
Abstract
The Mexican health paradox refers to initially favorable health and mental health outcomes among recent Mexican immigrants to the United States. The subsequent rapid decline in Mexican health outcomes has been attributed to the process of acculturation to U.S. culture. However, the construct of acculturation has come under significant criticism for oversimplifying complex relations between health, behavior, race and ethnic relations, and the environment. Moreover, measurement issues for the construct abound. This article reviews the current state of the acculturation debate, and argues for an integration of current theoretical perspectives and critiques of the construct in order to strengthen the explanatory power of acculturation with regard to the Mexican health paradox.
The purpose of this article is to review the current state of the acculturation debate, and argue for an integration of current theoretical perspectives and critiques of the construct in order to strengthen the explanatory power of acculturation with regard to the Mexican health paradox (MHP) or the decline of the initially favorable health and mental health outcomes of Mexican immigrants. The article begins with a brief overview of the MHP, followed by a review and critique of current debates surrounding the construct of acculturation. Challenges of quantifying and measuring levels of acculturation are also noted. Next, we articulate our refined view of Berry’s acculturation theory, including acculturative stress, as well as review related research based on segmented assimilation theory to deepen our understanding of the MHP. Finally, key health indicators in the paradox literature (mental health outcomes, birth outcomes, and Type 2 diabetes) are reviewed to underscore the need to integrate theory-based descriptive analyses of the acculturation/segmented assimilation experience to better understand how environmental, social, cultural, and individual determinants of health converge to affect the health and well-being of Mexican descent people in the United States. Recommendations for research and theory are offered.
The Mexican Health Paradox
The MHP has been the source of much intrigue for researchers. Low SES Mexican immigrants appear largely immune to many of the injurious health effects of migration, poverty, racism, discrimination, and other factors that typically affect racial and ethnic minorities in the United States. More specifically, Mexicans have lower overall mortality rates than Whites on most major health indicators (Morales, Lara, Kington, Valdez, & Escarce, 2002). However, this favorable disposition rapidly erodes with increasing time, and across generations, in the United States. The lower incidence of mental health disorders, cancer, cardiovascular disease, infant mortality and low infant birth weight among Mexican immigrants has been termed paradoxical because of this population’s generally low socioeconomic status (SES), stress of adapting to a new country, language and other access barriers to health care associated with negative health outcomes (Markides & Coreil, 1986; Zsembik & Fennell, 2005). For example, Guendelman & English (1995) showed that healthy birth outcomes among Mexican immigrants disappear within five years in the United States, a change that the authors attribute to increases in unhealthy behaviors such as maternal smoking, drinking, and poor diet. Multiple large-scale studies on the prevalence of mental disorders among Mexican immigrants and U.S. born Mexican Americans show a distinct increase in certain mental disorders over time and across generations (Alegria et al., 2007; Alderete, Vega, Kolody, & Aguilar-Gaxiola, 2000; Vega et al., 1998). Several theories have been posited to explain the MHP and in general, protective dimensions of Mexican culture have been described as responsible for initial positive health outcomes.
Acculturation to U.S. culture has been broadly deemed responsible for health and mental health declines of Latinos in the United States. (Abraido-Lanza, Armbrister, Florez, & Aguirre, 2006; Lara, Gamboa, Kahramanian, Morales, & Bautista, 2004; Viruell-Fuentes, 2007). Similarly, the construct of acculturation has been broadly adopted as the main explanatory factor without sufficient theoretical critique, measurement or even agreement on its definition (Chun, Balls Organista, & Marín, 2003; Hunt, Schneider, & Comer, 2004). The cultural buffer hypothesis posits that aspects of traditional Latino culture, in particular the centrality of family, seem to buffer stressful life circumstances that lead to the poor health outcomes experienced by other groups of similarly low SES (Hovey, 2000). Furthermore, religiosity (typically Catholicism) and spirituality have been associated with stress-buffering effects in Latino adolescents (Wills, Yaeger, & Sandy, 2003), as well as lower levels of drinking, smoking, and sexual risk-taking particularly among Latina immigrant women and adolescents (Aranda, Castaneda, Lee, & Sobel, 2001; Bacallao & Smokowski, 2007; Caballero, 2005; Campos et al., 2008; Guendelman, Gould, Hudes, & Eskenazi, 1990). According to acculturation theory, however, the protective buffer of traditional Mexican culture diminishes with greater acculturation to mainstream U.S. society. Given the centrality of the construct of acculturation in explaining the MHP, a critique of its popularity and controversy in the literature is provided.
Acculturation as a Problematic Explanatory Construct
There is currently no uniform definition of acculturation (Trimble in Chun et al., 2003; Hunt et al., 2004; Lara et al., 2004; Rudmin, 2003), originally defined in the anthropological literature as the process by which “members of different autonomous cultural groups come into continuous firsthand contact, with subsequent changes in the original cultural patterns and custom of either or both groups (e.g., language, values, lifestyle, attitudes, identity)” (Redfield, Lipton, Herskovits [1936, p. 5], in Organista, 2007a). It is now generally understood as a complex, multidimensional process that cannot be adequately described as linear movement from “Mexican” to “American,” but as involving multiple and distinct outcomes depending on individual, minority group-level, and minority-majority group relations and factors.
Historical context
An update of the original anthropological definition modifies the previous one by acknowledging multiple routes to and results of acculturation:
[Acculturation is] Culture change that is initiated by the conjunction of two or more autonomous cultural systems. Acculturative change may be the consequence of direct cultural transmission; it may be derived from non-cultural causes, such as ecological or demographic modification induced by an impinging culture; it may be delayed, as with internal adjustments following upon the acceptance of alien traits or patterns; or it may be a reactive adaptation of traditional modes of life. (Social Science Research Council, 1954, p. 974)
While this 1954 definition remains one of the most highly cited, an increasing number of scholars call for an expansion of the construct to guide research. For example, Padilla & Perez (2003) regard the above definition as an improvement upon earlier definitions because it provides for more choice in the acculturation process or selective patterns at the individual, psychological level.
While the multidimensionality of acculturation is now generally accepted, and researchers acknowledge that unidimensional models are antiquated, they remain the most widely used in large-scale health studies (Abraido-Lanza et al., 2006; Arcia, Skinner, Bailey, & Correa, 2001; Berry, 1997; Cabassa, 2003; Campos, Schetter, Walsh, & Schenker, 2007; Escobar & Vega, 2000; Hunt et al., 2004; Rumbaut, 1997a; Ward, 2008). The understanding of acculturation as a complex process is a recent addition to the cannon of social science literature. Based on the experience of many European immigrants to the United States in the early 20th century, sociological texts on assimilation espoused the theory that immigrants inevitably become part of the all-American “melting pot” by relinquishing their own cultural values, norms and beliefs to become “American” and shedding their native identity (Gordon, 1964; Warner & Srole, 1945). Furthermore, it was broadly believed that assimilation (generally to white, middle class norms) was necessary for “successful” and healthy adaptation to the United States (Rumbaut, 1997b).
