
Abstract
This study examined empirical evidence for clinical utility of the Wechsler Intelligence Scale for Children, fourth edition (WISC-IV) cancellation subtest by comparing data from 597 clinical and 597 matched control children. The results of dependent t and sequential logistic regression analyses demonstrated that (a) children with intellectual disabilities, motor impairments, head injuries, Autistic/Aszperger’s disorder, ADHD and learning disabilities, and mathematics disorder showed significant deficits on the cancellation subtest; (b) children with intellectual disabilities and Asperger’s disorder benefited when stimuli were randomly aligned, but children with ADHD benefited from structured conditions; (c) beyond the full-scaled IQ (FSIQ) and General Ability Index (GAI)–Cognitive Proficiency Index (CPI) discrepancy scores, the cancellation subtest added unique diagnostic power to identify children with reading disorders, mild intellectual disabilities, closed head injuries, and motor impairments. These results suggest the utility of the cancellation subtest in clinical assessment.
Cancellation is a new supplemental processing speed subtest in the Wechsler Intelligence Scale for Children-Fourth Edition (WISC-IV). The test asks the child to scan both a random and a structured arrangement of pictures, and marks target pictures within a specified time limit (Wechsler, 2003a). In neuropsychological settings, cancellation tasks are traditionally used as measures of visual inattention. These tasks primarily assess the capacity for sustained attention, accuracy and speed of visual scanning and discrimination, and activation and inhibition of responses (Lezak, Howieson, Bigler, & Tranel, 2012; Miller & Hale, 2008). Performance deficits in these tasks were reported to be associated with spatial inattention problems (Halligan, Marshall, & Wade, 1989), particularly for stroke patients with unilateral spatial inattention (Vanier et al., 1990; Ferber & Karnath, 2001). No other study has examined the incremental utility of this test when it was considered for an intellectual assessment battery, such as WISC-IV.
In WISC-IV hierarchical confirmatory factor analyses, cancellation is the subtest with the lowest g loading and the highest uniqueness (Chen, Keith, Weiss, Zhu, & Li, 2010; Keith, Fine, Taub, Reynolds, & Kranzler, 2006; Weiss, Keith, Zhu, & Chen, in press). Thus, larger percentages of subtest variance could be explained by factors other than those specified in the WISC-IV structure: full-scaled IQ (FSIQ), verbal comprehension (VCI), perceptual reasoning (PRI), working memory (WMI), and processing speed (PSI). This subtest was also evaluated by Ortiz who identified it as one of the few WISC-IV subtests with low cultural loading and linguistic demands. Therefore, this test may yield results more equitable for diverse individuals (Flanagan & Kaufman, 2004).
Wechsler tests are frequently used as part of diagnostic assessments (Prifitera, Saklofske, & Weiss, 2008). The consensus on the primary utilities of these batteries is that (a) they offer a reliable summary of general cognitive ability, and (b) they provide methods for evaluating cognitive strengths and weaknesses (Flanagan & Kaufman, 2004; Kaufman & Linchtenberger, 2002; Matarazzo & Herman, 1985; Sattler & Dumont, 2004), also known as profiles/discrepancies. Of these tests, the FSIQ has the highest reliability and achievement-related validity (Wechsler, 2003b). Thus, FSIQ is considered one of the best summaries for overall cognitive ability. Furthermore, Weiss et al. (2006) suggested that index scores should be considered the primary level of clinical interpretation of the WISC-IV. Wechsler index score profiles have tremendous clinical utility (Allen, Thaler, Donohue, & Mayfield, 2010; Calhoun & Mayes, 2005; Weiss, Prifitera, & Saklofske, 2005). In particular, the discrepancy between two WISC-IV indices, general ability (GAI) and cognitive proficiency (CPI), shows meaningful intrapersonal cognitive characteristics and predictive power (Raiford, Weiss, Rolfhus, & Coalson, 2005; Weiss, Beal, Saklofske, Alloway, & Prifitera, 2008; Weiss & Gabel, 2008). The GAI is a composite of the more highly g loaded subtests within WISC-IV. It provides an estimate of general intellectual ability, with reduced emphasis on working memory and processing speed relative to the FSIQ. The CPI is the counterpart to the GAI. It summarizes the performance of working memory and processing speed; thus, providing a more comprehensive summary of cognitive processing proficiency (Saklofske, Zhu, Coalson, Railford, & Weiss, 2010; Saklofske et al., 2012). Efficient cognitive processing frees cognitive resources for more complex or higher-level tasks. The GAI-CPI discrepancy provides a comparison of a measure of current knowledge and reasoning ability to cognitive proficiency, which could be considered as the one Wechsler cognitive profile/discrepancy with the broadest construct perspective and the smallest measurement error (Zhu, Railford, & Coalson, 2009).
