
Abstract
The purpose of this study was to evaluate the overall effectiveness of a three-tier model of positive behavior interventions and supports (PBIS), which was developed and tested in Head Start (HS) programs. Ten HS classrooms from five HS programs participated in the current study. Results indicated that PBIS was effective in improving classroom quality as evidenced by a statistically significant change on the classroom organization domain on the Classroom Assessment Scoring System and the overall score on the Early Childhood Environmental Rating Scale–Revised. We also found that children’s social skills on the Social Skills Rating System significantly increased from the pre- to post-assessment whereas problem behaviors on the Child Behavior Checklist decreased. The data described here are encouraging and add to the expanding database supporting the value of the three-tier model of PBIS.
Keywords
Children’s problem behaviors have been consistently identified as preschool teachers’ greatest concern (Joseph & Strain, 2003) with externalizing behavior described as most problematic (Snell, Berlin, Voorhees, Stanton-Chapman, & Hadden, 2012). As a result, a great deal of research has focused on the remediation of problem behaviors in the classroom setting. Data from such studies reveal that preschool teachers may lack the training or resources to implement research-based strategies (Carter & Norman, 2010), and thus, tend to resort to reactive interventions with a narrow focus. Individualized, reactive interventions for preschool children may be effective in reducing problem behavior on a short-term basis, but are insufficient as they do not teach children the appropriate behavior or social skills needed to replace problem behavior and produce long-term effects. The use of a three-tier positive behavior interventions and supports (PBIS) model with a continuum of supports to meet the needs of all students may be more effective in linking research-based methods for intervention to classroom practices.
Research-Based Prevention and Intervention Method
Program-wide positive behavior support (PWPBS) and the Teaching Pyramid are emerging models for preventing problem behavior in early childhood programs, such as Head Start (HS) and early childhood special education (ECSE) classrooms (e.g., Fox & Hemmeter, 2009; Frey, Park, Browne-Ferrigno, & Korfhage, 2010; Stormont, Lewis, Beckner, & Johnson, 2007). Both models use the PBIS framework that has been widely applied in K-12 settings. These models address the prevention of problem behavior and promotion of social competence in young children, and are portrayed as a pyramid with three tiers of increasing intervention intensity—Tier 1, Tier 2, Tier 3 (Dunlap, Ester, Langhans, & Fox, 2006; Fox, Dunlap, Hemmeter, Joseph, & Strain, 2003; Stormont et al., 2007). Multiple publications and training materials have provided guidance on the implementation of these models in early childhood settings (e.g., Benedict, Horner, & Squires, 2007; Fox, Carta, Strain, Dunlap, & Hemmeter, 2010; Frey et al., 2010; Hemmeter, Fox, Jack, Broyles, & Doubet, 2007). These studies report positive child outcomes (e.g., reductions in problem behavior, increases in social competence) and program outcomes (e.g., improvements in program quality and teacher skills, reduction of child referrals for mental health intervention).
Tier 1 or universal prevention is implemented with all children in a classroom and is considered the least intensive and most cost-effective. Tier 1 prevention typically includes the following key features: (a) careful planning of the classroom environment, schedule, and materials, (b) teaching children about routines and schedules, (c) rules that specify expected behavior across school settings, and (d) the development of responsive and positive relationships with children such as praising children for engaging in appropriate behavior (Fox et al., 2003).
Approximately 20% of children are not responsive to Tier 1 supports and require the use of Tier 2 intervention (Scott, Alter, Rosenberg, & Borgmeier, 2010). Tier 2 intervention uses intentional teaching strategies to promote children’s competencies in specific social and emotional skills such as emotional literacy, anger and impulse control, interpersonal problem solving, initiating and maintaining interactions, and friendship skills (Fox & Hemmeter, 2009). Theme-based activities (Craig-Unkefer & Kaiser, 2002, 2003) and shared-storybook readings and theme-based activities (e.g., Stanton-Chapman, Denning, & Jamison, 2008; Stanton-Chapman, Jamison, & Denning, 2008; Stanton-Chapman & Snell, 2011) have been used as Tier 2 interventions for preschool children who need targeted social skill interventions.