The “new immigration” after 1965, primarily of immigrants from Latin American and Asia, necessitated new ways of thinking about acculturation distinct from the more linear process of assimilation and upward mobility experienced by European immigrants (Kearney, 1995). For example, the immigrant experience for Latinos is distinct from their European counterparts who despite initial inter-European ethnic difficulties and discrimination were ultimately able to ascend the socioeconomic ladder given their racial and cultural similarity to mainstream society (Organista, 2007a). For Latinos, and other groups of color, acculturation and adjustment have been more challenging. Nguyen (2006) points out that, due to skin color, Latinos are generally distinguishable as “other” and thus upward mobility has been difficult because of racism and rising inequality wherein the middle rungs of the ladder, once thought accessible via the American dream of hard work, are missing for those without a college degree. This is a distinct change from the first wave of immigrants for whom hard work, working class wages, and racial and cultural similarity facilitated ascension to middle class status.
Social scientists referring to the new (post-1965) immigration experience, assert that immigrants experience a complex process in which they may incorporate aspects of the majority culture, retain aspects of their own culture, and everything in between, depending on the conditions of their immigration status (e.g., refugee vs. sojourner), their experience with the host culture and its policies, and their own individual expectations and desires or acculturation strategies (Zhou, 1997).
Current Critiques of Acculturation
Despite the emergence of more nuanced theories of acculturation (e.g., Castro, Shaibi, & Boehm-Smith, 2009; Padilla & Perez, 2003) many large-scale studies of acculturation and Latino health do not reference a theoretical framework, and a majority does not even define acculturation (Hunt, et al., 2004; Thomson & Hoffman-Goetz, 2009). Instead, most use proxy variables such as language preference or time in the United States. While these epidemiological studies are vital in documenting population level health trends over time, a growing body of critiques challenge such acculturation research because it may inadvertently reify antiquated notions of acculturation as linear process (Escobar & Vega, 2000), and oversimplify the complexity of health declines over time in some Latino populations.
A major criticism of studies invoking acculturation and the cultural buffer hypothesis is that they assume that Mexican immigrants bring with them a monolithic culture that is “new” to the United States. Hunt et al. (2004) point out that such studies ascribe so-called “traditional” characteristics such as familism, traditional gender roles and “religiously based morality” to Hispanic culture, whereas “purportedly ‘modern’ characteristics, such as individualism and greater independence from family support, high stress and tolerance for self-destructive behaviors are ascribed to ‘mainstream’ culture” (p. 979). Such assertions are both derogatory toward immigrant culture and illogical given that these two cultures have existed side-by-side and with increasing interpenetration for well over a century (Rudmin, 2003). Hunt and colleagues (2004) also point out that we now live in a globalized world wherein mass communication and media have few borders, thus the idea that Mexican and U.S. culture are new to each other seems embedded in the antiquated melting-pot model of immigrant assimilation.
Operationalization challenges
If acculturation refers to the process of adapting to “mainstream” culture, it becomes difficult to parse out what exactly is meant by “traditional” or “minority” versus “majority” culture, especially given the multicultural and transnational society in which we now live (Santiago-Irizarry, 2008). In their critique of the cultural buffer hypothesis, Hunt et al. (2004) assert that the haphazard application of “Latino culture” in acculturation studies both oversimplifies the fluidity and complexity of culture, and also tends toward stereotypy: “ethnic culture is understood as ‘primitive’ and natural, either disruptive and degenerate, or pristine and harmonious, but always instinctive and inherent rather than rational and intentional. Thus the ethnic culture is understood to lie in contrast to the advantages and pitfalls of Western culture, with the acculturating individual proceeding away from tradition and toward modernity” (p. 980). Rudmin (2003) similarly notes that historical constructions of acculturation are rooted in damaged or devalued views of minority ethnic groups that are remedied by acculturation. As noted below, our view is rooted in a view of the acculturation process as potentially damaging to certain minority groups, to varying degrees, depending on the circumstances.
Chun & Akutsu (2003) lay out a list of problematic assumptions inherent in current conceptualizations of acculturation throughout the literature: “(1) acculturation has been primarily viewed as a unidimensional and static construct; (2) measurement strategies are insufficient and inconsistent; (3) most acculturation research ignores macro level influences on family acculturation; (4) acculturation is primarily viewed as a post migration phenomenon; (5) acculturation experiences of generational cohorts are perceived to be monolithic and uniform; (6) ethnic minority families are viewed as passive respondents to their environment; (7) transnational experiences and identities are frequently overlooked” (pp. 111-113). Adding to this lengthy list is the premature conclusion that acculturation is hazardous to health. Although much of the current literature equates increasing acculturation with declining Mexican health, acculturation as originally conceptualized by Redfield et al. (1936), later by Berry (2003), and more recently by Rudmin (2009) and Lopez-Class, Castro, & Ramirez (2011), is not inherently negative, but highly dependent upon the conditions of acculturation for different racial and ethnic minority groups (Chun, Balls Organista, & Marin 2010).
Escobar and Vega (2000) consider acculturation a fuzzy construct due to the blanket use of the term throughout the literature and its entanglement with ethnocentric concepts of assimilation and “Americanization.” Furthermore, critics point out that the focus on acculturation as the main explanatory variable for decline in Latino health obfuscates the role of biological determinants of health, as well as mezzo-level (family, community) and macro-level (policy) systems that also contribute to health outcomes (Chun & Akutsu, 2003; Lopez-Class et al., 2011; Weigers & Sherraden, 2001; Zsembik & Fennell, 2005). Given such multilevel complexity, the construct of acculturation is starting to be conceptualized and operationalized in more nuanced ways. For example, Lopez-Class and colleagues (2011) advocate using an ecodevelopmental framework for studying acculturation and health to better capture the influence of contextual factors such as ethnic enclave and neighborhood characteristics, family and social networks, ethnic identity and language use, and so forth; and recommend studying acculturation longitudinally. Padilla and Perez (2003) similarly advocate focusing on social and environmental constraints on individual acculturation motivations and choices, especially when powerful majority groups dominate and stigmatize dissimilar minority groups who are then challenged to cope with stigma in different ways that influence their acculturation (e.g., toward or away from mainstream society).
