
Abstract
Early identification of discharge destination is an important aspect of hospital care for frail older adults. This retrospective cohort study examined whether physical, cognitive and social functioning assessments at admission are associated with discharge destination. Data from 114 community-dwelling patients aged ≥65 years, acutely admitted to a geriatric ward, were analyzed. Frailty was defined at admission by impaired Katz-Activities of Daily Living (ADL) or increased fall risk. Initial screening included Katz-ADL, fall risk and the Malnutrition Universal Screening Tool (MUST). Additional assessments comprised handgrip strength, Timed-Up-and-Go (TUG), Six-item Cognitive Impairment Test (6-CIT) and living situation. Multivariable logistic regression, adjusted for age and sex, showed that worse Katz-ADL scores (OR 1.45, 95% CI 1.18–1.78), lower handgrip strength (OR 2.28, 95% CI 1.02–5.10) and slower TUG performance (OR 11.19, 95% CI 3.40–36.89) were significantly associated with non-home discharge. Cognitive status and living situation were not. These findings indicate that these functional assessments are associated with discharge destination in frail older adults.
• Suggests that Katz-ADL, handgrip strength and TUG at admission are associated with discharge destination in frail older adults. • Highlights the relevance of assessing physical function in older adults during hospital admission.
• May support clinicians by highlighting associations between functional assessments and discharge destination in frail older adults early during hospitalization. • Can inform gerontological practice and policy by integrating simple functional assessments into discharge planning protocols. • Provides a basis for further research on whether associations between functional assessments at admission can be developed into tools to predict discharge destination and optimize care transitions for frail older adults.What This Paper Adds
Applications of Study Findings
Introduction
Of patients admitted to hospitals, 45% are over 65 years of age (Ziekenhuisopname en -patiënten; diagnose-indeling VTV, 2023). Due to the increasing aging population, this proportion is expected to rise (de Rooij SEJA et al., 2009). The prevalence of frailty is estimated at 15% among individuals aged 65 and older, increasing to 20-25% in those aged 85 and older (Buckinx et al., 2015). Frailty is a complex concept, determined by multiple factors, including physical, cognitive and/or social deficits (Gilbert et al., 2018).
During hospital admission, in particular frail older adults risk functional decline and prolonged length of stay (LOS) (Blomaard et al., 2020; Covinsky et al., 2011). In the Netherlands, older and frail patients are, after hospitalization, usually discharged home (with/without care), to geriatric rehabilitation or a nursing home (Leeuwen et al., 2024). To minimize LOS and prevent irreversible decline in frail older adults, early identification of discharge destination is crucial (Covinsky et al., 2011). Currently, discharge destination is usually determined after the patient has spent some time in the hospital and is deemed medically ready for discharge (Covinsky et al., 2011). This is unfavorable, as coordinating home care or institutional placement takes time and thus often results in prolonged LOS (Chen et al., 2022).
More insight into early determination of discharge destination, and the usability of assessments in older patients at admission is therefore warranted. Such assessments are done routinely in many hospitals, but so far, evidence on how these assessments relate to discharge destination is limited. In Dutch hospitals, the initial screening to identify frail patients includes functional ability (Katz-Activities of Daily Living: Katz-ADL) (Katz et al., 1963), fall risk, nutritional status (Malnutrition Universal Screening Tool: MUST) (Baxter et al., 2003) and delirium risk (de Rooij SEJA et al., 2009). These assessments are administered as part of the widely applied VMS (Safety Management System; Veiligheids Management Systeem) screening (de Rooij SEJA et al., 2009). In case of frailty, the assessment can be supplemented with additional functional tests such as handgrip strength (McGrath et al., 2018), the Timed up and Go test (TUG) (Podsiadlo & Richardson, 1991) or gait speed (Gait Speed Test, 2017).
Available studies on factors associated with discharge destination involving hospitalized community-dwelling adults—not explicitly classified as frail—have demonstrated that worse outcomes on functional assessment tools, such as the Katz-ADL, as well as other functional instruments to be completed by the nurse, including the Blaylock Risk Assessment Screening Score and the Barthel Index (D'Souza et al., 2021; D'Souza et al., 2022; Hirota et al., 2023) and performance-based measures such as the De Morton Mobility Index (D'Souza et al., 2021), were associated with discharge destinations other than home. However, the strength and consistency of these associations varied largely and the populations did not specifically concern frail elderly. Regarding frail older adults in particular, three Dutch studies reported an associations between a worse TUG test performance (ability to perform or test score) and discharge destination not to home (Bolderman, 2017; Leeuwen et al., 2024; Smits & Scheer, 2021). Two of these studies investigated handgrip strength (Leeuwen et al., 2024; Smits & Scheer, 2021), of which only one found an association with discharge destination (Leeuwen et al., 2024), with similar results. Additionally, these studies explored the role of cognitive functioning (Bolderman, 2017; Leeuwen et al., 2024; Smits & Scheer, 2021) and social functioning (Leeuwen et al., 2024), with only one study demonstrating an association between worse cognitive functioning and the discharge destination not being home (Leeuwen et al., 2024). Importantly, none of these studies included nutritional status or dependency on informal caregiving as potential determinants, whereas these aspects are included in the initial screening for frailty as well. Identification of all factors incorporated into routine care that could potentially be associated with discharge destination could aid in developing an efficient assessment battery and facilitate early care planning interventions to support either home return or institutional placement, with shortening of LOS and reducing functional decline as ultimate aim. As such, there is a clear need for studies in acutely hospitalized frail older adults that integrate multiple observational and performance measures—including handgrip strength, gait speed and TUG—as well as nutritive, cognitive and social elements. The aim of the present study was therefore to examine whether physical, cognitive and social functioning assessments at admission were associated with discharge destination in frail older adults who were acutely admitted to a hospital.