Tier 3 supports are provided to children whose behavior is not responsive to Tier 1 and Tier 2 supports. Tier 3 interventions are always individualized and often include a functional behavior assessment (FBA) and a behavior support plan (BSP) that is based on the data from the FBA (Dunlap et al., 2010). Key components of the BSP include (a) hypothesis statements that include a description of the behavior, antecedents for the behavior, maintaining consequences, and the purpose of the behavior, (b) prevention strategies that may be used to reduce the likelihood that the child will have problem behavior (e.g., environmental arrangements, changes in activities, changes in expectations), (c) instruction on alternative skills that will replace the problem behavior, (d) consequence strategies used to respond to the problem behavior in ways that will not maintain the behavior, and (e) long-term support strategies (Dunlap et al., 2010).
Consultation and PBIS
Consultation on PBIS techniques has been effective in strengthening teachers’ ability to manage problem behavior in the classroom and is an effective way to introduce PBIS to early childhood settings (Alkon, Ramler, & MacLennan, 2003; Benedict et al., 2007; Carter & Norman, 2010; Duda, Dunlap, Fox, Lentini, & Clark, 2007). Benedict et al. (2007) increased the use of PBIS practices by teachers in four preschool classrooms using consultation. However, a functional relationship was not evident between increased use of these practices and frequency of children’s problem behavior. In a similar study, Carter and Norman (2010) investigated the effects of consultation on teachers’ implementation of Tier 1 practices and preschoolers’ academic engagement. A strong correlation was found between consultation and teachers’ implementation of Tier 1 practices. High levels of academic engagement were maintained following the termination of consultation. More research is needed to strengthen this emerging evidence that consultation on PBIS can lead to positive outcomes in these settings.
Current Study and Its Extension of the Literature
The current study evaluates the overall effectiveness of a three-tier model of PBIS, which was developed and tested in HS programs by the Social Competence in Preschool (SCIP) project. The current study extends the literature in three ways. First, we treated universal prevention as an individualized process. Although teachers were taught to use a comprehensive set of prevention strategies, target strategies varied by classroom as teachers focused on difficult classroom routines they identified with consultants. Our prior experience shows that preschool teachers are typically asked to apply new social and academic skills programs in their classrooms, placing added demands on their time. Based on the advice of a project consultant, we asked teachers to adopt only a few universal prevention practices that we felt and they agreed would have the largest impact on children’s social competence and problem behavior. Second, we taught teachers to analyze the antecedent-behavior-consequences (ABCs) of problematic routines and develop a prevent–teach–respond (PTR) action plan that was feasible to use. The ABC–PTR process, typically a Tier 3 approach applied to individual children who have problem behavior (Dunlap et al., 2010), was used across all tiers to improve classroom routines and individual child behaviors. Third, we expanded the work of Stanton-Chapman and colleagues (e.g., Stanton-Chapman, Denning, & Jamison, 2008; Stanton-Chapman, Jamison, & Denning, 2008; Stanton-Chapman & Snell, 2011) by using the same Tier 2 approach, but had teachers implement it within the classroom setting using milieu prompting techniques (i.e., modeling and/or requesting a response) that were effective in the previous studies.
We report child observation data from separate evaluations of each intervention tier elsewhere (e.g., Snell et al., 2012; Stanton-Chapman, Walker, Jamison, & Smith, 2014). This article presents the results of pre–post child and classroom measures gathered at both the beginning and end of the school year prior to and after the implementation of all three intervention tiers. The following evaluation questions guided the current study: (a) Can classroom staff implement PBIS strategies with fidelity? (b) Does implementation of the three-tier model of PBIS result in an improvement in classroom quality as measured by the Classroom Assessment Scoring System (CLASS; Pianta, LaParo, & Hamre, 2008) and the Early Childhood Environment Rating Scale–Revised (ECERS-R; Harms, Clifford, & Cryer, 2005)? (c) Does implementation of the three-tier model of PBIS result in a decrease in teacher-rated problem behavior and increase in teacher-rated social skills behavior? (d) How do teachers and project consultants perceive the feasibility and effectiveness of the three-tier model of PBIS and of training procedures and materials?
