
Abstract
Intimate partner violence (IPV) is a pervasive problem in the United States affecting every demographic group. Victims of IPV suffer a wide range of negative health issues including depression, anxiety, and loss of self-esteem. However, little is known about help-seeking behaviors among IPV victims. This study utilized a university sample to explore who seeks counseling for exposure to threatening IPV. Results revealed that older students and females were more likely to seek counseling than younger students and males. Students who were exposed to greater levels of IPV and reported greater emotional distress were more likely to seek counseling than those with lower exposure to IPV and distress. Importantly, victimization accompanied by emotional distress was the key to explaining help-seeking help behavior. Programs and policies should focus on outreach to young students and males who have experienced IPV and provide focused services to victims with high levels of emotional distress.
Introduction
According to the National Intimate Partner and Sexual Violence Survey, over 35% of women and 28% of men in the United States have experienced some form of intimate partner violence (IPV) in their lifetimes, including stalking, rape, and/or physical violence (Black et al., 2011). Sexual violence, stalking, and IPV victimization are most prevalent among individuals under the age of 25 (Breiding, Chen, & Black, 2014). Therefore, the prevalence of IPV victimization among college and university students, the majority of whom are emerging adults, warrants considerable attention. This is particularly true because a sizeable number of students have experienced IPV prior to coming to college (Forke, Myers, Catallozzi, & Schwarz, 2008; Vagi, Olsen, Basile, & Vivolo-Kantor, 2015). Female college students are more likely than males to experience emotional, physical, and sexual victimization at the hands of intimate partners (Forke et al., 2008). However, it is important to note that many college students who have experienced IPV as perpetrators or victims may not recognize their experiences as abuse (Fass, Benson, & Leggett, 2008; Mummert, Policastro, & Payne, 2014) and forgo any reporting or help-seeking behaviors. Regardless, the negative consequences of IPV for students’ social, mental, emotional, and physical health are no less problematic.
Holistically, victims of IPV report emotional and mental health consequences ranging from fear and safety concerns to posttraumatic stress disorder (PTSD) and the need for crisis housing, legal, and other victims’ advocate services (Kilpatrick et al., 2003; Posick, 2014). Considering the wide-ranging negative emotional consequences of IPV, college campuses provide an opportunity for victimized students to seek and receive much-needed mental health treatment. Many colleges and universities are self-contained communities with independent law enforcement agencies, medical services, counseling centers, housing, legal, and other support services. Therefore, college students have access to health care and other services that may not be available in the broader community. This is particularly true in rural areas where significant shortages in mental health care often leave residents without adequate access to necessary services (Gamm, Hutchison, Dabney, & Dorsey, 2003; Human & Wassem, 1991).
The American College Health Association (ACHA) National College Health Assessment collects data from college students annually across multiple types of campuses nationwide. These data reveal that the proportion of college students who report depression diagnoses has increased from 10% to 15% since 2000 (ACHA, 2000, 2008). This increase in serious mental illness reflects a broader national trend of increased help-seeking behavior, although the severity of psychiatric symptoms reported by mental health professionals on college campuses has also increased (Hunt & Eisenberg, 2010). College students who report stressful interpersonal relationships and females who have experienced sexual victimization are particularly at risk for negative mental health outcomes (Blanco et al., 2008; Stepakoff, 1998). Consequently, colleges and universities must pay particular attention to this group of victimized students to ensure that needed mental health services are delivered appropriately to victims.
Despite the growing body of literature on IPV, and specifically research on dating violence and sexual assault among college students, questions remain regarding what factors affect help-seeking behaviors among college students. In particular, how do students’ IPV victimization status, prior experiences with IPV, levels of emotional distress, and demographics affect their likelihood of seeking counseling? This gap in the literature is particularly stark regarding college students in rural areas, who may lack important resources to effectively treat the negative consequences of victimization. At the same time, colleges in rural areas may provide services that are otherwise unavailable in the surrounding community, as many campuses provide counseling at little to no direct cost to the student (National Institute of Mental Health, 2012).
To date, we still know very little about what factors are associated with exposure to IPV, negative symptomology, and the likelihood of students to seek mental health services. The interplay between these factors is also not well understood. To explore these remaining questions, we use a sample of students from a southern university situated in a rural area. Insight into the answers to these questions is critical for developing specific campus programs and policies targeted at both victims and offenders (as well as the campus writ large) both to decrease incidents of IPV and get the help needed to those who are exposed to IPV.
