
Abstract
Social isolation and loneliness are associated with negative health outcomes, and these outcomes are exacerbated among older adults who are homebound. To address this issue, Meals on Wheels programs increasingly provide social connection services to clients in addition to home-delivered meals. This descriptive qualitative study examines the impact of three types of social connection programs on the well-being of homebound older adult clients, as well as on the volunteers and staff members who deliver the programs. Thematic analysis of semi-structured interviews conducted with 117 clients, volunteers, and staff in six Meals on Wheels social connection programs across the United States indicated that program participation was associated with substantial benefits. Benefits included the development of supportive friendships, reduced feelings of loneliness, and an improved overall sense of well-being. Insights from this study may inform the development, expansion, and sustainability of social connection programs provided by community-based organizations.
Keywords
• Social connection programs meet or exceed the expectations of homebound older adult clients, volunteers, and staff. • Social connection programs benefit homebound older adults by reducing feelings of isolation and loneliness. • While programs were designed to provide benefits for clients, volunteers and staff also derived significant benefits.
• Recruitment strategies for social connection programs should focus on identifying and responding to individuals’ goals for getting involved. • Flexibility was described as an important reason why volunteers engaged in social connection programs. Programs should provide as much flexibility as possible and emphasize this flexibility in volunteer recruitment efforts. • Social connection programs provide substantial value. Findings from this paper add to the evidence base supporting continuation and/or expansion of program funding.What this paper adds
Applications of study findings
Introduction
The United States Surgeon General recently issued an advisory outlining the severe, negative consequences of social isolation and loneliness on public health (U.S. Department of Health and Human Services, 2023), and put forth a national strategy to promote social connection. This strategy includes strengthening community connection programs, emphasizing volunteer opportunities to foster diverse connections within communities, and training health care providers to recognize the value of social connection and the risks of social isolation and loneliness for all ages. Central to the national strategy is an emphasis on improving the nation’s social infrastructure through the establishment of community connection programs.
The advisory draws on the socio-ecological model and a systems theoretical approach (Centers for Disease Control and Prevention, 2021; Holt-Lunstad, 2018) as organizational tools to describe the interrelated factors—individual, relationship, community, and societal—that contribute to a person’s sense of social connection, and affect social isolation and loneliness. Social isolation is defined as the objective absence of social relationships, limited social network ties, or infrequent social interactions. In contrast, loneliness is defined as the subjective experience felt by an individual due to the lack of social connections (National Academies of Sciences Engineering and Medicine, 2020). Also central is the concept of well-being, defined by the Centers for Disease Control and Prevention as “the presence of positive emotions and moods, the absence of negative emotions, satisfaction with life, fulfillment, and positive functioning” (CDC, 2022).
Within the context of the socio-ecological model and the systems theoretical approach, older adults are at particular risk of social isolation and loneliness, due to reasons including the loss of social connections (relationships), retirement (community), the impact of health conditions prohibiting or severely reducing mobility (individual), and norms around aging (society). Research has shown that these factors impact quality of life for older adults and lead to an increased risk of morbidity and mortality (Bedard-Thomas et al., 2019; Donovan, 2020; Qiu et al., 2010; Sakurai et al., 2019). For older adults who receive services from community-based organizations, studies have found reduced levels of loneliness and depression (Helfand et al., 2020; Millen et al., 2002; Rachasrimuang et al., 2018; Thomas et al., 2020). Building on this success, community-based organizations have increasingly invested in efforts to address social isolation and loneliness among their clients through the expansion of social support programming. However, most existing social connection programs require participation in a community setting and are unable to fully meet the needs of homebound older adults. Homebound older adults represented an estimated 13% of older adults in the United States in 2020 (Ankuda et al., 2021). When placed within the socio-ecological model and systems approach, homebound older adults are especially vulnerable to social isolation and loneliness (Kannan & Veazie, 2022; Xiang et al., 2020), as they may have limited capacity to be out with others (relationships) and reduced access to programs and services (community), for example.
