
Abstract
Psychometric properties of the 30-item Family Resource Scale (FRS) were examined in a sample of families seeking assistance for their child’s behavioral difficulties (N = 300). The FRS is a measure that assesses the adequacy of family resources across several contexts including intra-family support and personal resources. Our analyses supported a modified 29-item four-factor solution (basic needs, extra money and time, time for family, and essential) compared with the seven-factor solution provided by the developers. Results showed that families’ perception of their resources as adequate across all domains was associated with better family functioning and less caregiver strain. Combined, our findings suggest modifications to the existent structure of the FRS.
Introduction
Behavioral difficulties in children refer to a wide range of issues ranging from internalizing and peer problems to hyperactivity, inattention, and impulsivity (Goodman, 1997). The reciprocal associations between child behavioral difficulties and parental stress are well documented (Gross, Shaw, & Moilanen, 2008; VanderValk, De Goede, Spruijt, & Meeus, 2007). More specifically, studies have shown that child behavioral difficulties may place a burden on a family functioning resulting in disruption of the family plans, leisure activities, and parents’ careers because of a need to provide a constant supervision and management of a child’s difficult behavior (Huang et al., 2005). According to the Systems of Care theory (Stroul & Friedman, 1986), child problem behavior is embedded in a larger family system, and behavior health services focusing on the child problem behavior should be provided to a family as a whole. The importance of informal supports (e.g., including contacts from a family’s broader social network or within a community) in helping families with children with behavioral difficulties is well acknowledged in the current research literature (Cook & Kilmer, 2010). Once we look deeper, we can find that some behavioral issues of children are related to a family’s resources. For example, a child’s acting out in school may be related to the bullying experienced during the walk to and from school, so finding safe transportation or a place to stay before/after school may greatly improve the child’s functioning. Likewise, when working with families, some may discontinue seeking professional counseling services for their child because they cannot afford the services. Advising families on how to identify providers that accept a sliding fee payment or local assistance programs may be the primary help needed to the child receiving the needed professional support. Thus, it is essential that practitioners have access to family resource assessment measures that are quick and psychometrically sound, while providing information that they can use to develop meaningful service plans that meet the specific needs of the family. In addition, the use of the rating-scale-type measures for assessing family resources is more efficient for the child welfare practitioners because of the ease of administration and minimum training requirements, compared with the clinical interviews.
The Family Resource Scale (FRS)
The FRS is a widely utilized measure assessing the adequacy of resources across several areas of family functioning, including physical necessities and health, personal and financial resources, and intra-family support (Dunst & Leet, 1987). However, the FRS was developed more than three decades ago, and has serious limitations. The psychometric properties of the 30-item FRS questionnaire were originally established in a sample of 45 mothers, and the authors proposed a seven-factor solution (Dunst & Leet, 1987). The validation of the original FRS has been widely criticized in the research literature due to the fact the original sample size in the Dunst and Leet (1987) study was too small for the factor analysis that was conducted, and unrepresentative of the general population (McGrew, Gilman, & Johnson, 1992). Indeed, even though no specific rule exists with regard to the appropriate sample size for the factor analysis, common recommendations suggest using a ratio of at least 10 (Velicer & Fava, 1998), five (Bryant & Yarnold, 1995), three (Arrindell & Van der Ende, 1985), or two (Kline, 1979) subjects for each item in the instrument that is being used, which would require a sample size of 60 to 300 participants to test a 30-item questionnaire. Furthermore, only total scale reliability was reported (α = .92) in the original study (Dunst & Leet, 1987), whereas the evidence on the psychometric properties of the seven subscales derived during factor analysis was not provided. Therefore, this instrument requires psychometric validation to be used properly with the families of youth with child behavioral needs.
Given the limited psychometric evidence of the original FRS scale (Dunst & Leet, 1987), several efforts to validate the FRS factor structure were undertaken by various research groups providing support for the three-, four-, or a six-factor solution (compared with the seven-factors solution suggested by the developers). A three-factor solution was reported by Rhodes et al. (2012) who validated psychometric properties of the FRS in a sample of 235 families with children ages 4 to 11 years recruited at pediatric clinics in Australia as a part of the pediatric health promotion. For this sample, the exploratory factor analyses (EFA) provided support for a three-factor FRS solution: basic needs, additional financial needs, and time for self and family. In this study, about 15% of families were identified as having less than adequate resources on the FRS subscale of basic needs.