Method
Settings and Participants
Classroom settings
Ten HS classrooms from five HS programs in one mid-Atlantic state participated in the current study. These programs represented urban, suburban, and rural communities. Six of the 10 classrooms were from programs operated by public school systems. The remaining four classrooms were from programs operated by community organizations. Each classroom implemented both Tier 1 (universal) and Tier 2 (social skills) interventions as part of the study. However, only two classrooms had children who needed more intensive support and, therefore, implemented Tier 3 (individualized) interventions.
Adult participants
Each classroom team participating in the Tier 1 and Tier 2 intervention consisted of a lead teacher and a teaching assistant (TA). Demographic information for participating Tier 1 and Tier 2 teachers and assistant teachers can be found in Table 1. Lead teachers ranged in age from 28 to 49 years with an average of 28.8 years, and had between 5 and 14 years of teaching experience. TAs ranged in age from 29 to 57 years with an average of 40 years, and had between 3 and 14 years of experience in preschool settings.
Demographic Information for Classroom Team Participants.
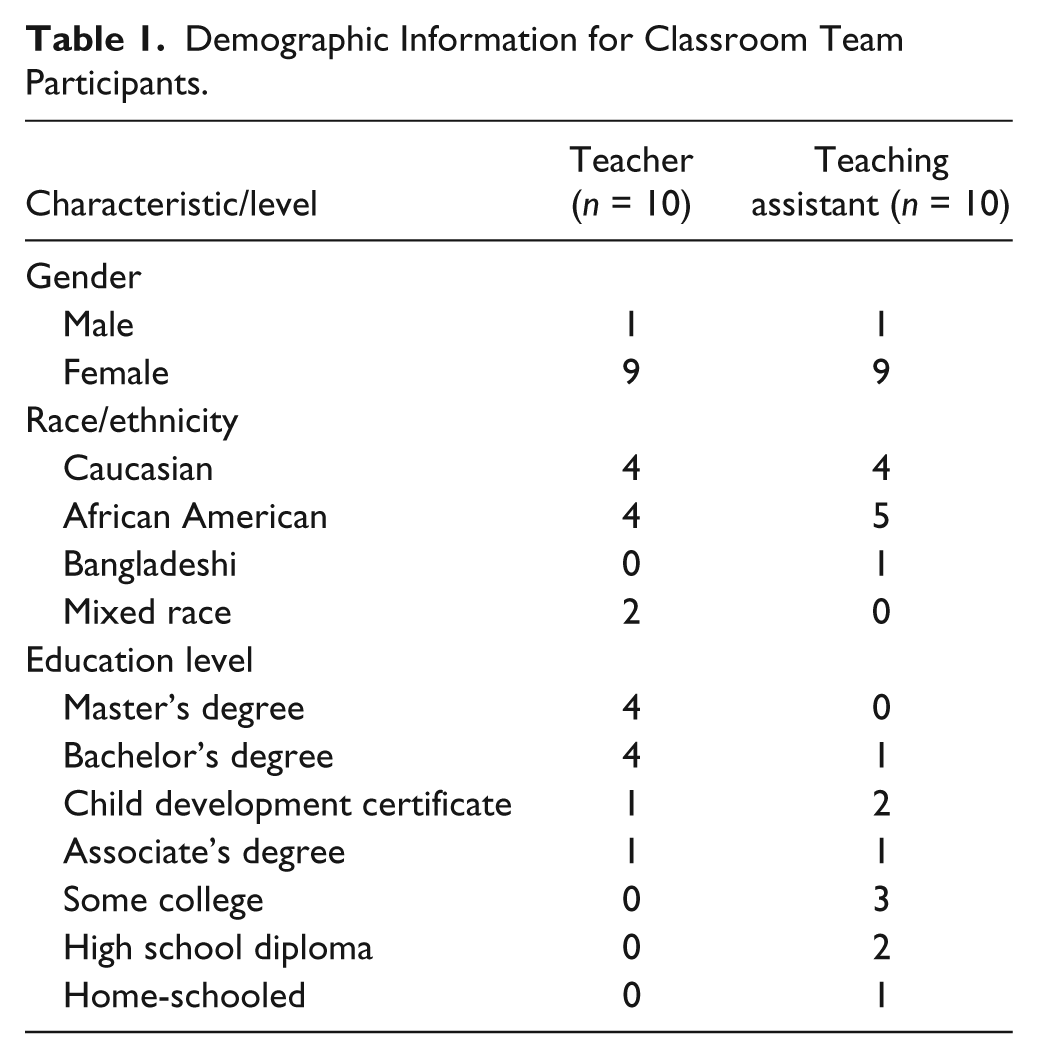
Two classrooms had children who met criteria for Tier 3 (individualized) intervention strategies. The lead teacher in Classroom A was a 45-year-old Caucasian female with 10 years of teaching experience. She had a master’s degree in ECSE and was certified to teach by a state agency. The TA was a 32-year-old Caucasian female with no educational degree and 6 years of teaching experience. The lead teacher in Classroom B was a 47-year-old African American female with 14 years of teaching experience. She had a Child Development Associate (CDA) degree. The TA was a 43-year-old Bangladeshi female with a BA degree in a non-related field and 4 years teaching experience.
Child participants
The Tier 1 intervention program targeted all children (N =179) in the participating classrooms. There was an average of 18 children per class (range of 16 to 20). Boys constituted 51% of children enrolled in the study. The majority of children across programs were African American (49%), followed by Caucasian (31%), and Hispanic (8%). Twenty-seven children (15%) in the 10 classrooms had an Individualized Education Plan (IEP); 14 children (51%) received services for their speech and language delays, 11 (49%) were identified with developmental delays, and two received services for autism. A total of 19 children (11%) had a primary language other than English (i.e., Spanish, Chinese, Farsi, Nepalese, Twi).