A limited body of research has examined social connection services for homebound older adults. Overall, available research is largely comprised of evaluations of targeted interventions, rather than evaluations of established programs for this population. Interventions that have been found to be effective in improving well-being for homebound older adults include one-on-one in-home technology training, home-delivered therapy, social clubs, and telephone reassurance programs (Bruce et al., 2021; Gadbois et al., 2022; Jesus et al., 2024; Kikuchi et al., 2023; Lee et al., 2021; Pepin et al., 2021), among numerous others. While community-based organizations including Area Agencies on Aging and senior centers often offer social connection programming to homebound older adults, most have not been formally evaluated for their impact on loneliness and isolation. An exception are the services provided by Meals on Wheels programs.
The Meals on Wheels network is made up of more than 5,000 community-based programs across the United States committed to addressing food insecurity and social isolation among older adults (Meals on Wheels, 2023). Meals on Wheels America (MOWA) is the largest leadership organization supporting the Meals on Wheels network. Existing research has documented the benefits of Meals on Wheels to well-being outside of just nutrition (Campbell et al., 2015; Gualtieri et al., 2018; Zhu & An, 2013), and has evaluated the impact of targeted social connection programs on well-being (Gadbois et al., 2022; Helfand et al., 2020; Middleton et al., 2022; Millen et al., 2002). Additionally, several studies have found that Meals on Wheels volunteers and staff reported positive experiences from their role in delivering meals (Dickinson & Wills, 2022; Papadaki et al., 2022; Thomas et al., 2020).
Outside of Meals on Wheels, the benefits of volunteerism among older adults are well-studied (Kim et al., 2020; Population Reference Bureau, 2011; Torres et al., 2023). Research has shown that older adults who volunteer, in general, have improved self-reported health, improved physical and cognitive functioning, reduced depression, and lower mortality rates (Filges et al., 2020; Hood et al., 2018). Within the socio-ecological model and systems approach, volunteers act as an important bridge between the client (individual) and services (community). At the height of the COVID-19 pandemic volunteerism declined, most likely due to measures implemented to decrease viral spread (AmeriCorps, n.d.). Yet, despite social distancing and other mitigation measures during the pandemic, informal helping of others remained constant (AmeriCorps, n.d.). As the U.S. population ages, organizations that provide services to older adults will need to grow their volunteer pool to continue to serve their communities. Understanding the benefits for volunteers and staff who deliver programming is little understood and critically needed.
While no research, to our knowledge, has examined the benefits of social connection programming on staff, existing research evaluating staff outcomes within community-based mental and behavioral health services and home healthcare non-profit organizations found high levels of burnout, compassion fatigue, and poorer health outcomes including higher rates of stroke, diabetes, arthritis, COPD, asthma, high blood pressure, and high cholesterol (Morse & Dell, 2021; Rossi et al., 2012; Sterling et al., 2021). Several of these negative outcomes were exacerbated by the pandemic (Gray et al., 2022; Sterling et al., 2020; Zhang et al., 2021). These outcomes highlight the importance of understanding what motivates individuals to work within this field.
However, research examining the motivational factors driving volunteering and working in social connection programming is limited. Such research has found that pride in the organization, its mission, and accomplishments, as well as having opportunities for both personal and professional growth and development motivate individuals to engage in community-based social services work (Colvin et al., 2021; Harmic, 2022; Houston, 2000; Kerschner & Rousseau, 2008; Wright, 2007). Further research examining the impact of social connection programming on staff and volunteers is a critically needed component of the evidence base to prevent volunteer and staff turnover and support retention.
As the U.S. Surgeon General’s advisory notes, social isolation and loneliness are urgent public health issues. The state of the research on effective interventions for social isolation and loneliness in older adults is still preliminary, with critical gaps in understanding the underlying volunteer and staff motivations to participate in social connection programming, and the applicability of social connection interventions to the homebound older adult population. This paper aims to address these gaps in knowledge, and presents findings from an evaluation of three types of social connection programs offered by MOWA community organizations: telephone reassurance, wellness activity programming, and friendly visitor. Explicitly, this paper presents findings regarding the reasons for participating in social connection programs, the impact of the programs on clients, as well as the unintended benefits for volunteers and staff.
Methods
This research included descriptive case studies (Yin, 2017) of six Meals on Wheels members’ social connection programs. In-depth, semi-structured interviews were conducted with clients, volunteers, and staff in the six social connection programs.
