
Abstract
Individualized short message service (SMS; i.e., text messages) and/or phone calls (PC) in Spanish were examined as an effective interventional approach to increasing daily fruits and vegetables (F&V) and physical activity (PA) among community-dwelling Spanish-speaking Hispanics. Participants were randomized to one of three ordered groups: Control (n = 25), SMS (n = 27), or SMS + PC (n = 26). PA and F&V intake were measured at baseline and 12 weeks later, when acceptability and usefulness were evaluated. Using the Cochran-Armitage test, we found an increasing trend in the proportion of vegetable intake (p = .03) and leisure time PA (p = .004) across the interventions. Most respondents from the SMS and SMS + PC groups approved the modalities and frequency of contact and reported following the advice provided. SMS + PC was the most effective intervention to improve PA and vegetable intake among respondents. These findings support feasibility and acceptability of using remote access platforms, specifically, text and phone-based health communication strategies, with Spanish-speaking participants.
Introduction
Accumulated evidence indicates protective roles of fruit and vegetable (F&V) intake and physical activity (PA) for multiple chronic diseases in the general population. High intakes of F&V protect against cancers and cardiovascular disorders and may prevent weight gain (WHO, 2019). Moreover, PA confers protection against some cancers, cardiovascular diseases (CVD), and type II diabetes (T2DM) and plays a critical role in maintaining a healthy body weight (CDC, 2020).
In the United States, there are significant disparities in health behaviors and chronic disease outcomes by race/ethnicity. Hispanics, who are the largest ethnic minority group in the United States, are disproportionately affected by T2DM and CVD (Aguayo-Mazzucato et al., 2019; Rodriguez et al., 2014). Additionally, cancer has recently surpassed CVD as the leading cause of death among Hispanics and Hispanics experience higher rates of cancers of the liver, stomach, and cervix than non-Hispanic Whites (Miller et al., 2018). Although a growing body of literature addresses the systemic reasons for these inequities, there is evidence that individual level educational interventions could be beneficial. For example, compared with non-Hispanic Whites, Hispanics are less aware of the protective role of PA in cancer (Coups et al., 2008). Although a higher proportion of Hispanics met recommendations for F&V intake than did non-Hispanic Whites at the national level, the differences were not statistically significant in New Mexico (NM) (Lee-Kwan et al., 2017), where the present study was conducted, suggesting local need for an educational intervention promoting PA and F&V intake.
Most existing studies featuring short message service (SMS; i.e., text messages) educational interventions have been conducted among non-Hispanic participants. A single US-based feasibility study in a Hispanic population in Los Angeles demonstrated acceptance of healthy living interventions delivered in Spanish via SMS (Whitley et al., 2019). Given regional sociocultural differences among Hispanics in the United States, the next step is to conduct demonstration studies to examine the acceptability and efficacy of SMS- and phone-based health education among different Hispanic populations.
We conducted a randomized controlled trial to assess the impact of an educational intervention delivered via SMS and by phone on self-reported PA and F&V consumption among Spanish-speaking Hispanics in NM. A secondary objective was to assess the usefulness and acceptability of the intervention. We hypothesized that the participants who receive SMS and/or phone calls would report increased intake of daily F&V and daily PA compared to a control group.
Methods
Study Design
This study was a randomized controlled trial of a 12-week educational intervention delivered via SMS and/or phone call (PC). Participants were stratified (male/female) and randomized in blocks of six to one of three groups: control, SMS education (SMS), or SMS + PC education (SMS + PC). Allocation tables were generated using PROC PLAN, SAS 9.4.
Setting, Recruitment, and Randomization
NM is a majority-minority state, with 49% of the population identifying as Hispanic, compared to the US average of 18.5% (Bureau, n.d.). Approximately one-third of the NM population that is more than 5 years old speaks a language other than English at home, 27% of which is Spanish (U.S. Census Bureau, 2018).
Using a convenience sampling approach, recruitment occurred at multiple locations in the Albuquerque and Santa Fe metropolitan areas including the local Mexican Consulate, an outpatient primary health clinic, a fitness center, and a local community center. Study staff verified participant eligibility including age ≥18 years, having preference and ability to read and speak Spanish, having a functioning mobile phone with SMS capabilities, being competent with text messaging, and being able to provide written informed consent.