Furthermore, Van Horn, Bellis, and Snyder (2001) examined the psychometric properties of the FRS in a large national sample of low-income families with children attending Head Start programs, and reported support for a four-factor solution: basic needs, time for self, time for family, and money. Their study was a part of a 31-site longitudinal intervention study of former Head Start children, and used a sample of N = 6,320 children for exploratory analyses, and N = 7,185 children for confirmatory analyses. However one major limitation of their analyses refers to elimination of about one third of the FRS items resulting in a short 20-item FRS scale that could potentially compromise the usefulness of the FRS in identifying unique family’s needs and stressors. Moreover, it was focused only on kindergarten and third-grade children, and did not include a range of child ages.
The FRS was also validated in a sample of families of children (N = 2,010) in treatment for emotional and behavioral disorders (Brannan, Manteuffel, Holden, & Heflinger, 2006). This study reported support for a six-factor solution of the FRS: basic needs, housing and utilities, benefits, social needs/self-care, child care, and extra resources. But despite its important contribution, this study has two major limitations. First, the data from this project was based on two research studies with very unique samples that can potentially compromise the generalizability of the findings. The sample in a first study consisted of children from military families (n = 984), whose emotional and behavioral problems might as well arise as a part of the military families’ experience, such as separation from a parent, frequent moves, change of schools, and difficulties with establishing and maintaining peer relations (Chandra et al., 2010). The sample in a second study was drawn from a larger study focusing on older children and adolescents (up to 22 years of age) with serious disabilities (e.g., participants were required to have a clinical diagnosis as defined by the Diagnostic and Statistical Manual for Mental Disorders [4th ed.; DSM-IV; American Psychiatric Publishing, 2013] that is present for at least 1 year). Second, both research studies were conducted back in 1992-1998, so the conclusions drawn from the data dated two decades ago may not have high relevance in the current social and economic environment.
Further reports on psychometric properties of the FRS subscales have been mixed due to the fact that majority of the studies used only a subset of the FRS items for analyses (e.g., time with family and friends, Hammer, Ernst Kossek, Bodner, & Crain, 2013; time adequacy, Moen, Kelly, & Lam, 2013; physical and human resources, and time allocation, Ompad et al., 2012; time adequacy for paid work, parenting, and family, Lee at al., 2015). Unfortunately, no further attempts have been made in validating psychometric properties of the FRS with a diverse population of families of children with emotional and behavioral issues. Thus, the purpose of this study is to examine the utility and psychometric properties of the FRS in a sample of families of children with behavioral difficulties, including the factor structure, internal reliability of the total score and factors, and the correlations among the factors and other related variables such as family-functioning and caregiver strain.
Method
Data used in the present study were collected as a part of the larger social intervention on improving parenting skills and family functioning that was conducted over the course of 5 years from August 2012; until September 2016, data for this study were obtained from the intake assessments prior to beginning of the in-home family services and include families assigned both to treatment and control conditions. Participants were caregivers that called a statewide family helpline to obtain support for children’s behavioral problems. Families eligible to participate (e.g., with children ages 5 to 14, fluent in English, and within a local geographic region) were invited to participate. Even though families could have called for assistance with multiple children at home, they were asked to identify a target child, and provided reports only for this child. After an intake assessment protocol was completed, families were randomly assigned to services as usual or an individualized intervention that lasted from 8 to 12 weeks. Study behavioral measures included caregiver strain, parenting practices and discipline, and child’s strengths and difficulties.
Participants and Procedure
Out of 1,385 families that met eligibility requirements for the study, 483 families (35%) agreed to talk with researchers about the study, 373 consented to participate, and 300 completed all intake measures. Thus, the final sample comprised 300 families. Data were collected using parent self-report via mailed paper and pencil surveys or online surveys. This study was approved by the University Institutional Review Board and all human subject protocols were followed. See Table 1 for the sample demographic information.
Demographic Characteristics of Families and Youth (N = 300).

