
Abstract
We examine what facility characteristics are associated with nurse turnover in residential care communities (RCCs). This is a cross-sectional study using the 2018 National Study of Long-term Care Provider Public Use File. There were 3331 RCCs (unweighted n = 272) represented when examining registered nurse (RN) turnover and when examining aide turnover there was a weighted sample of 13,676 RCCs (unweighted n = 68). RN turnover was 72% (95% confidence interval (CI) 59%, 84%), 52% reported 100% turnover. Aide turnover was 48% (95% CI 43%, 53%); 11% reported 100% turnover. We examined ownership and facility type, job design, economic, and working environment factors related to turnover. Using multivariate linear regression, non-profit RCCs had 25 percentage points lower RN turnover (95% CI: −44.46, −4.31) and 9.7 percentage points lower aide turnover (95% CI: 18.8, −0.6) compared to for-profits. We find larger RCCs had lower aide turnover.
Keywords
• We find non-profit facilities had lower aide and RN turnover. • Larger facilities had lower aide turnover rates. • Benefits and job design factors were not related to turnover rates.
• Policies aimed at turnover should consider prioritizing for-profit facilities for reducing turnover. • Qualitative research may be better suited to elucidate explanations for differential turnover.What this paper adds
Application of study findings
Background
Approximately 800,000 people live in residential care communities (RCCs). Also known as assisted living facilities (ALFs), residents in these communities need help with activities of daily living but generally do not require skilled care found in nursing homes. In 2018, there were an estimated 31,400 RCCs/ALFs that employed approximately 424,000 social workers, aides, licensed practical nurses, and registered nurses (National Center for Health Statistics, 2018). Staffing requirements of RCCs vary state to state but generally heavily rely on direct care from aides with support from registered nurses (Thomas et al., 2021).
Staff turnover in long-term care facilities has been of concern for several years. Long-term care turnover studies have been concentrated on turnover in nursing homes (Antwi & Bowblis, 2018; Banaszak-Holl & Hines, 1996; Castle & Engberg, 2005; Castle et al., 2007; Donoghue, 2009; Gandhi et al., 2021; Hinshaw & Atwood, 1983; Lerner et al., 2014; Loomer et al., 2022) as RCC/ALF research has been stymied by the lack of data. Nursing home research focused on outcomes finds higher turnover is associated with more survey deficiencies (Antwi & Bowblis, 2018; Lerner et al., 2014; Loomer et al., 2022) and worse clinical quality (Castle & Engberg, 2005; Castle et al., 2007). Since ALFs are not regulated nationally like nursing homes, research on turnover in these settings is limited to small state samples. Three studies to our knowledge have examined turnover in RCC/ALFs. One study examined factors associated with personal care aide turnover in RCC/ALFs from four states (Florida, Maryland, New Jersey, North Carolina) in 1997 and 1998 and found that chain-ownership and environmental factors were related to turnover but not benefits or non-profit status (Konetzka et al., 2005). A single-state study focused on eight nursing homes and 21 Residential Care/Assisted Living Facilities in North Carolina, measured an average of 30% turnover in residential care communities compared to 34% in nursing homes (Zimmerman et al., 2013). Most recently, another single-state study of examining retention in Ohio assisted living facilities found that non-profit ALFs had higher retention rates compared to for-profit assisted living facilities (Kennedy et al., 2021).
This study aims to build upon past research by using the only national source of data for RCC/ALFs, the National Study of Long-term Care Providers, which has been conducted since 2012 but only asked about turnover in 2018. This study will describe turnover rates of full-time aides and registered nurses (RNs) in RCC/ALFs and examine facility and benefits factors associated with turnover. We hypothesize that facilities that are for-profit, chain-owned, large, higher occupancy, presence of dementia special care unit, absence of electronic health records, do not offer a breadth of benefits to full-time care aides, do not involve aides in care planning, have inconsistent resident assignments, have higher rates of Medicaid payment, and have lower staffing levels will have higher turnover levels.
Methods
Data
This study used the 2018 public use file of the National Study of Long-term Care Providers, RCC Provider file, which is the fourth wave of a biennial study of post-acute and long-term care providers fielded by National Center for Health Statistics. Data was collected between July 2018 and February 2019. RCCs were included in the study population if they were licensed, registered, listed, certified, or otherwise regulated by the state. RCCs had to serve a predominantly adult population and provide room and board with at least two meals a day, around the clock on-site supervision, and help with personal care. The survey uses a two-stage probability-based sample design. There were 503 RCCs that completed the questionnaire (a response rate of 30%), representing a weighted sample of 31,400 RCCs.