Measurement
Although there are now many multidimensional scales, as well as scales that measure level of acculturative stress (see, Rudmin, 2009 or Thomson & Hoffman-Goetz, 2009 for comprehensive reviews), there is no widely accepted scale or construct. A majority of scales, particularly in large-scale epidemiological studies, reinforce the most simplistic behavioral model of acculturation at the expense of larger structural (Escobar & Vega, 2000) or ecodevelopmental (Lopez-Class et al., 2011) factors affecting health. To this end, there are a growing number of critiques of the use of simplistic models and measures of acculturation (Abraido-Lanza et al., 2006; Escobar & Vega, 2000; Hunt et al., 2004; Lara et al., 2004; Rudmin, 2003; Thomson & Hoffman-Goetz, 2009; Ward, 2008; Weigers & Sherraden, 2001). Increasing calls for a more complex conceptualization of acculturation has led to the development of bidimensional scales (see for example, Cuellar, Arnold, & Maldonado, 1995; Marín & Gamba, 1996) that assess Latino and Anglo-American culture separately.
Rudmin (2009) conducted an exhaustive review of the acculturation literature and has critiqued the proliferation of universal acculturation scales, which have shown poor convergent and divergent validity and poor reliability. Rudmin attributes this “chronic proliferation” (p. 110) of acculturation scales to poor citation of previous work due to the isolation of literatures across disciplines. Rudmin (2009) has critiqued repeated attempts by researchers to capture acculturative processes via “new” universal scales. He instead proposes the use of bilineal acculturation scales to inquire about specific components of the culture in question and thus allow for assessment of orientation to both minority and dominant (or other) cultures (i.e., biculturalism). He further suggests that more thorough reviews of the existing literature by researchers will reduce the unnecessary proliferation of unipolar, bipolar, or ipsative acculturation scales.
But what are we actually measuring? One issue with proxy variables such as English language proficiency is that the process of learning a language is more linear than acculturation (Rumbaut, 1997a). In a major review of the literature on Latino acculturation and health, Lara et al. (2004) found that, depending on the measure used, acculturation can have a positive, negative, or neutral relation to health outcomes. Furthermore, despite reviewing a range of health studies from diabetes, asthma, and heart disease to mental health, Lara et al. were only able to make conclusive statements about the role of acculturation on substance use, dietary patterns, and infant birth weight, because of the general lack of methodological uniformity across studies reviewed. Escobar and Vega (2000) assert that proxy variables such as language use have a valid place in large-scale epidemiological studies because they continue to explain the majority of variance in health outcome variables, even when multidimensional measures of acculturation (i.e., that include attitudes or cultural orientation) are included. This latter point is overlooked by critics of proxy indices. However, proxies still reinforce simplistic conceptualizations of acculturation as an inevitably negative process for Mexican immigrants, and with little explanation as to why.
Thus while language proficiency or time in the United States remain strong predictors of health, their use as acculturation proxies begs the question what exactly do these proxy variables represent in their relations to health and mental health outcomes? Some critics have even proposed that use of acculturation as a variable should be discontinued until a more holistic model can be developed (Hunt et al., 2004), while others (e.g., Escobar & Vega, 2000) recommend the continued use of language, country of origin, and so forth, but as variables in their own right, rather than representatives of the acculturative process. Furthermore, quantifying level of acculturation has mostly reinforced a simplistic causal relationship between acculturation and declining health outcomes (Weigers & Sherraden, 2001), and hence the need for behavioral interventions targeting individuals. Critics like Rudmin (2009) advocate studying acculturation in its own right apart from health outcomes.
Limitations of Acculturation in Explaining the Mexican Health Paradox
The oversimplification of acculturation in relation to health outcomes is problematic on at least two levels. First, it points health and mental health interventions in the direction of a simple cause-and-effect relationship between acculturation and behavior change, rather than also targeting the broader sociopolitical or ecodevelopmental context and social determinants of health and mental health outcomes. Second, the descriptive nature of large-scale epidemiological studies raises the larger question regarding what processes are being tapped by single variable proxy measures. That is, might acculturation itself be a proxy for larger processes affecting health outcomes (Betancourt & Lopez, 1993)? Understanding the environmental context of health is necessary to appreciate the combination of factors that contribute to the paradox and its subsequent decline (Alegria, 2009).
While several theories have been proposed to explain the MHP, namely, the salmon bias (i.e., elderly or infirm immigrants returning to Mexico to die), the healthy immigrant effect (selective migration pursued by the most vigorous immigrants), and faulty census data (misclassification of Hispanics as non-Hispanic), none of these have been supported by data and research (Morales et al., 2002). While the cultural buffer hypothesis has been shown to have some validity in relation to protective health effects (see for example, Hovey, 2000), a deeper examination of the literature suggests complex processes affecting health declines, not accounted for by acculturation as a direct causal mechanism in-and-of itself. An expanded view of the context of acculturation can enhance the explanatory power of acculturation as a construct in relationship to health outcomes.
Enhancing the Explanatory Power of Acculturation With Regard to the Mexican Health Paradox
The construct of acculturation is appealing to researchers because it seems to neatly explain that the erosion of protective cultural factors leads to the dissipation of the health paradox. The epidemiological evidence reinforces a simple acculturation model wherein greater acculturation to negative aspects of U.S. society causes erosion of protective factors such as familism and religiosity, and increased unhealthy behaviors which, in turn, explain declining health outcomes (Weigers & Sherraden, 2001). However, if the process of acculturation is as clear cut as it appears in large-scale studies, why does the relation appear to hold primarily for Mexicans rather than other U.S. Latino groups? That is, if protective Latino cultural values and norms are generally practiced across all major U.S. Latino groups, why don’t they seem to be buffered as well (e.g., Puerto Ricans)? Acculturation as a simple behavioral model from “Latino” to “U.S.” culture clearly cannot explain such inter-Latino differences yet the majority of public health studies point to it as the explanation of health declines (Cook, Alegria, Lin, & Guo, 2009; Hunt et al., 2004; Lara et al., 2004).
We believe that the explanatory power of acculturation can be enhanced by integrating several current acculturation-related theoretical perspectives and critiques, beginning with our own refinement and expansion of John Berry’s influential model. While Berry’s model has come under criticism for being more conceptual than empirical (Rudmin, 2003), and for underemphasizing the influence of individual and local contextual factors (Lopez-Class et al., 2011; Padilla & Perez, 2003), it remains a helpful heuristic for understanding Mexican versus other Latino adjustment in the United States, as described below.
Refinement of Berry’s Model of Acculturation
The relevance of Berry’s theory of acculturation to understanding U.S. Latinos is that it primarily focuses on indigenous and other racial and ethnic minority groups in North America and their historical experience with European colonial powers. As such, Berry notes that while in theory two groups in continuous contact can influence each other, in reality a larger and more powerful group typically dominates a smaller and less powerful group, and thus wields more power to influence and even oppress the nondominant group. Such dynamics set the stage for an acculturation process that is resistant, stressful, and conflictual for minority groups such as non-White minority groups in the United States. While critics of acculturation research (e.g., Rudmin, 2003) note the almost exclusive focus on minority rather than majority groups, such a focus is intended to study the negative side of SES and health disparities in the United States.