To examine the incremental utility of the cancellation subtest, both FSIQ and GAI-CPI discrepancy should be considered. FSIQ is the most reliable summary for overall cognitive ability, and GAI-CPI discrepancy is the most reliable measure for cognitive variability. These two measures cover the core information the Wechsler battery could provide. If the cancellation subtest provides diagnostic power in addition to that provided by FSIQ and GAI-CPI, its practical utility could be secured.
Utility of the cancellation subtest for types of disabilities has never been examined or reported. Cancellation is a measure of processing speed. The importance of considering the processing speed in a complete intelligence structure is well recognized (Carroll, 1993, 2005; Woodcock, McGrew, & Mather, 2001). Processing speed is found to have a significant effect on higher-level cognitive abilities, such as working memory and fluid reasoning (Fry & Hale, 1996, 2000; Kail, 2007; Nettelbeck & Burns, 2010); thus, providing greater weight to processing speed in the intelligence test battery is justified by neuropsychological findings. Sattler and Dumont (2004) suggested that more research is required to determine whether this new subtest (with random vs. structured tasks) is clinically useful. The purpose of this study is to compare and investigate the cancellation scaled scores of clinical and matched control children. The incremental contribution of the cancellation subtest for diagnosis at control versus clinical groups was also tested. More specifically, the research question was whether inclusion of the cancellation subtest improved the ability of FSIQ and GAI-CPI discrepancy to predict clinical status.
Method
Participants
The WISC-IV scores of 597 clinical and 597 matched control children were analyzed. The heterogeneous clinical sample included 15 groups: children with ADHD (n = 89); children with ADHD and learning disorders (n = 45); children with Autistic disorder (n = 19); children with Asperger’s disorder (n = 27); children with expressive language disorder (n = 27); children with mixed receptive-expressive language disorder (n = 40); children with reading disorder (n = 56); children with reading and written expression disorder (n = 35); children with mathematics disorder (n = 33); children with reading, written expression, and mathematics disorder (n = 42); children with intellectual disabilities of mild severity (n = 63); children with intellectual disabilities of moderate severity (n = 57); children with closed head injuries (n = 27); children with open head injuries (n = 16); and children with motor impairments (n = 21). These children were drawn from a variety of educational and clinical settings, and were accepted for participation in clinical samples based on specified inclusion criteria (see Wechsler, 2003b, pp. 145-149, Appendix D). For meaningful comparisons, 597 matched control children were selected from the WISC-IV standardization sample. These children were matched with the clinical children by demographic variables of age, gender, ethnicity, parental education, and geographic region. Demographics of all samples are presented in Table 1. The mean age and FSIQ of each sample is presented, and followed by percentages of sample representations by gender, race/ethnicity, parental education, and geographic region.
Demographic Data for the Studied Samples.

Note. Except for sample size (N), FSIQ, and age, data are reported as percentages.
FSIQ = Full-scaled IQ; ID Mild = Intellectual disabilities–mild severity; ID Moderate = Intellectual disabilities–moderate severity; RD = Reading disorder; RWD = Reading and written expression disorders; MD = Mathematics disorder; RWMD = Reading, written expression, and mathematics disorders; ADHD/LD = Attention-deficit/hyperactivity disorder and learning disorder; ADHD = Attention-deficit/hyperactivity disorder; ELD = Expressive language disorder; RELD = Mixed receptive-expressive language disorder; OHI = Open head injury; CHI = Closed head injury; AUT = Autistic disorder; ASP = Asperger’s disorder; MI = Motor impairment.
Instrumentation
The WISC-IV offers practitioners several cognitive measures, including an FSIQ, six composite scores (GAI, CPI, VCI, PRI, WMI, PSI), and scores from 15 subtests. This study analyzed FSIQ, GAI-CPI discrepancy, and cancellation scaled scores. Cancellation contains two items, the pictures of objects in Item 1 are arranged in a random pattern, and the objects in Item 2 are arranged in a structured pattern. For each item, the child is asked to scan the arrangements of pictures, and mark the target pictures within a 45-s limit. The reliability for FSIQ, GAI, CPI, GAI-CPI discrepancy, cancellation total (CA), cancellation random (CAR), and cancellation structured (CAS) is 0.97, 0.96, 0.93, 0.84, 0.79, 0.70, and 0.75, respectively.