Note. SDQ = Strengths and Difficulties Questionnaire.
Multiple responses allowed.
Measures
FRS
The original 30-item FRS (Dunst & Leet, 1987) was used in this study. The respondents were asked to indicate the response that best describes how well each need across several areas of family functioning was met on a consistent basis using a 5-point Likert-type scale ranging from “not at all adequate” to “almost always adequate.” Similar to procedures outlined by Van Horn et al. (2001), “does not apply” responses were recorded as “missing” because scoring them as zero in the original scale would mean treating the responses as “not adequate at all.”
The Caregiver Strain Questionnaire (CGSQ)
The CGSQ (Brannan et al. 1997) assessed the amount of strain associated with caring for children with behavioral difficulties. The CGSQ includes seven items that are rated on a five-point scale ranging from 1 = not at all a problem to 5 = very much a problem and assesses two dimensions of caregiver strain: subjective externalized strain (“How much of a problem was interruption of personal time resulting from your child’s problems?”) and subjective internalized strain (“How tired or strained do you feel as a result of your child’s problems?”). The total caregiver strain, calculated as a mean of seven items, was used for this study (α = .88). Higher scores indicate higher caregiver strain.
The Family Assessment Device (FAD)
The General Functioning subscale of the FAD (Epstein et al. 1983) was used for this study, which assessed family’s ability to make decisions regarding their functioning as a family (e.g., “Making decisions is a problem”). It includes 12 items on general family functioning that are rated on a four-point scale ranging from 1 = strongly disagree to 4 = strongly agree (α = .91). Higher scores indicate poorer family functioning.
Data Analysis
Our analyses were conducted over three phases. Fist, using a confirmatory factor analysis, the original factor structure of the FRS (Dunst & Leet, 1987) was not replicated, comparative fit index [CFI] = .83, Tucker–Lewis index (TLI) = .81, root mean square error approximation (RMSEA) = .07. In a search for the best solution, the factor structure of the FRS was examined using EFA in Mplus 7.3 (Muthén & Muthén, 1998-2010) with the robust weighted least squares (WLSMV) estimator to account for ordinal responses and non-normality. In Mplus, pairwise deletion is used when estimating models with the WLSMV estimator. After recoding “does not apply” responses on the FRS as “missing,” the amount of missing data in the FRS varied among items from 1% to 10%, with a few outliers having 13.6% (“Money to buy special equipment”), 21.9% (“Babysitting”), 37.2% (“Child care/day care”), and 37.9% (“Public Assistance”) of missing data. To determine the appropriate number of factors, model fit was evaluated across each of the six models (e.g., one-, two-, three-, four-, five-, and six-factor solution) using the CFI, the TLI, and the RMSEA. According to the current guidelines (Hu & Bentler, 1999), CFI and TLI values of .95 or greater and RMSEA values of .06 or less indicate acceptable model fit. The content of the items that factored together was further evaluated by the research team to determine the meaningfulness of each factor. Second, internal consistency of the newly emerged FRS was examined by estimating reliability coefficients using SPSS v. 22. Third, the relation between the revised FRS scale and other measures reflecting family functioning (e.g., caregiver strain and general family functioning) was examined by conducting bivariate correlation analyses.
Results
The first aim of the study was to examine the original factor structure of the FRS and explore potential existence of the other factors (Table 2). Although model fit indices for three-, four-, five- and six-factor solutions indicated a good model fit (i.e., CFI and TLI greater than .95, and standardized root mean square residual [SRMR] less than .08; Hu & Bentler, 1999), we carefully evaluated the content of the newly emerged FRS subscales considering application of our findings to family-centered child welfare services. Thus, despite the fact that model fit indices for five- and six-factor solutions were relatively good, they would have resulted in having highly correlated subscales as well as multiple factors with only two items, thus questioning the meaningfulness and usefulness of these subscales. A three-factor solution, on a contrary, would have resulted in having two heterogeneous factors (i.e., “basic needs” and “money and time for yourself”) consisting of sets of seemingly nonrelated items, and a third factor with only two items (i.e., “time for family”), which consistently emerged across all possible factor solutions. So, the four-factor solution provided the best explanation for heterogeneity in family resources, distinguishing between “basic needs,” “essential care,” “time for family,” and “extra money and time for yourself.” After eliminating one item (e.g., “Good job”) because it was contributing to two factors simultaneously with a loading of approximately .45, the four-factor solution still provided the best content and model fit. Correlations between factors ranged from r = .28 to r = .65 (Table 3). The resulting four-factor solution accounted for the 60.79% of the variance in the item response data.