Children were identified for Tier 2 intervention by their classroom teachers as having poor social and language skills, and problem behaviors (e.g., unable to recognize body language and facial expressions of peers; had difficulty joining in with groups of children; see Stanton-Chapman et al., 2014). One child was selected from each of the 10 classrooms based on meeting two or more of the following criteria: clinical ratings of problem behavior on the Child Behavior Checklist (CBCL–Teacher Form, Achenbach, 2000), poor social skills as indicated by the Social Skills Rating System (SSRS; Gresham & Elliott, 1990), social pragmatic skill deficits as measured by a social communication target selection form (Stanton-Chapman, 2009), and teachers’ anecdotal identification of challenging behavior. Participants (seven boys, three girls) included four Caucasian children, four African American children, one Hispanic child, and one biracial child. The children ranged in age from 3.75 years to 5 years with an average of 4.28 years. One participating child (Child 1 in Table 3) had an IEP for delays in the areas of speech/language, behavior, fine motor, and cognition.
Children were selected to receive Tier 3 intervention if they met two criteria: (a) The child, on a daily basis, caused injury to self or others, damaged the physical environment, or engaged in behavior that interfered with teaching or learning (Doss & Reichle, 1991), and (b) their problem behavior persisted after Tier 1 and Tier 2 interventions had been implemented. If a coach determined that a child’s behavior was a safety concern to the child or to his or her peers, he or she was immediately placed in Tier 3 intervention. Two children were placed in Tier 3 intervention based on safety concerns. Three children (two boys, one girl) from two classrooms met the criteria for participation in Tier 3 intervention; two of the children were in Classroom A, and one child was in Classroom B. Two children had identified delays or disabilities (Child 1 and Child 11 in Table 3), and one child had no identified delays (Child 12 in Table 3). One child (Child 11 in Table 3), whose family had multiple risk factors, did not follow directions and engaged in physically disruptive or aggressive behaviors. A second child (Child 12 in Table 3) who was diagnosed with autism, exhibited aggressive behavior during classroom transitions. The third child (Child 1 in Table 3) had participated in the Tier 2 intervention but required additional support. Her communication skills were significantly below age level. She typically did not join group activities and wandered in the classroom. When she participated in activities, she would engage in off-task behaviors and disruptive physical behaviors.
