
Abstract
We theorized that sociocultural contexts characterized by a form of interdependence that emphasizes mutual obligations, emotional positivity, and readily accessible social support from family may maximize the benefits of social support. This form of interdependence characterizes Latino culture and is captured by the cultural value familism. Eighty-six Latino and non-Latino participants completed measures of familism and perceived social support before taking part in a standardized laboratory stress task that elicits cortisol reactivity. Cortisol reactivity is an indicator of bodily response to stress that is linked to vulnerability to the adverse effects that stress can have on future health. As predicted, results revealed a moderated mediation pattern. Conditional process analysis showed that familism was indirectly linked to cortisol reactivity through perceived social support, and this mediation effect was moderated by sociocultural context; stress buffering effects were only observed in the Latino sample. These novel findings highlight the role of culture and, specifically, familism in Latinos, for maximizing the benefits that social support can have for stress physiology implicated in long-term health outcomes.
It is now well recognized that relationships that are emotionally supportive, close, and embedded within strong social networks are health protective (e.g., Umberson & Montez, 2010). Perceived social support, the perception that one is valued, cared for, loved, and can count on close others in times of distress (Dunkel-Schetter & Bennett, 1990; Wills, 1991), is robustly associated with more favorable coping responses with stressful life events (Harber, Cohen, Lucas, & Baltes, 2007). For this reason, scholars have theorized that the benefits of perceived support should extend to physiological responses that have implications for health, including those experienced in response to acute psychosocial stress. However, studies assessing physiological responses to laboratory stressors have not always found perceived support to be beneficial (e.g., Heinrichs, Baumgartner, Kirschbaum, & Ehlert, 2003; Roy, Steptoe, & Kirschbaum, 1998). One factor that may shape whether perceived support is beneficial, including under conditions of stress, is culture. Sociocultural contexts characterized by a form of interdependence that values mutual obligations, emotional positivity, and readily accessible social support from family may create affordances for the potential benefits of social support (Campos et al., 2008; Campos, Rojas Perez, & Guardino, 2016). This distinctive form of interdependence is prevalent among Latinos (Campos & Kim, 2017). Thus, we hypothesized that the benefits of perceived social support during a standardized acute laboratory stressor would be maximized for Latinos.
Culture and the Benefits of Social Support
Culture is acquired through social learning and reflects historically rooted, group-based solutions to recurring human challenges and opportunities (Heine, 2012; Kitayama, 2002). The creativity that humans have deployed in managing our species’ complex social relationships is evident in the great cultural variation in norms for relationships and for managing emotions (Markus & Kitayama, 1991; Triandis, 1996). At various times and places, emphasis has been placed on seeing the self as intertwined with important others or separated from others (Markus & Kitayama, 1991; Oishi, Diener, Napa Scollon, Biswas-Diener, 2004). Similarly, the emphasis on open emotion-expression or controlled emotion-expression in the service of managing one’s relationships is culturally variable (e.g., Ruby, Falk, Heine, Villa & Silberstein, 2012).
Social support processes are an area of human life that shows substantial cultural variation. In some cultures, open support seeking is considered appropriate, whereas in others it is avoided to prevent burdening or disrupting one’s important relationships (Chentsova-Dutton & Vaughn, 2012; Kim, Sherman, & Taylor, 2008; Taylor, Welch, Kim, & Sherman, 2007). Latino contexts are known to emphasize a form of interdependence that values readily accessible social support, emotional positivity, and mutual obligations among family (Campos et al., 2008; Holloway, Waldrip, & Ickes, 2009; Ruby et al., 2012; Sabogal, Marín, Otero-Sabogal, Marín, & Perez-Stable, 1987; Triandis, Marín, Lisansky, & Betancourt, 1984). This distinctive form of interdependence has been theorized to make it easier for people to perceive, obtain, and benefit from social support (Campos et al., 2008; Campos & Kim, 2017). In line with this thinking, at least two studies have found that Latinos report higher levels of social support than other U.S. comparison groups that included people of European, African, and, in the case of one of the studies, Asian background (e.g., Almeida, Molnar, Kawachi, & Subramanian, 2009; Kaniasty & Norris, 2000).
