
Abstract
The goal of this study is to investigate the association between chronic non-cancer pain (CNCP) and mild cognitive impairment (MCI)/Alzheimer’s disease and related dementias (ADRDs) development among adults aged ≥50 using administrative claims data from a national commercial health insurance company during 2007–2017. To reduce selection bias, propensity-score matching was applied to select comparable CNCP and non-CNCP patients. Time-dependent Cox proportional-hazards regressions were conducted to estimate the hazard ratios (HRs) of incident MCI/ADRDs. Of 170,900 patients with/without CNCP, 0.61% developed MCI and 2.33% had been diagnosed with ADRDs during the follow-up period. Controlling for potential confounders, CNCP patients had a 123% increase in MCI risk (HR = 2.23; 95% CI = 1.92–2.58) and a 44% increase in ADRDs risk (HR = 1.44; 95% CI = 1.34–1.54) relative to non-CNCP patients. CNCP is a risk factor for MCI/ADRDs. Promoting awareness and improving early CNCP diagnosis in middle-aged and older adults should be incorporated into cognitive impairment and dementia prevention.
• This study used clinical diagnoses of MCI, providing more clinically relevant into the association between chronic pain and cognitive impairment. • This study incorporated a propensity-score matching approach, addressing potential selection bias, which provides more reliable evidence on the link between CNCP and cognitive decline and dementia risk. • Extending the existing knowledge on the association between CNCP and cognitive impairment by focusing on a relatively younger population, aged 50 or older.
• By addressing pain effectively, healthcare providers can potentially reduce the risk of cognitive decline and dementia in this population. • Health education programs can raise awareness about the link between chronic pain and cognitive impairment, emphasizing the importance of managing pain and seeking early diagnosis and treatment to mitigate the risk of developing cognitive disorders. • Primary care physicians and healthcare professionals should be encouraged to assess and monitor patients with CNCP regularly for signs of cognitive impairment.What this paper adds
Applications of study findings
Introduction
Chronic pain is a commonly reported symptom in middle-aged and older population and its prevalence steadily increased in the past two decades (Zimmer & Zajacova, 2020; Zimmer et al., 2020). The physical and psychological consequences of chronic pain have major deleterious effects on older adults’ cognitive abilities (Baker et al., 2018; Karp et al., 2006; Landrø et al., 2013; Pickering et al., 2018; Weiner et al., 2006). A growing body of evidence from cross-sectional and longitudinal studies indicates that chronic pain symptoms have been linked to the development of Alzheimer’s disease and related dementias (ADRDs) (Innes & Sambamoorthi, 2020b).
The extant studies suggest a positive association between different types of chronic pain and incident ADRDs (Ezzati et al., 2019; Innes & Sambamoorthi, 2020a; James & Ferguson, 2019; Khalid et al., 2020; Sangha et al., 2020; Tzeng et al., 2018; Yamada et al., 2019), although studies varied widely in pain sites (e.g., back or knee) and types, study population (mainly focus on aged 65 and older), and length of follow-up (range from 2 to 16.5 years) (Innes & Sambamoorthi, 2020b). Even though the majority of these studies exclude pre-existing cognitive impairment or dementia to prevent the reverse causality, it does not eliminate other potential selection biases such as the predisposing factors of chronic pain being related to the development of ADRDs, which may distort the primary association.
The evidence on longitudinal association of chronic pain to cognitive decline remain relatively sparse and inconclusive (Leeuw et al., 2018; Mazza et al., 2018; Veronese et al., 2018; Whitlock et al., 2017). A prospective cohort study with 10,065 individuals aged 62 years and older concluded that persistent moderate-to-severe pain was a risk factor for an accelerated rate of memory decline over a 10-year follow-up period (Whitlock et al., 2017), whereas other two longitudinal studies did not find that the presence of pain was associated with cognitive decline among older people aged 65 years and older (Leeuw et al., 2018; Veronese et al., 2018). The conflicting findings about the relationship between chronic pain and cognitive function may be attributed to the inconsistent measures used to assess cognitive function in different studies (Leeuw et al., 2018; Veronese et al., 2018; Whitlock et al., 2017). For instance, in Whitlock et al.’s study, only one aspect of cognitive function (i.e., memory) was investigated. Clinically, cognitive impairment can be divided into two categories: mild cognitive impairment (MCI) and ADRDs. Given that an average of 32–38% of MCI patients developed dementia within 5 years (Mitchell & Shiri-Feshki, 2009; Ward et al., 2013), investigating the association between chronic pain and clinically-defined MCI provides evidence for pain management interventions in the early stage.