Methods
Design
This retrospective observational study used routinely collected healthcare data from January 2023 to August 2024 at the Clinical ward of Geriatric Medicine of Leiden University Medical Center (LUMC). The study was judged as not falling under the remit of the Dutch Human Medical Research Act (Wet Wetenschappelijk Onderzoek met Mensen, WMO) by a hospital scientific review board (ref nr: 2023-029). Oral consent for data usage was obtained from all participants by the physiotherapist during the physical assessments and documented in the electronic patient record. Data from the first 49 patients participating in this study have been published previously (Leeuwen et al., 2024). The present study reports on a larger sample of 114 patients and includes additional variables such as nutritional status and informal care.
Setting
In routine care, all patients aged 65 and older are screened for frailty by a nurse using the Safety Management System (Veiligheid Management Systeem, VMS) screening upon acute hospital admission at LUMC (de Rooij SEJA et al., 2009). The screening process is illustrated in Figure 1. The physical domains of frailty in the VMS include physical functioning (Katz-ADL) and a fall risk score. A positive score on one or both domains, leads to an additional assessment by both a physiotherapist and a geriatric nurse specialist. The physiotherapist performs additional physical assessments (handgrip strength, TUG and gait speed). The additional assessment by the geriatric nurse specialist includes cognitive functioning (Six-item Cognitive Impairment Test (6-CIT)) and social functioning (including living situation and need for informal caregiving) (Tuijl et al., 2012). Regarding the admission of the patients, if there is frailty without an indication for admission to a specific specialist ward (such as neurology, cardiology or orthopedics), patients are admitted to the general geriatric ward, which is specialized in the care of frail older adults. Discharge is determined biweekly in a multidisciplinary meeting considering all assessments and diagnostics. Procedure for screening of frail older adults during hospital admission at Leiden University Medical Center in the geriatric ward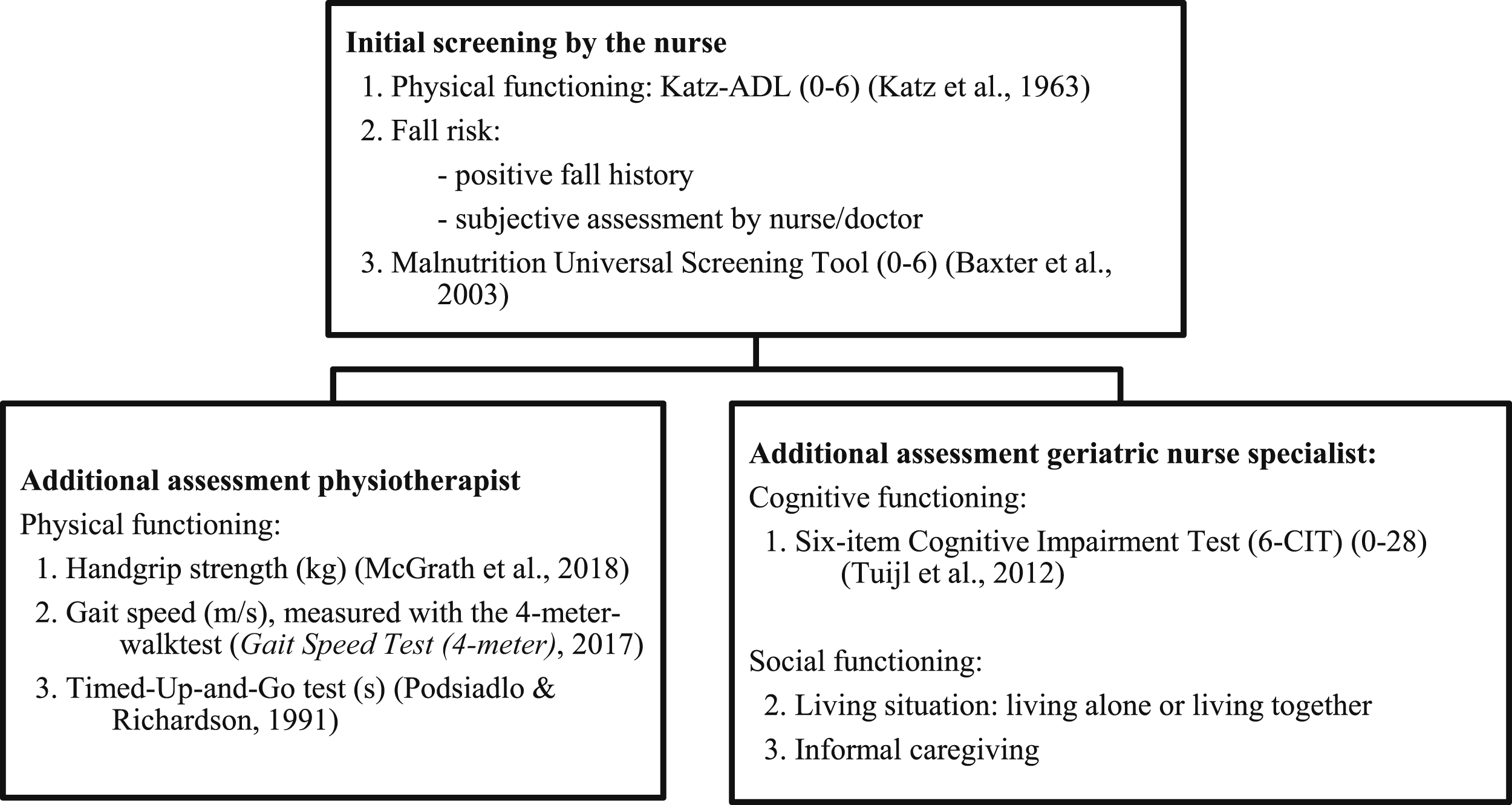
Patient Inclusion
For this study, patients were included if they were ≥65 years old, acutely admitted to LUMC, lived independently prior to admission, admitted to the geriatric ward, screened positive for frailty in the physical domains of fall risk or limitations in daily functioning using the VMS screening and were deemed eligible for additional assessment by a nurse and physiotherapist within the first week after admission. Exclusion criteria were inability to follow instructions during the physiotherapist screening due to cognitive impairment or language barriers, lower extremity fractures with weight-bearing restrictions interfering with physical testing and objection to the use of pseudonymized data. Patients who provided consent but died or were transferred to hospice or another hospital during admission were excluded, as they constituted a distinct group with often early-established palliative care plans, for whom discharge destination was not applicable.
Measurements
Demographic Data, Data on Admission and Discharge