Fit Indices for Exploratory Factor Analysis Model.
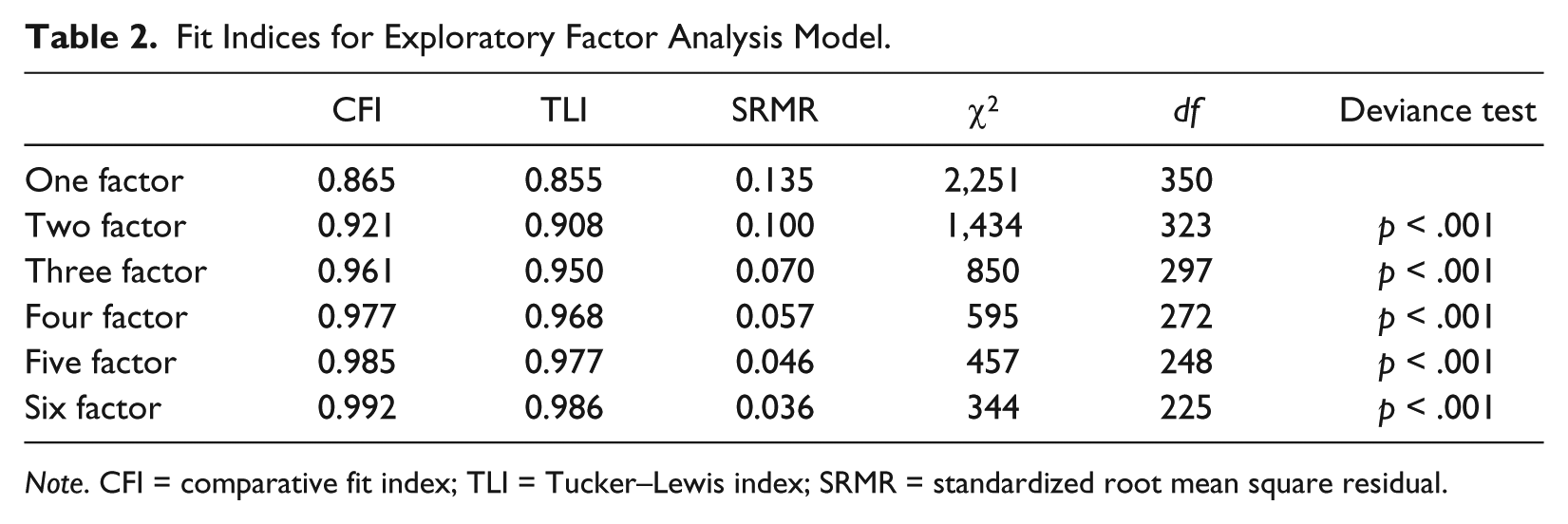
Note. CFI = comparative fit index; TLI = Tucker–Lewis index; SRMR = standardized root mean square residual.
Interfactor Correlation Matrix of FRS dimensions.