We recruited 89 Spanish-speaking Hispanic adults who were assigned to the control (n = 30), SMS (n = 29), or SMS + PC (n = 30) groups (see Figure 1). The University of New Mexico Health Sciences Center Institutional Review Board approved the study protocol (#15-041) and participants provided written informed consent for participation.
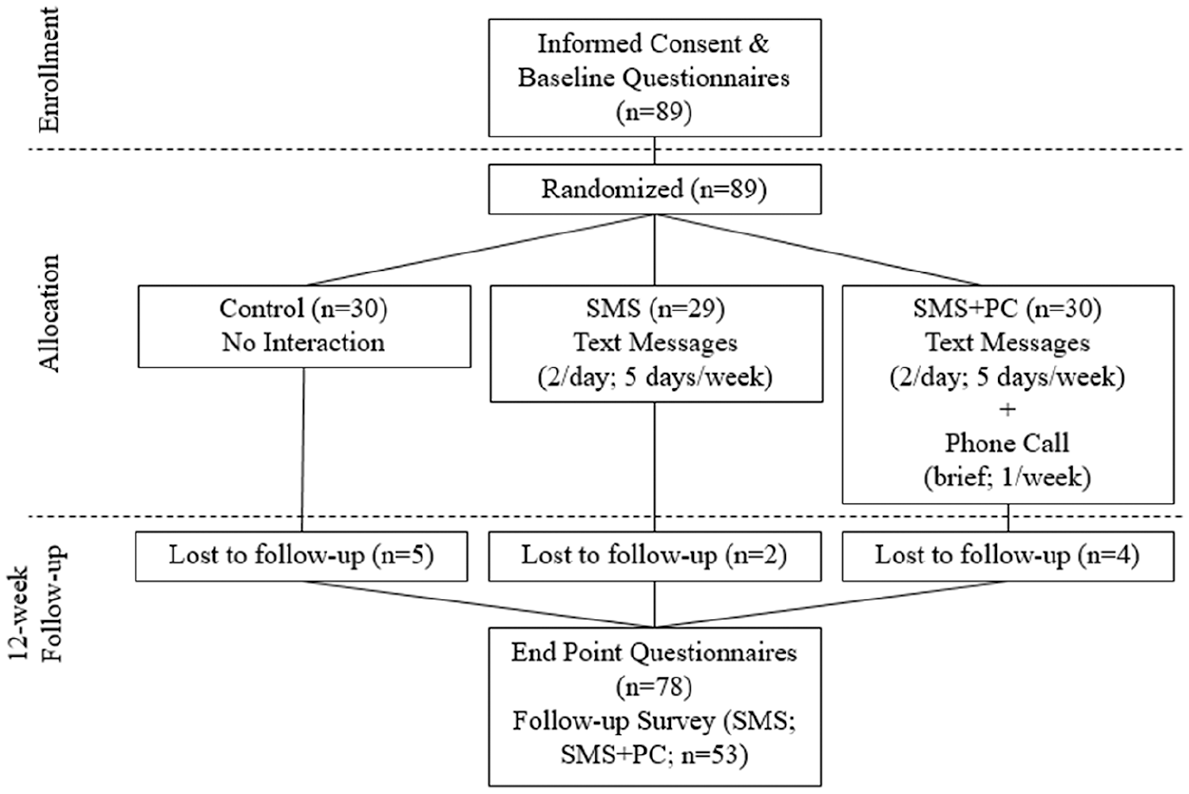
Consort diagram for enrollment through follow-up time period.
Educational Intervention
Forty-six different healthy behavior recommendation messages were developed in a previous (unpublished) project with focus groups of community members and were categorized into three domains: general healthy eating, tips to increase F&V consumption, and tips to increase PA (Table 1).
List of Short Message Service (SMS) Sent to Participants in Intervention Groups.