Victimization and Negative Emotions
Research indicates that victimization in general is related to a wide variety of negative mental health outcomes ranging from depression and anxiety to PTSD (Kilpatrick et al., 2003; Posick, 2014). Similarly, the IPV literature establishes numerous negative mental health effects among individuals who have been victimized by their partners (Coker et al., 2002; Dutton et al., 2006; Hines & Douglas, 2011; Pico-Alfonso et al., 2006; Stein & Kennedy, 2001). Studies based on college student samples identify an association between IPV victimization and heightened risk of depression and anxiety (Harned, 2001; Kaura & Lohman, 2007; Scherer, Snyder, & Fisher, 2013). For example, a study of 863 female college students found that dating violence victims exhibited higher scores on psychological problem indices than nonvictims for depression, anxiety, hostility, somatization, and interpersonal sensitivity (Amar & Gennaro, 2005). When focusing on polyvictimization, research suggests that college students who experience multiple forms of dating violence are at an increased risk of exhibiting posttraumatic stress symptoms (Straus & Sabina, 2008). Collectively, this evidence suggests that college students, like victims of crime and IPV in general, are likely to experience a host of negative emotions as a result of being victimized by an intimate partner.
Although negative emotional responses have been linked to IPV for all victims, research indicates significant sex differences in the prevalence, severity, and type of emotional consequences of IPV. For example, Ansara and Hindin (2011) found that among Canadian victims of IPV, only 4–6% of women reported that experiencing violence had no effect on them compared to 16–31% of men. Relatedly, female IPV victims, and low-income women in particular, reported numerous subsequent serious health problems (Dutton et al., 2006; Sutherland, Sullivan, & Bybee, 2001). In a review of 75 studies conducted between 2006 and 2012, Dillon, Hussain, Loxton, and Rahman (2013) identified a consistent pattern indicating that female IPV victims are more likely to report mental health problems including depression, anxiety, and PTSD. Further, their review highlighted an association between IPV victimization and attempted suicide, as well as suicidal ideation, among abused women.
A growing body of longitudinal research has begun to establish the lasting effects of exposure to violence by linking IPV to long-term poor mental health outcomes. A recent study relying on longitudinal data established that female victims of IPV were at an increased risk of developing depression, as well as a higher risk of reporting of symptoms of psychosis (e.g., mania, paranoia, hallucinations), compared to nonvictims (Ouellet-Morin et al., 2015). One developmental study by Exner-Cortens and colleagues (2013) used data from the National Longitudinal Study of Adolescent Health to explore the relationship between teen dating violence victimization and a variety of negative mental health outcomes in young adulthood. They found that psychological IPV victimization in adolescence was related to a heightened risk of suicidal ideation in adulthood among males and an increased risk of heavy episodic drinking among women. Females who reported experiencing both physical and psychological IPV in adolescence were at increased odds of experiencing depression and reporting suicidal ideation as adults (Exner-Cortens, Eckenrode, & Rothman, 2013). Considering the wealth of evidence pointing to both widespread and long-lasting mental health consequences of IPV victimization, particularly among college students and women, the present study examines the relationship between college students’ victimization status, levels of emotional distress, and help-seeking behavior.
Help-Seeking Behavior
IPV is underreported, and research suggests that many victims do not reach out for help from formal agencies like the police and/or social service providers (Coker et al., 2002; McCart, Smith, & Sawyer, 2010; Tsui, Cheung, & Leung, 2010; Wolf, Ly, Hobart, & Kernic, 2003). Victims of IPV who do reach out for help often rely on informal sources of social support such as friends and family (Amar & Gennaro, 2005; Douglas & Hines, 2011; Sabina, Cuevas & Schally, 2011; Sabina & Ho, 2014; Sylaska & Edwards, 2014). Studies of college students underscore similar patterns of help-seeking behavior among this specific population. In a study of 200 college students, Prospero and Vohra-Gupta (2008) found that while 86% of students indicated experiencing some form of IPV, only 16% sought help from a mental health provider. Similarly, Amar and Gennaro (2005) found that only 3% of their sample of college students who had been victimized by an intimate partner received services from a mental health provider, despite almost one third meeting the criteria for a mental health disorder diagnosis. It appears that victims of IPV, especially students, are not seeking help which they might urgently need.