This study used 11-year administrative health insurance claims data along with the propensity-score matching approach to investigate whether patients aged 50 or over with chronic non-cancer pain (CNCP) are more likely to have incident MCI/ADRDs, compared to pain-free counterparts. We hypothesized that newly diagnosed CNCP patients have a higher risk of developing MCI/ADRDs.
Methods
Data and Study Sample
This study used administrative health insurance claims data from the Optum’s de-identified Clinformatics® Data Mart Database, including both employer-sponsored plans and Affordable Care Act Exchange plans. The de-identified database used for this study is a specific sample comprised of approximately 22 million patients enrolled in the care network and had ever been prescribed any controlled drugs from 2007 through 2017. The database also included information on health insurance enrollment and sociodemographics (e.g., education level, household income, race/ethnicity). The Institutional Review Board of Indiana University approved the study.
The de-identified dataset was analyzed in 2019. Our analyses were limited to patients aged ≥50 who were continuously enrolled in a health insurance plan for more than two consecutive years in order to ensure the completeness of a patient’s diagnosis records. Continuous enrollment was defined as having no health insurance coverage gap of more than 31 days during the study period (Ku & Platt, 2022), including both the look-back and follow-up phases. Patients were excluded from this study if they had any diagnosis of: (1) cancer throughout the enrollment period; (2) CNCP; (3) MCI, ADRDs, or alcoholic and drug-induced persisting dementia; (4) acute pain, HIV, multiple sclerosis, or Parkinson’s disease before the index date (described below); and (5) follow-up period less than 6 months after the index date. These criteria allowed us to identify new CNCP as well as incident MCI and ADRD patients, minimizing the possibility of a false attribution to existing or previous symptoms for the outcomes of the present study. Figure 1 shows the sample flow chart. Sample flow chart.
Research Design
This study used a retrospective study design with the follow-up periods ranging from a half to 9 years to examine the study hypotheses (Figure 2). We created an index date for each patient to define the look-back (before the index date) and follow-up (after the index date) periods where the look-back period was two years or longer to ensure a long-enough period to capture the presence of pre-existing related conditions (Davis et al., 2022). Specifically, to determine eligible CNCP patients based on physician diagnosis, the date of the first physician visit for CNCP two years after the initial enrollment was used as the index date. Eligible CNCP patients should have at least one additional CNCP diagnosis within 1 year after the index date. When identifying eligible non-CNCP