The length of the educational intervention and frequency of contact were modeled similarly to other studies of SMS used for health management (Hall et al., 2015). The SMS group received two personalized SMS/day each weekday for 12 weeks. The SMS + PC group received personalized SMS at the same frequency as the SMS group, plus a brief weekly phone call (~1 minute) from an experienced native Spanish-speaking health educator (LN) who delivered identical messaging as the SMS. The SMS + PC group received a one-time $10 merchandise card to compensate for any expenses generated from phone calls. Over the 12 weeks, each of the 46 different recommendation messages was sent 2+ times using a fixed schedule via the BulkSMS Red Oxygen program.
Data Collection Instruments
Eligible participants completed a demographic survey and a pre- and post-intervention survey measuring PA (accounting for both leisure time and occupational PA) and daily F&V intake (with portion sizes described) in Spanish. The pre- and post-intervention survey was a seven-item module used to briefly assess cancer knowledge and beliefs as well as current lifestyle practices. Additionally, at the end of the intervention, participants in the SMS and SMS + PC groups completed a survey assessing acceptability and usefulness of the SMS or phone call contacts. Certified native speakers translated all questionnaires and educational messages from English to Spanish, with accuracy verified by back translation. Participants received a $25 merchandise card upon completion of the baseline survey and a $25 merchandise card at the end of the study. Data were collected/managed using REDCap (Harris et al., 2009).
Sample Size Calculation
Assuming a 20% increase in the proportion of participants reporting increased F&V consumption or PA from pre-to-post intervention between the groups, starting from 10% in the control group, a Cochran-Armitage test with a sample of 25 participants per group would achieve a power of 92% at significance level of .05 to detect an increasing trend among the three groups.
Data Analysis
Analyses were performed using SAS 9.4 (SAS Institute, Cary, NC). We used the Cochran-Armitage test to examine whether there was an increasing trend in the proportion of participants reporting increased F&V consumption or PA from pre-to-post intervention across the three study groups: control group < SMS << SMS + PC. Descriptive analyses were conducted to summarize findings from the acceptability and usefulness survey. p < .05 was treated as significant.