Despite the overall lack of help-seeking among college students victimized by an intimate partner, services provided by colleges and universities, and delivered on campus, are particularly important for this special population of young adults. College campuses are often self-contained communities that provide their own medical, counseling, and other services for students; therefore, the importance of these services for victims of IPV should not be discounted. Indeed, research indicates that campus physical and mental health services are utilized most often by college students who experience sexual assault and dating violence (see Sabina & Ho, 2014). Nasta et al. (2005) found that 22% of undergraduate women who were sexually assaulted utilized on-campus services for help related to the assault, compared to only 6% who sought help off campus. Few studies have examined service utilization in cases of dating violence among college students, thus a significant gap in the literature surrounds what factors are associated with victimization, negative symptomology, and the likelihood of students to seek mental health services. Prospero and Vohra-Gupta (2008) found that physical and psychological but not sexual dating violence victimization were associated with mental health service utilization in a college sample, suggesting that help-seeking behaviors vary by type of victimization. In addition, shame surrounding victimization and stigma regarding mental illness are serious barriers for help-seeking among college students (Guerette & Caron, 2007; Nasta et al., 2005; Walsh, Banyard, Moynihan, Ward, & Cohn, 2010).
Among the victims in Nasta and colleagues’ (2005) sample of students at a private, northeastern university, the reasons most cited for not using services were fear, embarrassment, guilt, and the perception of a lack of confidentiality. Student victims of IPV in another college sample cited embarrassment, thinking services would not help, and that others would perceive them as “crazy” as their reasons for not seeking mental health services (Prospero & Vohra-Gupta, 2008). Another major impediment to service utilization among victimized college students is an overall lack of knowledge of available campus services (Hayes-Smith & Levett, 2010; Walsh et al., 2010). Students appear to be more able to locate general information than specific services, such as crisis centers and services for victims of sexual assault (Banyard et al., 2007; Hayes-Smith & Levett, 2010; Walsh et al., 2010).
In light of the low levels of help-seeking among college students who experience IPV, and the numerous barriers to seeking treatment, the present study examines factors that affect college students’ utilization of counseling services. Specifically, since the severity of negative mental health symptoms are associated with seeking counseling and other services, in addition to the severity of victimizations (Krebs, Lindquist, Warner, Fisher, & Martin, 2007; Lindquist et al., 2013), we seek to determine what factors are associated with greater emotional distress and a higher likelihood to seek treatment among a sample of university students in the rural South. To that end, we examine the role of IPV victimization both prior to and since arriving at college, students’ levels of emotional distress, self-control, and demographics in seeking counseling.
The Current Study
Sample
The data for the current study were drawn from a larger study on relationship violence among university students conducted during 2014 at a large university located in the rural, Southern United States. Participants were asked to complete a 13-page pen and paper survey assessing experiences with IPV in adolescence and since arriving at the university as well as participants’ help-seeking behavior. Each class was randomly selected for participation from all of the courses taught at the university in the spring of 2014, excluding graduate and online courses. To ensure that the sample was representative of the university’s undergraduate student population, the list of classes was stratified based on the course enrollment size. All professors of selected courses were contacted to request permission to survey their class, and if a professor refused participation, another course was randomly selected from the sampling frame.
Once permission was obtained from a professor, a graduate student or one of the principal investigators administered the survey during the course’s regular class time. All students in the course were provided with an informed consent form and information on campus resources in the event that the sensitive nature of the survey led to emotional distress. Overall, 786 undergraduates in 28 classrooms completed the survey for a response rate of 60%. 1 The sample was generally a representative of the demographics of the university with Spring 2014 enrollment data, indicating roughly 52% of undergraduate students were female and 62% were White/non-Hispanic.
Measures
The focal dependent variable in this study is a dichotomous measure of whether or not the respondent has sought counseling. Respondents were asked, “Have you ever sought counseling or other mental health treatment for physical or emotional violence from an abusive relationship?” and the variable was coded as 0 = no and 1 = yes.
The focal independent variable in this study is a summative scale of 6 items corresponding to experiencing threatening IPV since attending college. Respondents were asked “please indicate whether you agree strongly, agree somewhat, disagree somewhat, disagree strongly, or are uncertain about the following statements” to the following six questions: (1) My significant other has tried to intimidate me, (2) My significant other has yelled or screamed at me, (3) My significant other has acted aggressively toward me, (4) My significant other is overly possessive of me, (5) My significant other has verbally threatened to harm me, and (6) My significant other has threatened to harm me with a weapon. The scale exhibited very good reliability (α = .85) and loaded on one dimension (eigenvalue = 3.08).