patients, a similar approach was used to determine the index date. For example, if a patient had never been diagnosed with CNCP during the enrollment period, his/her index date was the date of the first physician visit two years after enrollment. Subsequently, eligible patients with and without CNCP were matched based on the propensity score models (details to be described later). Matched patients were then followed up until the time they developed MCI/ADRDs, or the date of a censoring event (the end of health insurance enrollment). Research design. Abbreviation: CNCP, chronic non-cancer pain; MCI, mild cognitive impairment; ADRDs, Alzheimer’s disease and related dementias. a). Medical conditions included alcoholic and drug-induced persisting dementia, acute pain, cancer, HIV, multiple sclerosis, and Parkinson’s disease. b). At least a 2-year look-back period for each study patient.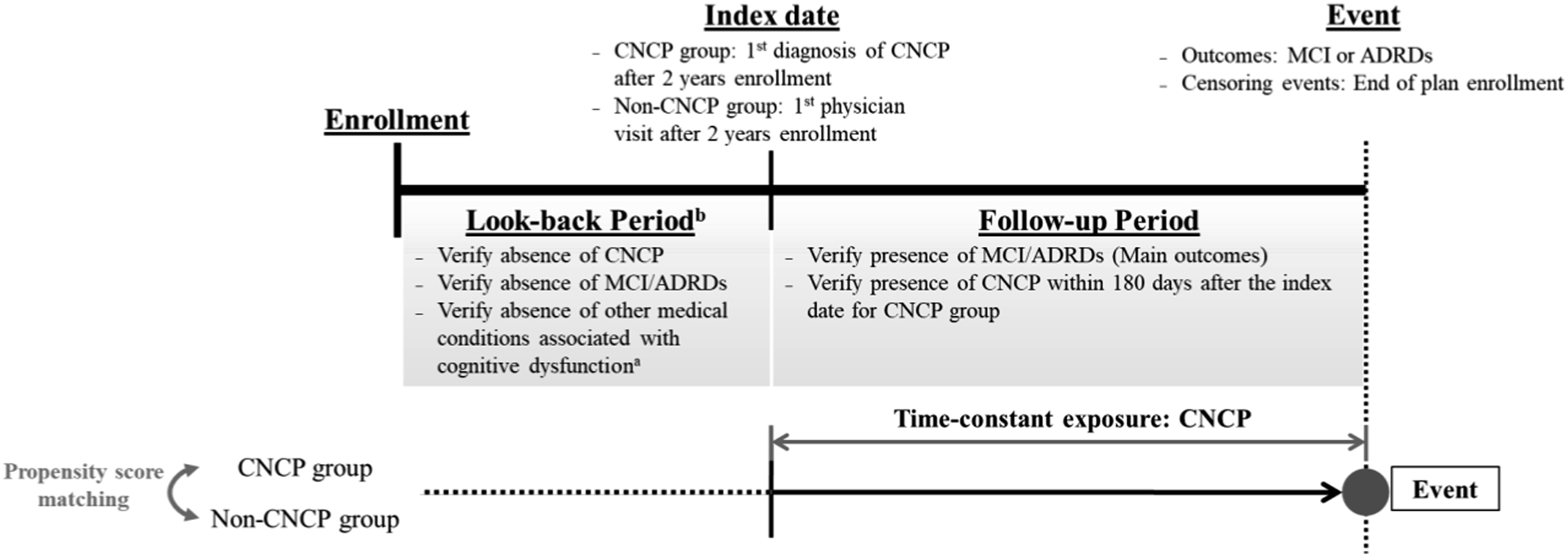
As suggested by a systematic review (Mazza et al., 2018), pain is not the only factor responsible for cognitive impairment or dementia. It is also possible that premorbid risk factors that predispose adults to chronic pain may show cognitive dysfunction. Therefore, selection bias may occur if those factors also contribute to the difference between patients who developed MCI/ADRDs and those who did not during the follow-up period. To reduce the potential selection bias, we employed a propensity-score-matched cohort design (Seeger et al., 2005) in order to obtain comparable CNCP and non-CNCP groups at each time block. We used six months for each time block, resulting in up to 17 half-year blocks of calendar time from January 2009 to June 2017 (Appendix Figure S1). Within each time block, each eligible CNCP patient was matched to a contemporaneous non-CNCP patient, where unmatched CNCP patients were discarded from the following matching processes. The matched cohorts (n = 170,900 patients) were followed up from the date of matching to the date of occurrence of MCI, ADRDs or the censoring events for survival analysis. The propensity-score-matched cohort design has been used in observational studies using claims data, which has the advantage that each matched cohort preserves the baseline comparability with regard to the observed characteristics (Rosenbaum & Rubin, 1983; Seeger et al., 2005).
Outcomes and Exposure Measures
Outcome Variables
Mild cognitive impairment and Alzheimer’s disease or related dementias (including Alzheimer’s disease, unspecified dementia, vascular dementia, frontotemporal dementia, and Lewy body dementia). MCI and ADRDs were defined according to the codes of the International Classification of Disease, Ninth and Tenth Revisions, Clinical Modification (ICD-9-CM and ICD-10-CM). Appendix Table S1 shows the diagnosis codes used to identify MCI and ADRDs. Incident MCI and ADRDs were defined as the first occurrence of a diagnosis after the time of matching.