The results of the few studies that have examined whether social support is linked with indicators of health in Latinos and non-Latinos are mixed. Two studies found that the links between familism, social support, and mental and physical health do not differ among Latinos and non-Latinos (Campos, Ullman, Aguilera, & Dunkel-Schetter, 2014; Corona, Campos, & Chen, 2017). Conversely, two other studies found evidence of moderation such that Latinos benefited more from social support than non-Latino U.S. comparison groups (Campos et al., 2008; Shavitt et al., 2016). Altogether, Latinos appear to either benefit as much or more from social support than non-Latinos. Consistent with theory, this pattern suggests that Latino sociocultural contexts may facilitate psychological and physical health benefits that can be derived from mutually beneficial and supportive family relationships, including under conditions of stress (Calderón-Tena, Knight, & Carlo, 2011; Campos et al., 2008; Campos, Ullman, et al., 2014).
Support from family is a core element of familism, the term that captures a way of valuing family relationships that is particularly salient among Latinos. Familism in Latinos emphasizes close, warm, and supportive family relationships that place family before the self (e.g., Campos et al., 2008; Campos, Ullman, et al., 2014; Sabogal et al., 1987). One’s obligations to family, taking family preferences into account during decision making, and considering family as a primary source of readily accessible social support are key facets of familism (e.g., Sabogal et al., 1987). The importance of family is a human universal but ways of valuing family vary and Latinos typically report higher levels of familism values than counterparts of European, and sometimes, Asian cultural background (e.g., Campos, Ullman, et al., 2014; Sabogal et al., 1987). Moreover, although familism values can be held by people across diverse cultural contexts (Campos et al., 2008; Campos, Ullman, et al., 2014; Schwartz et al., 2010), they do not always co-occur with interdependence and open expression of emotional positivity as they do in U.S. Latino culture. For example, in the sociocultural contexts of European Americans, familism typically co-occurs with independence (Cross & Madson, 1997; Markus & Kitayama, 1991), whereas in the sociocultural contexts of Asians and Asian Americans, familism frequently co-occurs with an emphasis on avoiding support seeking (Kim et al., 2008). In contrast, Latino sociocultural contexts distinctively blend familism, interdependence, and emotional positivity. Thus, we theorized that familism in Latino contexts may maximize the benefits of social support for health-relevant physiological processes.
Stress and Physiological Stress Reactivity
The human body is well prepared to respond to stress. Stress hormones, including cortisol, the end product of the hypothalamus–pituitary–adrenal (HPA) axis, are physiologically protective and behaviorally adaptive; they prepare individuals to respond to challenges and threats in their environments (Dickerson & Kemeny, 2004). In adaptive scenarios, cortisol rises in response to acute stressors. However, chronic stress dysregulates the body’s stress systems and, over time, can lead to stress-related disease (Chrousos & Gold, 1992; McEwen, 2002). When the stress system is dysregulated, cortisol’s rises in response to acute stress may be too high or not occur at all. Social support has been hypothesized to be one potential buffer against damage that leads to chronic dysregulation of the HPA system and, ultimately, to stress-related disease (e.g., Kiecolt-Glaser & Glaser, 1995). Perceived social support, specifically, has been theorized to buffer responses to acute stress (Cohen & Wills, 1985). However, studies examining cortisol reactivity in response to laboratory stressors such as the Trier Social Stress Test (TSST; Kirschbaum, Pirke, & Hellhammer, 1993) have been inconclusive. Perceived support has typically not been associated with stress reactivity in European samples from Germany, England, and Switzerland (Ditzen et al., 2007; Ditzen et al., 2008; Heinrichs et al., 2003; Kirschbaum, Klauer, Filipp, & Hellhammer, 1995; Roy et al., 1998) with the exception of one study of a Swiss sample with hypertension (Wirtz et al., 2007). To date, little evidence indicates that the link of social support with health extends to physiological pathways implicated in health.
Perceived support has rarely been found to buffer physiological responses to laboratory stressors but previous studies have relied on mostly European American or European samples. The role of sociocultural contexts that may facilitate the benefits of support has not been studied. Examining this possibility in Latino contexts, which are theorized to be particularly favorable for social support processes, is important for arriving at a fuller understanding of social support’s potential for buffering physiological processes with important downstream health implications.