Consultants
A consultant was assigned to each classroom team. Four SCIP project staff members served as consultants in the 10 classrooms. They were all Caucasian females ranging in age from 39 to 61 years and had special education teaching experience (three in preschool and one in early elementary). Two consultants had doctoral degrees in education, and two were doctoral students (one in educational psychology and the other in special education). Three of the consultants were each assigned to consult in two classrooms. The fourth consultant was assigned to four classrooms. A consultant manual was developed for each intervention tier that described the specific consultant procedures to be used with classroom teams. Consultants met prior to the initiation of training for each tier to review and discuss training and consultant procedures and then met weekly throughout the year to ensure implementation of consistent consultant practices.
Training of consultants consisted of a workshop on each intervention tier and the review of each consultant’s meeting with classroom teams using her completed ABC–PTR forms, the videos she reviewed with classroom teams, and fidelity forms. Workshop materials included a consultant’s manual, PowerPoint slides and handouts, illustrative videos of problematic classrooms and children, the ABC–PTR form, and directions on how to make edited videos from whole-day videos. The first and fourth authors reviewed each consultant’s paperwork and videos to ensure consultants were following procedures at 90% accuracy. No coaches fell below this criterion during implementation of Tier 1, 2, or 3.
Measurement
Classroom outcome measures
Classroom pre- and post-measures (i.e., CLASS, ECERS-R) were collected based on observations prior to the start of the full intervention (i.e., early fall) and observations after the Tier 3 intervention was completed to determine whether implementation of the three-tier model of PBIS used by the SCIP project resulted in classroom quality improvements. Both measures use a 1 to 7 rating scale (a rating of 6–7 indicates quality care; a rating of 3–5 indicates adequate care; a rating of 1–2 indicates inadequate care). CLASS is used to measure classroom interactional processes and includes 10 subscales organized under three broad domains: (a) emotional support (Positive Climate, Negative Climate, Teacher Sensitivity, Regard for Student Perspectives), (b) classroom organization (Behavior Management, Productivity, Instructional Learning Formats), and (c) instructional support (Concept Development, Quality of Feedback, Language Modeling, Literacy Focus). Interrater agreement across these subscales ranged from .79 to .97 (Hamre, Mashburn, Pianta, Locasale-Crouch, & LaParo, 2006). The ECERS-R evaluates the quality of early childhood programs including space and furnishings, personal care routines, language-reasoning, activities, interaction, program structure, and parents and staff. Interrater agreement across these subscales ranged from .71 to .88 (Perlman, Zellman, & Le, 2004). Two research associates (doctoral students majoring in educational psychology or special education) and two master’s students (majoring in early childhood special education) conducted pre- and post-observations. These individuals were not affiliated with any other aspect of the study. All test administrators were fully trained and reliable at 90% as part of their graduate training on the CLASS and ECERS-R.
Child outcome measures
The following formal teacher rating measures were used to examine children’s problem behavior and social skills: (a) CBCL and (b) the SSRS. Teachers completed the SSRS and the CBCL on each of the 10 children who were targeted for Tier 2 intervention and the three children targeted for Tier 3 intervention. The CBCL contains seven syndrome scales: Emotionally Reactive, Anxious/Depressed, Somatic Complaints, Withdrawn, Sleep Problems, Attention Problems, and Aggressive Behavior. These syndrome categories can be scored in terms of two broad groupings: internalizing and externalizing. CBCL responses to the questionnaire result in a raw score, which is plotted according to the gender of the child and then converted to a T score for all problem scales and syndrome subscales. A raw score 60 or above is considered clinical. The reliability coefficient is .79 for the internalizing behavior scale and .89 for the externalizing behavior scale (Achenbach, 2000). The CBCL has demonstrated content validity, criterion-related validity, construct validity, and concurrent validity.