Dependent Variable
The dependent variables for this study were percentage of full-time aide and RN turnover. Percentage of aide/RN turnover was calculated as the number of full-time aide/RN employees left between January 1, 2017 and December 31, 2017 divided by the number of full-time aides/RNs that were there on January 1, 2017, multiplied by 100.
Independent Variables
We follow past research (Banaszak-Holl & Hines, 1996; Konetzka et al., 2005) that examined ownership and facility type, job design, economic, and working environment factors related to turnover. We include ownership variables such as profit status and chain-ownership. For economic variables, we include binary variables of what benefits were offered to full-time aide employees including employee insurance, family insurance, life insurance, pension plans, and personal time off. For job design, we include variables for whether aides were included in care planning meetings, whether resident care plans changed due to their input, and if aides were able to work with the same residents. Economic and job design variables were only measured for Aides and so was excluded in the RN regression. Facility characteristics such as bed size (categorical variable), occupancy (binary variable above/below 85%), dementia special care unit (binary variable), and use of electronic records (binary variable). For environmental factors, we include aggregate variables of resident characteristics including female, age over 85%, % with bathing needs, % with eating needs, and % with Medicaid payment. We also include controls for the staffing levels measured by aide/RN hours of care per resident per day.
Analysis
Data was restricted to non-missing values of the dependent variable. The full survey sample started with a weighted representation of 31,422 RCCs (unweighted sample of 503 RCCs). We restricted the sample examining aide turnover to non-missing for all regression variables resulting in a weighted sample of 13,014 facilities (unweighted sample of 261 RCCs). We restricted the sample examining RN turnover to all non-missing regression variables resulting in a weighted sample of 3332 facilities (unweighted sample of 67 RCCs). We show survey-weighted descriptive means with lower and upper bound where available for variables in both regression samples and for the full sample to assess impact of missingness.