The Present Study
Drawing on theorizing that Latino sociocultural contexts create affordances for the potential benefits of social support (Campos et al., 2008), we hypothesized that high levels of familism would predict high levels of perceived social support which, in turn, would predict reduced cortisol responses to a laboratory stressor among U.S. Latinos. Figure 1 shows our conceptual model. Given the mixed pattern reported in previous studies, we also explored whether the hypothesized pattern extended to non-Latinos.
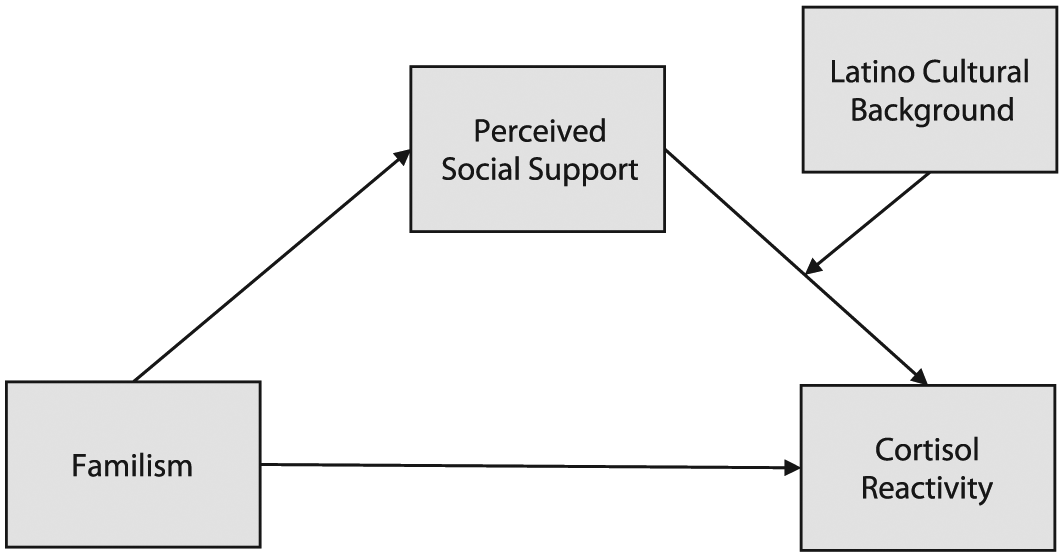
Conceptual moderated mediation model.
Method
Participants
The present research is part of a larger study on culture, relationships, and health (N = 158; Campos, Busse, et al., 2014; all study information can be obtained from B. Campos upon request). Participants included in this study were those who completed the laboratory stressor, had cortisol data available for analyses, 1 and reported a Latino, Asian, or European cultural background. Participants who reported a cultural background that was partly Latino and partly non-Latino were excluded (five participants). The final sample consisted of 86 participants (56 women and 30 men) with a mean age of 20.28 (SD = 1.94; range = 18-26 years). Of these, 51 participants (59 %) self-reported a Latino cultural background (e.g., Mexican, Colombian). The non-Latino group consisted of 35 participants who self-reported an Asian (69%) or European (31%) cultural background. The non-Latino group was selected based on research highlighting Latino and Asian cultural differences (Campos & Kim, 2017; Ruby et al., 2012) as well as previous research on this data set documenting Latino and non-Latino (Asian and European background) differences (Campos, Busse, et al., 2014). Both groups were majority women (Latino = 27 women, 24 men; non-Latino = 29 women, six men). Both groups were also predominantly first generation, defined as born outside of the United States (Latino = 39%; non-Latino = 37%), and second generation, defined as the U.S. born children of at least one foreign-born parent, (Latino = 51%; non-Latino = 34%). Participants were recruited from a large public university and community colleges in Orange County, California, the United States. All participants were free of conditions known to affect stress hormones (e.g., drug or alcohol abuse and major medical conditions).
Procedures
Study sessions always began at 2 p.m. to control for circadian variation in cortisol. Participants were provided with detailed information about the study prior to giving informed consent. After a 6-minute rest period, the first saliva sample was obtained. Next, the TSST was administered and eight additional saliva samples were collected over the course of the subsequent 90 minutes. Self-report questionnaires were completed prior to the 6-minute rest and after the TSST. As compensation for their time, participants received course credit or a modest monetary incentive. Participants were fully debriefed at the end of the study. All study procedures were approved by the University of California, Irvine, institutional review board.