Primary Exposure
Chronic non-cancer pain. In this study, CNCP included general chronic pain (James & Ferguson, 2019), back pain (Yamada et al., 2019), fibromyalgia (Tzeng et al., 2018), osteoarthritis (Innes & Sambamoorthi, 2020a), arthritis/joint pain (Yamada et al., 2019), and rheumatoid arthritis (Sangha et al., 2020), which have been shown to be associated with cognitive impairment or certain subtypes of dementia. Appendix Table S1 shows the ICD-9-CM and ICD-10-CM diagnosis codes of CNCP. Once a patient was diagnosed with CNCP, the patient was retained in the exposure group until the end of the follow-up period.
Covariates
Sociodemographics included age, sex, self-reported race/ethnicity, education level, and household income. Based on the literature (Cheng et al., 2012; Patel et al., 2013; Pickering et al., 2018), we also adjusted for other comorbidities that may affect the relationships of CNCP with MCI/ADRDs, including type-2 diabetes, hypertension, cerebrovascular disease, tobacco use disorder, and alcohol use disorder. These comorbidities were ascertained based on ICD-9-CM/ICD-10-CM codes and coded as time-dependent binary variables. Time-varying pain medication use (Y/N), including opioid analgesics and non-opioid analgesics (Allegri et al., 2019; Dublin et al., 2015; Pask et al., 2020), was included as a potential confounder in the final models. All comorbidities and pain medication use were coded as time-varying variables.
Statistical Analysis
To reduce potential selection bias between patients with and without CNCP, we created the matched sample using the 1:1 nearest-neighbor matching based on propensity scores. First, a logistic regression model was used to estimate propensity scores for having CNCP based on the patients’ age, sex, race/ethnicity, education level, as well as pre-existing conditions including hypertension, type-2 diabetes, major depressive disorder, generalized anxiety disorder, insomnia, tobacco use disorder, and alcohol use disorder over the 1-year period preceding their index dates. These covariates have been shown to be highly correlated with chronic pain and cognitive function in previous research (Blyth & Waite, 2010; van Hecke et al., 2013). Then, each CNCP patient was matched with a non-CNCP patient within the recommended caliper size that equals 0.2 standard deviations of the logit of the predicted propensity scores (Austin, 2009).
To ensure that matched cohorts were adequately balanced, we used the “PSMATCH” procedure in SAS software, version 9.4 to check the overall balance after matching (SAS Institute Inc., 2016). Additional bivariate tests were conducted to compare group differences in sociodemographic characteristics and common comorbidities between the CNCP and non-CNCP groups, using a t test for the continuous variable (age), a Kruskal–Wallis test for the ordinal categorical variable (household income), and Chi-square tests for other nominal categorical variables such as sex, race/ethnicity, education level, comorbidities, and pain medication use. We also reported the absolute difference in these variables and computed the effect sizes such as Cohen’s d for the continuous variable, and Cramer’s V for categorical variables to compare group differences. Cohen’s d less than 0.2 is considered a small effect size and a Cramer’s V of 0.1 indicates small effect (Cohen, 2013).
On the matched sample, survival analysis was conducted using a time-dependent Cox proportional-hazards model to test the research hypotheses. The outcome variable was the time from the date of matching to the occurrence of MCI/ADRD or a censoring event. Two separate time-dependent Cox proportional-hazards models were fit, adjusting for the aforementioned covariates, to examine the association between CNCP and the risk of incident MCI and ADRDs, respectively. Both models generated hazard ratios (HRs) with their 95% confidence intervals (CIs). All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc, 2016). A p-value of .05 was considered the threshold for statistical significance.
Sensitivity Analysis
A series of sensitivity analyses were performed to examine the effects of interactions between CNCP status and all covariates on the risks of MCI/ADRDs. We found a slightly higher risk of developing ADRDs in CNCP patients who have been diagnosed with diabetes or hypertension during the follow-up period. In addition, CNCP patients who have been prescribed pain medication have a slightly greater risk of incident ADRDs, compared to their counterparts. Subgroup analysis for adults aged 65 and older found similar results. To ensure age is balanced between the two groups at the individual level, we also performed matching on both propensity score and age (in 5-year bin increments). The additional matched sample yielded the same conclusion and similar risk estimates as the results based on the matching only on propensity scores.
There is no clinical guideline that states the average time for a CNCP patient to develop MCI/ADRDs. In our main analysis, we excluded subjects with follow-up period less than 6 months because it is unlikely that a newly diagnosed CNCP leads to MCI/ADRDs within 6 months. We further performed three subgroup analyses for subjects who were followed up at least 1, 2, or 3 years after the index date, respectively. The results are similar and therefore only primary results were reported.