Demographic data included age (years), sex (male/female), disease severity (assessed based on the method of arrival at the emergency department, specifically whether the patient arrived by ambulance or not (de Gelder et al., 2016)), main reason for admission (categorized as functional decline or fall, infections, cardiac conditions or other medical conditions), Charlson Comorbidity Index (CCI) (cumulative value of present comorbidities regarding the risk of death and severity of the condition ranging from 0 to 37) (Charlson et al., 1987), number of different medications at hospital admission, length of stay (days), delayed discharge days (days) (defined as the difference between when a patient is medically ready for discharge and the actual discharge date) and duration between hospital admission and in hospital physiotherapy consultation (days). Assessments performed during the initial VMS screening and subsequent assessments are described in Figure 1.
Initial VMS Screening (Nurse)
Katz-ADL
The Katz-ADL scale is used to assess physical functioning by evaluating the level of physical dependency in six domains of daily living. The scale ranges from 0 to 6, with higher scores indicating greater dependency. A score of 6 reflects full dependency in performing ADL, while a score of 2 or higher suggests significant impairment in physical functioning and is generally considered a poor outcome (de Rooij SEJA et al., 2009; Katz et al., 1963).
Fall Risk Score
A history of falls in the past 6 months and/or the subjective judgment of the nurse regarding an increased risk of falls determines indicate an increased risk of falls (de Rooij SEJA et al., 2009).
Malnutrition Universal Screening Tool (MUST)
The MUST is a screening tool utilized to assess the severity of malnutrition. It comprises three questions concerning BMI, food intake and acute illness, each assigned a score ranging from 0 to 2. The cumulative score ranges from 0 to 6, with a score of 2 or higher indicating a high risk of malnutrition (Baxter et al., 2003; de Rooij SEJA et al., 2009).
Physical Therapy Assessment
Handgrip Strength
Handgrip strength (HGS) was measured in kilograms (kg) using the Jamar handgrip dynamometer (Sammons Preston Rolyan, Bolingbrook, IL) following a previously published protocol (McGrath et al., 2018). A cutoff value of <16 kg for women and <27 kg for men was used to distinguish between normal or low HGS (Cruz-Jentoft et al., 2019).
Timed-Up-and-Go Test
The TUG measures the time (in seconds) required for a patient to rise from a chair, walk 3 m, walk back and sit down again (Podsiadlo & Richardson, 1991). A cutoff of ≥20 seconds indicates and increased fall risk and was used in this study to define a “reduced score” (Cruz-Jentoft et al., 2019; Podsiadlo & Richardson, 1991). Patients were allowed to use their personal walking aid and/or orthosis, but no physical assistance or verbal encouragement was permitted during the test (Podsiadlo & Richardson, 1991).
Gait Speed
Gait speed was measured using the 4-m Gait Speed Test (4MGST). This test involved measuring the time (in seconds) it took participants to walk a distance of 4 m (Gait Speed Test (4-m), 2017). Outcomes were categorized into three groups: (1) test not performable if participants exceeded the maximum allowable time of 30 seconds to complete the test or were unable to complete the 4MGST, (2) 0.1–0.8 m/s, and (3) > 0.8 m/s (Cruz-Jentoft et al., 2019; Studenski et al., 2011).
