontherapy ancillary services, including supportive or diagnostic measures like lab testing and wound care (MedPAC, 2011). Patients whose care is paid by Medicare generated the highest revenue for SNFs, with reimbursements of nearly US$500 per person per day, compared to US$300-US$400 for privately insured patients or less than US$200 for Medicaid recipients (LuRui & Seidmann, 2018). In 2018, MedPAC findings highlighted a near doubling of SNF spending between 2003 and 2016 (MedPAC, 2018). Consequently, SNF reimbursement became a major target of policy reform by Medicare. In October 2019, the Centers for Medicare and Medicaid Services (CMS) implemented a new SNF Prospective Payment System (PPS) model throughout all Medicare certified facilities nationwide, named the Patient Driven Payment Model (PDPM), in an attempt to reduce spending and balance incentives.
The PDPM was announced in July 2018, and implemented in October 2019 resulting in SNFs having just over a year to analyze and prepare for the new payment model. As the PDPM shifted reimbursement methodology, it also created the potential for significant operational changes for SNFs with respect to documentation, training, patient care, and staffing mix. The more stringent admission documentation and, therefore more detailed clinical assessment requirements, meant that the PDPM system relied on accurately coded patient medical conditions to optimize payment and determine eligibility for reimbursable skilled services (Centers for Medicare and Medicaid Services CMS, 2023). Training staff to ensure proper coding became increasingly important. Additionally, under the PDPM, SNFs are financially incentivized to admit a case mix of more clinically complex patients, as they can bring greater reimbursement (Makam & Grabowski, 2021). In order to provide adequate care for a more medically complex cohort of patients, SNFs needed to reevaluate their staffing mix and provide staff training to accommodate the greater clinical needs of the patients they serve.
Another potential operational change from the PDPM is in terms of therapy. Since the amount of therapy is no longer a key driver of payment within the PDPM, providing less therapy reduces costs for SNFs. Concurrent or group therapy can be seen as a more favorable option as it uses fewer resources and has direct cost-savings compared to individual therapy sessions. In addition, the PDPM gives therapists flexibility in determining the size of therapy groups, from exactly four patients to a range of two to six (Zhang et al., 2022). These potential implications for overall operational costs and staffing are thus considerable and far-reaching (Brady & McKittrick, 2021).
Existing quantitative research has found evidence of the impact of the PDPM on therapy utilization and therapy staffing in SNFs. A cross-sectional study of patients admitted to a SNF after hip fracture between January 2018 and March 2020 found a significant reduction in therapy volume (Rahman et al., 2022). Another study found that SNFs appeared to have responded to the PDPM with both immediate and gradual reductions in therapy staffing, with an average decline of 80 therapy staffing minutes over the average patient stay of 25 days. In the first six months after the PDPM implementation, this equates to an immediate decline of about 30 min of therapy staffing per patient stay, or the duration of 1 typical therapy treatment session. Of all the types of therapy staff, assistant and contract staff experienced the most immediate declines (Prusynski et al., 2021). While these findings suggest that the PDPM did have its intended effect of altering financial incentives for SNFs related to therapy provision, research is needed to examine the underlying mechanisms for how these early findings regarding reductions in therapy volume and staffing were achieved. Of note, the emergence of the COVID-19 pandemic in the beginning of March 2020 impacted the execution of the PDPM, including by placing constraints on the use of group therapy. To the best of our knowledge, there is no prior qualitative examination of the implementation and outcomes of the PDPM at SNFs prior to COVID-19. No existing research has examined SNF efforts to prepare for the PDPM, or focused qualitatively on changes that occurred as a result of the PDPM. Findings from this descriptive qualitative study provide context for quantitative studies reporting the impact of the PDPM on Medicare certified SNFs. The purpose of this paper is to explore SNF administrator perspectives on the process of implementing a new payment model, the PDPM, at their facilities.
Methods
Data included in this paper are drawn from the qualitative arm of a large, mixed-methods research study that aimed to examine the implementation and outcomes of the PDPM, as well as the impact of the COVID-19 pandemic on skilled nursing facilities. The qualitative arm included repeated, semi-structured qualitative interviews with administrators in 40 SNFs in eight healthcare markets across the United States. SNF administrator perspectives were gathered regarding the preparation for and early implementation of the PDPM from July 2020 through December 2021, after the policy was initially enacted. This paper considers preparation for the PDPM as the time from when the policy was announced to when the policy went into effect, and implementation from after the policy went into effect until the start of COVID-19, around February and March 2020. See [anonymized for peer review] for additional information on the methods.
Sample Selection and Administrator Recruitment
Markets were selected to reflect different nursing home utilization patterns. Hospital Referral Region (HRR) table from the Centers for Medicare and Medicaid (CMS) 2017 Geographic Variation Public Use File were used to identify all beneficiaries and the percent of Medicare beneficiaries within an HRR that had any post-acute nursing home use in the year 2021 (Centers for Medicare and Medicaid Services CMS, 2023). This population-level measure of nursing home use incorporates a region’s propensity to use hospital care, and rank orders HRRs to identify areas with varying rates of nursing home use. HRRs were separated into four categories of nursing home utilization: 1–75 (nursing home use ranged from 1.36% to 4.03%), 76–150 (4.04%–4.67%), 151–225 (4.68%–5.37%), 225–306 (5.38%–7.44%).