The mediator variable of interest is an index measure of experienced negative emotions and behavioral reactions as a result of IPV victimization. This index of distress was constructed from 7 items on the survey which asked respondents, “Have you ever experienced any of the following problems as a result of violent or emotional victimization? Check all that apply.” The respondents could check the following items: (1) insomnia, (2) depression, (3) anxiety, (4) fear of leaving the house, (5) withdraw from personal relationships, (6) avoidance of social situations, and (7) other emotional reaction. The index exhibited good reliability (α = .80) and loaded on one factor (eigenvalue = 2.57).
Several variables are used as statistical controls in the following analyses. Demographic variables include age (continuous variable from 18 to 50), gender (0 = male; 1 = female), race (0 = White; 1 = non-White), and setting of where the respondent grew up (0 = nonrural; 1 = rural).
A measure of self-control is used to account for its correlation with victimization (Schreck, 1999). Recent studies have found that individuals with low self-control are much more likely than those with average or high levels of self-control to be victimized, due to their risky lifestyles and impulsive behavior (Pratt, Turanovic, Fox, & Wright, 2014; Schreck, Stewart, & Fisher, 2006). We capture self-control using the full 24-item scale developed by Grasmick, Tittle, Bursik, and Arneklev (1993) including measures such as, “I often act on the spur of the moment without stopping to think,” “I dislike really hard tasks that stretch my abilities to the limit,” and “I lose my temper pretty easily” with responses ranging from 1 = disagree strongly to 5 = agree strongly. The measure produced very good reliability (.86) but was shown to be multidimensional. Since self-control is used as a control measure in the current study, and for parsimony and ease of interpretation, the measure was kept as a single variable. Previous victimization is controlled for using 1 item from the survey, asking respondents whether or not a significant other had threatened them in middle or high school (0 = no; 1 = yes). Descriptive statistics for the sample are given in Table 1.
Sample Descriptive Statistics.

Note. n = 786. IPV = intimate partner violence.
Analytic Strategy
We begin our analyses by presenting sample means and percentages for our study variables. To examine associations between victimization and study variables, zero-order correlations are calculated among our variables. Our main analysis is a moderation analysis using sequential equations modeling. The first sequence is completed using negative binomial regression and the second using logistic regression. A multiplicative interaction term is entered into the final model to investigate the moderation effects of victimization on emotional distress in predicting help-seeking behavior. To retain our sample size and avoid biased estimations which sometimes occur after listwise deletion (Acock, 2005), we use imputation through chained equations to construct 10 data sets with full information (Royston, 2009). In the multivariate analyses, we center our scale variables to avoid collinearity in our interaction term and to aid in the interpretation of the results, as the coefficient represents the change in the dependent variable for every standard deviation increase in the independent variable—controlling for the effects of all other variables in the model.
Results
In order to investigate the associates of victimization, zero-order correlations are calculated for each study variable and IPV. Table 2 presents the bivariate correlations and indicates that each study variable is positively related to victimization. Older, female, and non-White students are more likely to experience IPV than their counterparts. Students with low self-control, those who have experienced prior victimization, and those with high levels of emotional distress are all more likely than others to have experienced IPV. Additionally, those who seek counseling are more likely to have experienced IPV. The setting (urban or nonurban) in which the student grew up had no association with IPV.
Bivariate Correlations Between IPV and Study Variables.