Geriatric Nurse Assessment
Cognitive and Social Functioning
Cognitive functioning was assessed using the Six-item Cognitive Impairment Test (6-CIT) (0-28) (Tuijl et al., 2012). This questionnaire comprises six items, each scored on a scale of 0 to 10. A higher total score indicates greater cognitive impairment (Brooke & Bullock, 1999; Tuijl et al., 2012). Pre-existing diagnosed cognitive disorders, inability to complete the 6-CIT due to cognitive impairment or delirium, or a 6-CIT score greater than 7 were considered indicative of impaired cognitive functioning (Brooke & Bullock, 1999). Social functioning was evaluated based on participants’ living arrangements (alone or with others) and the presence of informal caregiving support (with or without an informal caregiver).
Discharge Destination
Due to the limited number of patients discharged to a nursing home, the categories geriatric rehabilitation and nursing home were merged to distinguish only between “discharge to home” and “not to home.”
Statistical Analyses
Patient data were extracted from the electronic patient record system Healthcare Information eXchange (Hix, Chipsoft, Amsterdam, the Netherlands) by the Information and Communication Technology (ICT) department. Data were pseudonymized stored and analyzed using SPSS (IBM SPSS Inc., Chicago, Illinois, version 25). Continuous variables were reported as means with standard deviations, or as median with ranges, based on their distribution. Data normality was assessed visually using histograms and Quantile-Quantile (Q-Q) plots. Categorical variables were reported as frequencies and percentages. An initial assessment was conducted to evaluate whether missing data were completely at random. All missing values were then examined to identify potential reasons for their absence. When more than 10% of the data was missing and in order to determine whether the missing could be classified as random, the characteristics of patients whom the data were missing were compared to those of patients of whom data were available. Comparisons were performed using the independent samples t-test or the Mann–Whitney-test