2018 data from the Certification and Survey Provider Enhanced Reporting (CASPER) system were used to generate a list of every SNF in the eight markets, along with each SNF’s bed count, percent of Medicare-paid patients, and profit status. SNFs’ overall quality star rating (1–5) was linked using federal provider numbers. SNFs with fewer than 50 beds or less than five percent of their patients paid for by Medicare were excluded because we sought facilities that we expected would be most affected by implementation of the PDPM (more patients, and more patients subject to reimbursement changes under the PDPM). From each market, five SNFs varying in size, profit status, quality, and payer mix were recruited.
In an innovative strategy to capture SNF administrators’ developing perspectives over the course of approximately one year, administrators were recruited by email or telephone to participate in a series of four interviews, spaced three months apart. Administrators were identified by the facility’s website, if possible, and when we called to obtain or verify their contact information. In instances when an administrator left a facility, we followed the SNF over the study period by continuing the interviews with the incoming administrator. Study materials were sent to the Brown University IRB for review and determined to not be human subject’s research.
Interview Protocol Design and Piloting
The qualitative team developed interview guides with questions designed to examine how the implementation of the PDPM was carried out and how it impacted SNFs, including the delivery of therapy. Our questions focused on eliciting administrator perspectives on strategies used to prepare for and implement the PDPM, and the impact of the PDPM on their daily operations, staff, and residents. While outside the scope of this paper, the interview guide also included questions focused on the impact of the COVID-19 pandemic on SNFs. We conducted three cognitive interviews to test the flow, clarity, and comprehension of the interview guide and made revisions based on the feedback we received. Pilot interviews were conducted with three SNF administrators to further test our interview guide, resulting in final revisions to our questions. While each of the four interviews followed the same structure and included the same core questions, interviews two through four were modified as appropriate to follow-up on information discussed in prior interviews. Questions and probes were also added or discontinued as needed over time. The interview guide for the fourth round of interviews included reflective, “look-back” framing of the primary questions to explore new information over time.
Interview Procedures
Interviews with SNF administrators were conducted from July 2020 to December 2021. Interviews were repeated at three-month intervals (or as close to that timeframe as possible) throughout the study period. Each interview lasted approximately 60 min and, based on participant preference, was conducted either virtually or by phone. Two qualitative team members were present during the interviews: one conducting the interview and the other taking notes. Participants provided consent to audio record at the beginning of each interview. At the end of each interview, the next interview was scheduled for three months in the future, for a total of four interviews per SNF. Participants were emailed an incentive for each interview they took part in. Audio files were professionally transcribed, then reviewed, corrected, and de-identified by team members.
Research Team and Reflexivity
The interviews for the study were conducted by a team of four, comprising of two PhD-level faculty members and two Master’s level staff, all of whom were female and had extensive experience (5–35 years) in conducting qualitative research. The team had no prior relationships with the interview participants but developed working relationships with them over the course of four interviews conducted over the one-year period. The team shared the purpose of the research with the participants during recruitment and at the start of each interview.
Method of Analysis
Interview transcripts were qualitatively analyzed using a modified grounded theory approach (Alnsour, 2022; Strauss & Corbin, 1994). First, a preliminary coding scheme was developed based on interview questions. Each of the four members of the analytic team independently applied the coding scheme to the same transcripts, then met to discuss and revise the coding scheme iteratively to add/delete codes, and refine definitions. Once a high level of agreement was reached, four researchers, in teams of two, independently coded transcripts and reconciled coding differences. Coding pairs rotated for coding rigor and consistency. Overarching themes recurring across interviews were identified and discussed weekly by the whole team (Braun & Clarke, 2006). After reconciling 84 transcripts using these methods, and a high level of coding consistency was reached, the remaining transcripts were then divided such that one in every three was coded by rotating pairs and the rest were individually coded by one member of the team. During analysis, it was determined that saturation was achieved (Saunders et al., 2018). The qualitative software package NVivo Version 12 Plus (QSR International) was used. During analysis, the team kept a comprehensive audit trail to record decisions, questions and comments, code definitions, and emerging themes (Ritchie et al., 2013). For additional information about our methods, see Gadbois et al., 2022.