MOWA Network Program Selection and Recruitment
In November 2020, MOWA conducted a survey of 1,062 network programs to understand the impact of COVID-19 (Meals on Wheels America, 2020). Based on the 350 responses from this survey, MOWA identified 194 programs that had an existing, in-house social connection program. Of the 194 programs, 29 indicated their preference to opt out of research projects. The research team, consisting of Brown University staff and MOWA researchers, conducted an extensive review of MOWA network social connection program descriptions provided during the survey and/or available online. Social connection programs were defined as service offerings that aim to reduce social isolation and loneliness, such as friendly visiting, telephone reassurance, volunteer opportunities, pet assistance, and group classes or group activities. The research team chose to evaluate telephone reassurance, friendly visitor, and wellness activity programs, as the programs were commonly occurring but varied greatly in structure and systems of delivery. In addition, programs with diverse characteristics, including budget size, rurality, and client racial/ethnic diversity were selected. Twenty-six potential network programs were identified that had these types of social connection programs, did not opt out of involvement in research projects, and varied in program characteristics. The research team contacted these 26 potential programs and requested additional information including the number of clients served, the impact of the COVID-19 pandemic on social connection programming, and whether the social connection program was still in existence. After reviewing program responses, the research team invited eight programs to participate in this evaluation. Of the eight programs invited, two declined participation, resulting in six programs electing to participate.
Participant Recruitment
Each MOWA network program identified a principal point of contact who worked closely with the Brown University research team, and facilitated interview participant identification and recruitment. To best characterize each program, we sought to interview five staff members and/or program leaders, five volunteers involved in program administration or delivery, and ten client recipients of the program. Contact information for potential participants was shared with the Brown University research team. The research team contacted potential participants via telephone or email, recruited participants, and scheduled interviews. Contact attempts were made once per week and ranged from one to five attempts before the potential participant was removed from the contact list. Interviews were first conducted with program staff, then volunteers, then clients.
Qualitative Interview Procedures
The qualitative team developed interview guides with questions designed to understand the benefits and challenges of social connection programming from multiple perspectives. Questions for program staff were designed to learn specifics about the social connection program including its structure, clientele, and data/metrics collected. In addition, questions focused on assessing program feasibility, with the goal of understanding the most effective and scalable program components, and identifying barriers/challenges for program implementation. Lastly, a primary focus, and the focus of this paper, was on understanding staff perceptions regarding program benefits. Staff responses to interview questions informed the questions developed for volunteers. Volunteer interview questions were designed to understand the program from their perspective: the barriers/challenges, the benefits for volunteers and clients, and their suggestions for improvement. Similarly, client interview questions were informed by previous interviews with staff and volunteers. Client questions were designed to focus on participants’ experiences with the goal of understanding program benefits and challenges.
Participants were recruited from January through September 2022. Staff interviews were conducted from February through March 2022; volunteer interviews from March through May 2022, and client interviews from April through September 2022. Interviews were conducted by telephone or Zoom depending on participant preference. This study was reviewed by the Brown University Institutional Review Board and was determined not to meet the criteria for human subjects research. We did adhere to important ethical standards. Prior to each interview, we used our IRB’s standard informed consent as a guide for obtaining participant verbal consent to participate. At the beginning of each interview, we stated the purpose of the interview, the research objective, that participation was voluntary, that data collected would be de-identified, and that the participant was free to decline answering any questions or stop the interview at any time. After this language, we asked participants if they would like to participate and if the interview could be recorded. Once verbal consent to participate and to audio record was obtained, the interview started. Since our interviews were focused on understanding participant experiences with a social connection program, we did not collect any participant demographic information.
Interviews lasted approximately 1 hour. Two team members participated in each interview for staff and volunteer interviews: one conducted the interview while the other took detailed notes. This approach was also used for five of the ten client interviews at each site. For the remaining five client interviews per site, one interviewer conducted the interview and took notes. Interview summaries were written and reconciled by both interviewers prior to being shared with the entire project team. The approach of having two qualitative team members on each interview ensured adherence to the interview protocol and facilitated team discussions throughout analysis.
Analysis
Transcripts were analyzed using a modified content analysis approach (Strauss & Corbin, 1994). A preliminary coding scheme was first developed based on the interview guide and informed by the interview summaries. This scheme was adjusted iteratively to add and remove codes and refine code definitions. The scheme was then applied to the transcripts by qualitative team members. Three team members individually coded the first three transcripts, meeting weekly for reconciliation, then two team members individually coded eighteen transcripts, meeting weekly for reconciliation. As a high level of agreement was obtained, the remaining transcripts were coded by individual team members. The coded data extracts were then subjected to rigorous examination to identify themes, or patterns of response across the data. In weekly meetings, themes were continually discussed and refined. In addition, a detailed audit trail of developing thoughts and interpretations of the data was maintained (Ritchie et al., 2013).