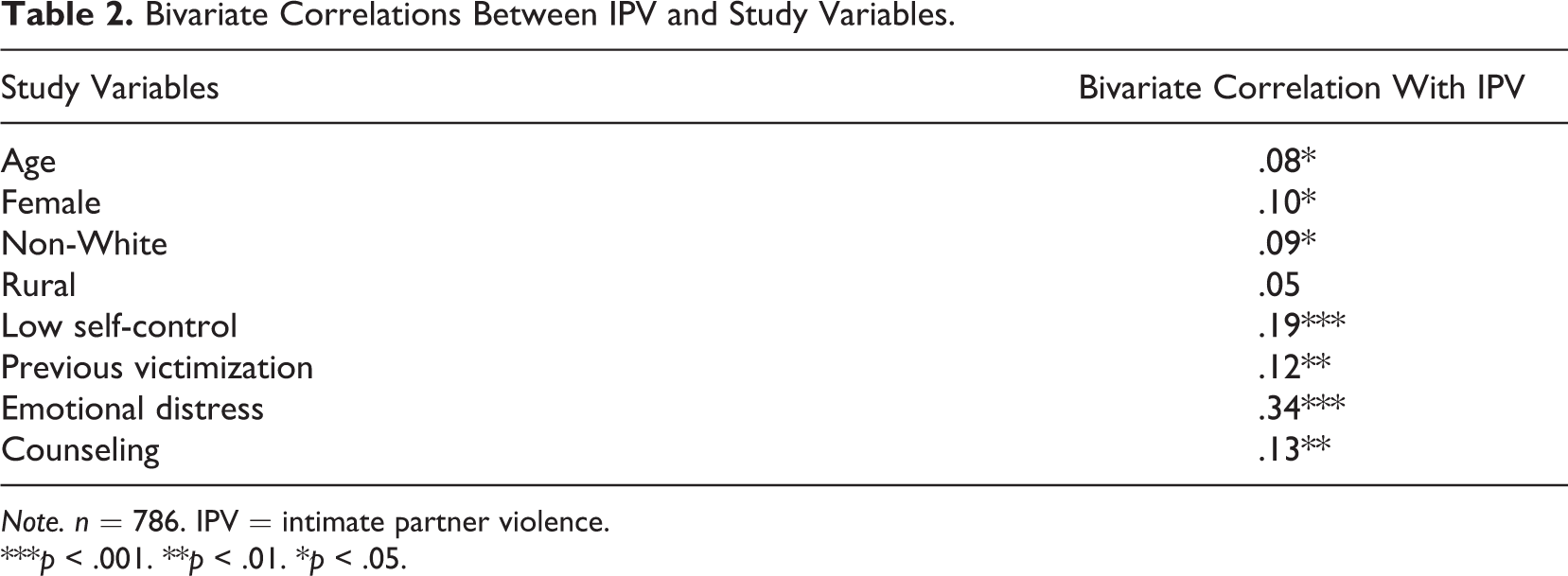
Note. n = 786. IPV = intimate partner violence.
***p < .001. **p < .01. *p < .05.
Table 3 shows the results of two equations, which were the steps in our sequential equation model (which were estimated in the same model using generalized sequential equations). Step 1 indicates that IPV increases emotional distress by 53.73% ([(e 46−1)] × 100). Being female, having low self-control, and experiencing prior victimization all increase the level of emotional distress. Age and the setting in which students grew up are unrelated to the level of emotional distress.
Path Model of Emotional Distress and Counseling on IPV and Covariates.
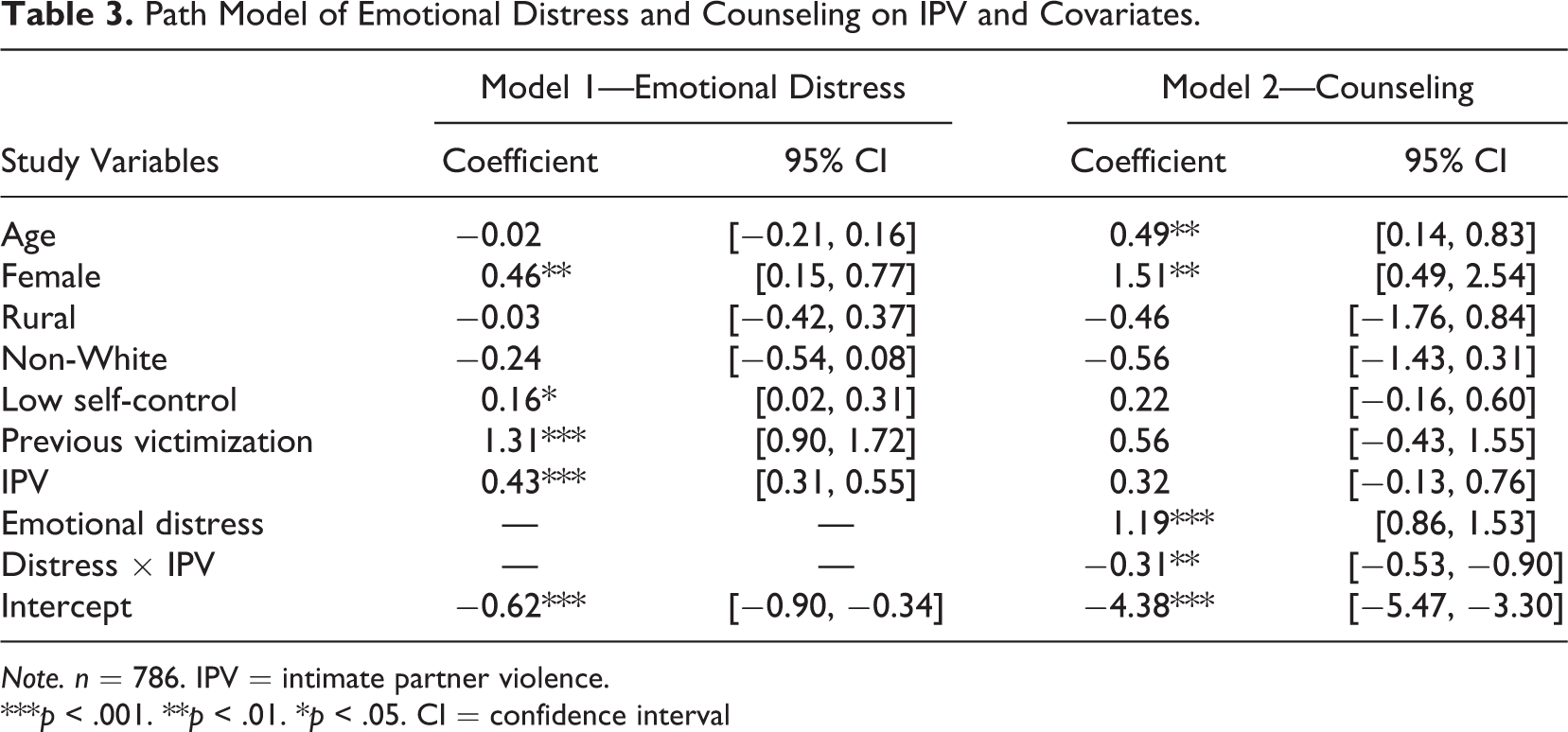
Note. n = 786. IPV = intimate partner violence.
***p < .001. **p < .01. *p < .05. CI = confidence interval
The second step presents the results from the second equation, which indicates that emotional distress increases the odds of seeking counseling by 228.71% ([(e 1.19−1)] × 100) or over 2 times those with lower levels of distress. Importantly, victimization is not statistically