Results
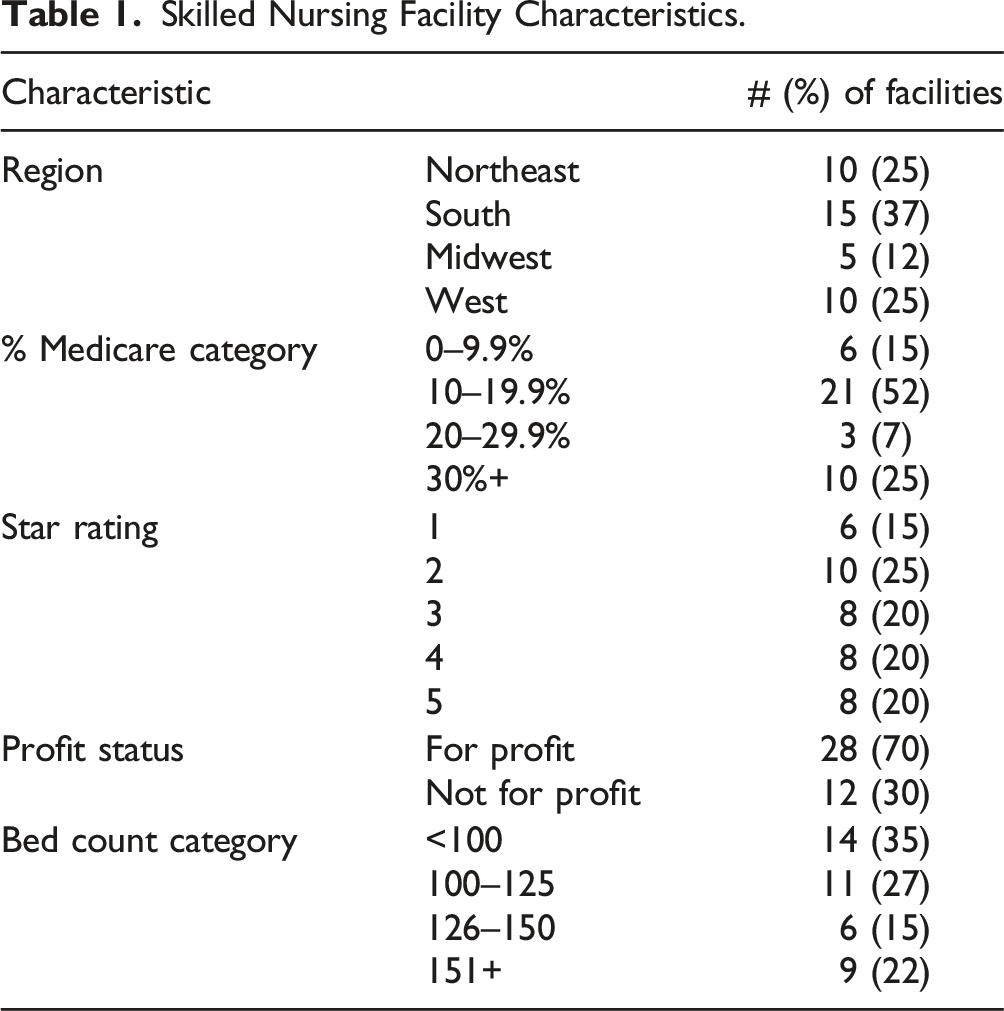
Skilled Nursing Facility Characteristics.
We identified common themes across interviews as we learned about the varied administrator experiences in preparing for and implementing the PDPM. First, reflecting back to the initial period of the PDPM implementation, most administrators reported feeling adequately prepared for the transition. Second, administrators described substantial advanced preparation from the time of the announcement of the PDPM in July 2018, until it’s implementation in October 2019, which included training provided either internally or through contracting with outside organizations. Third, in addition to training, administrators discussed modifications they made to staffing models to prepare for the PDPM. Last, administrators reported staffing reductions among contract employees, while maintaining basic and continuing patterns of therapy delivery and SNF-employed therapist staffing.
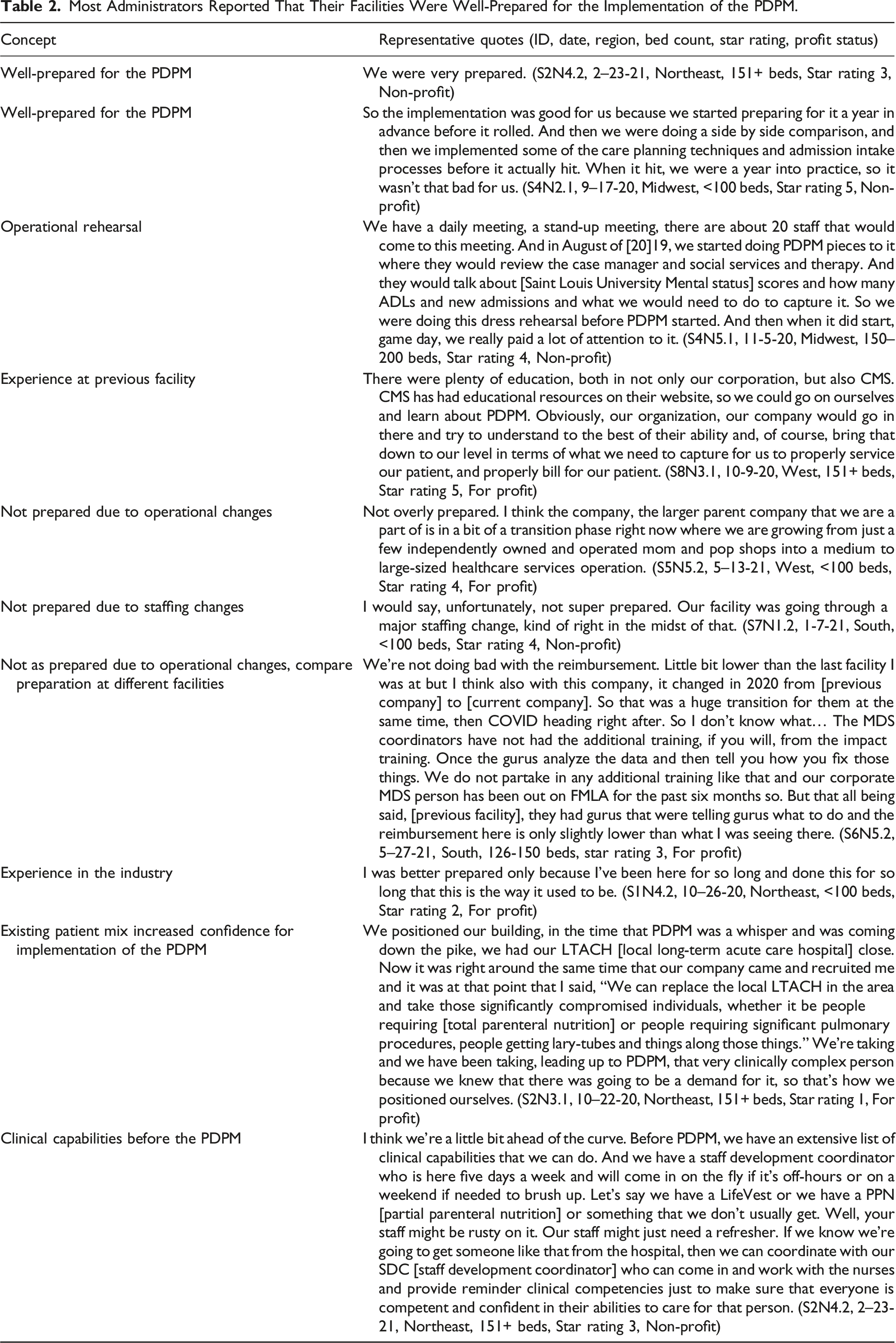
Most administrators reported that their facilities were well-prepared for the implementation of the PDPM. Nursing home administrators were asked how prepared they felt their facilities were for implementing the PDPM in October 2019, and the majority responded positively, expressing that they were “very prepared” (S2N4.2). One of them noted: I think we were really prepared. I mean, I would say on a 10-point scale, I'd say probably a nine or something like that. We have really strong corporate support and especially one individual who's just very, very knowledgeable and just helped distill everything for us. We did send our MDS staff up to the corporate office to receive training and then there were many regular updates and that type of thing, so yeah, I would say we were very well-prepared. (S6N2.2) To ensure smooth transitions, facility wide education was commonly discussed. Some skilled nursing facilities conducted operational rehearsals before the official implementation, which consisted of a gradual shift in coding and documentation for an extended period of time before the official implementation date. Some of the administrators included in the interviews had only worked at their respective facilities for a few months, and assessed their current facility’s preparation level compared to their prior experience at a different facility. They reported similar strategies for the PDPM implementation at their