Familism
Familism was assessed with a widely used 14-item scale (Sabogal et al., 1987). This measure consists of three subscales assessing the extent to which family obligation (e.g., “One should help economically with the support of younger brothers and sisters”), support from family (e.g., “When one has problems, one can count on the help of relatives”), and family as referents (e.g., “Much of what a son or daughter does should be done to please parents”) are valued. Participants rated their level of agreement on each item using a Likert-type scale ranging from 1 (very much in disagreement) to 5 (very much in agreement). Recent research indicates that these three facets of familism load onto one factor (Campos, Ullman, et al., 2014); thus, all items were averaged into one overall familism score. Cronbach’s alpha coefficient was .79 for the overall sample (.78 for Latinos; .81 for non-Latinos). Higher scores indicated higher levels of familism.
Perceived social support
The Medical Outcomes Study (MOS) Social Support Survey (Sherbourne & Stewart, 1991) consists of 19 items assessing four types of non–source-specific support: affectionate (expressions of love and affection), emotional/informational (expressions of positive affect and understanding, offering advice and guidance), positive social interaction (availability to do fun things), and tangible (material aid or behavioral assistance). Participants rated the availability of each type of support on a 1 (none of the time) to 5 (all of the time) Likert-type scale. Item responses were averaged for an overall score. Cronbach’s alpha coefficient was .95 for the overall sample and Latinos and non-Latinos separately. Higher scores indicated higher perceived social support.
TSST and salivary cortisol assessment
The TSST (Kirschbaum et al., 1993) is a well-validated laboratory stressor consisting of a 3-minute preparation period, a 5-minute speech task, and a 5-minute mental arithmetic task. It evokes social-evaluative threat with components of uncontrollability and unpredictability that reliably elicit cortisol responses (Dickerson & Kemeny, 2004). The TSST took place in front of two neutral, nonsupportive expert evaluators of diverse cultural backgrounds (e.g., Latino, European, East Asian, mixed background) and male and female genders.
Saliva samples were obtained from each participant using sterile cotton swabs (Salivettes; Sarstedt, Numbrecht, Germany). The first sample was taken 2 minutes prior to the beginning of the TSST and the eight additional samples were taken post-TSST (1 minute, 5 minutes, 10 minutes, 20 minutes, 30 minutes, 45 minutes, 60 minutes, and 90 minutes). Samples were stored at room temperature until the end of each session and then stored at −70°C until assayed. Samples were thawed for biochemical analysis and centrifuged for 10 minutes at 2,000 X g and 4°C. Cortisol in saliva was determined by a commercially available enzyme-linked immunosorbent assay (ELISA, IBL-America, Minneapolis, MN). The assay sensitivity is 0.033 nmol/L and the dynamic range is 0 to 82.77 nmol/L. Inter- and intraassay coefficients of variance are reported at 4.9% and 4.1%, respectively.
A careful read of the literature (e.g., Cohen & Wills, 1985; Nicolson, 2008) guided us to focus on the typical increase experienced in response to the TSST as the most relevant cortisol outcome for understanding potential buffering effects while accounting for the possibility of variation in a diverse group that includes people of non-European background whose HPA axis systems have been little studied (e.g., Nicolson, 2008). Thus, we subtracted the pre-TSST cortisol value from the average of the first five samples following the TSST (1-minute to 30-minute samples) to obtain a single variable reflecting salivary cortisol responses to the TSST for hypothesis testing. This variable, termed mean cortisol increase, indexed cortisol increases to the TSST, a key indicator of an individual’s HPA axis response to a stressor. Mean cortisol increase is highly correlated with other commonly used indices of cortisol reactivity, including the area under the curve (AUC) with reference to ground which is reflective of overall cortisol output in response to the TSST (computed using simple AUC computations from pre- to +90-minute samples; AUCg with mean cortisol increase: r = .61, p < .001) and the maximum cortisol increase experienced by each individual participant in response to the TSST (computed by subtracting the pre-TSST cortisol value from individual peak cortisol values obtained at any time between +1 and +90 minute post-TSST; maximum cortisol increase with mean cortisol increase: r = .95, p < .001). These measures are highly intercorrelated but capture somewhat different aspects of the stress response (Khoury et al., 2015).