for continuous variables and the Chi-Square test or Fisher’s Exact test for categorical variables (de Vocht, 2017). The same statistical methods were used to univariately assess whether the risk factors evaluated during the initial screening (Katz-ADL, VMS-fall risk score, MUST), physical therapist assessment (handgrip strength, TUG, gait speed) or geriatric nurse specialist assessment (6-CIT, living situation), as well as length of stay, were associated with discharge destination groups (home versus non-home). Multivariable logistic regression analyses were conducted separately, each including one independent variable that showed a statistically significant association with the dependent variable in the univariate analysis (P < 0.10), adjusted for age and sex, to examine associations with discharge destination (home vs. non-home).
Results
Between January 2023 and August 2024, 156 patients were acutely admitted to the geriatric ward and received physical therapy consultation. Of these, 146 met the inclusion criteria. Consent was due to logistic reasons not requested from 14 patients and 2 patients declined to provide consent for data use, resulting in the inclusion of 130 patients. After 10 patients died, 3 were transferred to a hospice and 3 to another hospital, data from 114 participants were analyzed (Figure 2). Patient flow diagram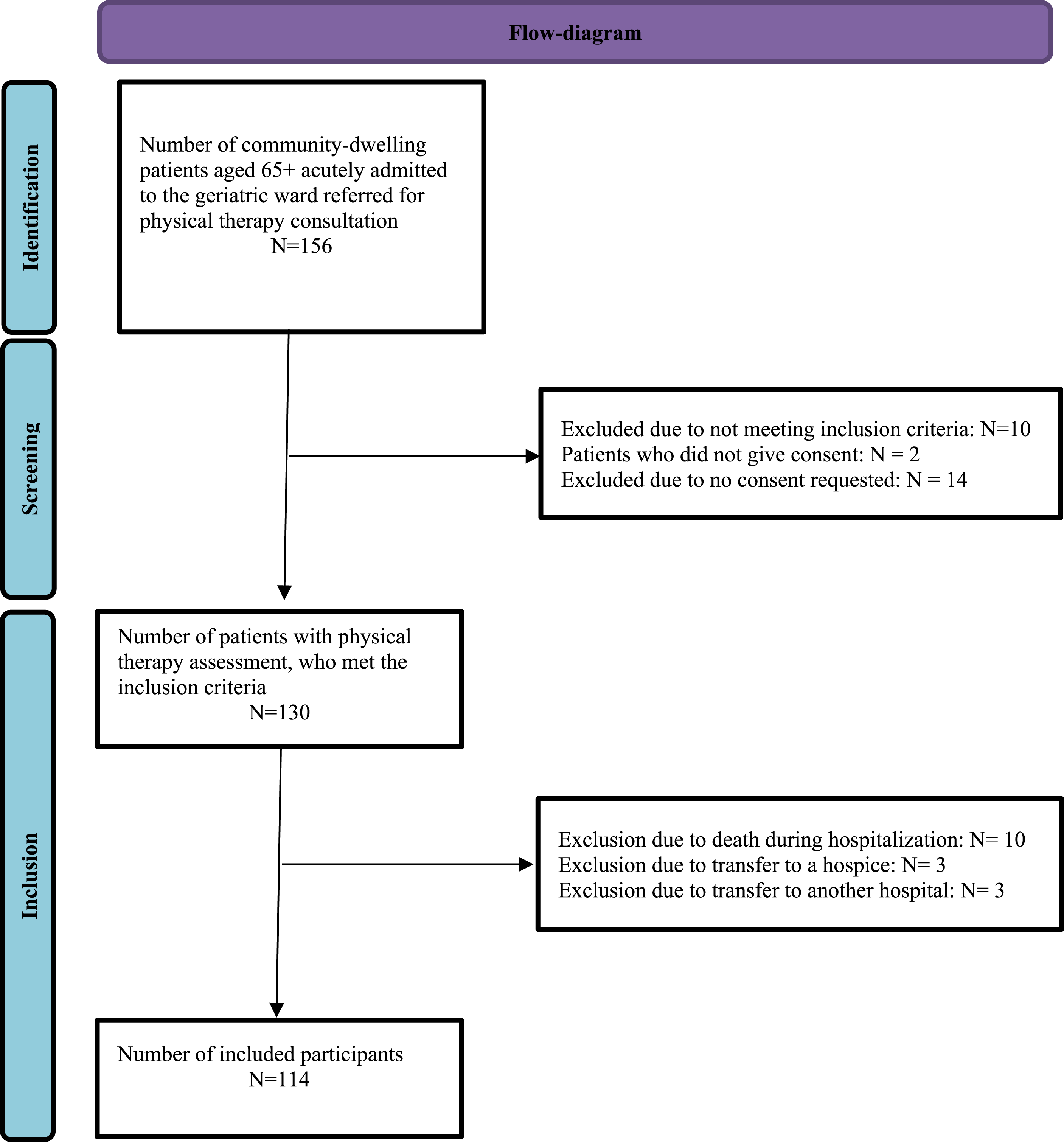
Data were available for 92% or more of patients across all variables, except the TUG (83%), which was not performed due to isolation or visitors (n = 4) or for unknown reasons (n = 16). Patients without TUG data were more often male (75% vs. 48%, p = 0.03), had a higher Charlson Comorbidity Index (8.2 vs. 6.8, p = 0.02) and more often showed high gait speed (36% vs. 27%, P = 0.02; see Supplemental Material). TUG data were therefore not considered missing at random.
Patient characteristics of frail older individuals and their hospital stay at the Geriatric Ward: group differences between discharge destinations to home and not to home
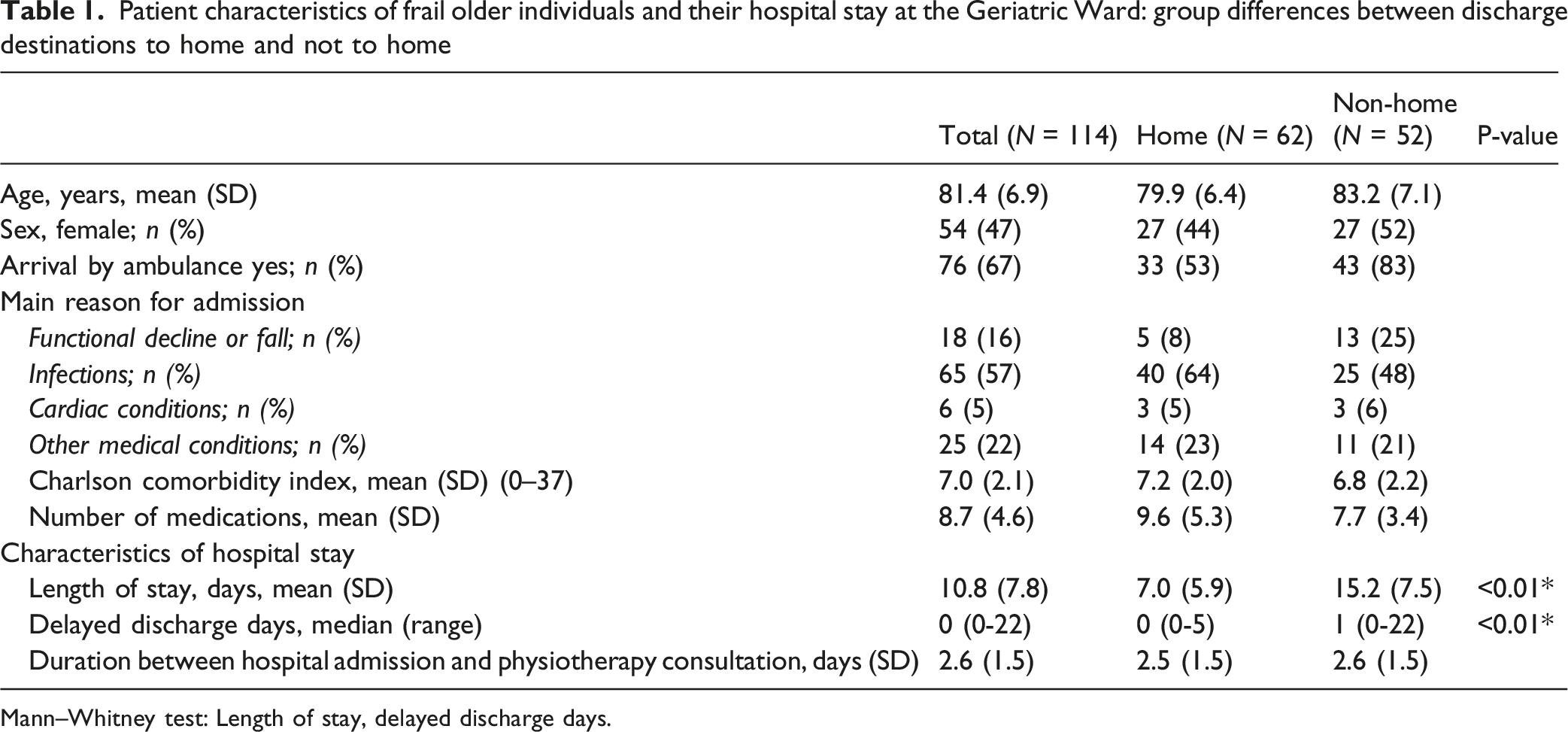
Mann–Whitney test: Length of stay, delayed discharge days.