Results
The seventy-eight (88%) participants across the three groups who completed both the pre- and post-intervention surveys (loss to follow-up by group: control, n = 5; SMS, n = 2; SMS + PC, n = 4), are included in the analysis. Fifty-three participants in the SMS (n = 27) and SMS + PC (n = 26) groups completed the acceptability and usefulness survey.
Characteristics of the study participants, summarized in Table 2, were comparable across the three groups. The majority of participants that completed the study (n = 78) were adult women (71%), mean age 38.6 ± 13.6 years, who had a high school education or less (55%) and a yearly household income of less than $20,000/year (64%). All participants identified as Hispanic, with the majority reporting Hispanic New Mexican or Mexican-American or Mexican/Chicano/a origins.
Socioeconomic and Recruitment Data for Participants Who Completed Entire Study Overall, and by Group (n = 78).
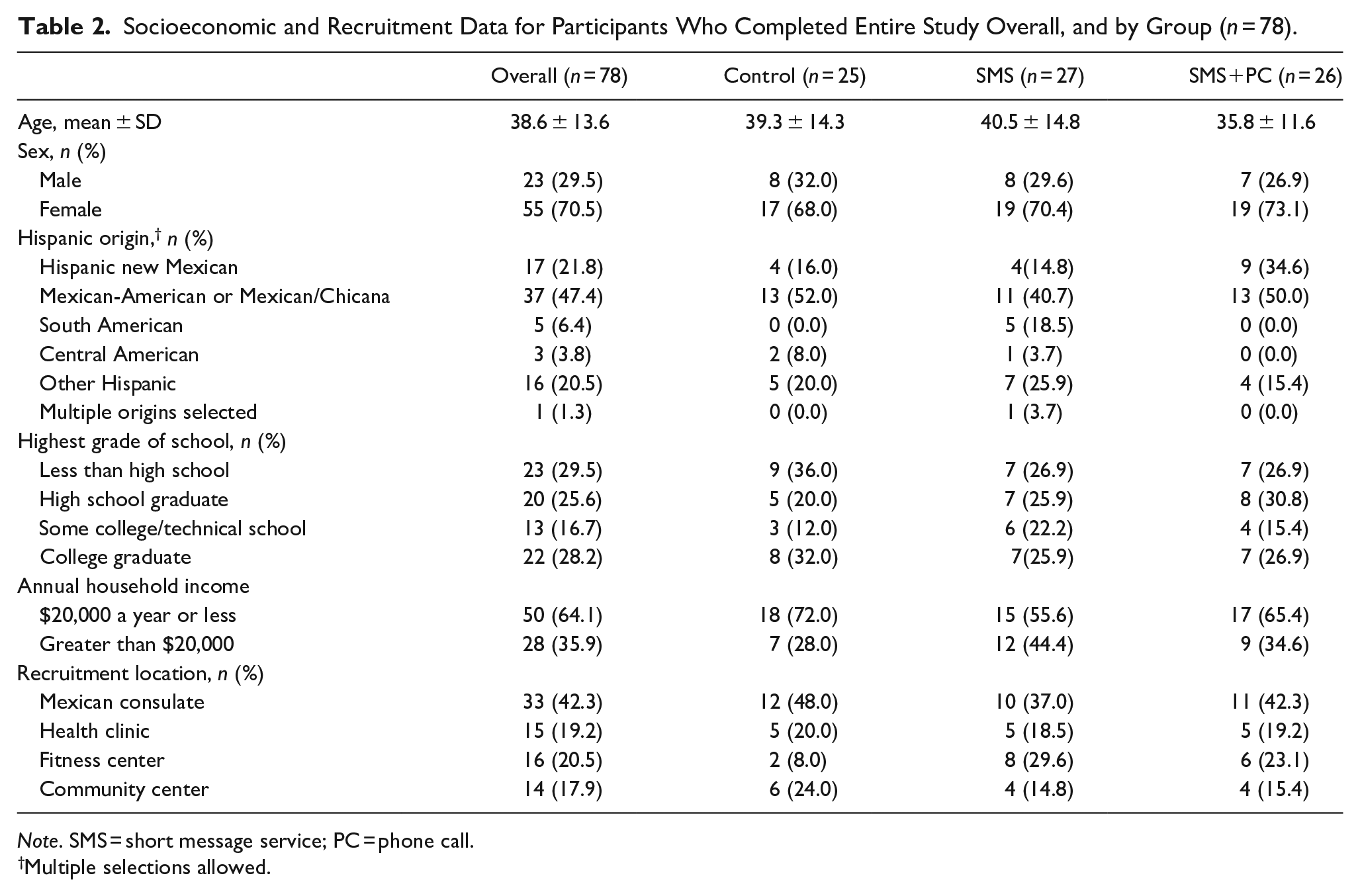
Note. SMS = short message service; PC = phone call.
Multiple selections allowed.
The study results are summarized in Table 3. There was a positive trend in the proportion of participants reporting increased vegetable intake from pre-to-post intervention across the study groups, with the most impact observed in the SMS + PC group (p = .03). About half (54%) of SMS + PC participants reported a pre-to-post intervention increase in vegetable intake, compared to 26% of the SMS group and 28% of the control group. A non-significant positive trend (p = .09) was also noted for reported fruit intake. In addition, there was a positive trend in the proportion of participants reporting an increase in leisure time PA across the three groups (p = .004). Almost three-fourths (73%) of SMS + PC participants reported a pre-to-post intervention increase in leisure time PA, compared to 41% of the SMS group and 36% of the control group. The intervention had no observed effect on reported PA at work across the three study groups.
Results of Testing for Positive Trend Across the Three Study Groups (Control, SMS, or SMS + PC) on Target Behaviors (n = 78).

Note. SMS = short message service; PC = phone call.
Positive trend describes the proportion of the Group with an increase in target behavior where (1) Control < SMS < SMS + PC; or (2) Control < SMS + PC and SMS < SMS + PC. Flat describes equality across ordinal groups.
Cochran-Armitage test for increasing trend in percentages across the three ordinal groups.
p < .05.