significant in this model. This is likely due to the way in which it works in combination with emotional distress. In fact, the effect of victimization in predicting help-seeking behavior is decreased in the presence of distress (coefficient = −.31). This does not mean that victimization decreases seeking counseling, only that the effect is weakened in the presence of emotional distress, suggesting that the emotional reactions to IPV are the driving force behind seeking counseling among college students in our sample.
To graphically illustrate the model, Figure 1 presents the results of our main study variables and their associations with counseling. It should be noted that the model depicted in the figure controls for the effects of all variables in the previous model. Victimization does not have a direct effect on seeking counseling but moderates the effect of emotional distress. Distress, in turn, increases seeking counseling directly and in combination with IPV.
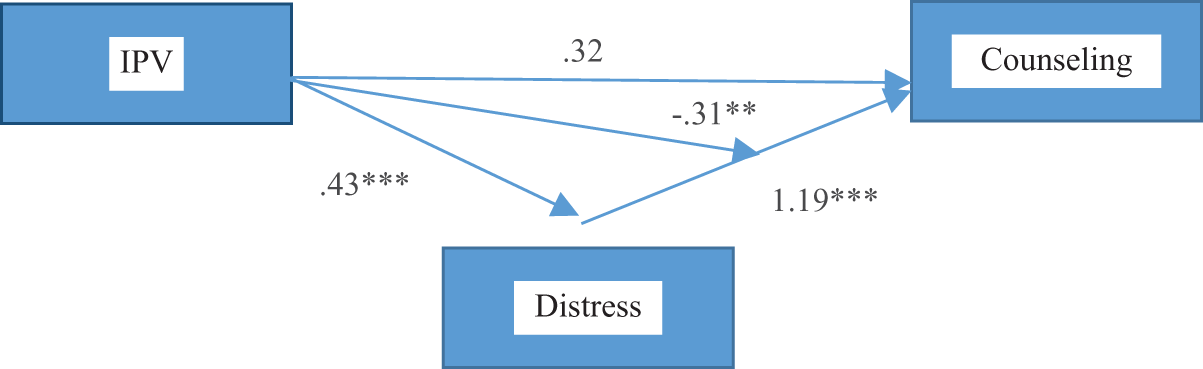
Trimmed model pathway from intimate partner violence to counseling.