We also performed a repeated analysis but excluding CNCP patients with rheumatoid arthritis and fibromyalgia, because these two diseases may work through a different mechanism to cause cognitive decline compared to other etiologies. Since we excluded all pre-existing CNCP patients during the 2-year look-back period, these two diagnoses were rare in the newly diagnosed CNCP cohort. Our conclusions were unchanged when excluding the rheumatoid arthritis and fibromyalgia sub-populations.
Results
Descriptive Statistics of Sample Before and After Propensity Score Matching.
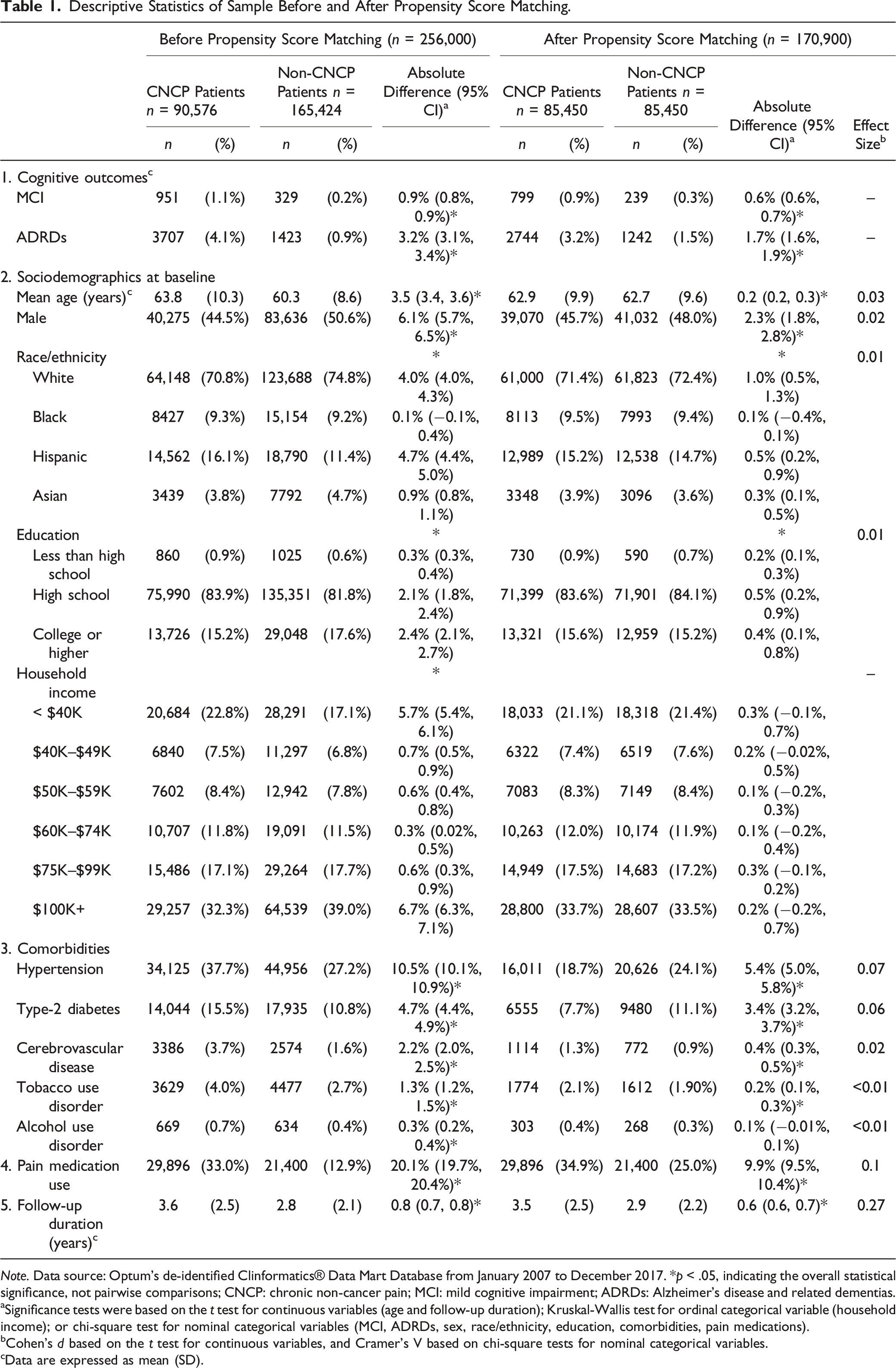
Note. Data source: Optum’s de-identified Clinformatics® Data Mart Database from January 2007 to December 2017. *p < .05, indicating the overall statistical significance, not pairwise comparisons; CNCP: chronic non-cancer pain; MCI: mild cognitive impairment; ADRDs: Alzheimer’s disease and related dementias.