Screening and assessment outcomes of frail older adults admitted to the Geriatric Ward and their comparisons between discharge destinations to home and not to home
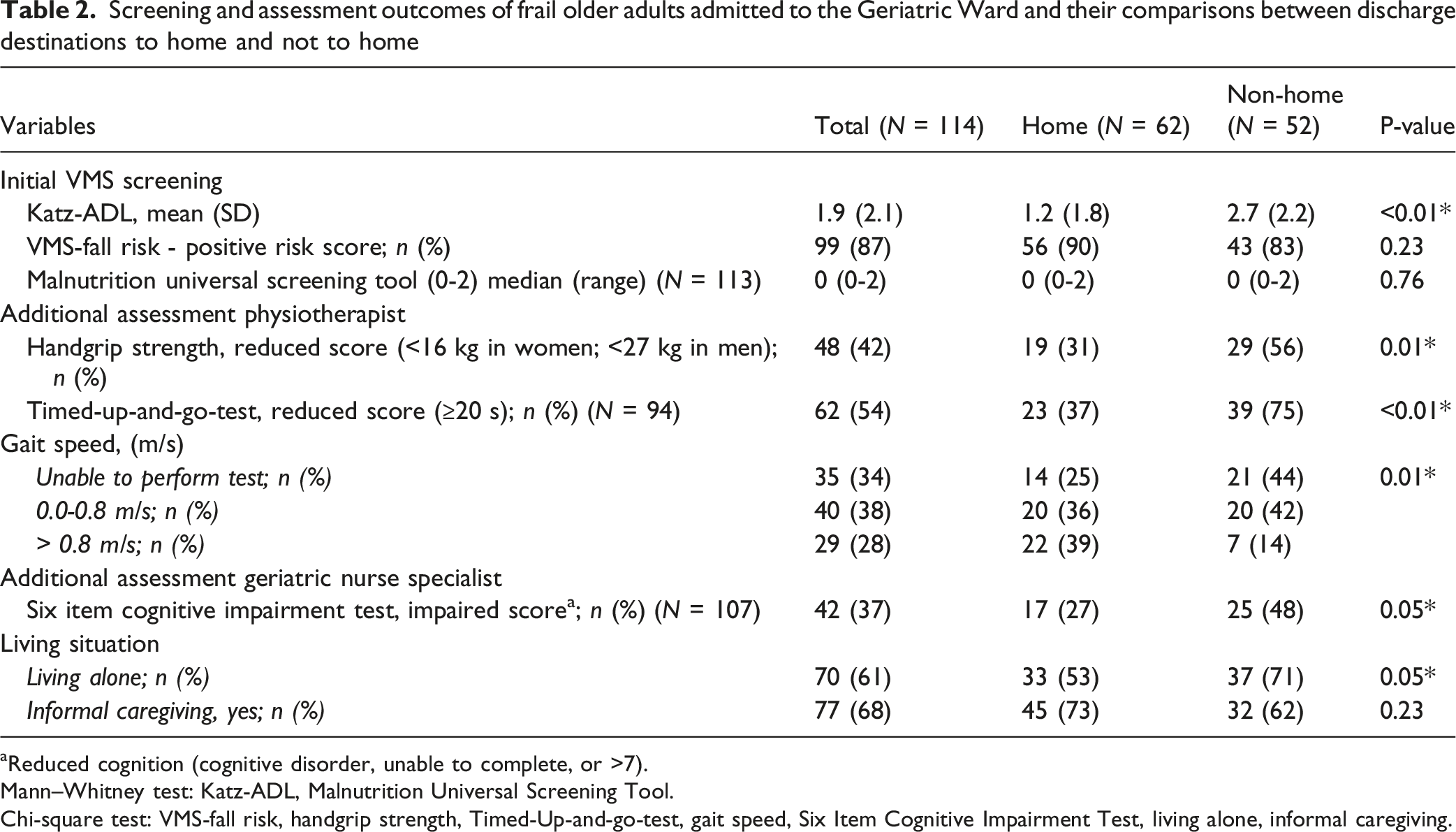
aReduced cognition (cognitive disorder, unable to complete, or >7).
Mann–Whitney test: Katz-ADL, Malnutrition Universal Screening Tool.
Chi-square test: VMS-fall risk, handgrip strength, Timed-Up-and-go-test, gait speed, Six Item Cognitive Impairment Test, living alone, informal caregiving.