Results
Program Characteristics.
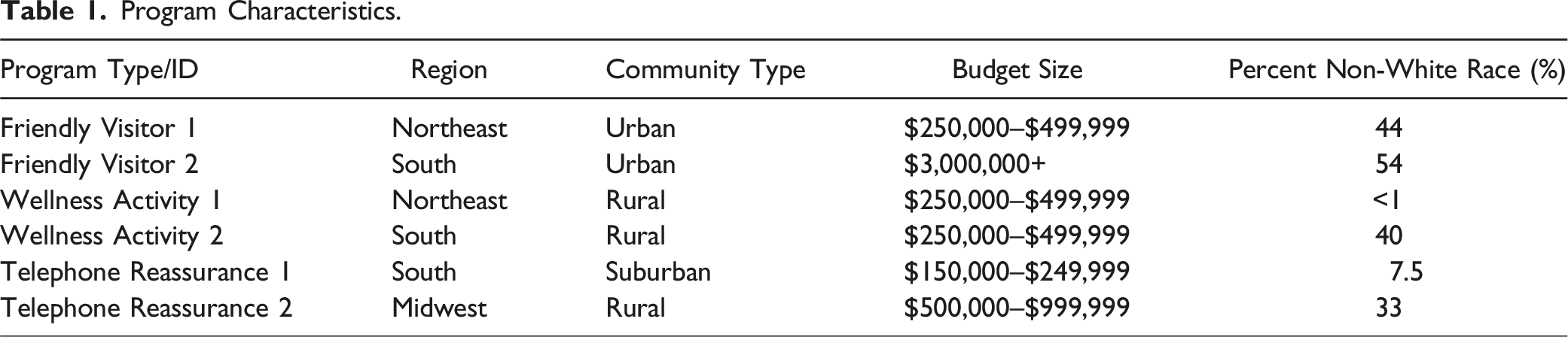
In total, across the six programs, 116 interviews were conducted with 117 participants (one interview included two staff members). This included 31 staff interviews, 30 volunteer interviews, and 55 client interviews. Across all participant types there were 37 interviews conducted with individuals involved with telephone reassurance programs, 38 interviews conducted with individuals involved with friendly visitor programs, and 41 interviews conducted with individuals involved with wellness activity programs. While participant demographic information was not uniformly gathered as part of this study, many interview participants volunteered such details. Based on demographic information provided by program staff during their interviews, interviewed staff had been associated with their respective organizations ranging from less than a year to over 30 years. Many volunteers shared their employment status during interviews, and volunteers included a number of college students but a majority of individuals who had retired. The client participants who shared their age ranged from 72 to 88 years old. Nearly half of the clients interviewed mentioned living alone and many were widowed.
Analysis of interviews with client participants, volunteers, and staff of social connection programs yielded four themes that were consistent across the six programs and different program structures: 1. Clients discussed their rationale or motivation for joining social connection programs including being isolated or lonely, wanting someone to check in on them, a desire for connection or friendship, and wanting to share their knowledge and life experiences with others. 2. Participation in social connection programs was associated with substantial benefits for clients. Reported benefits included friendship, knowing that someone cares about them, being able to contribute and feeling like a person, participation in activities of interest, and reduced loneliness and improved well-being overall. 3. Volunteers and staff described their rationale for getting involved in social connection programming, and reasons included wanting to give back, share knowledge, and/or contribute in some way, especially during retirement, and knowing their work is meeting a societal need. In discussing their motivation for signing up, volunteers further discussed the importance of flexibility provided by this social connection programming. 4. Volunteers and staff also reported deriving substantial benefits from participating in social connection programs. Benefits experienced by volunteers and staff included positive feelings from helping others and meeting their needs, feeling able to contribute and share their expertise, and the development of genuine connections and friendships.