Data analytic approach
We expected Latino culture’s distinctive characteristics, captured by familism, to maximize the benefits of perceived social support for cortisol reactivity in Latinos. Thus, we focused on two groups for hypothesis testing: Latinos and non-Latinos of European and Asian background. 2 Cultural background was dummy coded such that Latinos were coded 1 and non-Latinos were coded 0. Conditional process analysis using the PROCESS macro for SPSS was used for hypothesis testing (Hayes, 2013). This approach uses a regression-based analytic framework for estimating direct and indirect effects in a single model, including complex moderated mediation models that test for moderation along a particular mediation path or paths (Hayes, 2013). To evaluate the significance of moderated mediation effects, an index of the approximate size of the moderated mediation effect is generated as a formal test of moderation (Hayes, 2015). Significance is indicated when the bias-corrected 95% confidence intervals (CIs) do not cross zero. PROCESS also allowed us to test alterative possibilities. For example, it was possible that moderation also occurred, or exclusively occurred, along the path from familism to perceived social support rather than the path from perceived social support to cortisol reactivity. All analyses using PROCESS were conducted with 5,000 bootstrap samples.
Results
Preliminary Analyses
First, the distribution of each predictor variable was examined for outliers and normality among the Latino and non-Latino groups. There were no outliers. Skewness and kurtosis coefficients were less than 1, indicating no problems with normality. Cortisol responses to the TSST were typical and comparable among the Latino and non-Latino groups.
3
Second, the data were examined for cultural background or gender differences on all study variables. ANOVAs (2 × 2) did not provide any evidence of significant differences by cultural background, gender, nor their interaction for familism, perceived support, or mean cortisol increase (all Fs < 2.07, all ps > .16, all
Means, Standard Deviations, and Intercorrelation Matrices by Latino and Non-Latino Cultural Background.
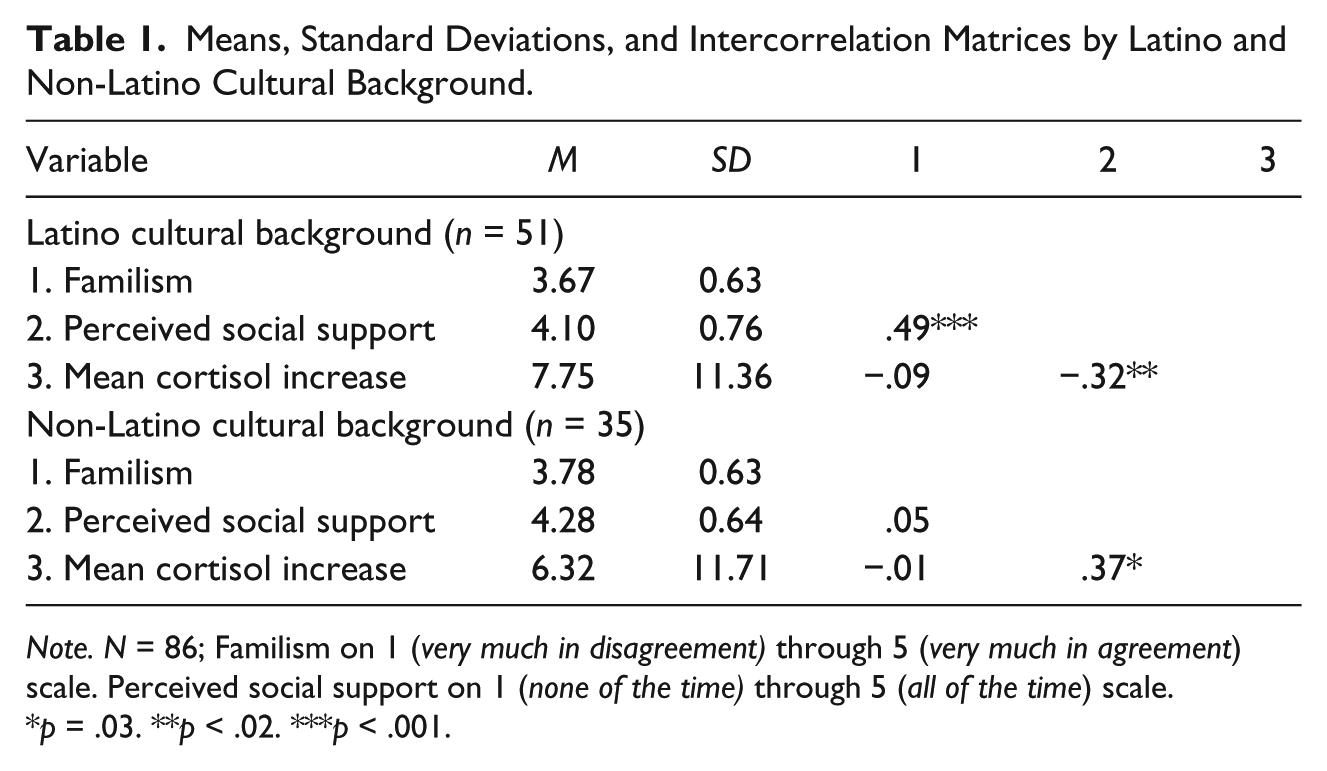
Note. N = 86; Familism on 1 (very much in disagreement) through 5 (very much in agreement) scale. Perceived social support on 1 (none of the time) through 5 (all of the time) scale.