The intervention had high acceptance and usefulness (Table 4). Almost all (n = 49; 92%) of participants in the SMS and SMS + PC groups that completed the survey “often” and/or “always” read the SMS sent by the study team. Most (n = 36; 68%) participants indicated they were “likely” or “very likely” to follow the advice in the SMS. A few participants proposed to include recommendations about how one “should be eating. . .” and requested information about local low-cost or group PA resources. Many participants (n = 42; 79%) had unlimited text messaging, with 72% of respondents indicating that they use text to communicate 50% or more of the time. Of those who also received a phone call, almost all participants (n = 24; 94%) considered one weekly phone call to be enough. Most (n = 21; 81%) reported that the phone calls lasted the right amount of time. However, despite the expectation that the call would last approximately 1 minute and simply include a randomly selected health message each week, several (n = 5–7) participants kept the educator on the phone longer each week (up to 15 minutes).
Results of Acceptability Survey of Participants in Intervention Groups (n = 53).
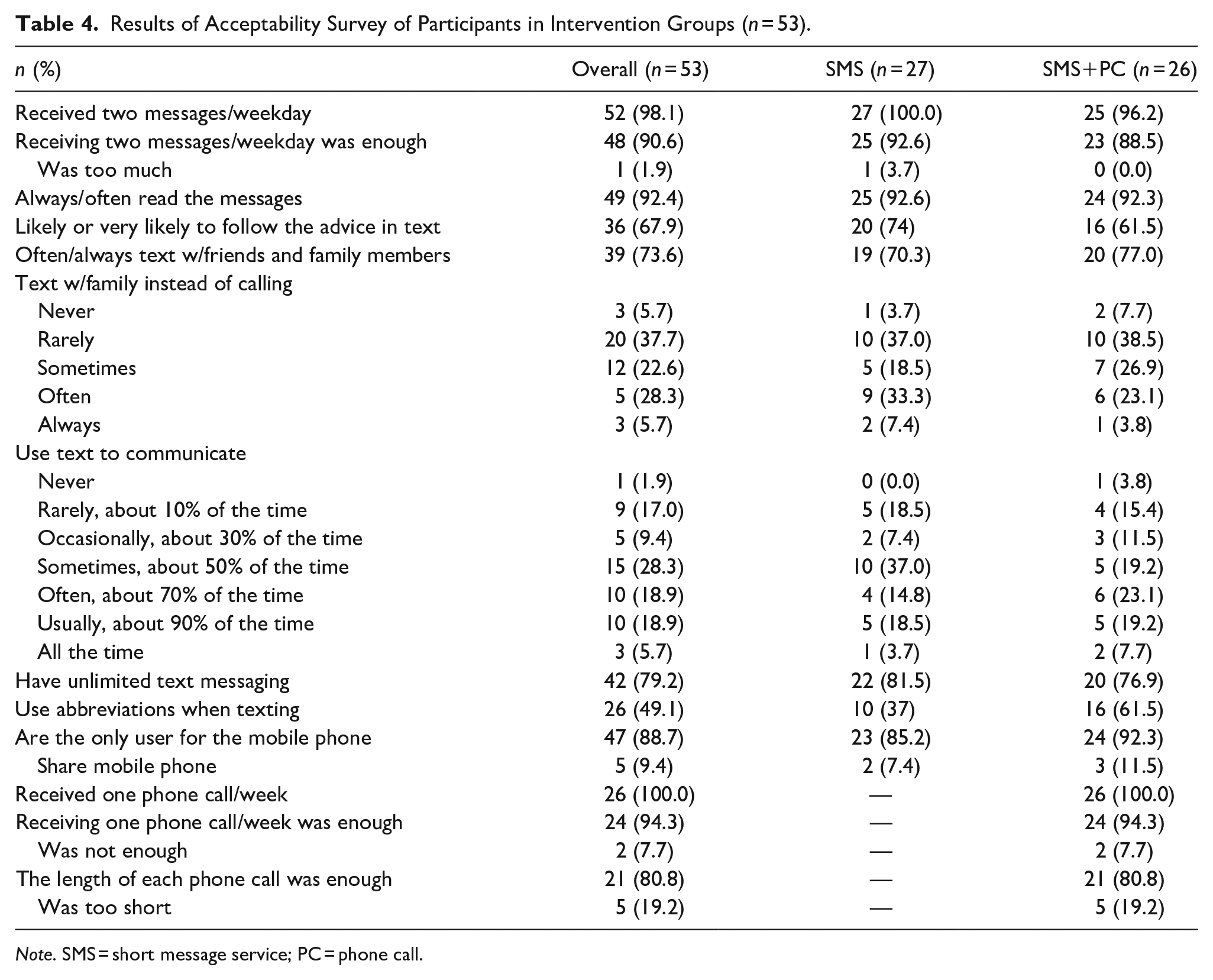
Note. SMS = short message service; PC = phone call.