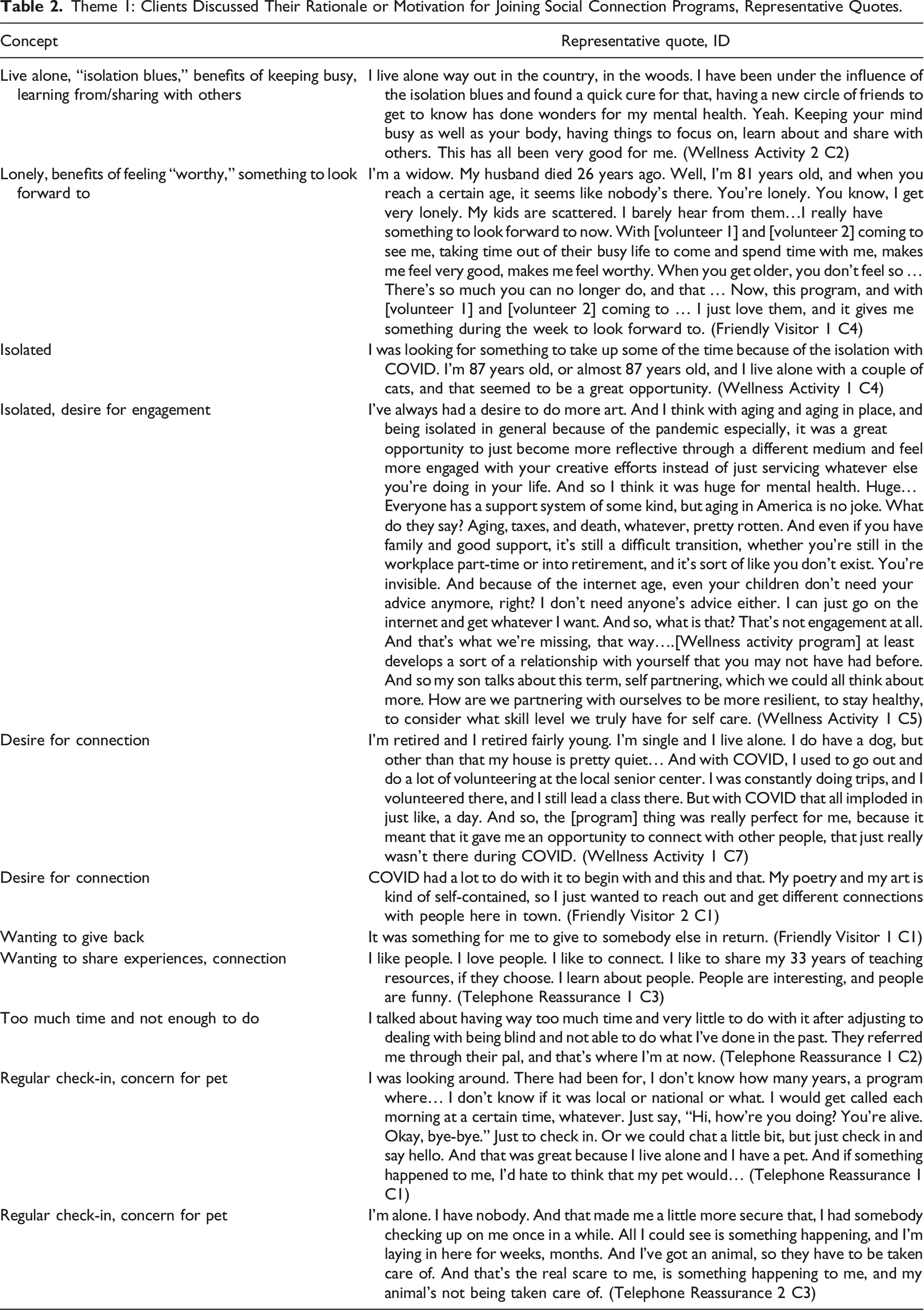
Theme 1: Clients discussed their rationale or motivation for joining social connection programs.
Clients who participated in social connection programs identified a number of reasons why they signed up. Most clients were motivated to join the program because they described themselves as isolated and lonely. Many clients reported living alone and having the “isolation blues” (Wellness Activity 2 C2). One client eloquently described the challenges of aging: Aging, taxes, and death, whatever, pretty rotten. And even if you have family and good support, it's still a difficult transition, whether you're still in the workplace part-time or into retirement, and it's sort of like you don't exist. You're invisible. (Wellness Activity 1 C5)
Theme 1: Clients Discussed Their Rationale or Motivation for Joining Social Connection Programs, Representative Quotes.