Multivariable Analysis
Multivariable logistic regression analyses for discharge destination not to home for frail older adults admitted to the geriatric ward for the initial screening and the additional assessments all adjusted for age and sex
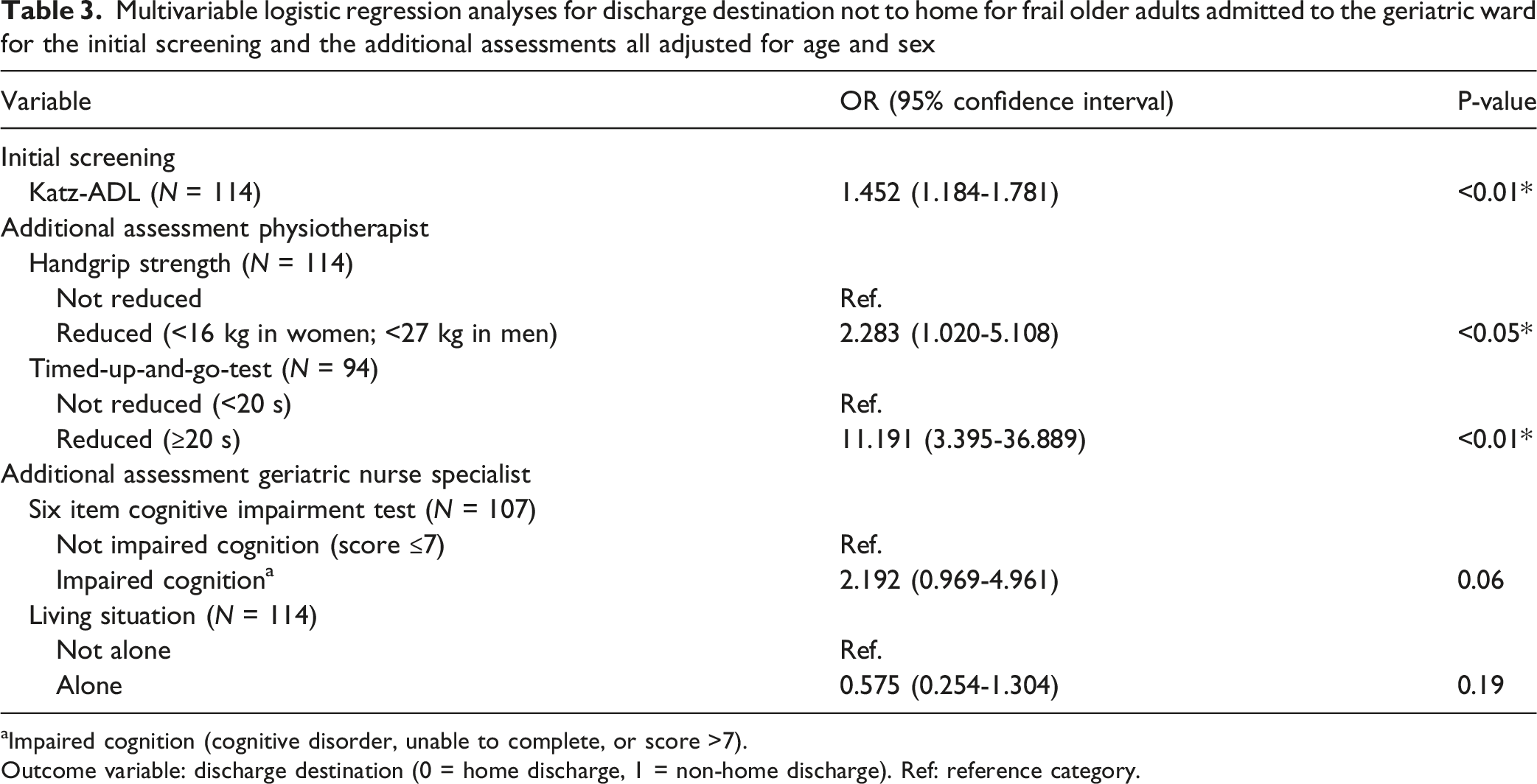
aImpaired cognition (cognitive disorder, unable to complete, or score >7).
Outcome variable: discharge destination (0 = home discharge, 1 = non-home discharge). Ref: reference category.
Discussion
In frail older adults acutely admitted to a hospital, a higher Katz-ADL score, poor handgrip strength and a worse TUG-score were significantly associated with not being discharged home. Furthermore, patients who were not discharged home had a longer hospital stay. The findings of this study provide both a valuable confirmation of existing knowledge and a significant contribution to understanding the association between patient characteristics at presentation and the likelihood of being discharged home or not.
Our study confirms previous international findings that overall the outcomes of functional assessment tools are associated with discharge destination (D'Souza et al., 2021; D'Souza et al., 2022; Hirota et al., 2023). Regarding the TUG, two studies also found and association between TUG and discharge destination (Bolderman, 2017; Smits & Scheer, 2021). However, it should be noted that these studies used a different interpretation of the TUG test (i.e., ability to perform the test: yes/no) (Bolderman, 2017; Smits & Scheer, 2021). For HGS, a previous study did not find an association (Smits & Scheer, 2021). However, similar to the TUG, different cutoff values were applied. This contrasts with the current study, in which cut-off values for HGS and TUG were interpreted according to the international guideline of sarcopenia (Cruz-Jentoft et al., 2019).