How stressful acculturation may be or not be depends on its historical course. Berry views the course of acculturation as a three-phase process characterized by (1) contact; (2) conflict; and (3) adaptation. Contact refers to the conditions under which two cultural groups meet (e.g., invasion, immigration, seeking refuge, etc.). Conflict refers to the predictable tension and fighting that results when one group attempts to dominate another, and adaptation refers to the eventual form of accommodation between groups that is intended to reduce conflict. While it is possible for little conflict to occur, the frequent dynamics of dominance and subordination make conflict a probable and often protracted phase of acculturation (e.g., non-White minority groups in the United States).
Which form of adaptation an ethnic minority group eventually experiences depends on the original conditions of contact, the degree of conflict between groups, and the dominant society’s tolerance for ethnic and racial diversity. Such factors influence the degree to which the nondominant group attempts to maintain or reinvent its culture of origin, and the degree to which positive relations between groups is possible. According to Berry, the four major forms of adaptation can be described by listing all possible combinations of yes/no answers to the following two questions: (1) Does the minority group attempt to retain its culture of origin, and (2) are positive relations possible between the minority and majority groups? (see Table 1)
Varieties of Adaptation to Acculturation for U.S. Minority Groups.
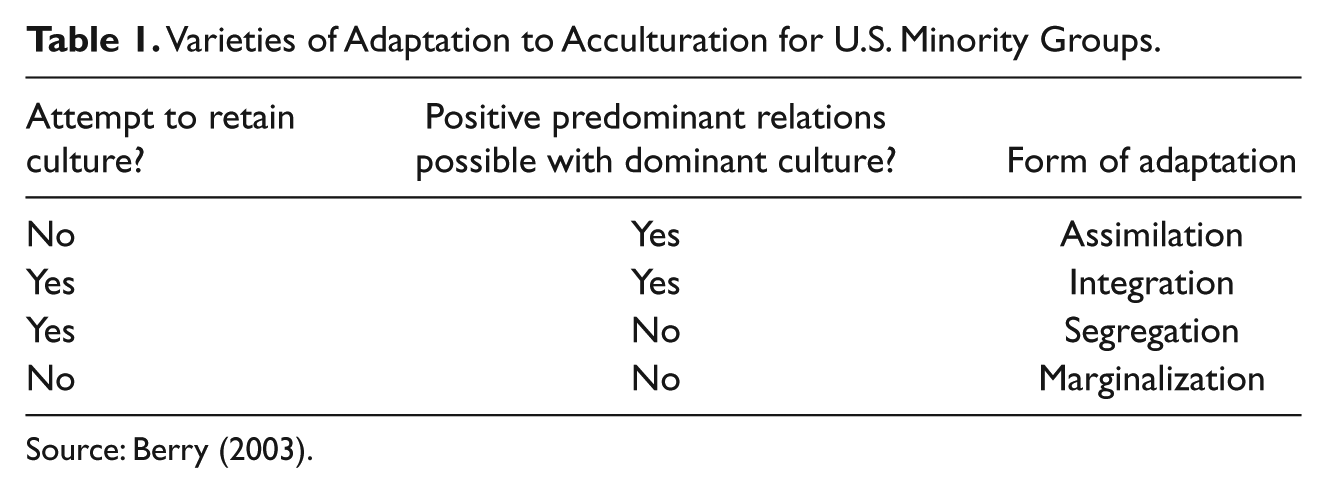
Source: Berry (2003).
For example, while indigenous in small numbers to what is now the southwestern United States, the historical course of acculturation for Mexican Americans has primarily involved voluntary immigration followed by domination, forced segregation and multiple forms of discrimination by the majority culture, as well as fairly high retention of Mexican culture. That Mexican culture is frequently replenished by regular immigration from Mexico is a factor not fully considered in Berry’s model. The slow historical pace of Mexican American adaptation from segregation to integration, a function of minority-majority relations, and frequent immigration flows from Mexico, is also not depicted in Table 1. Still, Berry’s fourfold model provides a basic understanding of how stressful acculturation can be for different U.S. minority groups. Indeed, these four forms of adaptation can be viewed as an acculturative stress gradient in which scenarios of assimilation and integration have been far less stressful forms of adaptation to American society than segregation and certainly marginalization. Such a preliminary conceptualization of acculturative stress can serve as a starting point for understanding a minority group’s level of social stratification as reflected in disparities in SES, health, and so forth.
Berry’s fourfold model has been criticized for its lack of predictive validity with regard to minority adjustment. For example, in a review of correlations between Berry’s four types of adaptation and various indices minority adjustment, taken from 18 of Berry’s Canada-based studies, Rudmin (2003) found that two-thirds of the correlations were nonsignificant, including 28 of 30 between integration and adjustment, a bicultural form of adaptation that Berry and many others view as optimal. Rudmin did find significant correlations between segregation and distress, for minorities with little economic and political power, as well as between marginality and stress. Thus while Rudmin’s review provides only partial support for Berry’s four-fold model, it seems premature to dismiss the model based on this preliminary review. That is, the 18 studies reviewed included very different acculturating minority groups (e.g., Korean, French, Portuguese, various Amerindian groups) and scenarios, and were typically small in sample size (i.e., which ranged from 31 to 150 with an average of 61 participants per study). Furthermore, while such quantitative critiques are useful, a historical and sociological analysis of majority-minority ethnic and race relations in Canada or the United States represents an alternative way of describing predominant forms of acculturation and adjustment.
For example, Organista (2007a) has conducted a historical analysis of major U.S. Latino groups, emphasizing what he considers a generally inverse relation between degree of acculturative stress and adjustment at the population level. Table 2 illustrates the varying historical courses of acculturation for major U.S. Latino populations and varying consequent levels of acculturative stress and adjustment. By expanding the logic of Berry’s three course model of acculturation, Organista’s framework deepens our understanding of why some Latino groups fare worse than others, despite sharing common cultural values and practices. For example, Puerto Ricans generally fare worse on most indicators of adjustment (SES, health, etc.) while Cuban Americans generally fare the best, with Mexican Americans in the middle given their broader variance in acculturation.
Relation Between Acculturation, Degree of Acculturative Stress, and General Level of Adjustment for Major U.S. Latino Groups.

Note: Plus signs signify progression from one predominant form of adjustment to another.
