
Abstract
The diagnosis of attention deficit hyperactivity disorder (ADHD) distinguishes two dimensions of symptoms, inattention and hyperactivity-impulsivity for ages 3 to adulthood. Currently, no separate classification for preschool-age children exists, whereas preliminary research suggests that the two-factor structure of ADHD may not match the presentation of symptoms in a preschool sample. The present study explored this incongruity by examining the factor structure of the 18 Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev; DSM-IV-TR) ADHD symptoms on the ADHD-Rating Scale-IV–Preschool Version within a normative preschool sample (n = 976). Confirmatory factor analyses (CFAs) were performed on results from teacher and parent ratings. The findings indicate a three-factor model, inattention, hyperactivity, and impulsivity, for the presentation of ADHD in preschoolers based on both parent and teacher report data.
Attention deficit hyperactivity disorder (ADHD) is one of the most commonly diagnosed childhood disorders (Barkley, 2005). In fact, ADHD is diagnosed in approximately 9% of children ages 3 to 17 years (Centers for Disease Control and Prevention [CDC], 2010). Egger, Kondo, and Angold (2006) report that the prevalence of ADHD in preschool children ranges from 2% to 7.9%. Despite this relatively high percentage of preschool children diagnosed with ADHD, the number is conjectured to be even higher, given that the diagnostic criteria were designed for older children and may not capture the distinct characteristics of preschool children. For example, Sonuga-Barke, Daley, Thompson, and Swanson (2003) state that preschool children with ADHD not only exhibit impulsivity, inattention, and hyperactivity but also experience motor coordination problems, developmental deficits, and difficulty in social play and considerable stress in families. Given these findings, and considering the rapid developmental change in the preschool period, plus the number of behaviors associated with ADHD that are developmentally appropriate for children of preschool age (e.g., carelessness, disorganization, and aggression), the diagnosis of ADHD in a young child is extremely difficult (DuPaul & Kern, 2011).
As a result, before a diagnosis of ADHD in preschool children may be rendered, the problem behaviors must be assessed both in terms of typical developmental expectations and the severity and pervasiveness of the behaviors. Currently, the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) definition of ADHD contains 18 symptoms that create three subtypes of the disorder: inattentive type, hyperactive/impulsive type, and combined type. The three subtypes are actually two dimensions of symptoms, inattention and hyperactivity-impulsivity, each containing nine symptoms. The same DSM-IV-TR (APA, 2000) criteria are used to diagnose children from age 3 to adults. Numerous studies have supported the validity of the two DSM-IV-TR (APA, 2000) dimensions of ADHD (e.g., Collett, Crowley, Gimpel, & Greenson, 2000; DuPaul et al., 1997; Molina, Smith, & Pelham, 2001) for elementary and secondary school samples; however, the same model of ADHD has not been validated with a normative sample of preschool-age children.
Furthermore, Lahey, Pelham, Loney, Lee, and Willcutt (2005) investigated the stability of the presentation of ADHD symptoms and subtype in a sample of 118 four- to six-year-old children diagnosed with ADHD. Participants were followed for 8 years to assess the stability of ADHD. Findings indicate that most of the children maintained a diagnosis of ADHD over the course of the study; however, the presentation of symptoms and subtypes was unstable. Children originally diagnosed with ADHD-combined type were more likely to continue to be diagnosed with ADHD than children in the hyperactive-impulsive subtype. Children originally diagnosed with combined type and inattentive type did show some shift in subtype presentation, but children initially diagnosed with hyperactive-impulsive type were most likely to shift subtype as they aged. Thus, these results lead to a conclusion that the use of the subtype classification may not be useful in the diagnosis of preschool children (Lahey et al., 2005).
Given the lack of developmentally appropriate criteria, the rapid developmental change in the preschool years (DuPaul & Kern, 2011) and the shift in the presentation of symptoms as a child developed (Lahey et al., 2005), researchers have posited that the factor structure may be different for preschool-age children. Hardy and colleagues (2007) recognized the need for this research and investigated the factor structure of ADHD within a clinic-referred preschool-age population. Parent and/or teacher ratings were collected from 532 clinic-referred preschool-age children. Parent and teacher ratings were analyzed separately using confirmatory factor analysis (CFA) and follow-up exploratory factor analysis (EFA). Initial CFA ratings revealed moderate fit for the two-and three-factor models of ADHD symptoms for parent ratings and poor fit for all three models based on teacher ratings. However, maximum likelihood EFAs confirmed a two- and three-factor model with satisfactory fit for both the parent and teacher ratings. Thus, the accepted model for older children with ADHD and the model espoused by the DSM-IV-TR (APA, 2000) may not be accurate for younger children with ADHD. However, a clinic-referred population of preschool children may yield significantly different results than a normative sample.