p = .03. **p < .02. ***p < .001.
Hypothesis Testing
The full moderated mediation model with familism, perceived support, cultural background, and the interaction of perceived support and cultural background at the pathway from support to cortisol reactivity (Figure 1) explained 12% of the variance in mean cortisol increase, F(4, 81) = 2.79, p = .03. As Table 2 shows, familism directly predicted perceived social support, perceived social support directly predicted mean cortisol increase, and cultural background predicted mean cortisol increase. The interaction of perceived support and cultural background also predicted mean cortisol increase. There was no significant direct effect of familism on mean cortisol increase. Importantly, there was a significant indirect effect of familism on mean cortisol increase through perceived social support that was moderated by cultural background at the path from social support to mean cortisol increase. As reported in Table 2, Latino and non-Latino cultural background moderated the path linking perceived social support with mean cortisol increase. Familism indirectly predicted lower mean cortisol increases in response to the TSST through perceived social support among Latinos. For non-Latinos, familism indirectly predicted higher mean cortisol increases through perceived social support. This Latino and non-Latino difference was significant per the index of moderated mediation test, b = −4.48, SE = 2.04, CI = [−9.62, −1.31]. 4
Results for Hypothesized Moderated Mediation Model Predicting Cortisol Reactivity.
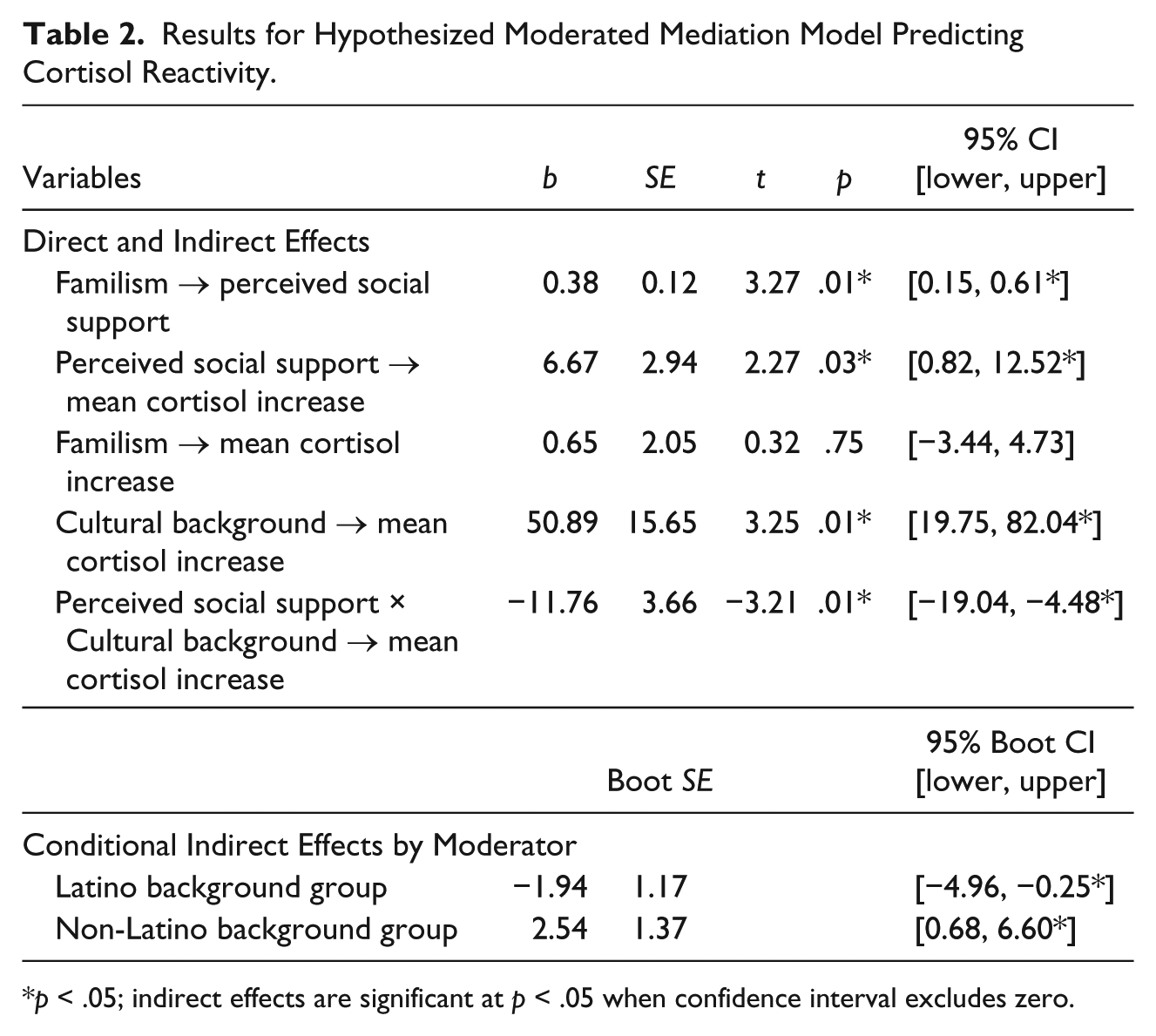
p < .05; indirect effects are significant at p < .05 when confidence interval excludes zero.
Ruling out Alternative Possibilities
The finding that familism indirectly buffered cortisol reactivity in the Latino sample by maximizing the benefits of social support ruled out the possibility that cultural background would only moderate the path from familism to perceived social support. However, it was still possible that cultural background might moderate the path from familism to perceived social support and also the path from perceived social support to mean cortisol increase. Testing for that possibility revealed a pattern similar to the hypothesized model but with key differences. First, the direct effect from familism to perceived social support was not significant in the overall model (b = .05, SE = .18, p = .78, CI = [−.30, .42]). Second, cultural background, separately, and in interaction with familism, did predict perceived social support (bs = −2.15 and .54, SEs = .88 and .23, CIs = [–3.90, −.40] and [.08, 1.00]). Third, the conditional indirect effect was no longer significant for non-Latinos (b = .34, SE = 1.36, CI = [−2.38, 3.26]) and the index of moderated mediation test was no longer significant (b = −3.34, SE = 2.09, CI = [−7.86, .33]).