previous facilities. One administrator pointed out: “I felt like I was really well trained for PDPM. I think I shared with you before, the company I worked for previously was really on top of it. I feel like I'm really prepared, and my team is doing pretty well. I would say this building the staff here weren't as prepared as I would've liked to see them, but I have a new MDS coordinator, and she really gets it, and she's doing a great job.” (S6N3.3) Few administrators reported feeling “not super prepared” (S7N1.2) for the PDPM, often due to unrelated transitions of ownership or staffing. In addition, administrators’ experiences with previous payment reforms, staff members’ clinical capabilities, and existing patient case mix were also discussed as factors influencing administrators’ levels of confidence regarding implementing PDPM. See Table 2 for representative quotes.
Most Administrators Reported That Their Facilities Were Well-Prepared for the Implementation of the PDPM.
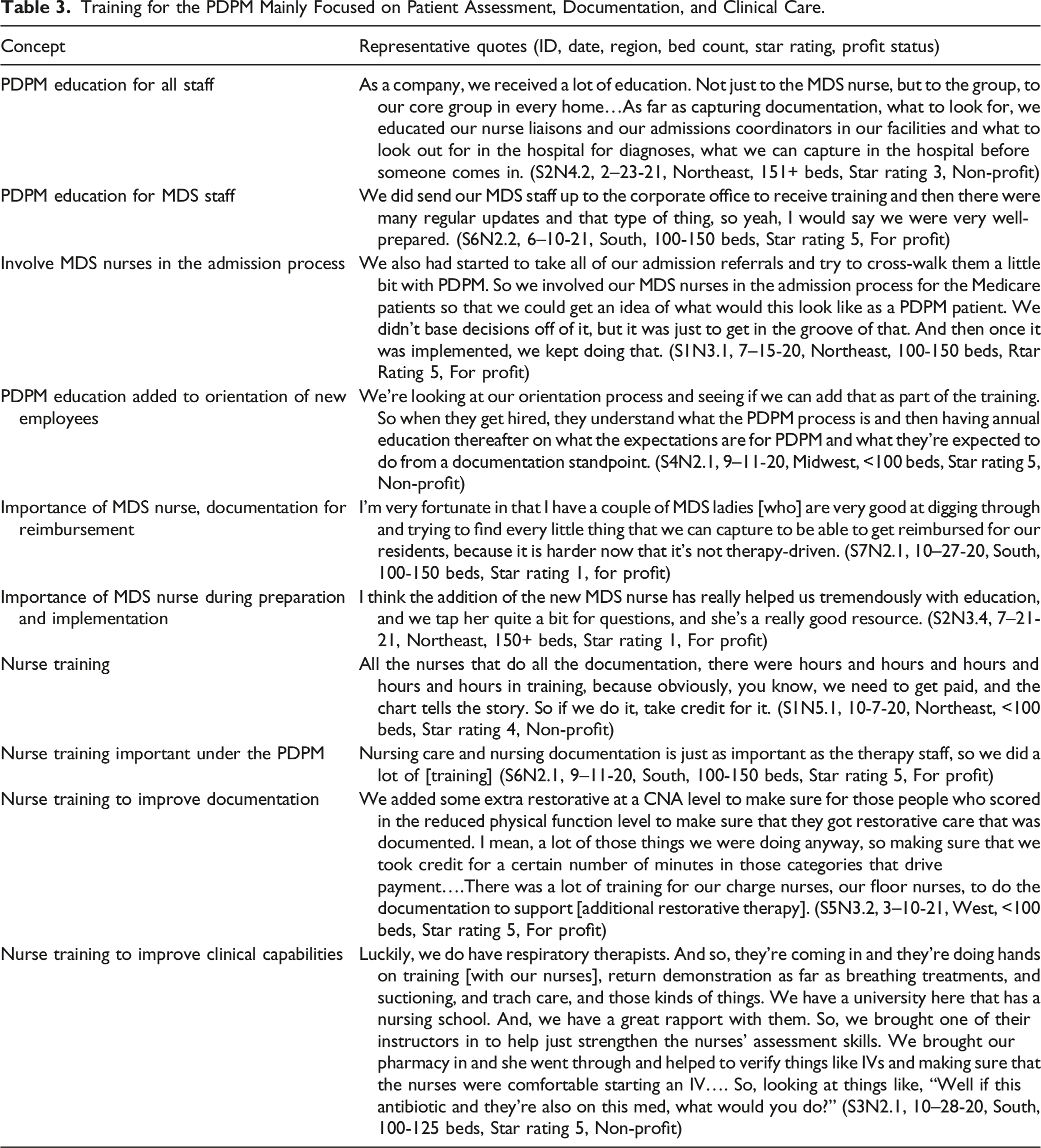
Training for the PDPM focused on patient assessment, documentation, and clinical care. Administrators described the technical training they received in preparation for the PDPM, to optimize thorough patient assessment and documentation. According to administrators, most SNFs provided extensive education regarding the PDPM to all staff, particularly those responsible for coding and reimbursement, such as the Minimum Data Set (MDS) nurse. In general, education, provided internally or externally, ensured that all staff would have some understanding of the PDPM. For new employees, some administrators discussed how they added PDPM education as part of the orientation training. The importance of training MDS coordinators was highlighted as key to a smooth transition to the PDPM. As one administrator explained: “We have an MDS nurse who really embraced PDPM. It had made it very easy for our team as a whole to embrace it. She’s very thorough, and knows the questions to ask, what to look for” (S6N4.4). One administrator talked about involving “MDS nurses in the admission process for the Medicare patients” prior to the implementation of the PDPM to “get an idea of what would this look like as a PDPM patient” (S1N3.1). Having the MDS nurse involved in admissions was found to be beneficial during the preparation for and implementation of the PDPM. In addition to MDS staff training, administrators