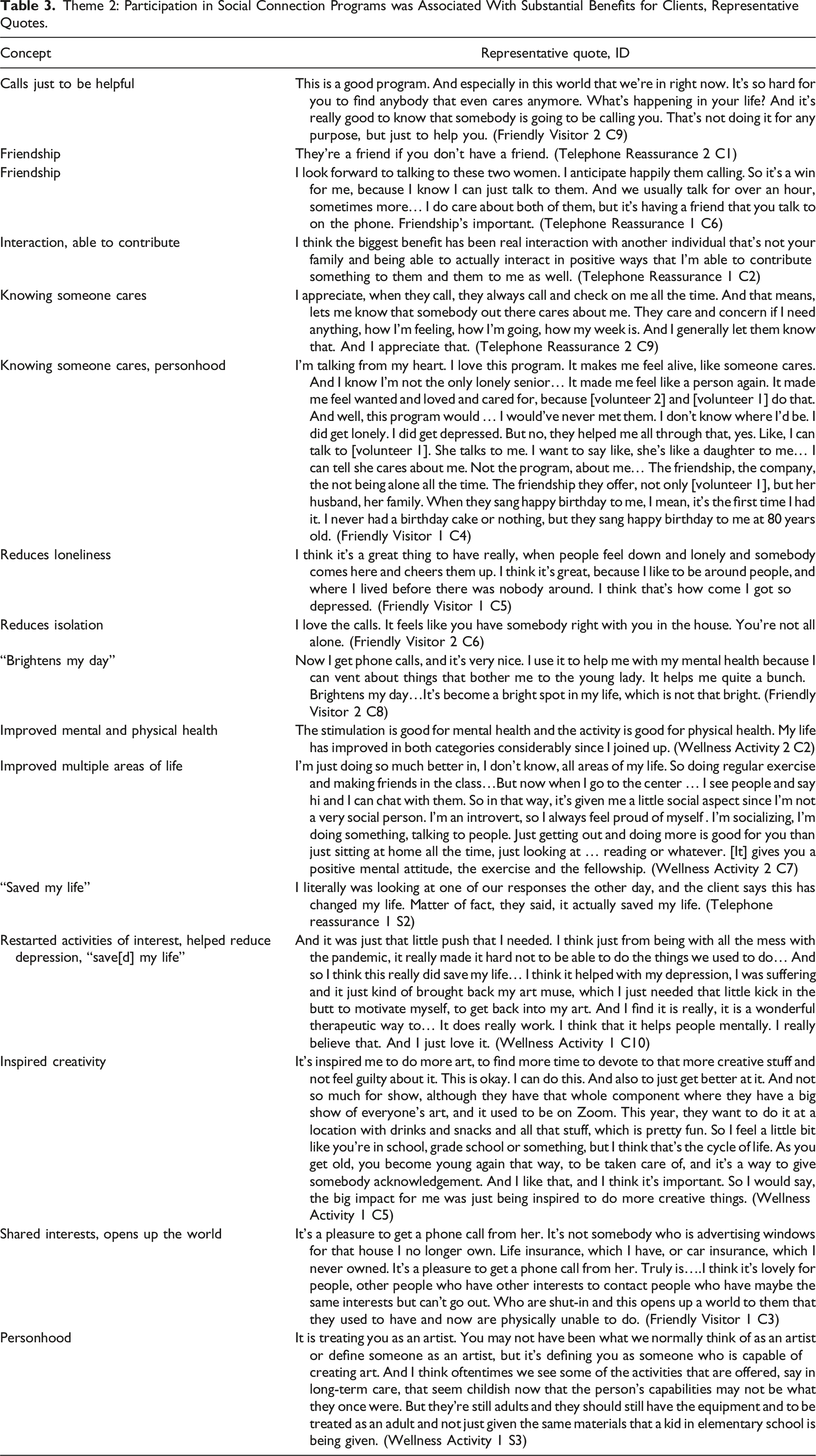
Theme 2: Participation in social connection programs was associated with substantial benefits for clients.