Discussion
We theorized and found evidence that familism indirectly buffered cortisol responses to an acute laboratory stressor via its association with perceived social support in Latinos. These patterns were not observed in non-Latinos. These findings provide new evidence that perceived support can buffer against the physiological consequences of stress. This has been widely theorized but empirical evidence has been scarce. These findings also provide empirical evidence that familism can be beneficial for physiological processes implicated in health. Familism has long been thought to be relevant for Latino physical health patterns but this possibility has only recently begun to be empirically tested (e.g., Ruiz, Campos, & Garcia, 2016). Finally, these findings provide new evidence of Latino culture’s affordances for the benefits of social support. Altogether, this work advances understanding of factors that can maximize the benefits of social support and highlight the role of Latino culture in these processes.
Research on the cultural value of familism has grown in recent years and much of this work has found evidence of benefits for Latinos and sometimes non-Latinos as well (e.g., Calderón-Tena et al., 2011; Campos et al., 2016; Campos, Ullman, et al., 2014). Our findings indicate that familism contributed to the buffering effect of perceived support for Latinos’ cortisol responses to an acute laboratory stressor. Given the substantial body of work that implicates the HPA axis in stress-related disease (Chrousos & Gold, 1992; McEwen, 2002), our findings suggest that familism values are a cultural factor that may shield Latinos from the wear-and-tear that repeated stress exposure can inflict on the body’s stress-response system. Familism, and perhaps other cultural values, thus point to promising new research directions. Additional study of the role of familism on HPA axis functioning may yield new insights for understanding Latino health, including the better-than-expected health profile of immigrant Latinos (Latino Health Paradox) that worsens with time in the UnitedStates (Markides & Coreil, 1986; Ruiz, Steffen, & Smith, 2013).