also discussed extensive training for nursing staff, which included patient assessment, documentation, and clinical care. One administrator explained that the goal of this training was making sure patients with different needs received the appropriate care, and that care was documented correctly in order for facilities to receive “credit for a certain number of minutes in those categories that drive payment” (S5N3.2). While in many cases, training was not designed to change care delivery, and was instead focused on better documentation to ensure appropriate reimbursement, some administrators described implementing clinical care training such as “hands on training, return demonstration as far as breathing treatments, and suctioning, and trach [tracheotomy] care” (S3N2.1) to improve nurses’ clinical capabilities in taking care of more clinically complex patients. For representative quotes, see Table 3.
Training for the PDPM Mainly Focused on Patient Assessment, Documentation, and Clinical Care.
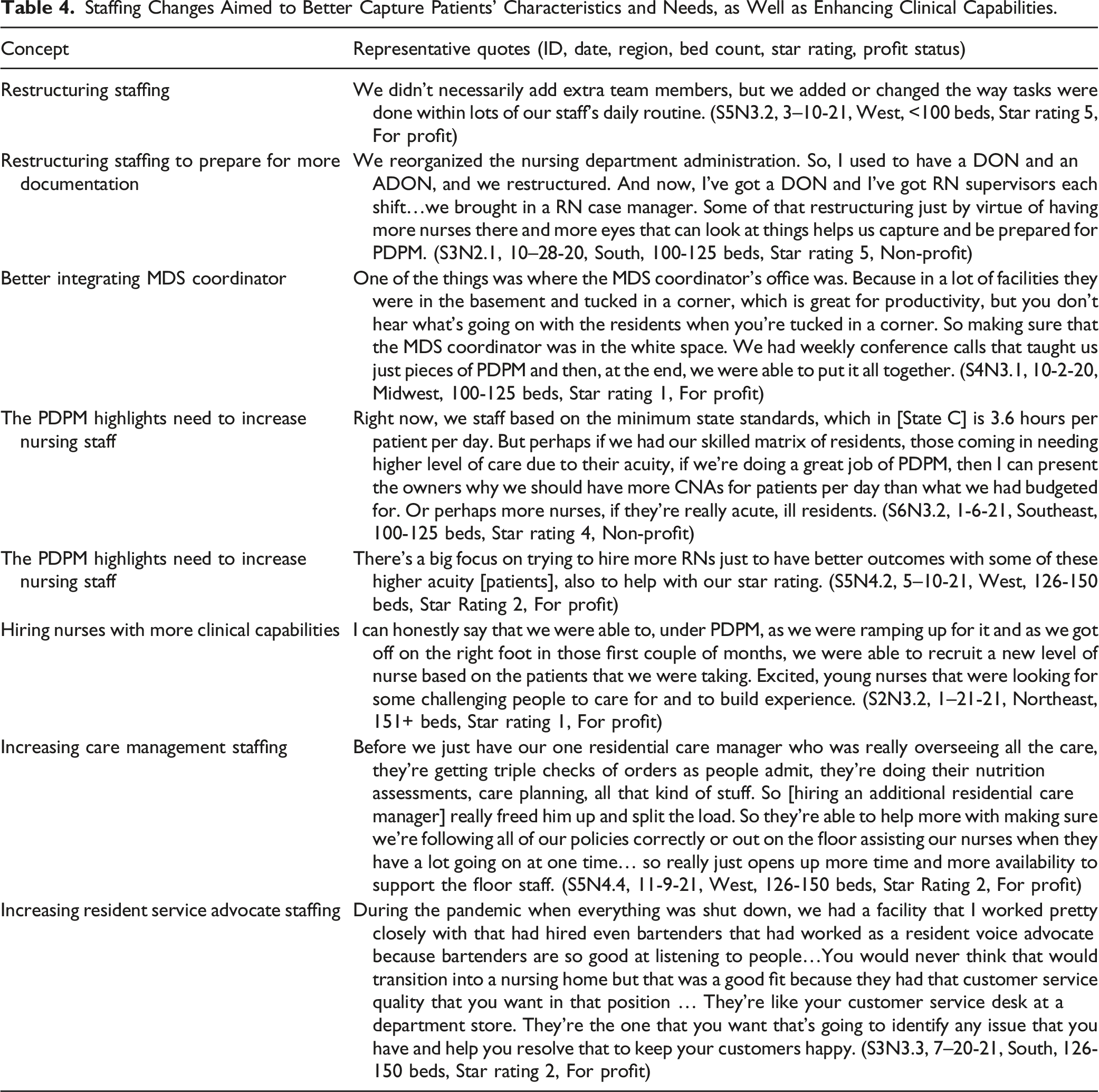
Staffing changes aimed to better document patients’ characteristics and needs, as well as to enhance clinical capabilities. In the process of preparing for and implementing the PDPM, SNF administrators talked about adding or changing “the way tasks were done within lots of [their] staff’s daily routine” (S5N3.2) rather than changing their staffing mix. For example, a change such as moving the MDS office from the basement to an open space where the rest of the staff and administration can see each other was mentioned as a way to better integrate the MDS coordinator into the SNF’s daily operations. Implementation of the PDPM highlighted the importance of documentation for reimbursement, and staffing changes mainly aimed to serve that end. One administrator made it clear that the goal was to have “more eyes that can look at things” (S3N2.1). However, some administrators talked about adding licensed nursing staff to not only increase their ability to care for more clinically complex patients, but also to provide more well-rounded care suited to individual patient needs. The specific measures administrators took included recruiting “a new level of nurse based on the patients that [they] were taking” (S2N3.2), hiring additional resident care managers to ensure new protocols for the PDPM were followed, and providing additional support to the nurses (S5N4.4). One SNF administrator reported that they hired additional staff to serve the role of resident service advocate (S3N3.3). For representative quotes, see Table 4.