Statistical Analyses
The statistical analyses examining the clinical utility of the WISC-IV cancellation subtest were conducted using SAS. Repeated measure t-tests determined the differences between each clinical group and its matched control counterpart. Sequential logistic regression (Menard, 2000; Spicer, 2005) determined the incremental diagnostic utility of the cancellation subtest after adjusting for the FSIQ and GAI-CPI discrepancy. For each of the 15 clinical groups, fit index, and the parameters of the two logistic regression models were compared with FSIQ and GAI-CPI discrepancy as independent variables, and the cancellation was used as the third predictor. The logistic regression coefficient and odds ratio for the cancellation subtest, classification hit rate, and model R2 were reported.
Results
Comparison of Cancellation Scores
Table 2 presents score differences between clinical and matched control groups. The groups with the most salient deficits were intellectual disabilities, motor impairment, head injuries, Autistic/Asperger’s disorders, ADHD with LD cormorbidity, and mathematics disorder. Table 2 also presents the percentages for each clinical sample, as well as for the corresponding control group, that show impaired performance (lower than two standard deviations below the mean) on the cancellation subtest. Numerous clinical groups showed higher impairment rates. Particularly, the children diagnosed with head injuries, motor impairments, reading disabilities, Autistic spectrum disorder, and intellectual disabilities showed higher impairment rates, which were at least twice more than the rates shown in the corresponding control groups.
Group Differences on Cancellation Subtest Performance.

Note. CA= Cancellation total; CAR = Cancellation random; CAS = Cancellation structured; ADHD = Attention-Deficit/hyperactivity disorder; ADHD/LD = Attention-deficit/hyperactivity disorder and learning disorder; LD = Learning disorder; RWM = Reading, written expression, and mathematics; ID = Intellectual disabilities.
p < .05; **p < .01
Table 3 presents discrepancies in cancellation-random and cancellation-structured scores between clinical and matched control groups. Children with intellectual disabilities, Asperger’s disorder, and ADHD showed the largest discrepancies between random and structured tasks. Children with intellectual disabilities and Asperger’s disorder showed a slight advantage under random conditions compared to structured conditions. However, children with ADHD benefited significantly from the alignment of stimuli under structured conditions.
Group Differences in Cancellation Random Minus Structured Discrepancy Score.
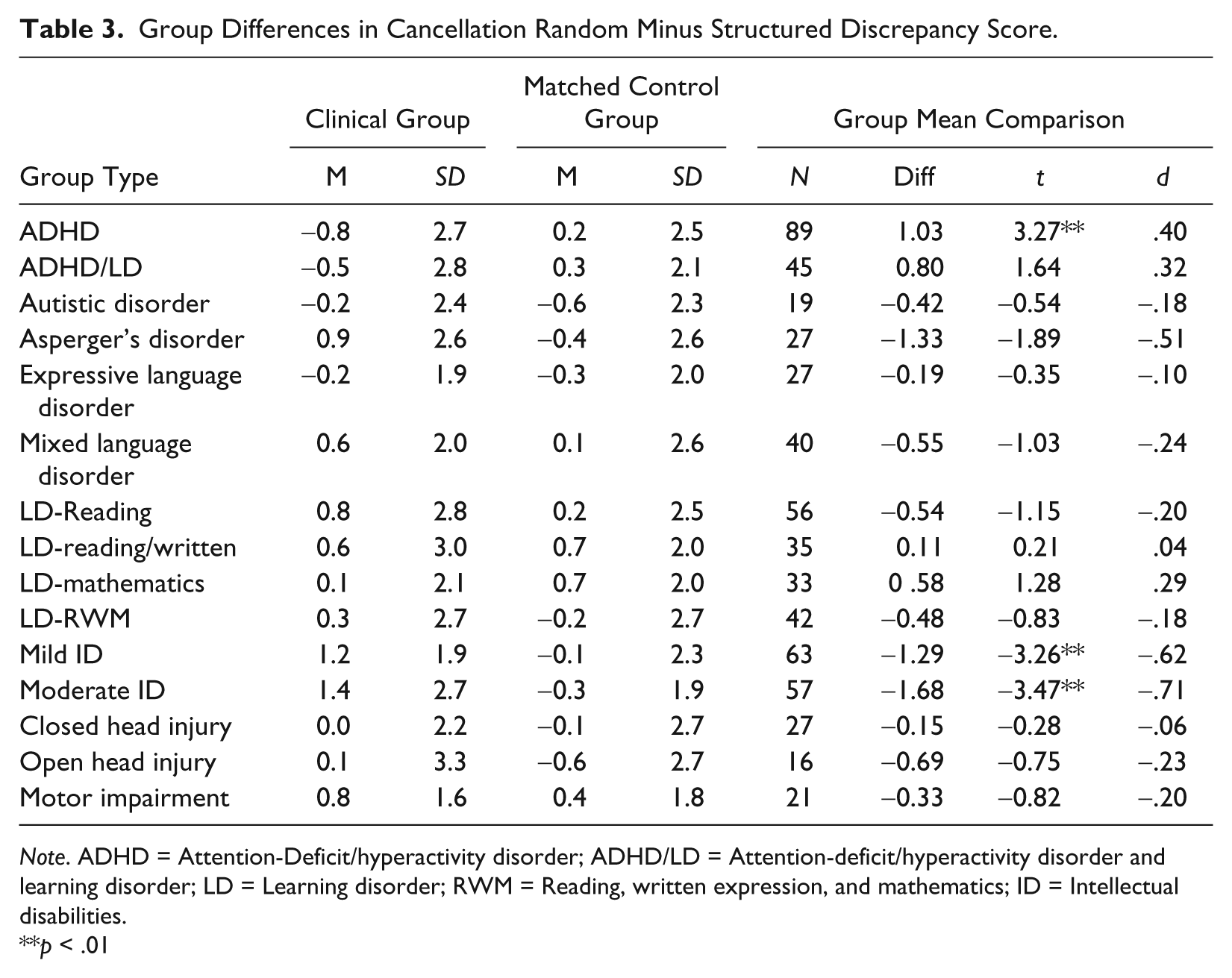
Note. ADHD = Attention-Deficit/hyperactivity disorder; ADHD/LD = Attention-deficit/hyperactivity disorder and learning disorder; LD = Learning disorder; RWM = Reading, written expression, and mathematics; ID = Intellectual disabilities.
p < .01
Evaluation of the Incremental Diagnostic Utility of Cancellation Subtest
Cancellation was found to improve the predictive power of FSIQ and GAI-CPI discrepancy scores on four clinical types: reading disorders; mild intellectual disabilities; closed head injuries; and motor impairments. The results of the sequential logistic regression analyses of these four clinical types are presented in Table 4. Nonsignificant results are available by request.