aSignificance tests were based on the t test for continuous variables (age and follow-up duration); Kruskal-Wallis test for ordinal categorical variable (household income); or chi-square test for nominal categorical variables (MCI, ADRDs, sex, race/ethnicity, education, comorbidities, pain medications).
bCohen’s d based on the t test for continuous variables, and Cramer’s V based on chi-square tests for nominal categorical variables.
cData are expressed as mean (SD).
After matching, all variables except sex and household income statistically differed between two groups but the group differences were trivial (Cohen’s d < 0.2 and all Cramer’s vs. < 0.1). Based on the results of PSMATCH procedure (SAS Institute Inc, 2016), two measures of balance diagnosis were examined for each matched cohort. The standardized difference of the means of propensity scores between groups was within the recommended limits (i.e., −0.25 and 0.25) and the ratio of variances of propensity scores was between 0.5 and 2 (Stuart, 2010). This indicates that most of the before-matching group differences between the CNCP and non-CNCP groups were eliminated via the propensity-score matching.
Association of Chronic Non-Cancer Pain With Mild Cognitive Impairment or Alzheimer’s Disease and Related Dementias (n = 170,900).
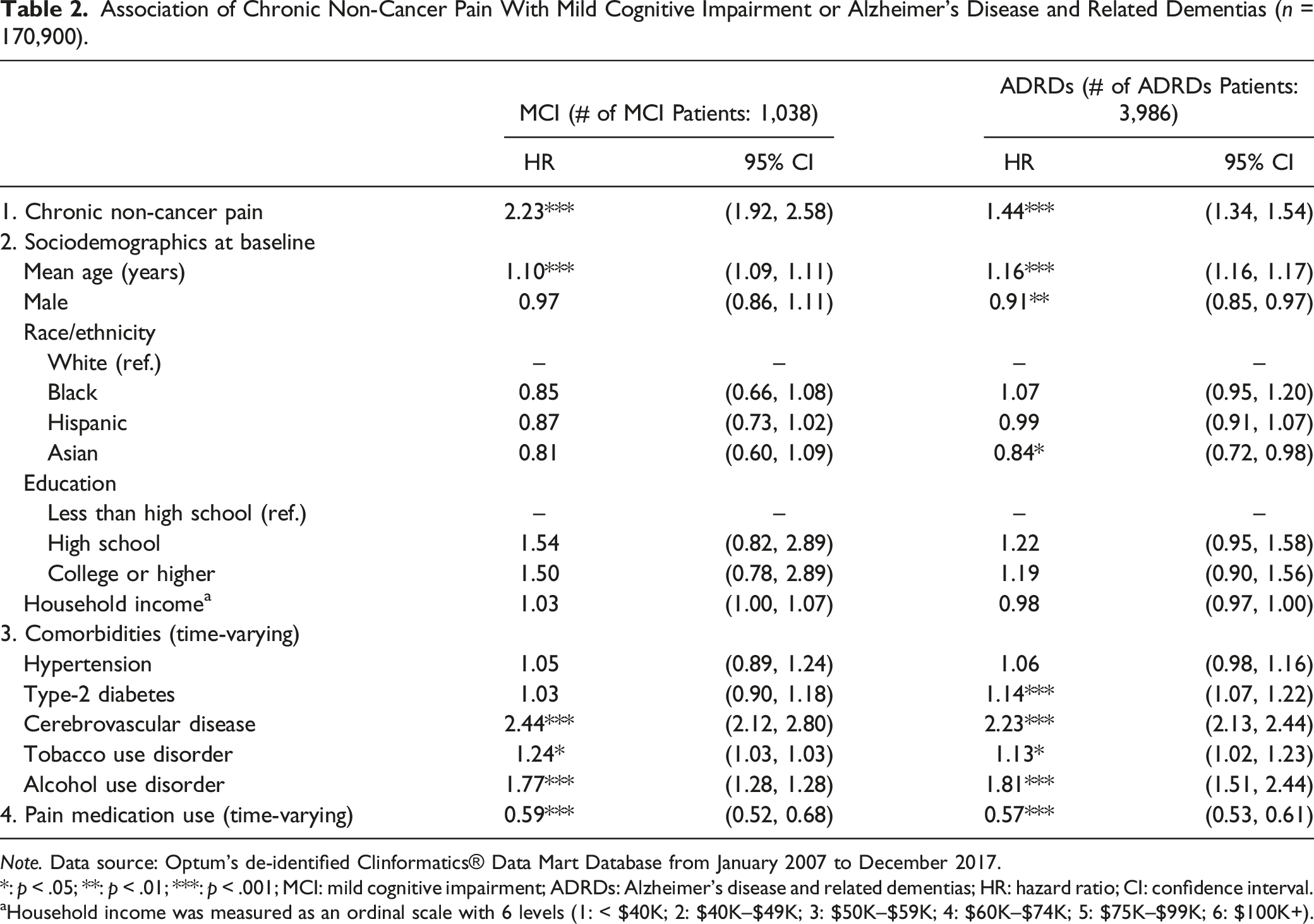
Note. Data source: Optum’s de-identified Clinformatics® Data Mart Database from January 2007 to December 2017.
*: p < .05; **: p < .01; ***: p < .001; MCI: mild cognitive impairment; ADRDs: Alzheimer’s disease and related dementias; HR: hazard ratio; CI: confidence interval.
aHousehold income was measured as an ordinal scale with 6 levels (1: < $40K; 2: $40K–$49K; 3: $50K–$59K; 4: $60K–$74K; 5: $75K–$99K; 6: $100K+).
Discussion