Many of the reasons clients cited for joining social connection programs were realized as reported benefits. During interviews, clients described that participating in the programs resulted in friendships, and also discussed the importance of being able to help others and knowing that someone else cares about you. Clients said that the program reduced their loneliness, brightened their day, improved physical and mental health, and in some cases “saved [their] life” (Wellness Activity 1 C10, Telephone Reassurance 1 S2). In addition, clients expressed that these programs inspired creativity, facilitated the sharing of interests, and supported feeling like a person, with one client sharing: I love this program. It makes me feel alive, like someone cares. And I know I'm not the only lonely senior… It made me feel like a person again. It made me feel wanted and loved and cared for, because [volunteer 2] and [volunteer 1] do that. And well, this program would ... I would've never met them. I don't know where I'd be. I did get lonely. I did get depressed. But no, they helped me all through that. (Friendly Visitor 1 C4)
Theme 2: Participation in Social Connection Programs was Associated With Substantial Benefits for Clients, Representative Quotes.
Theme 3: Volunteers and staff members identified the reasons they became engaged with social connection programming.
Volunteers and staff members also described the reasons they decided to engage in social connection programs. Many of these individuals expressed awareness of the needs of older adults and a desire to reduce isolation and loneliness. For some, this was about paying it forward or was consistent with a belief in the importance of helping others: If I'm not part of the solution, I'm part of the problem. And so it's my goal to go out and try to change somebody's life every single day. I don't care what that looks like. I don't care how I do it, but that's my goal to every day make an attempt to make somebody else's life better. And in doing what we do here at Meals on Wheels, we’re no longer just our Meals on Wheels. I had a dream for this center and to change people's lives. My mom was very ill for the last 15 years of her life. I know what she went through and to have somebody be there to put a smile on her face every day changed her livelihood and it takes so much more effort to be negative than it does to bring joy to somebody's life. This is the best thing I've ever done ever. (Telephone Reassurance 1 S1)
Theme 3: Volunteers and Staff Members Identified the Reasons They Became Engaged With Social Connection Programming, Representative Quotes.

Theme 4: Volunteers and staff reported deriving substantial benefits from participating in social connection programs.
As was the case for clients, volunteers and staff members experienced numerous benefits of their participation in social connection programs, consistent with their reasons for joining. Several expressed the benefits of knowing that they are meeting a need and helping others, including giving “[clients] hope, something to look forward to” (Telephone Reassurance 1 V5). Often, volunteers expressed that the relationships that were built were reciprocal, and “supremely rewarding” (Telephone Reassurance 2 V1). Participants expressed building meaningful relationships and connections, ones which “helped [them] get through the pandemic” (Wellness Activity 2 V1). Volunteers and staff also reported that being a part of these programs provided purpose: I actually had a little bit of anxiety when I first retired because I didn't know ... I thought, “What is my purpose now?” I thought, “I'm going to go back and do some kind of volunteer work again.” …I think it not only helps the lady that I'm visiting, but it actually helps me. Because I feel like I have a purpose... I like to do for people. That's my personality. I guess I'm a nurturer. I just enjoy doing things for people. I feel like I have a purpose, and it just makes me feel better. (Friendly Visitor 1 V1)
Theme 4: Volunteers and Staff Reported Deriving Substantial Benefits From Participating in Social Connection Programs, Representative Quotes.

Discussion
Findings from this qualitative study illustrate that social connection programs are sought after and meet a wide range of needs. For clients, irrespective of the social connection program they participated in (telephone reassurance, wellness activities, or friendly visitor), similar motivations for and perceived benefits from participating in the social connection program were described. Similarly, volunteer and staff interviews highlighted the numerous motivational factors for committing time and effort towards providing and delivering social connection programs in their communities. The U.S. Surgeon General’s advisory on social isolation and loneliness draws on the socio-ecological framework and systems approach as tools with which to describe social connection in American society. We use this model to contextualize our findings below.
Existing research has demonstrated that socially connected individuals live longer (Gronewold et al., 2020; Holt-Lunstad et al., 2015; Shor & Roelfs, 2015). Within this context, the social connection programs provided by community-based organizations fill a critically needed role in the lives of older adults. As our findings indicated, clients, volunteers, and staff reported a variety of reasons that motivated participation in social connection programs. Reasons to participate included factors we consider individually focused, such as reducing loneliness and providing purpose. Often, these individual motivational factors are closely tied to relationships with others. As our interviews revealed, motivational factors to participate in social connection programming also included building relationships with other people: clients, volunteers, and staff reported that they were motivated to participate by a hope to reduce social isolation for themselves and others, a wish to build friendships, and a desire to engage and connect with others. Individual and relationship factors are intricately linked to one’s community and society. For volunteers and staff in particular, community-focused motivational factors such as a desire to give back to their communities and help others were reported. These tiered findings illustrate the intersections and interconnections throughout a community, from an individual client to the overarching community, and by extension society, which create a vast network of critically important social connections for older adults.