Sequential Logistic Regression Analysis: Predictors of Clinical Status.

For the reading disorder group, inclusion of the cancellation subtest statistically improved the model (p = .0086). As the logistic coefficient for cancellation is 0.22, when FSIQ and GAI-CPI discrepancies are statistically controlled, children with one increase in cancellation scaled score have a 0.22 increase in their log odds of being in the reading disabled group. The odds of 1.24 also meant that after FSIQ and GAI-CPI discrepancy scores were adjusted, each increase in cancellation scaled score increased the odds of being in the reading disabled group by 24%. Classification analysis showed that 74% of all cases were correctly classified by the probabilities derived from the model using all three independent variables (compared to an overall hit rate of 72% for the model without the cancellation subtest).
All three predictors significantly improved prediction of mild intellectual disabilities (p = .0134). The logistic coefficient for the cancellation subtest was −0.38 and the odds ratio was 0.68, suggesting that for every one unit increase the cancellation subtest scaled score, the odds of being mildly intellectually disabled decreased by 32%. Of the cases, 95% were correctly classified by the model using all three predictors, of which 3% was contributed by the cancellation subtest.
For the closed head injury group, Δχ2 also showed significant differences (p = .0166) between the two- and three-predictor models. The logistic coefficient for the cancellation subtest was −0.27, and the odds ratio was 0.76. This suggested that for every one point increase in the cancellation subtest scaled score, the odds of being in the closed head injury group decreased by 24%. Inclusion of the cancellation subtest raised the classification hit rate from 73% to 75%.
Finally, the motor impairment group showed a significant (p = .0490) difference between the models. The logistic coefficient for the cancellation subtest was −0.27, with odds of 0.77. Thus, for every scaled score increase in the cancellation subtest, the odds of being in the motor impairment group decreased by 23%. Classification analysis showed that 67% of the cases were correctly classified by the probabilities derived from the model using all three independent variables (compared to an overall hit rate of 64% for the model without the cancellation subtest).
Discussion
The results supported the clinical utility of the cancellation subtest. Children with individual disabilities, motor impairments, head injuries, Autistic or Asperger’s disorder, ADHD/ LD, and mathematics disorder showed significant deficits in performance on the cancellation subtest. Children with intellectual disabilities and Asperger’s disorder performed better when stimuli were randomly aligned. Children with ADHD benefited significantly from structured conditions. The cancellation subtest contributed extra predictive power to that explained by the FSIQ and GAI-CPI discrepancy scores for identifying children with reading disorders, mild individual disabilities, closed head injuries, and motor impairments.