The purpose of the present study is to expand the previous literature based on the factor structure of the 18 DSM (4th ed.; DSM-IV; APA, 1994) ADHD symptoms according to parent and teacher ratings within a large, community, normative sample of preschool children. While the research is robust for school-age children with ADHD, the validity of the two-factor model of ADHD for preschool-age children is lacking. Previous research has been conducted with clinic-referred preschool-age children but no large-scale study of data from a community, non-referred sample has been undertaken. The goal of the study is to examine three alternative models based on theoretical and empirical arguments concerning the latent structure of the data from the ADHD-Rating Scale-IV–Preschool Version. The hypothesis is that the three-factor model will fit the data best.
Method
Participants
Parent ratings were collected on 907 children in the South, Northeast, West, and Midwest regions of the United States. The sample included 479 boys (53%) and 423 girls (47%), and 5 not indicating gender, 3 years 0 months to 5 years 11 months of age (M = 3.80, SD = 0.66). Categorization of the children’s ages was as follows: 33% of the children were 3 years of age, 53% of the children were 4 years of age, and 13% were 5 years of age. Ethnicity of the children was as follows: 44% Caucasian, 37% African American, 3.4% Hispanic American, 6.5% Asian American, 4.5% designated as other, and just over 4% not indicating ethnicity. Parent respondents to the ADHD questionnaire were primarily mothers (87%), with 7% being fathers and 4% classified as other. Of the 907 parent responses on the 18 items of the survey, only a handful of parents did not fill out all of the items, leaving a final sample size of 863 for analysis. This is just less than 5% of the sample. A missing data analysis in EQS did not indicate any specific pattern, so missing at random was assumed.
Teacher ratings on 995 children, 3 years 0 months to 5 years 11 months of age (M = 3.84, SD = 0.64) were examined. Thirty percent of the children were 3 years of age, 57% were 4 years of age, and 14% were 5 years of age. Teachers were predominantly teaching in general education preschool settings (95.7%) with experience ranging from 1 to 46 years (M = 11.58, SD = 8.06). Thirty-two teachers were dropped from the analysis due to missing data, and another 11 were dropped due to multi-variate normality problems, leaving a total of 952 complete teacher ratings.
Based on MacCallum, Browne, and Sugawara (1996), there is adequate power for the analysis.
Measures
ADHD-Rating Scale-IV–Preschool Version, an 18-item symptom questionnaire, was used to obtain parent and teacher ratings on the sample. Each teacher rated the frequency of occurrence of ADHD symptoms. The symptom descriptions of this scale were derived from the DSM-IV-TR (APA, 2000) and appear to be a reliable and valid measure (McGoey, DuPaul, Haley, & Shelton, 2007). Raw scores for inattention, hyperactivity-impulsivity, and total scores were converted to T scores and percentile ranks. Reliability coefficients ranged from .80 to .95, indicating good test–retest reliability.
Procedures
The sample used for this analysis was part of a larger data set that was collected to provide normative data, reliability, and validity of the ADHD-Rating Scale-IV–Preschool Version. Procedures specific to the collection of the ratings can be found in McGoey et al. (2007).
Data Analysis
A CFA was conducted to evaluate the factor structure of ADHD for young children as rated by parents and teachers. The three alternative models examined included a one-factor, two-factor, and three-factor model with the use of both parent and teacher data. The fit of each model was analyzed to determine the best fitting factor structure for each set of data.
Results
The EQS 6.1 (Build 97) software was used to conduct the CFA using maximum likelihood with robust standards and considering the data as ordered categorical. Data were cleaned and examined for outliers, normality, and linearity (Tabachnick & Fidell, 2001). The item-correlation tables are available from the first author.