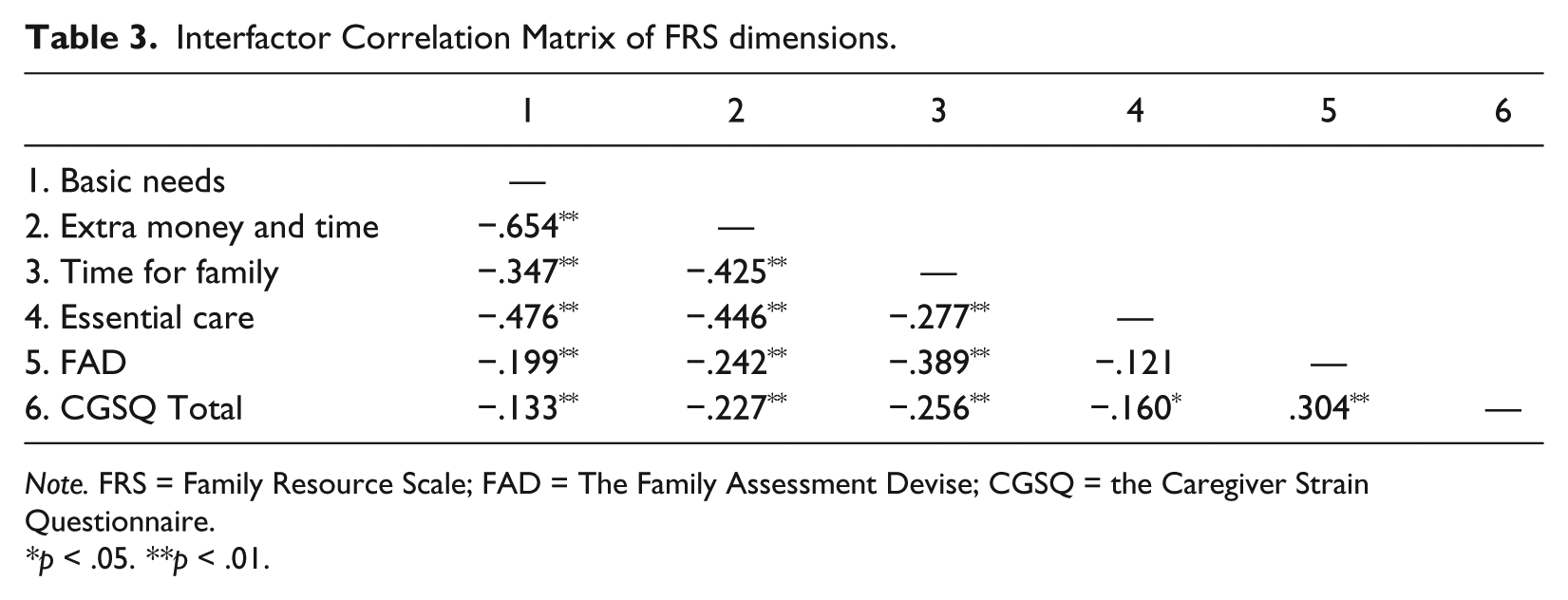
Note. FRS = Family Resource Scale; FAD = The Family Assessment Devise; CGSQ = the Caregiver Strain Questionnaire.
p < .05. **p < .01.
The second aim of the study was to examine internal consistency of the newly emerged subscales. Subscale scores were created by taking the mean of the items with the caveat that no more than 20% to 25% of the items should be missing for that subscale (for subscales with three or more items). The four subscales were basic needs (10 items; α = .89), extra money and time (13 items, α = .94), time for family (two items, α = .90), and essential care (four items, α = .64). Table 4 presents the item factor loadings for each of the four subscales.
Emerged Factor Structure of the Family Resource Scale.

Note. aItem was deleted during factor analysis.
The third and final aim of the study was to examine the relation between the revised FRS and other variables reflecting family functioning (e.g., caregiver strain and general family functioning). As expected, correlation analyses demonstrated that higher satisfaction with the family resources across all of the FRS domains including basic needs (r = −.13, p < .05), extra money and time (r = −.23, p < .01), time for family (r = −.26, p < .01), and essential care (r = −.16, p < .05) was associated with significantly less caregiver strain. Similarly, higher satisfaction with the family resources in domains of basic needs (r = −.20, p < .01), extra money and time (r = −.24, p < .01), and time for family (r = −.39, p < .01) was associated with better general family functioning.
Discussion
In our study, we utilized an EFA approach to examine psychometric properties of the FRS in families of children with behavioral difficulties. Two major findings evolved from our analyses: First, our results provided support for a four-factor solution for the family resources: basic needs, extra money and time, time for family, and essential care. Second, the revised FRS subscales were examined for relation with the other variables reflecting family functioning (e.g., caregiver strain and general family functioning) and demonstrated associations that were in expected directions. Each of the findings is discussed in the following.