Discussion
The study aimed to evaluate the impact, usefulness, and acceptability of an educational intervention delivered via SMS and/or phone calls on reported F&V intake and daily PA among an Hispanic, Spanish-speaking population. Reported vegetable intake and leisure time PA were improved across groups, with the largest proportional increases from pre-to-post intervention observed in the SMS + PC group. The majority of participants in the SMS and SMS + PC groups found the intervention to be acceptable and useful.
Overall, the SMS + PC intervention was more effective in increasing reported vegetable intake and leisure time PA relative to the SMS intervention and the control condition. This is consistent with one previous study reporting the effect of automated reminders on behavior change, which may not be as effective if only one modality was employed (Greaney et al., 2012). As part of the intervention, the addition of individualized phone calls as a form of remote coaching might enhance the likelihood of preventing relapse and promoting self-regulation. Multichannel campaign information has been proven effective in English-speaking research contexts (Patrick et al., 2009). This study demonstrates that regular, short, live contacts with a health educator were important for behavior change.
Pre-to-post intervention surveys showed that the SMS + PC intervention had a stronger impact on reported leisure time PA than on vegetable intake. There are several potential explanations for this observation. SMS and/or phone calls regarding PA during free time might have suggested relatively more actionable tasks, compared to the dietary tips. Most of the 16 physical activity tips provided a concrete example of something to do. In contrast, many of the dietary tips were less tangible and more general (i.e., “Live a healthy lifestyle and eat healthy meals”).
The health educator who conducted the phone calls noted that multiple participants commented on the cost burden of fresh F&V. In addition, in the follow-up survey, some participants requested that more details and motivational techniques related to F&V be included, suggesting that their ability to translate their intentions into action might have been limited (Rothman et al., 2009). Third, baseline occupational physical activity levels did not preclude participation, perhaps masking the effect of the interventions in promoting total PA, and not leisure time PA.
Strengths and Limitations
The strengths of our study include a high retention rate, with 88% of participants completing the study, and high reported acceptability and participation in the study interventions. However, the study has some limitations. Self-reported F&V intake and PA may be subject to social-desirability bias, especially in the context of an educational intervention. Twenty-one percent of the participants were recruited from a fitness center, implying that some of these participants were predisposed toward making health improvements or that we observed a ceiling effect among these participants. The present study used a fixed SMS frequency, which might be less effective than an individualized/variable schedule. We assessed this issue in the feedback survey, which will allow us to improve the design of future interventions. Despite best efforts to maintain call length within a minute or two, several participants spoke with the health educator at length (with some calls lasting up to 15 minutes) resulting in some variability in the intervention. Future studies may consider automating the phone call similar to the SMS, if the burden or intervention fidelity of longer calls is a concern.
Implications for Research and Practice
Our findings support feasibility and acceptability of SMS and phone-based health communication strategies with Spanish-speaking participants in NM. Although conducted among a small sample, participants were very accepting of the methodology and reported improved health behaviors. Our results suggest these mobile methods could be used for interventions to promote healthy lifestyles with Spanish-speaking participants and possibly reduce risk of development of non-communicable diseases. Furthermore, given the present intervention challenges posed by the global COVID-19 pandemic, we anticipate these results may serve to inform present and future health promotion efforts.
Footnotes
Acknowledgements
The authors thank Mr. Mauricio Ibarra Ponce de León, Consul of Mexico (2011–2015), Erika Robers, and Maria Otero.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by UNM Comprehensive Cancer Center Support Grant Supplement NCI 3P30CA118100-07S3 and the Behavioral Measurement and Population Science (BMPS) and Biostatistics Shared Resources as well as the Office of Community Partnerships and Cancer Health Disparities.