Familism contributed to a buffering effect for perceived support on cortisol reactivity in Latinos, but not in non-Latinos. We interpret this pattern as reflecting the distinct way that Latino familism is blended with interdependence and emotional positivity as a socially desirable norm. In contrast, for example, familism in Asian contexts is likely to be complicated by the desire to not burden others with one’s support needs (Taylor et al., 2007). Altogether, this pattern points to the need for future studies that examine familism values within the broader contexts in which these values are personally held. Familism values are core to Latino culture but there is now increasing evidence that these values are also held by members of various other cultural groups (e.g., Campos, Ullman, et al., 2014; Schwartz et al., 2010). The findings of the present research suggest that future studies may find that the effects of familism, including its links to social support, may vary by cultural context in complex ways.
Early research expected familism to have a direct effect on outcomes, including health outcomes, but empirical evidence increasingly paints a more complex picture. Familism values may instead have a direct effect on relationship processes and downstream outcomes of interest. In this study, familism values were directly correlated to perceived support in the Latino sample but not directly correlated with the outcome variable of cortisol reactivity. This pattern of direct and indirect links makes theoretical sense. It is reasonable to expect that contexts that value familism socialize favorable relationships; familism is thus likely to be directly linked to relationship relevant variables such as perceived social support. Given the strong and growing literature on the association of relationships for health, it is also reasonable that familism is indirectly associated with health-relevant outcomes through its links with relationship-relevant variables. As more research explores familism across cultural contexts, the circumstances when familism can help maximize the benefits of social support will be better understood and may include other cultural pathways for harnessing the benefits of family relationships in non-Latino contexts.
Why did the observed buffering effects not extend to non-Latinos, including Asian Americans? We interpret this pattern in terms of the distinct forms of collectivism that characterize Latino and East Asian cultures (Campos & Kim, 2017; Ruby et al., 2012). Whereas Latino Americans report family encouragement of support seeking (Chang, 2015), East Asian American norms emphasize refraining from support seeking to avoid disrupting important relationships (Taylor et al., 2007). This latter approach may render social support a more complicated process from which to derive benefit. For European Americans, personally held familism values are at odds with prevailing norms that emphasize independence from family of origin and this mismatch may reduce the benefits of familism for social support. Put simply, more work on this topic is needed. Research that examines distinct paths to resilience offered by specific sociocultural contexts—including varied collectivist contexts—can add to an increased understanding of cultural variation that matters for health.
An important strength of this work was its diverse sample that differed on cultural factors in theoretically meaningful ways. Much more research in this vein is needed. For example, future studies should examine familism and support in response to naturally occurring stressors as well as examine other types of social support. Received support, for example, can threaten self-efficacy (Bolger & Amarel, 2007) and has been found to be most effective when support givers are perceived to be high in responsiveness (Maisel & Gable, 2009). The potential boundary conditions posed by cultural factors for these patterns are not yet clear. Also, HPA axis dysregulation unfolds with long-term exposure to stressors (McEwen, 2002). Thus, stress responses in diverse samples need to be studied over time and include cultural factors that may modulate physiological processes. This work also had limitations. Our sample was small and few men participated. However, the sample size is typical of research that includes biomarker outcomes and was sufficiently powered to detect hypothesized effects. Given the almost complete lack of cultural diversity in experimental studies of stress reactivity, this unique sample that allowed for the study of comparative effects is a valuable contribution.
Humankind’s many cultures offer multiple distinct paths to social support. Our findings suggest that the benefits of perceived support for stress physiology are maximized in Latino contexts that emphasize familism. This is a key step forward to better understanding cultural variation in social support processes and physiological processes that we hope helps move the field toward a full understanding of the potential of social support under conditions of stress.
Footnotes
Acknowledgements
The authors thank Libier Isas for her contributions to this work. The authors also thank the 2009-2011 members of the UCI Culture, Relationships, and Health laboratory for their assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a Multi-Investigator Faculty Research Grant from the University of California, Irvine to Belinda Campos and Ilona S. Yim.