Parent Ratings
Three alternative models were examined with the parent response data: one-, two-, and three-factor models. The one-factor model failed to converge even after changing the iteration levels multiple times. The two-factor model results indicate a good fit between the data and the model. The Satorra–Bentler Chi-Square was 493.71 (df = 134), root mean square error of approximation (RMSEA) = 0.054 (90% confidence interval [CI] [0.048, 0.059]), comparative fit index (CFI) = 0.98, and the non-normed fit index (NNFI; Tucker–Lewis index [TLI]) = 0.98. These fit indices were chosen based on their consistency over time in simulation studies such as Sivo, Fan, Witta, and Willse (2006). The residuals were normally distributed and the Lagrange Multiplier test did not indicate need for any statistical changes to the model though the chi-square value and RMSEA do indicate some misfit overall. The three-factor model had a Satorra–Bentler Chi-Square of 455.16 (df = 131), RMSEA = 0.054 (90% CI [0.048, 0.059]), CFI = 0.98, and the NNFI (TLI) = 0.99. To compare the two- and three-factor models, the Akaike information criterion (AIC; Klein, 2011) was used. The AIC for the two-factor model is 200.58, and for the three-factor model, it is 193.16. These values indicate that the three-factor model is a better fit and more likely to replicate (Klein, 2011). Bayesian information criterion (BIC) values provide the same inference. The BIC was 1,537.03 for the two-factor model and 1,442.74 for the three-factor model. Table 1 provides the factor values for each item for the three-factor model.
Structure Matrix for Standardized Solution Parent and Teacher Responses.
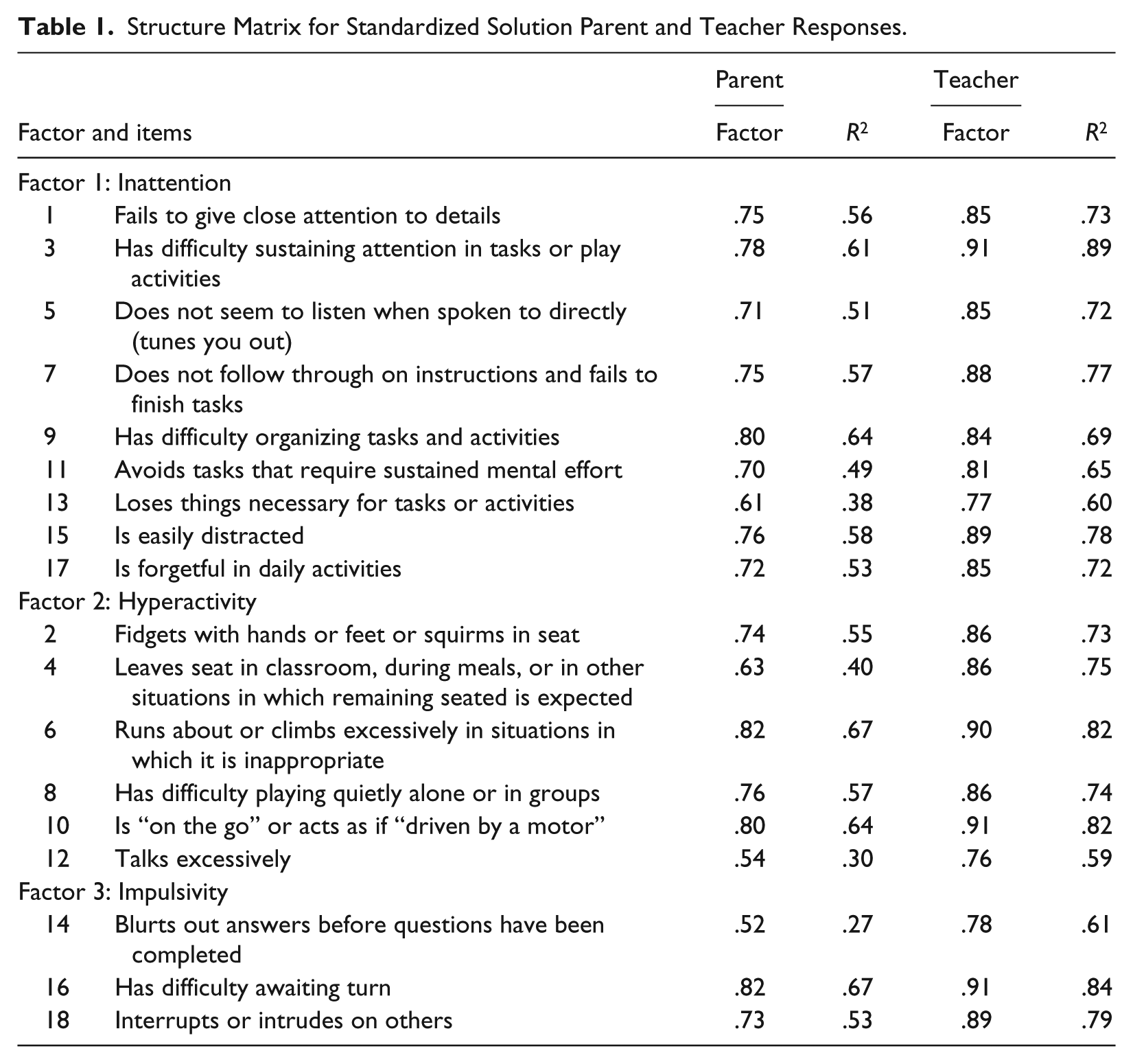
Given these results, examining the three-factor model more closely indicates that the model is not explaining the relationship between Items 12 and 14 very well; a residual value of 0.19. This value is due to the association between the items talks excessively and blurts out answers and theoretically this makes sense. Therefore, we correlated the errors between these items and the results indicate a better fit. The Satorra–Bentler Chi-Square is 348.23 on 130° with a CFI = 0.99, TLI = 0.99, and RMSEA = 0.044 (CI [0.039, 0.050]). See Figure 1.

Three-factor model of ADHD symptoms in preschool-age children as rated by parents.
Teacher Ratings