We use multivariate linear regression for ease of interpretation with survey weights to ensure representativeness of the sample. We include all mentioned variables above where applicable in the regression analysis. We assumed a two-sided null hypothesis at the 0.05-level to be statistically significant.
Results
The weighted distribution of full-time aide and RN turnover is shown in Figure 1. Full-time RN turnover ranged from 8.3% to 100% with a mean of 72.1% (95% confidence interval (CI): 60.2%–84.5%). The average full-time RN turnover for non-profits was 55.4% and 80.6% in for-profit facilities. Full-time aide turnover ranged from 5.9% to 100% with a mean of 47.9%. The average full-time aide turnover for non-profits was 34.8% and 52.6% in for-profits facilities. Distribution of turnover of full-time registered nurses and aides.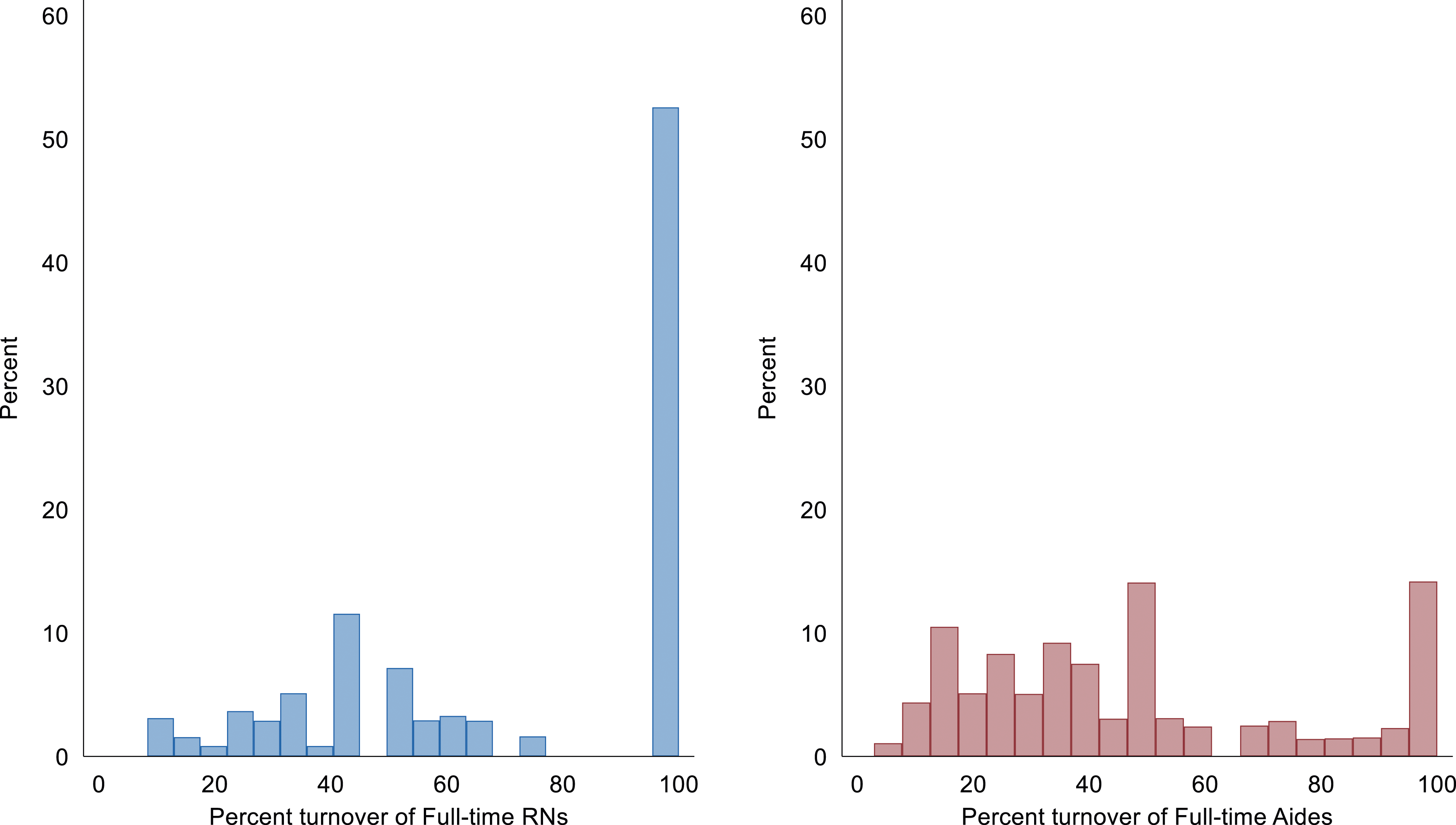
Sample Characteristics.

Note. Benefits and job design characteristics were only asked whether they were offered to full-time aide employees. RN, Registered Nurse.
Multivariate Regression Results Examining Facility Characteristics Associated With Turnover.
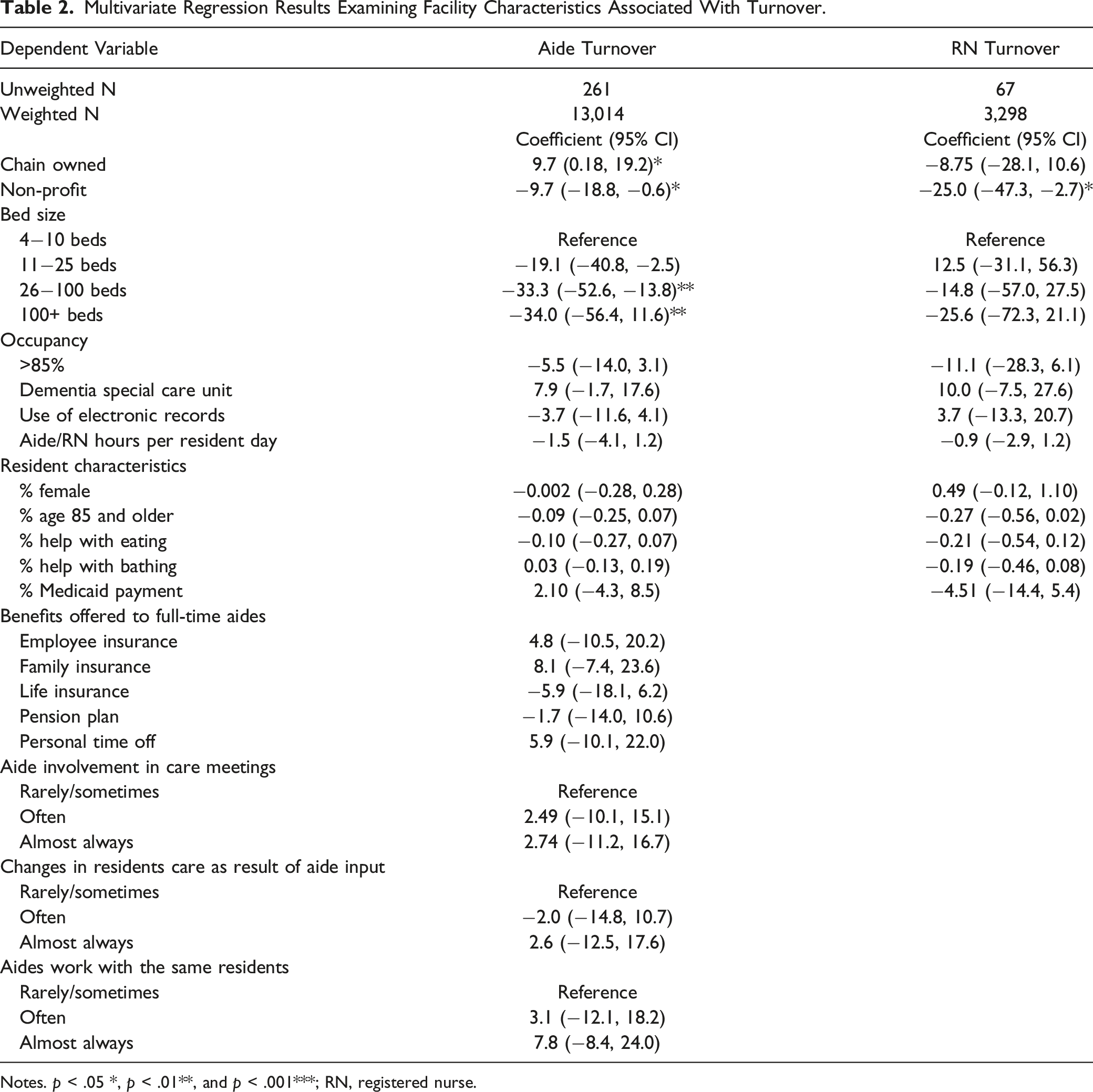
Notes. p < .05 *, p < .01**, and p < .001***; RN, registered nurse.
Discussion
In 2018, we found high but variable aide and registered nurse turnover in residential care communities. We found non-profit residential care communities had lower full-time aide and full-time RN turnover compared to for-profit residential care communities. We found chain-owned facilities had higher full-time aide turnover. Contrary to expectation, we found larger residential care communities had lower full-time aide turnover rates. Finally, we found that economic and job design variables such as offering benefits and including aides in care planning were not related to turnover rates.
Our finding that non-profit facilities had lower turnover is similar to research on Ohio RCCs (Kennedy et al., 2021) and similar to Dr Konetzka and colleagues’ study who found a difference by chain-ownership, even though they found no difference by profit status (Konetzka et al., 2005). Finally, our rates of aide turnover averaging 48% are much higher than the averages in Dr Zimmerman and colleagues study that focused on North Carolina assisted living facilities (Zimmerman et al., 2013). This is suggestive that turnover rates have worsened over time. Consistent with Dr Konetzka and colleagues study, job design and resident characteristics were not associated with turnover, when taking into account structural factors such as ownership and size (Konetzka et al., 2005). This