The historical course of acculturation for U.S. Latinos is consistent with their SES, psychosocial and health disparities. For example, Puerto Ricans have experienced a “double legacy of conquest and colonization” followed by racialized discrimination and hypersegregation alongside African Americans in the United States. (Organista, 2007a; p. 21). In contrast, the first wave of predominantly elite, professional, and White Cubans that fled the new Castro regime benefited from a generous open-door refugee policy replete with plentiful programs that maximized their adaptation to United States. Subsequent waves of similarly upper and middle professional class Cubans, most relatives of first wave, experienced the same reception, through the 1960s and 1970s, further consolidated a thriving ethnic enclave in South Florida. While a small wave of poorer and darker Cubans, called “Marielitos” because they sailed from the Cuban Port of Mariel, did receive a harsh reception during the 1980s (i.e., military detention centers, “tent city” encampments and deportations), the majority did eventually receive refugees status and were quickly absorbed into the Miami’s vibrant ethnic enclave (Garcia, 1996).
Thus no health paradox has been documented for Cubans given their initially high social capital, rapid integration and assimilation into U.S. society, and economically successful ethnic enclave. Nor is the paradox in evidence for Puerto Ricans whose historical experience of invasion and colonization in their country of origin, followed by dominance and subordination in the United States, has blurred the distinction of experiences in both locations (i.e., considerable acculturation stress following initial contact with American society followed by protracted conflict through adaptation in both Puerto Rico and the United States.). Furthermore, their status as U.S. citizens has led to much revolving door migration between Puerto Rico and the East Coast, further blurring any clear immigration experience. Hence, the rather profound differences in the acculturation histories of U.S. Latinos comprise the basis of different trajectories of adjustment rooted in varying levels of acculturative stress.
Acculturative stress
Berry and Annis (1974) originally defined acculturative stress as collective confusion and anxiety, loss of identity, feelings of alienation, and striking out against larger society. More specifically, acculturative stress refers to behaviors and experiences generated during acculturation that are pathological and disruptive to the individual and ethnic group (e.g., deviant behavior, psychosomatic symptoms, and feelings of marginality). As noted above, we would extend this early definition to include population-level disparities in SES and health that accrue over decades and even centuries of conflictual minority-majority relations.
According to Berry (2003), acculturative stress will be highest when the cultural and behavioral similarity between two groups in contact is lowest, and where pressure is placed upon the minority group to acculturate due to the dominant group’s low tolerance for racial and cultural diversity. For example, Native Americans and African Americans would rank highest in terms of acculturative stress given their low cultural (and we would add racial) similarity to Anglo Americans, and the tremendous historical pressure placed upon these involuntary Americans to relinquish their cultures of origin. Such pressure has been especially stressful considering that the original contact experiences of these two groups involved invasion and forced relocation, respectively, followed by policies of rejection and segregation from mainstream society (e.g., reservations for Native Americans and enslavement followed by legal segregation for African Americans). In contrast, European immigrants have historically experienced lower acculturative stress, relative to people of color, given their higher cultural and racial similarity to the dominant group and because the pressure to acculturate has been mitigated by their voluntary immigration, and the option to assimilate.
Interestingly, Rudmin (2009) considers acculturative stress to be confounded with acculturation, and too flawed a construct to be useful because it ignores the demonstrable role of discrimination and SES on health outcomes. However, as conceptualized above, acculturative stress is not separate from but a characteristic of acculturation that varies in degree depending on the course of acculturation for different minority groups. Thus rather than simply control for discrimination and SES in acculturative stress research, as recommended by Rudmin (2003), such characteristics of acculturation should be teased out and analyzed as potential pathways driving the relation between acculturation and health outcomes.
For example, Cook et al., (2009) used data from the National Latino and Asian American Study (NLAAS) to examine potential pathways by which time in the United States relates to differences in the predicted probability of past year psychiatric disorders among immigrant and U.S. born Latinos. By adjusting for different combinations of covariates, Cook et al. examined six potential pathways by which time in the United States might predict mental disorders: perceived discrimination, family cultural conflict, economic dissatisfaction, ethnic identity, U.S. standing (i.e., perception of own group relative to others ), and neighborhood safety. Findings revealed that increased time in the United States was associated with higher risk for immigrant Latinos (i.e., the paradox), that rates of psychiatric disorders between immigrant and U.S. Latinos disappeared when covariates were adjusted, but most importantly that perceived discrimination and family cultural conflict were the two significant pathways in the relation between time in the United States and risk for mental disorders.
Ideally, Cook et al. (2009) would have conducted the above analysis separately for each Latino group within the NLAAS, given their different courses of acculturation discussed above (see Table 2), but not enough power was available for such analyses. Thus certain questions arise: how can Cook et al. talk about an “immigrant paradox” when Puerto Ricans are not immigrants, and Cubans hail from a refugee community? Might Mexicans in the sample be driving the results? Still, this study is one of the very first to examine contextual factors of acculturation in relation to mental health outcomes for Latinos. Castro and colleagues (2009) similarly approach Latino acculturation and health research by studying relations between different trajectories of acculturation informed by segmented assimilation theory.
Segmented assimilation theory
Segmented assimilation theory is a recent variant of acculturation theory that focuses on the new (i.e., post-1965) immigration to the United States, and the process by which the new second generation (i.e., children of contemporary immigrants) become incorporated into the American stratification system with various outcomes (Portes & Zhou, 1993; Zhou, 1997). Segmented assimilation has gained appeal over the past 20 years because of its relevance to contemporary immigrants in the United States, and for its emphasis on the interaction between individual (e.g., social capital) and contextual (e.g., discrimination, immigration policies, ethnic enclave characteristics, etc.) factors in determining “downward” or “upward” assimilation into different segments of the U.S. stratification system (Portes & Zhou, 1993). According to Portes and Zhou (1993), there are three main pathways of assimilation: “traditional” upward assimilation into the White middle-class segment of society (as with the first wave of European immigration), downward assimilation into the “underclass” segment (especially impoverished low SES racial and ethnic minority groups), or an intermediate path towards biculturalism, in which immigrants may achieve economic advancement, while still preserving their cultural heritage (equivalent to Berry’s integration strategy). Thus segmented assimilation theory would attribute behavior changes, such increased alcohol and substance use or poor diet, to a combination of individual markers of acculturative stress and downward assimilation into impoverished communities where, for example, fast food is cheap, ubiquitous, and too often beats out healthier foods (Finch, Lim, Perez, & Do, 2007; Portes & Zhou, 1993).
Interestingly, Portes & Zhou (1993) document that Mexican immigrants do not generally assimilate as far downward as the so-called underclass. While some Mexican American subgroups do appear to assimilate to the underclass, more information is needed regarding which structural and individual factors promote or prevent such movement. For example, in a comparative ethnographic account of low-SES Mexican American adolescents, those who were biculturally oriented were able to take advantage of educational opportunities toward upward mobility, while those who did not speak Spanish and eschewed both Mexican and American cultures (i.e., marginality) showed a downward trend (high dropout rates, higher rates of maladaptive behaviors such as drinking).