Staffing Changes Aimed to Better Capture Patients’ Characteristics and Needs, as Well as Enhancing Clinical Capabilities.
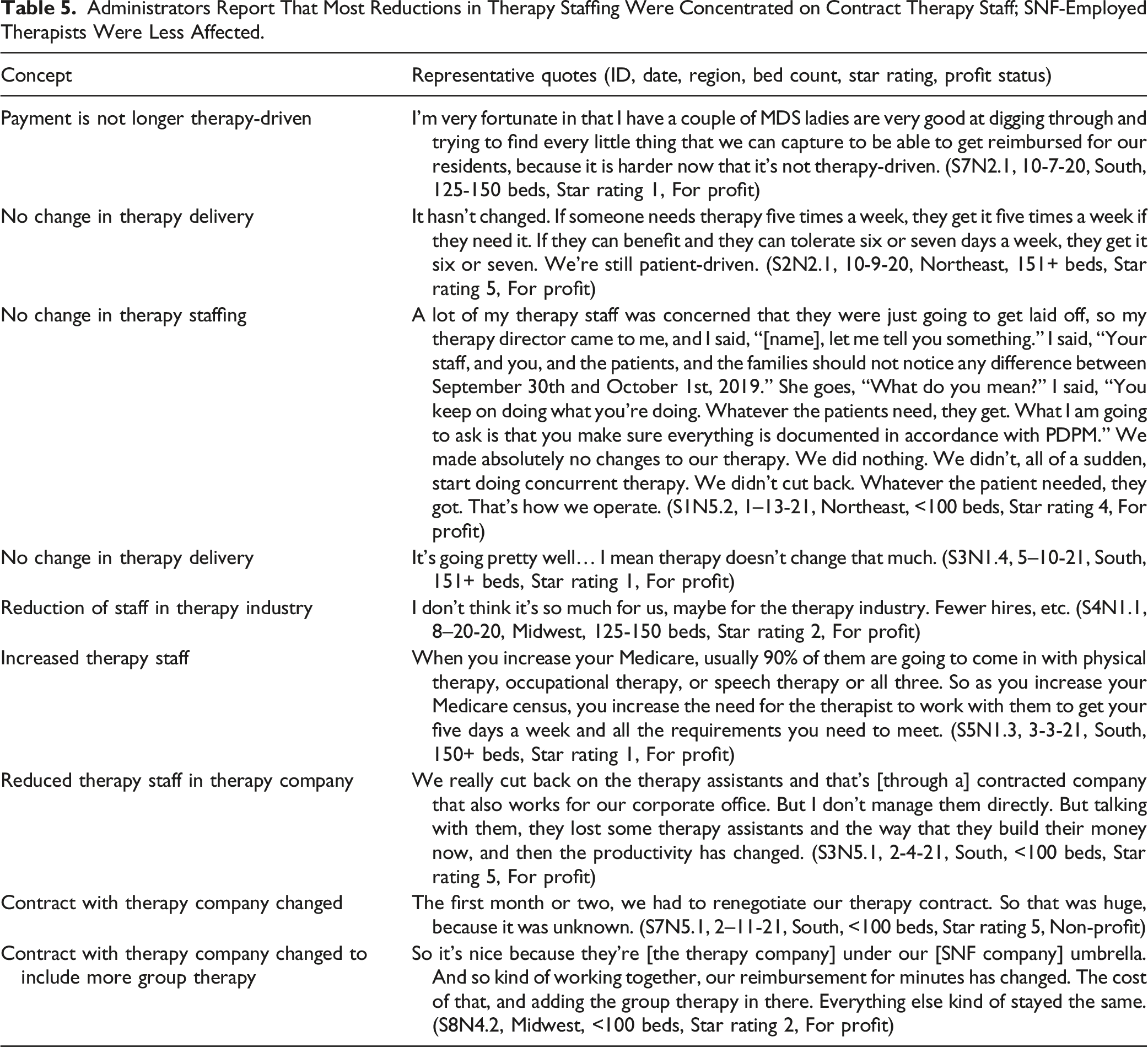
Administrators report that most reductions in therapy staffing were concentrated on contract therapy staff; SNF-employed therapists were less affected. The administrators recognized that the PDPM is not as “therapy-driven” as the prior system of reimbursement (S7N2.1). While many of them reported that they did not need to implement large reductions or furloughs of therapy staff as a result of the PDPM, reduction in total therapy volume and large reduction among contract therapy staff were discussed. However, it appeared that the impact of the PDPM on therapy staffing was not so much on facilities’ in-house staff, but more on the therapy industry as a whole (S4N1.1). One administrator explained that they “didn’t cut back” and “made absolutely no changes to their therapy.” The SNF simply continued to provide patients with the appropriate amount of care and therapy as always and “didn’t… start doing concurrent therapy” (S1N5.2), which would require less therapy staff and reduce costs. When administrators reported a reduction in therapy staff, it tended to be among contract employees. One administrator worked at a facility whose corporation also owned their contract therapy company, and described the reduction of contract therapy staff as: Our corporation also owns the therapy company. So there was a lot of dialog about what this was going to mean to them. And they have reduced a number of positions. At one time, they had maybe 300 staff. And now they probably have closer to 230 staff. (S4N5.1) Another administrator noted having to “cut back on the therapy assistants” in their “contracted company” and not including employees under his direct management (S3N5.1). In addition, some administrators reported that they renegotiated their therapy contract as a part of the preparation for the PDPM, mainly to include more group therapy (S7N5.1). Complementing results from existing research, administrators in this study noted significant reductions in therapy volume (Rahman et al., 2022) or major changes to therapy staff levels (Prusynski et al., 2021) among contract employees. Administrators pointed out