The same analysis was run with teacher response data. Three alternative models were examined with the teacher response data: one-, two-, and three-factor models. The one-factor model for teachers did converge with a Satorra–Bentler Chi-Square value of 1088.96 (df = 135) and an AIC of 818.96. The two-factor model results indicate a good fit between the data and the model. The Satorra–Bentler Chi-Square was 683.66 (df = 134), AIC = 415.67, RMSEA = 0.065 (90% CI [0.060, 0.070]), CFI = 0.99, and the NNFI (TLI) = 0.99. The residuals were normally distributed, and the Lagrange Multiplier test did not indicate a need for any statistical change to the model though the chi-square value and RMSEA do indicate some misfit overall. The three-factor model had a Satorra–Bentler Chi-Square of 467.06 (df = 131), AIC = 205.06, RMSEA = 0.052 (90% CI [0.047, 0.057]), CFI = 0.99, and the NNFI (TLI) = 0.99. To compare the three-factor alternative, again the AIC was used (Klein, 2011). The AIC for the three-factor model was the lowest again, indicating that the three-factor model is the best fit and most likely to replicate (Klein, 2011). BIC values provide the same inference. The BIC values were 430.44 for the two-factor model and 334.39 for the three-factor model. Table 1 provides the factor values for each item for the three-factor model.
Based on the previous results, we correlated the relationship between Items 12 and 14. The Satorra–Bentler Chi-Square value was 457.29 (df = 130), CFI = 0.99, TLI = 0.99, and RMSEA = 0.044 (CI [0.039, 0.050]). One can consider the correlated error as a nested model and look at the difference in chi-square values and degrees of freedom as a test. There is a difference of 9.77 and 1 degree of freedom, which would be statistically significant at the .01 level, indicating that the correlated error model is a statistically better fit.
For both final models, the correlations between the three factors are quite high indicating a strong relationship between the three. When considering parent responses, there was a positive correlation between the factors: Inattention (Factor 1) and Hyperactivity (Factor 2), r = .88; Inattention (Factor 1) and Impulsivity (Factor 3), r = .87; and Hyperactivity (Factor 2) and Impulsivity (Factor 3), r = .86. Correlated errors were calculated and found to be .26. A similar pattern of correlations was found with the factors according to teacher responses: Inattention (Factor 1) and Hyperactivity (Factor 2), r = .92; Inattention (Factor 1) and Impulsivity (Factor 3), r = .89; and Hyperactivity (Factor 2) and Impulsivity (Factor 3), r = .92. Correlated errors were calculated and found to be .42. Both models were characterized by strong relationships among all three factors. Although the correlations are high among the factors, a higher-order factor model did not fit the data. See Figure 2.

Three-factor model of ADHD symptoms in preschool-age children as rated by teachers.