Castro and colleagues (2009) applied segmented assimilation theory to a quality of life study using a sample of 140 Mexican American, 85 non-Hispanic white, and 33 men of other backgrounds from the Phoenix metropolitan area. These men were categorized into four distinct segmented assimilation groups: Extreme “upward” and “downward” (Types 1 & 2), and moderate upward and downward (Types 3 & 4). The men were categorized retrospectively by assessing their cultural and economic integration into mainstream society at four different milestone periods of their lives: elementary school years, middle school years, high school years, and adulthood. Results revealed that the extreme upward assimilation group (Type 1) reported higher life satisfaction than the moderate downward group (Type 4), and lower consumption of unhealthy foods as compared to the extreme downward and moderate upward groups (Types 2 & 3). Castro et al. (2009) claimed partial support for segmented assimilation theory, and concluded that early development of human and social capital, especially during the transition from high school into adulthood, is important for upward assimilation and positive health outcomes. While this is a key study in terms of empirically modeling divergent assimilation trajectories related to health and wellbeing, as with the Cook et al. study, the following question arises: Why combine Latinos and non-Hispanic whites in the analyses when it could be argued that the latter are not experiencing acculturation but social mobility while the former are experiencing both?
Consistent with segmented assimilation theory, Latino health and mental health researchers have begun to call for increased attention to individual, familial, community, SES and political-level factors that may converge and impinge on Latino health outcomes over time (Castro, Marsiglia, Kulis, & Kellison, 2010; Castro et al., 2009; Finch et al., 2007; Hunt et al., 2004; Lara et al., 2004; Padilla & Perez, 2003). Specific recommendations include utilizing qualitative methodologies to gain an emic perspective of the acculturative experience; accounting for covariates in statistical models that may have an additive or multiplicative relationship with acculturation (e.g., SES, stigma and discrimination, residence in an ethnic enclave, or social capital); and longitudinal study designs to better understand causal pathways between acculturative factors, including social mobility, and health outcomes over time.
With the above review in mind, we review below key studies supportive of the MHP in the areas of mental health, and birth outcomes of Mexican immigrant women. We also review key studies pertaining to diabetes, an area of research far less clear about the role of acculturation, and with implications for further research and theory.
Applying the Enhanced Construct of Acculturation to the Mexican Paradox Literature
Mental Health and Acculturation
The MHP is strongly supported by major mental health research (Alderete et al., 2000; Alegria et al., 2007, 2008; Vega et al., 1998), especially in mental disorders with rates more sensitive to stress (i.e., depression and anxiety disorders, alcohol and substance use disorders) than disorders with more stable prevalence (e.g., schizophrenia).
The Mexican American Prevalence and Services Survey (MAPSS) conducted by Vega et al. (1998) provides one of the most compelling demonstration of the MHP. These researchers surveyed lifetime prevalence of psychiatric disorders in a stratified random sample of 3,012 adults of Mexican background in Fresno County, California. This population based sample was divided into short-term (less than 13 years) and long-term (13 years or longer in U.S.) immigrants, and U.S. born Mexican Americans. Results revealed a dramatic pattern of positive relations between increasing time in the United States and lifetime prevalence when comparing short-term, long-term immigrants, and U.S. born Mexican Americans for any mental disorder (18.4%, 32.3%, & 48.7%, respectively), any abuse/substance use disorder (9.7%, 14.3%, & 29.3%, respectively), any anxiety disorder (7.6%, 17.1%, & 24.1%, respectively), and any affective disorder (5.9%, 10.8%, & 18.5%, respectively).
However, to better understand the MHP, MAPSS findings were also compared to the National Comorbidity Survey (NCS), and a Mexico City prevalence survey. The NCS was the first national probability survey of mental disorders to contain a representative sample of Latinos, but only English speaking (i.e., more acculturated). The Mexico City survey allowed for a comparison of the mental health profiles of Mexican immigrants in the United States with their counterparts in Mexico in order check for any differences due to immigrant selection bias (i.e., immigrants healthier than nonmigrant counterparts). Comparisons revealed comparable lifetime prevalence rates between U.S. born Mexican Americans, and rates for NCS general U.S. population and English speaking Latinos (i.e., about 50% lifetime prevalence for any disorder assessed). In contrast, the lifetime prevalence rate for any disorder for immigrants in the MAPSS was half the rate of U.S. born Mexican Americans, and comparable to the prevalence rate in the Mexico City survey (25.4, 48.7 & 23.4, respectively). Vega et al. concluded that their results support the MHP but not because of the selective migration hypothesis given the comparable prevalence rates for Mexican immigrants in the MAPSS and their Mexico City counterparts. While this study did rely on time in the United States as the proxy index of acculturation, it examined a countywide representative sample, compared three distinct time periods, and compared data with both national U.S. and Mexico City data in order to better attribute the declining mental health of Mexican Americans to the stressful effects of acculturation experienced at the population level.
While unusually rigorous, the MAPSS still leaves us to study, more in-depth, which aspects of acculturative stress are related to poor mental health outcomes. Such research will likely tap contradictory nuances at the individual level. For example, in their study of sociopsychological predictors of acculturative stress, Miranda & Matheny (2000) found that first generation immigrants face more acculturative stress than their second-generation counterparts who are more likely to grow up speaking English and thus can navigate society more easily. This finding is interesting because mental health outcomes are worse in second generation and English-speaking Mexican Americans as noted above. Thus additional aspects of acculturation, such as the role of ethnic identity development and segmented assimilation, suggest that each generation is likely to face different types and degrees of stress in need of closer investigation (Caplan, 2007).
In light of Cook et al.’s (2009) findings on the role of perceived discrimination in predicting poor mental health outcomes, recent interest in colorism and the role of phenotyping may shed additional light on the perceived discrimination as a moderating factor in the relationship between acculturation and health. The construct of phenotyping and the role of skin color on mental health among Latinos add a dimension largely ignored in the Latino paradox/acculturation literature. For example, Montalvo & Codina (2001) review a variety of studies highlighting the relationship between level of acculturation, phenotype, and life chances. In general, the authors found that lighter skin Mexican immigrants were more likely to rise up the socioeconomic ladder and live outside ethnic barrio enclaves, while darker skinned Mexican Americans were more likely to remain poor and have lower self-esteem. Interestingly, their review also found evidence of an inverse relationship between acculturation and likelihood of self-identifying as “brown.” This trend suggests that time in the United States is likely to be associated with discrimination and increased feelings of “otherness” due to skin color and indigenous features.