The analyses involving the search for the best factor structure solution favored a four-factor solution, and highlighted the similarities and differences with the previous research on FRS. Thus, the four-factor solution supported by our analyses supports certain core factors, such as basic needs, time for self, time for family, and money that were present in different variations in previous studies (e.g., basic living needs, additional financial needs, time for self and family, Rhodes et al., 2012; basic needs, housing/utility, benefits, social needs/self-care, child care, extra resources, Brannan et al., 2006; basic needs, money, time for self, time for family, Van Horn et al., 2001).
Furthermore, similar to previous research emphasizing the reciprocal associations between child behavioral difficulties and parental stress (Gross et al., 2008; VanderValk et al., 2007), family perception of their resources as more adequate across all four domains (e.g., basic needs, extra money and time, time for family, and essential care) was associated with the lower scores on caregiver strain and higher family functioning. Although these associations were in the expected direction, they were mostly moderate in size, possibly indicating the omission of important factors (which were beyond the scope of the present study) that could potentially influence the associations between caregivers’ perceptions of their resources and their strain and family functioning. Previous research indicated that some characteristics of the caregivers, such as emotional and physical health (Butterworth, Pymont, Rodgers, Windsor, & Anstey, 2010; Williams et al., 2008) were associated with more caregiver strain and family conflict, even after controlling for caregivers’ age, gender, education, and income. In this regard, future research should consider taking into account not only child but also caregivers’ characteristics when assessing the perceptions of their resources.
It is also of note that the four-factor solution supported with our data did not replicate any of the existing factor solutions from the previous studies. For example, our exploratory analyses indicated that a three-factor solution that was originally considered by our research team would not have matched a three-factor solution reported by Rhodes et al. (2012). Similarly, five- and six-factor solutions that were also considered during our exploratory analyses would not have matched a six-factor solution reported by Brannan et al. (2006), and a final four-factor solution from our study is different from a four-factor solution reported by Van Horn et al. (2001). The fact that the FRS performs differently in different studies may be due to different populations used by the researchers. Thus, the studies reviewed above reported using data from pediatric clinics (e.g., Rhodes et al., 2012), low-income Head Start families (e.g., Van Horn et al., 2001), and families with children and adolescents (up to 22 years of age) in treatment for emotional and behavioral disorders (e.g., Brannan et al., 2006). These discrepancies suggest that a future research should consider a multiple-group confirmatory factor analysis, which would allow simultaneous tests of data from different populations to see how measurement models differ across different populations, and to test whether these differences are statistically significant. Qualitative analyses, where respondents are asked to explain their understanding of what each item is asking and their response option, also might be helpful in refining the quality of the FRS (Bowen, 2008). For example, some items, such as “public assistance” or “money for special equipment,” may be interpreted differently by families who are using public assistance or in need of a special medical equipment for their child compared with families who do not have these needs. Interviewing families to gain understanding of their perceptions of the items may be a critical next step in improving FRS.
Limitations and Future Research
There are several methodological limitations of the study that need to be acknowledged. First, the results of this study are based on a sample of families and children with behavioral difficulties that was drawn from one geographic location, which may potentially limit the generalizability of the findings, especially given differences in the available resources for families living in urban versus rural locations. It will be important to replicate these findings with multiple samples drawn from different geographic locations, and urban and rural settings. In addition, future studies may consider revising the FRS to include addition constructs that might influence family resources, such as religious/spiritual needs, needs for continuous adult education, legal help, and financial future planning, which are not a part of the FRS (McGrew et al., 1992).
However, despite these limitations, our study has important implications for practitioners. Using a tool with known psychometric properties would allow practitioners to have a clear starting point for a discussion of the areas of need for the family. As shown in a previous research (e.g., Pecora, Whittaker, Maluccio, & Barth, 2012), many behavioral difficulties in children develop as a result of the difficult living conditions in a family (e.g., difficulties with acquiring dependable transportation, lack of the telephone), rather than a consequence of mental health issues. Appropriate assessment of the family resources can make a significant difference in establishing connections between a family and the services they need from the various agencies, and ultimately result in better health and well-being outcomes for families of children with behavioral difficulties.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant 2617100101001 to the University of Nebraska–Lincoln by Father Flanagan’s Boys Town.