Discussion
The purpose of this study was to examine alternative models of the 18 item DSM-IV-TR (APA, 2000) ADHD symptoms of inattention and hyperactivity-impulsivity for the preschool population. The findings of the present study indicate that a three-factor model, inattention, hyperactivity, and impulsivity, for the presentation of ADHD in preschoolers based on both parent and teacher report data had the best fit. Although the factors were highly correlated, and the two-factor model also fit the data, statistically the three-factor model was the best fit to the data. Thus, according to this study the presentation of ADHD in young children may include three behavioral domains (inattention, hyperactivity, and impulsivity). Similar results were found for both parent and teacher report, pointing to a consistent behavioral profile for children exhibiting these behaviors in the home and school environments.
The three-factor model of ADHD for preschool children found in this study differs from the DSM-IV-TR (APA, 2000) and DSM-5 (APA, 2013) two-factor model currently widely accepted for elementary- and secondary-age children (Collett et al., 2000; DuPaul et al., 1997; Molina et al., 2001). However, the three-factor model may match the research, clinical findings, and unstable behavioral presentations for preschool children with ADHD (Hardy, et. al., 2007; Lahey et al., 2005). The combined domain of hyperactivity and impulsivity that is typical for older children with ADHD was not completely supported by the results of the present study. The results indicate that the conceptualization of ADHD may include a distinction between hyperactivity and impulsivity that is more applicable to younger children.
The current findings are also supported by the minor changes in the diagnostic criteria in the new DSM-5 (APA, 2013). The new guidelines kept the same symptoms but provide developmentally appropriate examples of each one. This may help the clinician determine whether the child is presenting outside of typical developmental expectations. In addition, the DSM-5 (APA, 2013) no longer classifies subtypes of ADHD but rather uses different presentations to qualify the symptoms. This allows for a more continuous view of the symptoms as opposed to a dichotomous view in previous DSM guidelines. These changes are supported by the current findings in that ADHD may not present as two distinct dimensions in the preschool age. The changes in the DSM-5 (APA, 2013) allow for growth and change as the child develops.
Implications for Practice
The findings of this study indicate that preschool children with ADHD symptoms may present with three distinct clinical profiles. Clinicians may want to gather information on hyperactive and impulsive symptoms separately as opposed to using one descriptor that encompasses both characteristics. By focusing on each characteristic separately, the clinician may be able to better parse out the developmentally appropriate behaviors from the atypical presentation, thus guiding the clinician to a more accurate diagnosis.
Clinicians may also want to target each factor separately in treatment. A young child may need treatment goals that target difficulties that are specific to hyperactivity and impulsivity separating. Relevant treatment goals may include waiting in line, sitting still, and finishing a task, all of which may be separate skills to be mastered. When considering a three-factor model of ADHD, clinicians could then expect young children to respond to treatment in differing ways in the domains of attention, hyperactivity, and impulsivity. As a result, providing interventions to address a child’s hyperactive behaviors may not also help improve his or her impulsive behaviors. The results of the present study allow for more individualized and clinically relevant treatment planning for young children presenting with ADHD symptoms.
Limitations
The use of a community-based sample of parent and teacher ratings is advantageous in many respects, however not without limitations. The parent and teacher ratings in this study appeared to have a floor effect with children receiving a rating of never for most symptoms. In addition, parent and teacher ratings were not conducted for the same children in the sample. The present study used only the ADHD-Rating Scale-IV–Preschool Version as its measure of ADHD symptoms. A comprehensive assessment of ADHD would combine rating scales with parent and teacher interview and clinical impressions, possibly creating a different constellation of symptoms.
The use of Structural Equation Modeling (SEM) also gave rise to a number of limitations based on human error. As the researcher chose a model based on sound theory, the model chosen may not be the only accurate representation of the data. It was possible that other permutations of the measures and pathways may also yield results that “fit.” In addition, it was dependent on the researcher to choose the best indicators of the underlying latent variables with the least amount of measurement error. Therefore, it was possible that “truer” measures of the latent construct were not included.
In conclusion, this study provided support to the variability in ADHD symptoms in early childhood and the need for developmentally appropriate, thorough, multi-method, multi-informant procedures when assessing preschool children with ADHD. Furthermore, the results of this investigation imply that a three-factor model of symptoms of ADHD may be the best fit for parent and teacher ratings of preschool children, thus differing from the current DSM conception of ADHD symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.