In contrast with previous studies and our expectations, malnutrition and informal caregiving were not associated with discharge destination in the univariate analyses. For living situation, an association with discharge destination was observed in the univariate analysis; however, this association was no longer present after adjustment in the multivariable model. This contrasts with studies in community-dwelling older adults, in which living situation has been associated with independent living at home (Ahlqvist et al., 2016; Molenaar et al., 2023). This discrepancy may be explained by differences in study populations, as the present study included frail hospitalized older adults, in whom the factors associated with discharge destination may differ. Furthermore, regarding malnutrition no patient scored 3 or higher on the MUST, suggesting that its stratification may be inadequate for this population.
Overall, the comparison of our study with previous research differs in that our population had a higher comorbidity burden (CCI), longer hospital stays, and a higher prevalence of cognitive impairment (Bolderman, 2017; D'Souza et al., 2021; D'Souza et al., 2022; Hirota et al., 2023; Smits & Scheer, 2021). This may be due to a selection bias since our study was conducted in an academic hospital, whereas prior studies took place in non-academic hospitals (Bolderman, 2017; Smits & Scheer, 2021). Additionally, earlier studies focused on community-dwelling older adults who were not classified as physically frail (D'Souza et al., 2021; D'Souza et al., 2022; Hirota et al., 2023), while our study included patients at increased risk of frailty based on physical limitations or fall risk. The higher prevalence of cognitive impairment in our cohort may also be due to the exclusion of patients with cognitive deficits in previous studies, which often omitted frail older adults (Bolderman, 2017; Smits & Scheer, 2021).
Our study is unique as the analysis was conducted in accordance with the sequence of assessments in clinical care, following a standardized protocol. Notably, during the initial assessment, the Katz-ADL showed a clear association with discharge destination. However, the added value of subsequent assessments remains to be determined. Further exploration of this requires a significantly larger study population, allowing for the simultaneous inclusion of more variables in the analysis. Additionally, the group that did not qualify for a physiotherapeutic assessment should also be considered.
A key strength is the systematic, multidisciplinary screening of frail older patients at LUMC. This comprehensive assessment, which included key determinants such as gait speed, TUG, handgrip strength, living situation, caregiver status, malnutrition and cognitive function, strengthened the multivariable design and data quality. Since multiple factors are associated with discharge destination, this multidisciplinary assessment is important in this context.
Several limitations should be noted. The retrospective design resulted in incomplete or missing data. The small sample size and limited number of patients discharged to nursing homes hindered differentiation between discharge to geriatric rehabilitation and nursing home care. Sample size constraints also restricted the inclusion of several variables in the multivariable analysis. The single-center design limited predictive modeling due to a homogenous population. The measurement instruments used in this study were also routinely applied during hospitalization to guide multidisciplinary discharge planning. As the data were collected retrospectively from routine care, the assessments and the discharge destination may not have been fully independent, potentially introducing information bias, which could have influenced the observed observations. Our findings apply only to patients discharged to home, geriatric rehabilitation or a nursing home. The exclusion of those with different care trajectories may have influenced the characteristics of the study population. Established cut-off values were used for handgrip strength, TUG, 4-m Walk Test, and the 6-CIT. Patients unable to complete a test due to severe physical or cognitive limitations were classified as having a reduced performance or impaired cognition. Excluding these patients could have introduced selection bias, so their inclusion ensured a more representative sample. Although dichotomizing measures may reduce statistical power compared with continuous scores, it maintained clinical interpretability and allowed inclusion of patients with the most severe limitations. Additionally, patients who were unable to perform the physical tests due to severe cognitive impairment or language barriers were excluded from these analyses, which may have led to underrepresentation of individuals with more severe cognitive limitations. Finally, while key determinants were analyzed, other factors affecting independent functioning at home, such as environmental and psychological variables, were not included (Ahlqvist et al., 2016; Gobbens et al., 2010; Molenaar et al., 2023).
Conclusion
This study demonstrates that Katz-ADL, handgrip strength and TUG, routinely assessed during hospital admission, are associated with discharge destination in frail older adults. Further research with larger, more diverse cohorts across multiple hospitals is needed to investigate whether these associations can be translated into predictive tools or inform interventions.
Supplemental Material
Supplemental Material - Physical, Cognitive and Social Characteristics of Frail Older Adults Associated With Their Discharge Destination Following Hospitalization
Supplemental Material for Physical, Cognitive and Social Characteristics of Frail Older Adults Associated With Their Discharge Destination Following Hospitalization by Manon K. van Leeuwen, Marieke S. van Dam, Frederique A. de Croock, Inge J. Perquin, Thea P. M. Vliet Vlieland, Maaike G. J. Gademan, Frederiek van den Bos in Journal of Applied Gerontology.
Footnotes
Ethics Considerations
The study was judged by the hospital scientific review board as not falling under the remit of the Dutch Medical Research Involving Human Subjects Act (ref. no.: 2023-029).
Consent to Participate
For this retrospective study, oral consent was obtained for the use of data, which was documented in the electronic patient record.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.