The findings that children with intellectual disabilities and head injuries performed poorly on the cancellation subtest was expected because processing speed plays a crucial role in the development of intelligence (Kail, 2000), and is sensitive to brain dysfunction (Allen et al., 2010; Calhoun & Mayes, 2005). Performance on cancellation revealed information on general cognitive development and brain function. Children with motor impairments, Autistic or Asperger’s disorder, and mathematics disorder appeared to have a common characteristic. Many of them have difficulties in managing nonverbal (pictorial) materials and perceptual–motor coordination (Boreas, Rintala, & McCubbin, 2009; Panaoura, 2006; Taylor, Espy, & Anderson, 2009; Wechsler, 2003b). Children with these clinical types may also show delayed developmental coordination (Henderson & Henderson, 2002). As cancellation requires children to scan arrangement of pictures and mark target pictures in a timely fashion, deficit performance on this task may reveal their difficulties in processing pictorial materials in a timely fashion and their poor perceptual–motor coordination.
Structured instruction is recognized as a useful strategy for teaching children with ADHD (Walcott & Landau, 2004; Young & Amarasinghe, 2010). Our results from the cancellation subtest coincided with this line of research (Flanagan & Kaufman, 2004). The reason intellectually disabled children and children with Asperger’s syndrome process simple pictorial figures faster under random conditions was less obvious. When a task requires more cognitive ability, structured guidance is assumed to help. When a task is relatively easy, structured guidance may hinder these children because they are known to have more rigid and less flexible thinking patterns (Mintz, 2008; Polirstok & Houghteling, 2006). In the cancellation subtest, structured alignments may imperceptibly lead these children to process each figure in sequence, resulting in lowered performance. Our results suggest that the effects of various stimuli presentation on these types of children should be more carefully differentiated. Structured alignments may not always work the best.
Profile analyses showed that FSIQ typically represented overall cognitive ability, and GAI-CPI discrepancy provided hints for breadth in ability. With the well-documented predictive power of these two composite-based indices (Glutting, Watkins, Konold, & McDermott, 2006; Lynn & Vanhanen, 2006; Pesta, McDaniel, & Bertsch, 2010; Watkins, Glutting, & Lei, 2007; Weiss & Gabel, 2008), and the quick and easy administration of the cancellation subtest, it was noteworthy that the cancellation subtest contributed statistically significant power to identification. After controlling for the FSIQ and GAI-CPI discrepancy, reduced cancellation performance was associated with greater probability of mild intellectual disabilities, closed head injuries, and motor impairments. In comparison, children with reading disabilities had a higher probability of obtaining higher cancellation subtest scores once the FSIQ and GAI-CPI discrepancy was controlled. The processing speed for stimuli of different modalities (no meaningful symbols vs. meaningful pictorial figures) appeared to have a difference. A follow-up examination revealed that children with reading disabilities showed significant deficits in performance on two other processing speed tests, coding (t = 2.47, p < .05), and symbol search (t = 2.01, p < .05). Both of these subtests required children to process nonmeaningful symbols quickly.
In general, the current study examined the practical usefulness of the WISC-IV cancellation subtest in a broad perspective. However, the limitations deserve attention. First, our study examined 15 major clinical types but was not exclusive. There are other clinical groups that need to be studied. Second, these clinical samples were not randomly selected but were selected based on availability by educational and clinical professionals across states. Certain clinical groups had small sample sizes, and cross-validation was not able to be conducted. Future research is recommended to employ large, representative, randomly selected, and independent samples, with independent validation when possible. Third, the numerous comparisons and the relative marginal levels of significance for certain findings could be a weakness. Since this is the first study in this area, we interpreted the conventional significance levels and effect sizes. More conservative data interpretation is suggested. Finally, we judged the subtest utility primarily by its predictive power. Other clinically meaningful qualitative information from this subtest were not examined, such as the location of first cancellation, systematic slowing with time, and function of target location. This information is useful for assessing people with right hemisphere injuries (Samuelsson, Hjelmquist, Naver, & Blomstrand, 1996) and unilateral spatial neglect (Manly et al., 2009). Therefore, the findings of this study should not be considered as the sole use of the cancellation subtest.
Overall, our findings supported the utility of the WISC-IV cancellation subtest. Children with several clinical types showed reduced performance on this subtest. In addition, this subtest was found to be able to improve the predictive power of FSIQ and GAI-CPI discrepancy in four clinical types. The current results permit future comparisons and interpretations.
Footnotes
Authors’ Note
For readers interested in the details of the inclusion criteria for participants, please contact the corresponding author for a summary.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.