The SSRS contains a Social Skills Scale, which measures teacher perception of children’s cooperation, empathy, assertion, self-control, and responsibility, and a Problem Behaviors Scale, which measures teacher perception of externalizing problems, internalizing problems, and hyperactivity. For the SSRS, raw scores are converted to a standard score with a standard score between 85 and 115 to be within the average range of functioning. A social skill score below 85 or a problem behavior score above 115 on the SSRS is considered clinical, significantly below the average preschooler in functioning. The SSRS Teacher Form has high external consistency for the Social Skills Scale ranging from .93 to .94 and for the Problem Behaviors Scale ranging from .82 to .86 (Gresham & Elliott, 1990). Test–retest reliability coefficients are also high: .85 for the Social Skills Scale and .84 for the Problem Behaviors Scale (Gresham & Elliott, 1990). The SSRS has demonstrated content validity, construct validity, and concurrent validity with measures such as the CBCL.
Fidelity of implementation
Intervention fidelity data (see Note 1) were collected using videotaped data. For each intervention tier, two research staff (doctoral student and fourth year undergraduate student) were trained to collect fidelity data reliably. Fidelity of Tier 1 and Tier 2 strategies was measured by indicating whether strategies were implemented at any point during the videotaped observation using a yes/no checklist. Tier 3 strategies were measured using three recording components: (a) duration for structural components (e.g., close proximity to adults), (b) percentage of opportunity (e.g., teacher use of transition signal), and (c) percentage of intervals for interactive components (e.g., reinforcement of appropriate behavior). One student served as the primary coder for all videos. To assess interobserver agreement (IOA), 33% of the baseline tapes and 25% of the intervention tapes from each tier (three tapes from each classroom representing a tape from each tier) were randomly selected and then independently coded and scored by two coders (primary and secondary). A criterion of at least 80% IOA was set for the coders on targeted behaviors. If coders fell short of the 80% criterion, both coders simultaneously coded training videos, discussed the videos, and recoded until they met or exceeded criterion. This step occurred once during the entire study (Tier 1).
To compute IOA, we compared agreements between coders on a point-by-point basis by dividing the number of agreements by the number of agreements plus disagreements and multiplying by 100. IOA was as follows: (a) Tier 1—95% (baseline) and 93% (intervention), (b) Tier 2—94% (baseline) and 95% (intervention), (c) Tier 3—structural (95%) and 100% (interaction components). In addition, workshop and consultation fidelity data were collected across each intervention tier to measure the extent to which consultants adhered to the procedures for delivering each workshop and consulting session. Consultants completed self-monitoring checklists after each workshop and consulting session.
Social validity
After all three tiers of the intervention were implemented, seven teachers completed a questionnaire to evaluate the three-tier model of PBIS and training procedures. Teachers were asked to rate the ease of use of each tier of the intervention, the support received from consultants, and the benefits to children on a scale of 1 to 5 (1 = very difficult, 3 = neither difficult nor easy, and 5 = very easy). Open-ended questions were also included to elicit suggestions for improving the training and consulting procedures. SCIP consultants also completed questionnaires on aspects of the intervention training and consultation process. These questionnaires asked consultants to provide feedback on strategies that worked well and suggestions for improvement. Because only three children needed Tier 3 intervention, social validity was assessed by having evaluators rate whether a change in behavior occurred and the social acceptability of Tier 3 intervention procedures.
Description of the Three-Tier Model of PBIS
An introductory meeting was held with each collaborating program prior to the start of the school year. This meeting was designed to welcome the teams to the SCIP project, to describe their roles and responsibilities, and to obtain informed consent. No information related to intervention components was shared at this time to avoid contaminating the baseline data.