As noted by Padilla & Perez (2003), experiences of stigma and discrimination influence acculturation-related choices at the individual level (i.e., how ethnocentric to be, or how much to attempt or integrate or assimilate outside of one’s group). For example, in a qualitative study of the integration experience of first and second generation Mexican immigrant women, Viruell-Fuentes (2007) found that second generation women were more likely to describe experiences of discrimination and stigmatization (also called “othering”) than their first-generation counterparts. These second generation women, who from childhood had more interaction with mainstream society (outside the ethnic enclaves of their first-generation counterparts) described feeling like outsiders, and struggling to know where they “fit in.” As the author concludes, the second generation’s experience of social exclusion, consistent with a segmented assimilation framework, suggests that “‘othering’ processes and discrimination [are] potential pathways through which ‘becoming American’ might erode the health of immigrants and their descendants” (p. 1,525).
The above studies underscore how social contextual and interpersonal factors may be implicated and interrelated, and raise questions regarding how generational status, ethnic identity, phenotyping, perceived discrimination, and family cultural conflict interrelate and may differentially affect mental health and other health outcomes for Mexican Americans adjusting to American society.
Infant Birth Outcomes and Acculturation
Perhaps the most robust support for the MHP comes from research on infant birth outcomes in California. Guendelman and colleagues (Guendelman, 1995; Guendelman & English, 1995; Guendelman et al., 1990; Guendelman, Thornton, Gould, & Hosang, 2006), among others (see, Acevedo-Garcia, Soobader, & Berkman, 2007; Bender & Castro, 2000; Campos et al., 2008; Harley & Eskenazi, 2006; Johnson & Marchi, 2009; Magana & Clark, 1995; Padilla, Boardman, Hummer, & Espitia, 2002; Scribner & Dwyer, 1989; Sherraden & Barrera, 1997; Weigers & Sherraden, 2001) have repeatedly found favorable birth outcomes (i.e., healthy birth weight) in first generation Mexican immigrants that disappear by the second generation. In fact, Guendelman and English (1995) found an increase in low-birth weight and preterm deliveries among Mexican women after just five years of residence in the United States. The authors attribute this increase in unfavorable pregnancy outcomes over time to an increased risk profile among Mexican immigrant that includes higher rates of risky health behaviors such as drinking, smoking and drug use during pregnancy. Longer term residents were also more likely to work in physically strenuous, low-paying jobs throughout pregnancy such as cleaning houses or factory work, potentially increasing their exposure to toxins during activity.
Expanding on the above findings, a review by Rumbaut (1997a) found the following main differences between first and second generation Mexican origin women, with U.S.-born women tending to have in common the following characteristics with U.S.-born Anglo women: worse dietary patterns (higher fat consumption, reduced fiber & fresh produce consumption), increased likelihood for smoking and drinking during pregnancy, and less reported familial support.
Several studies have shed light on components of acculturation affecting birth outcomes. Sherraden & Barrera (1997) applied segmented assimilation theory to the birth outcomes of 41 second generation Mexican American women in Chicago and found that high levels family/social support was more strongly associated with positive birth outcomes and upward assimilation than were maladaptive health behaviors such as smoking and drinking and poor diet. Interestingly, high support families were more likely to visit Mexico and send their daughters there to stay with relatives for vacations. In comparison, women with low family support and poorer birth outcomes knew little to nothing about their parents’ Mexican heritage (i.e., where they were from in Mexico, etc.). These findings suggest that a strong sense of ethnic identity/heritage within a cohesive family unit has an important role in birth outcomes and merit further study.
A study by Johnson & Marchi (2009) found that neighborhood was related to maternal stress and infant birth weight, with English-speaking Mexican women living in ethnic enclaves likely to report higher levels of stress than those living in diverse or white neighborhoods. Although counterintuitive to what the authors had hypothesized based on segmented assimilation theory, the role of discrimination and racism within Latino groups adds yet another dimension to the experience of acculturation. Likely interrelated with issues of phenotyping and ethnic-identity development, Latinos who do not speak Spanish but live in ethnic enclaves may not feel fully accepted by their more Mexican-oriented counterparts. Surprisingly, the authors found a four-fold increase in low-infant-birth weight among English-speaking Mexican women living in ethnic-enclaves versus English-speakers in other neighborhoods (racially/ethnically diverse). This finding is consistent with Berry’s conception of marginality, and helps to fill in some of the details of this form of adaptation that may be related to poor health outcomes.
Type 2 Diabetes and Acculturation
Obesity and Type 2 diabetes Mellitus (DM2) are particularly interesting health problems to explore in light of the current state of acculturation theory. Among Mexican Americans, the risk of diagnosed diabetes is 87% higher than for non-Hispanic Whites, and is 66% higher among Latinos in general (National Diabetes Fact Sheet, 2011). Latinos generally suffer more complications and DM2-related amputations and deaths than non-Hispanic Whites, and rates of diabetes are higher among Mexican Americans and Puerto Ricans as compared to non-Hispanic Whites and Cuban Americans (Organista, 2007b). However, the role of acculturation in the DM2 epidemic is not well understood, partly due to the tendency to group all Latinos together, or to use proxy measures of acculturation across studies (Antecol & Bedard, 2006; Abraído-Lanza, Chao, & Flórez, 2005).
Conflicting findings about behavior change over time underscore the complex determinants of diabetic health outcomes among Mexican Americans. For example, Mexican American dietary change with increased length of residency in the United States has been the source of much research interest, but studies have shown inconsistent results in regards to explaining rising obesity trends among Mexican Americans because dietary changes have been documented as both positive and negative (Abraido-Lanza et al., 2006; Akresh, 2007; Caballero, 2005; Crespo, Smith, Carter-Pokras, & Andersen, 2001; Perez-Escamilla & Putnik, 2007; Schulz et al., 2005; Yeh, Viladrich, Bruning, & Roye, 2009). A literature review by Antecol & Bedard (2006) showed that studies looking at the relationship between acculturation and factors contributing to DM2 (including obesity, diet, alcohol use, etc.) are filled with contradictory results depending on which measure of acculturation was used.
In a dated yet insightful study, Hazuda, Haffner, Stern, & Eifler (1988) used data from the San Antonio Heart Study to measure the role of acculturation and socioeconomic status on obesity and diabetes among Mexican Americans. The study represents one of a few that utilized multiple acculturation indices to help account for the nonlinear process of acculturation and focuses specifically on Mexican Americans (as opposed to all Latinos). The authors found that acculturation was negatively correlated with prevalence of obesity and DM2 in both men and women. That is, less acculturated men and women of low SES showed higher prevalence of DM2 and obesity than their more acculturated and higher SES counterparts.
Interestingly, Hazuda and colleagues (1988) also found that rates of diabetes correlated with Indian heritage (Mexican Americans with darker skin and Indian heritage were also more segregated in lower SES barrios), suggesting a genetic predisposition. Results call into question the relationship between SES, ethnoracial appearance and stress potentially exacerbating genetic predisposition to DM2. While the authors did not explore this relationship, the work of Montalvo & Codina (2001) suggests interactions among these factors that merit further exploration. The results from Hazuda and colleagues’ study seem to contradict the MHP, and raise questions about the complexities of contributing factors to diabetes. Caballero (2005) discusses the role of the following factors among Latino populations: genetic predisposition, social and cultural factors of immigration, level of acculturation, body image, depression, education-level, fears, general level of familial integration and support, and health literacy. Biopsychosocial factors experienced by Latino immigrants may also affect adherence to treatment regimens, and the risk of complications and mortality due to DM2.