that SNF-employed therapists were less affected in their preparation or implementation process. Many administrators emphasized that they continued to deliver the care patients needed and the PDPM did not change the levels of care or amount of therapy delivered. Their emphasis of this point clarified their commitment to a continuation of adequate therapy despite the payment model change. Some administrators reported observing large reductions among contract therapy staff rather than in-house staff. Changes in contracts with therapy companies were also mentioned. This is consistent with existing quantitative studies, which found the largest staff reductions occurred in therapy assistant and contract therapy staff immediately after the implementation of PDPM (Prusynski et al., 2021). Some administrators did discuss changes in therapy contracts to include more group therapy, which may partially explain the reduction in therapy volume found quantitatively. For representative quotes, see Table 5.
Administrators Report That Most Reductions in Therapy Staffing Were Concentrated on Contract Therapy Staff; SNF-Employed Therapists Were Less Affected.
Discussion
Our interviews with SNF administrators revealed several main themes. First, the majority of administrators we interviewed reported that their SNFs were ready for the PDPM implementation due to extensive preparation beforehand. Operational rehearsal of the PDPM involving the entire care team was mentioned by several administrators as a training exercise in preparation. Administrators also discussed other factors that increased their levels of confidence regarding the PDPM implementation, including the SNF’s clinical capacity, current patient mix, and the administrator’s previous experience with payment reforms. Secondly, much of the preparation facilities undertook in the lead-up to the adoption of the PDPM involved training MDS and nursing staff in areas of patient assessment, documentation, and improving care capabilities for clinically complex patients. Thirdly, administrators described restructuring current staff responsibilities in preparation for the PDPM’s implementation. Some staffing changes included adding additional nurses and resident care managers. Finally, different from what was hypothesized in advance of the PDPM, administrators in our sample did not report significant reductions of therapy staff except for among contract employees.