Overall SCIP training
After school was in session for 1 month, baseline assessments were conducted using the CLASS and ECERS-R. Following the completion of the baseline measures (5 to 6 weeks after the start of school), an orientation workshop was held to provide an overview of PBIS and the benefits of using a three-tier PBIS approach in preschool classrooms. Following the orientation workshop, we provided training and consulting on each of the three intervention tiers. Training for each tier consisted of a workshop with classroom teams on the particular PBIS component followed by a series of consulting sessions designed to support classroom team implementation fidelity. Although workshop content varied by tier, all workshops used PowerPoint slides and handouts, case studies, role modeling, and illustrative videos as instructional strategies.
The SCIP training and consulting followed the same problem-solving process for each intervention tier. This process involved identifying the ABCs for problem behavior or social skill breakdowns and then developing an action plan with PTR strategies to address the problem behavior or social skill deficiencies. Although this process is typically only used for Tier 3 interventions (e.g., Dunlap et al., 2010), we simplified and adapted the process for use with Tiers 1 and 2 to encourage classroom teams to examine and address all critical factors contributing to children’s problem behavior or social skill breakdowns (e.g., the classroom environment, teacher interactions). All 10 classrooms participated in each of these workshops. Tier 1 was implemented over a 4-week period. Tier 2 was implemented for 10 weeks. Classroom teams were encouraged to continue implementing each tier throughout the duration of the study without additional consulting. Tier 3 was implemented for 4 weeks. Based on consultants’ anecdotal records, all classrooms continued to implement Tier 1 and Tier 2 strategies after consulting had been discontinued.
Tier 1
The Tier 1 workshop averaged 1 hr 42 min with a range of 1 to 2 hr. A six-step ABC–PTR problem-solving process aimed at improving classroom routines was used: (a) Identify a problematic routine, (b) identify the ABCs for problem behavior in the routine, (c) identify strategies to improve the routine, to reduce problem behavior, and to increase social skills (using a universal strategies checklist), (d) develop an action plan that used PTR strategies to improve the routine, (e) implement the plan, and (f) evaluate the plan’s effectiveness and revise if needed. Each classroom selected one problematic routine to target for intervention; nine classrooms selected a transition routine (e.g., transition from cleanup time, large group circle into small groups) and one selected a literacy activity.
A Universal Strategies Checklist (Berlin, Voorhees, & Snell, 2010) was provided for teams to use to assist in the selection of evidence-based strategies to improve targeted routines. Two categories of universal strategies were included in the checklist: (a) classroom preventative practices that cease or reduce children’s problem behavior and increase children’s engagement and learning (e.g., rules, defined schedule, planned transitions, developmentally appropriate activities, room arrangement, positive discipline), and (b) strategies that promote positive relationships including teacher–child interactions (e.g., supportive conversations, responsiveness, nonverbal communication). Checklists were modified to meet the needs of individual children. Classroom staff also received a manual that included detailed information about Tier 1 implementation (see Snell et al., 2014, for more information pertaining to Tier 1 procedures).
Tier 2
The Tier 2 workshop averaged 1 hr 45 min with a range of 1 hr 20 min to 2 hr. We used the Social Pragmatic Storybook Intervention (SPSI; Stanton-Chapman et al., 2014) as the Tier 2 intervention. SCIP consultants taught classroom how to implement SPSI strategies to teach children the following social communication skills: (a) Talk to your friend (Initiations): verbally initiating a conversation to a peer, (b) listen then respond to what your friend says (Responding): verbally responding to peer verbal initiations with adequate responses, (c) use your friend’s name (Use of name): stating a peer’s name to gain his or her attention before talking to him or her, and (d) take a turn and give your friend a turn (Turn-taking): taking an appropriate number and length of turns in conversation or play.