Discussion
Consistent with past research, our findings indicate that college students who have experienced high levels of IPV are more likely to experience emotional distress than students who have not been victimized by a partner. Additionally, the results suggest that emotional distress increases help-seeking behavior among college students. The present study points to a clear need for colleges and universities to educate students about available mental health services on campus. This is particularly important for students who have experienced IPV, since we find that IPV victimization both prior to and since attending college are associated with greater emotional distress. The interaction between victimization and emotional distress was key to help-seeking among the students in this rural university sample. Therefore, it is imperative that universities provide as much information as possible regarding not just counseling, but other available services specific to victims of IPV. Studies of sexual and IPV victimization suggest that victims often disclose their victimization to and seek help from informal sources, including friends (Amar & Gennaro, 2005; Douglas & Hines, 2011; Sabina et al., 2011; Sabina & Ho, 2014; Sylaska & Edwards, 2014). Thus, university efforts to increase general awareness among students about available resources as well as encouraging students to direct their peers to these resources in the event of a victimization disclosure may lead to increased levels of service utilization among victims.
Regarding students’ demographics associated with seeking counseling, older and female students are more likely to seek treatment for emotional distress. As younger students and males are less likely to seek counseling, outreach to these students is imperative for a healthy campus. A number of studies suggest that young males, particularly college students, are at risk of being victimized by their partners (see Desmarais, Reeves, Nicholls, Telford, & Fiebert, 2012; Straus, 2004). Although we did not find that males were at an increased risk of being victimized or experiencing emotional distress, it may be that males experience different forms of IPV and distress that were not adequately captured in the current research. Alternatively, research shows that males underestimate their actual exposure to IPV because they do not define certain behaviors as IPV or are reluctant to consider themselves victims (see Fondacaro, Holt, & Powell, 1999). 2 Efforts must be increased to reach and support these students, as male students might be more reluctant than females to seek opportunities to deal with emotional distress in general (Addis & Mahalik, 2003) and reactions to their victimization experiences in particular.
Further, recent research by Scherer and colleagues (2013, 2014) suggests that other subsets of the university student population, namely individuals with disabilities, may be more likely to experience negative mental health outcomes as a result of IPV victimization compared to students without disabilities. Thus, it is important that future research considers additional characteristics of students that may affect their risk of IPV as well as their emotional health and help-seeking behavior following an IPV incident.
A set of limitations of the current study points to avenues for future research. First, it is not possible to definitively determine the temporal order of distress and IPV. Longitudinal data are needed to confirm the relationships found in the present study. Second, our sample comes from one university in the South and cannot be generalized to all college students. Future studies should replicate this analysis using both nationally representative samples and other colleges/universities. Although our measure of emotional distress encompassed many emotional and behavioral responses to victimization, we were unable to assess severity of the reactions (only that they had them or not). Research should continue to examine both the prevalence and the magnitude of emotions as they both may have independent and reinforcing impacts on seeking counseling (see Agnew, 2001). Finally, we were only able to assess the impact of threatening IPV victimization experiences on student distress and help-seeking. Our measure does not fully tap into other forms of IPV, including more severe acts of physical and sexual partner violence, which are likely to lead to strong emotional responses. Future research should consider the impact of a broad range of violent behavior by partners on victims’ emotional well-being and help-seeking.
Another important area for future research relates to the implications of Title IX mandatory reporting requirements for help-seeking behavior among university students. Despite confidentiality protections afforded to counseling professionals on college campuses, university faculty and other staff including, but not limited to, academic advisors and graduate teaching assistants are required to report students’ disclosures of relationship or sexual violence experiences to the institution. 3 Although it is speculative at this point, this change in the university climate is likely to affect student disclosures to individuals who may be able to direct them to appropriate services and may reduce help-seeking behavior among victims. More specifically, a student may be hesitant to discuss his or her personal victimization experiences with a professor or other members of the campus community, if the individual is required by law to disclose the details of the conversation to campus officials. At the same time, a student might be more likely to seek and receive counseling or other support services, as universities are required by Title IX to make known where victims can find local and on-campus confidential support services. In addition, if a Title IX investigation is initiated, and if the investigation reveals wrongdoing, universities are required to provide remedies, including counseling, to help victimized students continue with their education. Future research should examine the effects of Title IX mandatory reporting requirements to determine their effects on help-seeking among victims of IPV, particularly considering the findings of the present study that victimization coupled with emotional distress affects college students’ help-seeking behaviors.