could be because the benefits are measured in a binary instead of a more descriptive categorical variable or because of the high rates of benefits reported compared to the entire sample. For example, the survey asks whether personal time off was offered or not versus how much personal time is offered. Unfortunately rates of insurance among this population are low due to the prohibitive costs (Squillace et al., 2009), so policies that expand Medicaid may be more effective (Xu & Sharma, 2023).
Contrary to our hypothesis, we found that larger facilities had lower full-time aide turnover. One possibility is that larger facilities have more staff so there may be more flexible scheduling and allowance for personal time off. Another possibility is that larger facilities may have more opportunity for advancement within the organization. Qualitative interviews would be important in understanding this relationship further.
There are several limitations to this study. This study is survey data from 2018 which is before COVID-19 which impacted turnover in the long-term care sector significantly. However, the turnover questions were not included in surveys since 2018. We recommend the National Post-Acute and Long-term Care study include survey questions that address turnover regularly as it is an important predictor of quality for nursing homes (Antwi & Bowblis, 2018; Castle et al., 2007; Lerner et al., 2014; Loomer et al., 2022) and is likely related to residential care quality as well. Second, there was a lot of missing data for turnover in this data set, in particular for other types of turnover such as for licensed practical nurses and part-time workers, and our findings may not be representative of assisted living facilities nationally. States could start requiring payroll data from their assisted living facilities like the payroll-based journal which is required for nursing homes by Centers for Medicare and Medicaid Services. This is likely data that RCCs already have and thus would be easier than filling out a survey.
Overall, our results have important implications for regulation regarding RCCs. There is not a one-size-fits-all answer to reducing turnover. For-profit facilities may need to be prioritized for resources to reduce turnover over non-profit facilities. Nurse turnover is an important indicator of quality of long-term care communities and thus consistent data collection for this measure should be undertaken.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.