This study analyzed 11-year administrative health claims data to examine the associations between CNCP and the development of MCI/ADRDs. The main result shows that newly diagnosed CNCP patients aged 50 or older had a higher risk of developing MCI/ADRDs, compared to non-CNCP patients of the same age group, after adjusting for other comorbidities that are known to be related to MCI/ADRDs. In agreement with previously published longitudinal studies (Cao et al., 2019; Ezzati et al., 2019; Innes & Sambamoorthi, 2020a; Khalid et al., 2020; Tzeng et al., 2018), our findings based on newly diagnosed CNCP patients provide empirical evidence that CNCP is indeed a risk factor for incident ADRDs. While previous studies provide inconsistent evidence on the association of CNCP to cognitive decline based on cognitive battery tests (Leeuw et al., 2018; Veronese et al., 2018; Whitlock et al., 2017), our findings indicate that CNCP patients have a greater risk of developing MCI.
While confirming findings in the extant literature, our study makes two notable contributions. First, unlike previous studies that did not exclude pre-existing conditions of chronic pain, our study followed the cohort of patients who were newly diagnosed with CNCP without diagnoses of MCI, ADRDs, Parkinson’s disease, multiple sclerosis, AIDS, cancer, and acute pain at least 2 years before their first diagnosis of CNCP. Thus, our study provides robust evidence of an association between CNCP and the development of MCI/ADRDs in middle-aged and older adults using a more rigorous study design than previous works. In addition, our study employed a propensity-score matched cohort design to select comparable patients with and without CNCP, which minimized potential selection bias (Rosenbaum & Rubin, 1983; Seeger et al., 2005).