Implications for Policy and Programming
Our results show that only 7% of the sample sought counseling. Although access to university health and counseling centers is near ubiquitous among college students nationwide (National Institute of Mental Health, 2012), several barriers may prevent victims of IPV in college from seeking out these services. First, some students may not define their situation as abuse or IPV. Campus-wide initiatives to raise awareness about the signs of IPV may provide much-needed information to college students that can help them define and identify abusive situations in their own and others’ relationships. In addition to classes that educate students about victimization (see Mummert et al., 2014), campus-wide programs can not only inform students about the signs of relationship violence but can provide information on local resources, including counseling services, that can help students deal with both emotional distress and IPV. The Red Flag Campaign, 4 for example, was created by college students and personnel to raise students’ awareness of the signs of dating violence (i.e., relationship red flags). Similarly, many universities nationwide implement programming designed to reach a wide campus audience. For example, at the University of Georgia, the Relationship and Sexual Violence Prevention (RSVP) office implements programs and workshops that educate students broadly on sexual assault and dating violence as well as providing counseling, support, and advocacy services to victims at no cost. 5 For males, who may be reluctant to classify their victimization as IPV or view themselves as a “victim,” we advocate for extending Jewkes’ (2002) prevention strategy of changing community (and even societal) norms to focus on males’ identification of IPV and reporting. Discussing gender and violence in school and community sexual and reproductive health programs can mark the beginning of acknowledging IPV and promoting help-seeking. Advocating and establishing nonviolent conflict resolution programs, such as restorative justice, can provide a safe space for discussing and addressing the impact of IPV.
Future research should evaluate the effectiveness of these awareness-raising programs on students’ ability to identify IPV in their own and others’ relationships as well as the effects of such programming on students’ likelihood to seek help, including counseling, in cases of victimization and emotional distress. While raising awareness through campus-wide programming may better enable students to identify signs of IPV, it remains unknown if these programs effectively connect students to needed mental health services. This is particularly important as students may lack knowledge of available campus services (Hayes-Smith & Levett, 2010; Walsh et al., 2010).
A second impediment to help-seeking among student victims of IPV is a fear that their abuser could find out that they have sought help and could retaliate in some way. College and university personnel can work to educate students regarding their rights in cases of IPV. First, according to the Clery Act, students should be informed that their “institution [can] change a victim’s academic and living situations after an alleged sex offense” (Clery Act, 669.46b11v). This option may provide survivors of IPV involving sexual assault the safety that they need to report an incident of violence and to seek counseling for related emotional distress. Further, Title IX requires universities to have processes and procedures in place to ensure students who experience IPV or sexual violence are afforded a safe school environment free from retaliatory behavior by the abuser or any third parties.
Finally, students may fear the stigma associated with seeking help for mental health problems as well as the stigma of IPV victimization. Research highlights considerable stigma surrounding mental illness (see Pescosolido, 2013) and suggests that stigma is a significant barrier to help-seeking among minorities (Gary, 2005; Snowden, 2001; U.S. Department of Health and Human Services, 2001). A number of programs have emerged to reduce negative public perceptions of mental illness as well as alter attitudes toward persons with mental illness. A recent review of 75 studies suggests education programs (e.g., educational videos, flyers, websites) targeting stereotypes, as well as actual contact with an individual with a mental disorder, are promising strategies for reducing stigma (Corrigan, Morris, Michaels, Rafacz, & Rusch, 2012). The results further indicated the effects of educational programming and contact varied for different age-groups with contact having a greater impact on attitudinal change among adults and education efforts having a greater impact on adolescents. Since the majority of college students are emerging adults, a blend of programming including educational strategies as well as face-to-face encounters with persons who have mental illness may help reduce the stigma attached to mental illness among this specific population. Further, these programs should help raise awareness of the mental health effects of victimization and be culturally sensitive in order to address negative perceptions among ethnic and racial minorities. Programs aimed at changing attitudes toward mental illness may ultimately increase help-seeking behavior among college students experiencing emotional distress, including those who have been victimized by a partner.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.