Cultural factors may also contribute to lower obesity rates among more acculturated, higher SES Latinos. A qualitative focus-group study by Diaz, Mainous, & Pope (2006) found conflicting views regarding ideal body weight and health as dictated by U.S. culture versus traditional Latino culture. One male interviewee in the Diaz study summarized his experience of cultural conflict: “In the Latin culture, from when you are a child, you hear that being fat is ‘saludable’ [healthy]. That is wrong, but in the culture, if you are not fat, then you are sick. You have to convince the family and the individuals themselves that being fat does not mean you are ‘saludable’” (p. 329). While the research clearly shows that DM2 and obesity is a problem of epidemic proportions among Mexican Americans and Puerto Ricans, our understanding of the epidemic and the specific role of acculturation remains inconclusive due to current limitations of the construct.
Taken together, the above studies underscore the need to enhance the role of social determinants in future of acculturation research on DM2. To this end, Castro and colleagues (2009) have recommended the use of an ecodevelopmental framework for understanding factors contributing to the development of DM2 among Latinos. Specifically, they suggest that traditional systems models which account for contextual factors at multiple levels (e.g., individual-level, family-level, community-level, etc.) should be expanded to include a temporal developmental perspective, wherein key life milestones (e.g., transition to adolescence, adulthood or old age) would better map the ways in which contextual factors interact over the life course to affect the development of DM2. For example, the role of familial dietary norms (often associated with acculturative change) may differentially affect Mexican Americans at different life stages (e.g., during childhood and adolescence versus young adulthood). The authors further suggest that an ecodevelopmental framework that accounts for gender, age, socioeconomic status, acculturation, and other social and cultural factors over time, and at multiple levels (micro, meso, and macro), can help us better understand the development of DM2, and will ultimately allow us to more effectively intervene to prevent DM2 disparities among Latinos and other populations.
Implications for Research and Theory
This article has reviewed and critiqued the current state of acculturation theory as related to the MHP literature. More specifically it suggests ways of refining and enhancing the explanatory power of the construct of acculturation by integrating current theoretical perspectives and critiques, to better understand the multiple pathways or contextual factors affecting mental health, birth outcomes, and Type 2 diabetes/obesity, in Mexican origin people in the United States. There remains considerable need for more integrated analyses of mechanisms and contextual factors surrounding acculturation that lead to the decline of the initially positive health outcomes experienced by Mexican immigrants. The degree of stress related to acculturation is useful for explaining declining health outcomes related to predominant forms of adaptation (i.e., integration, assimilation, marginalization, and segregation) resulting from individual and sociological factors. Segmented assimilation theory, wherein more recent Latino and Asian immigrants’ acculturation experience is shaped by societal and community factors resulting in upward or downward assimilation, and points in between, has also proven helpful for guiding research.
Today’s “fuzzy” state of acculturation theory is related to the difficulty of defining and measuring aspects of culture, let alone cultural change. The fact that many studies still refer to the phenomenon of better health outcomes among Mexican immigrants as the Latino health paradox is symptomatic of a larger issue in the social sciences regarding an oversimplification of what defines ethnic populations and culture. In particular, the emphasis on the role of language as a proxy for acculturation, particularly in large-scale studies, contributes to a simplistic model of adaptation, and for many a false dichotomy of good/traditional Mexican and bad/U.S. cultures. While epidemiological studies are imperative to alert us to population-level trends, it is frequently unclear what the use of proxy measures of acculturation such as language or time in the United States signify. From the literature reviewed above it seems that for Mexican descent people more time in the United States too often means more exposure to poverty, discrimination, and the eroding of protecting factors such as close knit and supportive families, lower levels of drinking and smoking among both men and women.
While operationalization of a multidimensional construct is challenging, without agreement about what more precisely is being studied, results will continue to vary across studies based on the type of measurement used. Rudmin (2003) recommends avoiding universal and developing local scales of acculturation for specific populations and problems, preceded by qualitative research to explore how group members view acculturation and why. The continued use of acculturation as an underdefined and poorly measured explanatory factor reinforces the idea that acculturation is detrimental to Mexican health and well-being in the United States.
Building on the critiques and recommendations reviewed here, we recommend the following to further enhance our understanding of acculturation and its role in the MHP:
As asserted by Rudmin (2003), the proliferation of universal acculturation scales without sufficient attention to prior scholarship does not contribute to a progressive science. Instead, there is need to develop local scales for specific groups and health outcomes, preceded by qualitative research that teaches us how acculturation is experienced by Latinos and others minority group members.
The use of ecodevelopmental and/or other context-driven theoretical models, such as segmented assimilation theory, or the refined and expanded version of Berry’s four-quadrant model described above, provide useful frameworks for examining contextual factors in the relation between acculturation and health and mental health outcomes at the population level.
Acculturation stress should be conceived of as a characteristic of acculturation that varies in degree depending on the course of acculturation for different U.S. ethnic and racial minority groups, rather than simply be discarded as recommended by Rudmin (2009). In fact, historical and sociological analyses of ethnic and race relations in the United States support acculturation stress as inversely related to minority adjustment at the population level. A compelling question posed by Rudmin is how do we differentiate acculturative stress from more general stress? While this question needs to be addressed more fully, we would begin by suggesting that SES, psychosocial and health disparities, rooted in inequality and social injustice represent acculturative stress at the population level. Perhaps when Mexican Americans or other minority groups attain parity with mainstream society in terms of SES and health profiles at the population level, then individual level problems can more easily be attributed to general stress.
Qualitative exploratory and descriptive accounts of acculturative experiences, studied for their own sake rather than in relation to health outcomes, should be pursued. Such explorations should include premigration experiences, neighborhood context such as residence in an ethnic enclave, neighborhood resources, experiences of racism, discrimination, stigma and othering, the role of back-and-forth migration to and from Mexico or transnationalism, family cohesion and breakdown, individual-level psychological acculturation strategies, gender and ethnic identity, among others hold much promise. Padilla and Perez (2003) describe the usefulness of social and cognitive psychology for understanding motivations for psychological acculturation in Latinos and other minority groups often confronted by stigma and discrimination from the dominant culture and society. A broader and deeper approach to research building upon such areas of inquiry would elucidate the rich and dynamic complexities of the acculturative process, historical and current contextual factors that shape it, and the subsequent adaptation and health outcomes of Mexican and other populations experiencing it.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.