Although the causal relationship between chronic pain and incident cognitive impairment or dementia has yet to be expounded, the cumulative evidence alludes to a potential mechanism by which chronic pain may impair cognition. The hallmarks of impaired cognitive function related to chronic pain include that the presence of pain may interrupt cognitive processing and require attention to reduce chronic pain, resulting in competition for limited attentional resources (Eccleston & Crombez, 1999). Additionally, the presence of pain may also lead to discernible brain changes in gray matter volume (Malfliet et al., 2017) and the posterior parietal cortex and the middle cingulate that are both related to memory function (Buckalew et al., 2008). A recent review study pointed out that chronic pain may increase central neuroinflammation in certain brain regions which contributes to microglial dysfunction (Cao et al., 2019). Moreover, the diminished attentional capacity may have a cumulative effect on cognitive functioning, which leads to more chronic deterioration of cognitive functioning over time (Leeuw et al., 2015). Using more rigorous sample selection criteria and robust inference methods than prior studies that examined this issue, we were able to demonstrate that chronic pain itself could be a cause of MCI/ADRDs.
There were limitations to the present study. First, due to the nature of administrative claims data, our results only reflect the situation in the insured population. This potentially limits generalizability to uninsured, underinsured, or individuals outside this insurance network, who may have different healthcare access and experiences. This is a common limitation of administrative claims-based research. This kind of large administrative database, however, allowed us to adopt a strict sample selection procedure, ruling out subjects with pre-existing conditions while still retaining adequate statistical power to examine the research questions. Second, cognitive impairment was determined by clinical diagnosis, and therefore minor, unreported, and unmeasurable changes in cognitive abilities may not have been observed. Nevertheless, the diagnosis of MCI is an important precursor of ADRDs. On average, 32%–38% of people with MCI develop one type of dementia during a 5-year follow-up period (Mitchell & Shiri-Feshki, 2009; Ward et al., 2013). Therefore, investigating the risk factors of MCI may be beneficial in delaying or preventing dementia. Third, the severity of pain was not considered due to data unavailability. Fourth, our study’s follow-up durations, averaging 3.6 years among CNCP patients and 2.8 years among non-CNCP patients, provided critical early insights but may not capture the full long-term progression to MCI and ADRDs, especially in younger demographics. In addition, because mortality data are unavailable from our dataset, our models did not adjust for competing risk of death, which might overestimate the risk of CNCP on MCI/ADRD. However, it is indicated in a previous study that when the mortality is low in the study population, the difference in risk estimate between Cox regression and the competing risk approach is minor (Berry et al., 2010). Given that our study population is relatively young (aged 50 and older), the impact of survival bias on our study results may be small.
Despite the aforementioned limitations, this study makes several critical contributions to understanding the association of CNCP with the development of MCI/ADRDs. This study assessed cognitive impairment based on clinical diagnoses rather than cognitive assessment tests (Leeuw et al., 2018; Veronese et al., 2018; Whitlock et al., 2017). Most importantly, this study applied the propensity-score matched cohort design to identify comparable cohorts of patients with and without CNCP, which provided more valid inferences.
Conclusions
Our findings demonstrate that suffering from CNCP is a significant risk factor for MCI/ADRDs among middle-aged and older adults. This study provides strong evidence that chronic pain should be carefully and effectively managed by patients and healthcare providers to reduce MCI/ADRDs risks. Health education is needed to inform patients with chronic pain in managing pain and recognizing symptoms of cognitive impairment. Healthcare providers should be encouraged to improve early diagnosis of chronic pain and conduct appropriate pain management in order to reduce the risk of developing mild cognitive impairment or Alzheimer’s Disease and related dementias among people living with CNCP.
Supplemental Material
Supplemental Material - Chronic Non-cancer Pain and Associated Risks of Incident Mild Cognitive Impairment and Alzheimer’s Disease and Related Dementias in Middle-Aged and Older Adults
Supplemental Material for Chronic Non-cancer Pain and Associated Risks of Incident Mild Cognitive Impairment and Alzheimer’s Disease and Related Dementias in Middle-Aged and Older Adults by Yi-Han Hu, Dong-Chul Seo, Lesa Huber, Patrick C. Shih, and Hsien-Chang Lin in Journal of Applied Gerontology.
Footnotes
Acknowledgement
Y.H. Hu is currently a research fellow at the Intramural Research Program of National Institute on Aging.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse [grant numbers: R01 DA039928] titled “Doctor shopping for controlled substances: Insights from two-mode social network analysis.” (Principal Investigator: Dr Brea Perry); and the Addictions Grand Challenge Initiative, Indiana University, IN.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.