Our research has several limitations. First, although we obtained interview data from a robust sample of 40 SNFs across eight healthcare markets, our findings may not be generalizable to all SNFs and all markets in the U.S. Additionally, since interviews were conducted between July 2020 and December 2021, recall of preparation for the PDPM may have been impacted by the time elapsed since implementation, as well as the co-occurrence of the COVID-19 pandemic. Since the interviews were conducted during the middle of the pandemic, it is possible that the facilities included in our sample were the better functioning facilities; therefore, their administrators had the capacity to participate in the interviews, and were better able to implement the PDPM. Facilities where administrators did not have the capacity to participate in interviews may have had different experiences. These results also may not reflect the effects of long-term implementation of the PDPM alone: subsequent papers using these data will report on the impacts of the pandemic on the implementation of the PDPM. However, since this paper focuses on the preparation and initial implementation of the PDPM, which took place in October 2019 and was thus actively underway by the time the pandemic hit, it is unlikely that the COVID-19 pandemic impacted administrator experiences of the first four to five months of implementing a new payment model. Lastly, although we present perspectives from administrators and include their observations of SNFs’ responses to the PDPM, we did not interview other staff roles and thus are unable to present staff points of view. Further research is needed to understand the long-term impacts of the PDPM on all stakeholders.
Despite these limitations, our findings present a fresh point of view on the impact of payment reform for SNF administrators and have significant implications for future research and policy. The interviews with SNF administrators add significant depth and nuance to our understanding of how the shift in payment model to the PDPM was experienced by administrators over the initial period of implementation. Consistent with the existing literature on previous payment reform, such as the transition to the RUG payment model, SNF administrators explored ways of adjusting documentation to maximize reimbursement levels (Unruh et al., 2020). It appears that administrators devoted substantial time and resources in trying to achieve that higher reimbursement goal, including hiring external consultants for the PDPM education, training MDS coordinators and nurses for more exhaustive patient assessment and appropriate documentation of the care provided, as well as practicing operations (i.e., assessments and coding) prior to the PDPM taking effect. Administrators also commonly expressed the indispensable role of MDS nurses throughout this transition. In addition, administrators’ experiences with previous payment reforms, staff members’ clinical capabilities, and existing patient mix were reported as contributing factors to administrators’ levels of confidence on their implementation of the PDPM.
Existing quantitative research has found evidence of the impact of the PDPM on therapy utilization and therapy staffing in SNFs. Rahman et al. (2022) found a significant reduction in therapy volume during hip fracture patients’ stay in SNFs between January 2018 and March 2020. In terms of therapy staffing, there was evidence of both immediate and gradual reductions after the PDPM implementation (Prusynski et al., 2021). PDPM appears to have had its intended effect on SNFs regarding changing financial incentives related to therapy provision. However, the impact of specific measures SNFs took to achieve these reductions in therapy volume and staffing is only partially explained and should be further explored.
This paper explores SNF administrator perspectives on the process of implementing a new payment model, PDPM, at their facilities. Our findings expand on the existing literature on the impact of the PDPM on skilled nursing facilities. Similar to previously published research, administrators in this study reported changes to therapy staff levels (Prusynski et al., 2021) among contract employees, and pointed out that SNF-employed therapists were less affected in their preparation or implementation process. Many administrators emphasized that they continued to deliver the care patients needed and the PDPM did not change the levels of care or amount of therapy delivered. Their emphasis of this point clarified their commitment to a continuation of adequate therapy despite the payment model change. Some administrators did discuss changes in therapy contracts to include more group therapy, which may partially explain the reduction in individual therapy volume between January 2018 and March 2020 found quantitatively.
Findings from this paper highlight the importance of training for MDS nurses during the transitioning phase to the new PDPM payment model. Administrators emphasized that MDS nurses were key to a smooth payment model transition and the closer integration of their role into SNFs’ daily operations was especially beneficial. This paper also reveals potential effects of the PDPM on SNFs’ patient mix. Existing studies have pointed out that the PDPM would give SNFs financial incentives to admit a case mix of more clinically complex patients (Makam & Grabowski, 2021). From the administrators’ perspectives, SNFs recognized the increased incentive for admitting patients with more complex needs under the PDPM and prepared accordingly. The administrators described efforts to improve nurses’ clinical capabilities and implemented different strategies to pay closer attention to patients’ needs. This finding is consistent with existing quantitative research that found no significant changes in SNF patient outcomes (Zhang et al., 2022). However, the effect on access to care for patients with less severe clinical care needs should be closely monitored.
Findings from this paper highlight the importance of MDS nurses in-patient admissions, documentation, and SNF daily operations. Future policy and practice should be designed to train and support MDS nurses in this role. Policymakers should recognize the relationships between SNFs' financial incentives and the provision of care to patients. Payment methods should be designed to reflect the cost of providing different services, such as physical therapy and ancillary care, to SNF patients. It is important for SNFs to provide care patient need and get appropriately reimbursed for them. At the same time, SNFs will likely take the opportunity to maximize profit if reimbursement on certain services brings disproportionate financial reward. Payment policies should consider SNFs as rational agents and strive to incentivize appropriate care for different types of patients so that the goal of comprehensive and appropriate care is properly provided. Overall, instead of being based on the types and amount of care services provided, payment should be driven by patient needs and optimal patient outcomes. According to this study, the initial implementation of the PDPM seemed promising that care began to be reimbursed more appropriately.
Footnotes
Acknowledgments
We thank Courtney Hawes, BS, for her editorial contributions to this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Warren Alpert Foundation. The funder did not play a role in the design, methods, subject recruitment, data collection, analysis, or preparation of the article.
Human Subjects Approval
This study was not considered human subjects research and was not subject to Institutional Review Board approval.