Existing social connection programming provides a successful model for addressing social isolation and loneliness in older adults. As our findings showed, clients reported the benefits of participating in social connection programs. These benefits included improved mental and physical health, decreased loneliness, and the opportunity to be creative, physically active, or engaged in other activities. These findings are consistent with prior literature, which found that receiving services from community-based organizations was associated with improved well-being (Helfand et al., 2020; Millen et al., 2002; Rachasrimuang et al., 2018; Thomas et al., 2020). Additionally, these findings add to the evidence base that Meals on Wheels programming is beneficial outside of nutrition (Campbell et al., 2015; Gualtieri et al., 2018; Zhu & An, 2013). For staff and volunteers in our sample, benefits of participation in program delivery were also identified and included personal satisfaction of meeting a need identified in the community, helping others, and a sense of connection and purpose. These benefits are also consistent with prior research on volunteers, which reports that volunteers derive meaningful benefits from their engagement (Filges et al., 2020; Hood et al., 2018; Kim et al., 2020; Population Reference Bureau, 2011; Torres et al., 2023). Existing research has yet, to our knowledge, to examine benefits specifically received by staff of social connection programs.
Findings from this study have important implications. First, our research expands on the existing literature and provides depth regarding the underlying motivational factors that drive people to join or deliver a social connection program. These findings are important as understanding motivation at the individual and relationship level ensures that new programming can meet not only individual goals, but also those of the surrounding community and society: to reduce social isolation and loneliness. Second, to our knowledge, our research is the first to examine the benefits of social connection programs for staff. As community-based organizations recruit new staff and volunteers, it is critically important to be able to demonstrate the benefits of participation, especially in light of declines in volunteerism and workforce challenges. Third, our findings expand the evidence base exploring what motivates individuals to volunteer and work in social connection programming. Previous research has found that people are motivated to do community-based social services work because of pride in the organization and its accomplishments (Colvin et al., 2021; Harmic, 2022; Houston, 2000; Kerschner & Rousseau, 2008; Wright, 2007). Our findings add to this body of work as volunteers and staff from our sample also expressed an explicit desire to connect with others, share knowledge, and feel useful. Lastly, the data provided through these interviews highlight the importance of time and commitment flexibility as a critical component volunteers and staff take into consideration when deciding to engage.
Although this research included a large sample by the standards of qualitative research, results are not intended to be generalizable. Further, our study included participants from six social connection programs representing three program types. Additionally, in order to recruit volunteers and clients to participate in our interviews, we relied on assistance from staff members. This may have meant that we heard from those who had the most positive experiences to report and is consistent with the largely positive information shared by participants and reported in this paper. However, in interviews, we also heard constructive feedback and areas for program improvement, which will be the focus of a subsequent paper. Future research would benefit from recruitment of interview participants with little to no assistance from staff to prevent possible biases, and interviews among more programs in order to encapsulate a broader understanding of how different programs impact outcomes for clients, volunteers, and staff.
Findings of the current study provide critical insights to community-based organizations that operate social connection or other programs seeking to recruit clients, volunteers, and staff. In an effort to develop and support programs that enable social connection, it is imperative to understand the driving factors that motivate individuals to join programs, as well as the resulting benefits that individuals experience. Findings also have implications for organizations that deliver social connection programs: insights into the benefits allow programs to expand or tailor their services to build on those strengths and minimize program weaknesses. Consistent with the Surgeon General’s national strategy to promote social connection through strengthening the infrastructure for social connection in local communities (U.S. Department of Health and Human Services, 2023), our research adds to the evidence base demonstrating the value of community-based social connection programs for homebound older adult clients, as well as volunteers and staff involved in program delivery, which may lend support for continuation and/or increases of funding.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Meals on Wheels America.
Authors Note
Study materials and the interview protocol were sent to the Brown University Institutional Review Board for review and determined to not be human subjects’ research.