Coaches and classroom teams collaborated to determine which children had social communication delays and were in need of a social interaction intervention. Teams reviewed language assessments completed by the schools’ speech–language pathologist and conducted in-class observations of children interacting with peers to make the final selection. SSRS and CBCL assessments were completed on the selected children. The specific storybook reading procedure included (a) introducing children to target vocabulary words that corresponded to the play theme, (b) introducing the roles for each theme, (c) reading the storybook, and (d) having children plan their play by selecting play partners and discussing roles. Classroom teams also learned to use prompting strategies to support children’s play during center time. Teachers learned to stay in the play area to observe play and prompt play when social interactions were not taking place. Prompting was used to encourage children (a) to engage in the thematic play activity, (b) to use target vocabulary words, and (c) to interact using the social communication strategies. Classroom staff received a manual with details about SPSI implementation that they could use as a reference guide during SPSI intervention (see Stanton-Chapman et al., 2014, for more information about Tier 2 procedures).
Tier 3
Classroom teams then participated in a Tier 3 workshop that averaged 2 hr. A five-step individualized PBIS process was used: (a) Initiate procedure for considering individualized support, (b) plan and conduct functional behavioral assessment and write a hypothesis, (c) design and write a PBIS plan, (d) implement and monitor effectiveness of PBIS plan, and (e) plan for child’s transition into another grade/school with long-term maintenance. Classroom staff received a manual that summarized the individualized PBIS steps. Online resources, such as the Routine-Based Support Guide for Young Children With Challenging Behavior (Lentini, Vaughn, & Fox, 2004), were reviewed to illustrate how to select PTR intervention strategies based on the function of a child’s challenging behavior. This guide listed strategies for use during different routines (e.g., transitions, center time) that matched specific behavioral functions (e.g., escape, attention, sensory). The guide also supported classroom staff to select strategies linked to the hypothesized functions of a child’s behavior. Consultants conducted assessments and provided support to classroom teams to develop hypothesis statements and corresponding BSP strategies. BSP’s plans comprised of prevention, teaching, and consequence strategies were developed through the use of the ABC–PTR process and matched the identified function(s) of the targeted problem behaviors for each child (see Voorhees, Walker, Snell, and Smith [2013)] for more information about Tier 3 procedures).
Description of SCIP consulting
Consulting sessions were conducted for all three intervention tiers to support classroom team’s implementation fidelity; the same consulting process was followed for each tier. Consultations averaged 16.5 hr in the classroom across all tiers. While in the classroom, consultants observed and videotaped the target routine or child, modeled action plan strategies, and provided feedback. An additional average of 8.4 hr was spent in consulting meetings per classroom. Prior to each consulting meeting, consultants reviewed tapes and selected exemplar footage to share with the classroom staff. These segments were selected to illustrate the teacher’s use of the PTR strategies identified in the action plan. During the meetings, consultants and classroom staff reviewed the video footage, compared it with the action plan, and used the problem-solving process to determine what was working well or whether changes were needed in the plan. After agreeing on any needed changes to the action plan, the classroom staff implemented and videotaped their use of the strategies in the revised plan the following week. Consultants recorded changes on the action plan and left a copy with the team.
Data Analysis
Given the small sample size, average pre-test and post-test scores for all programs were analyzed using a t test analysis. Average pre-test and post-test data from classroom outcomes (i.e., ECERS-R, CLASS) and from child outcomes (i.e., SSRS, CBCL) were compared to determine whether there was a significant difference in scores (either positive or negative). Cohen’s d (1988) was used to calculate effect sizes where d is the difference between the means divided by the standard deviation of either group. A small effect size is d = 0.20, a medium effect is d = 0.50, and a large effect is d = 0.80.
Results
Fidelity of Implementation
Implementation fidelity varied across teachers and intervention tier. Fidelity during Tier 1 averaged 85% with a range of 63.8% to 100%. Fidelity for structural components was slightly higher (M = 85.66%) than for interaction components (M = 80.4%) during implementation. Tier 2 implementation fidelity varied greatly across classrooms and across intervention components. Teachers completed on average 97% of center set-up intervention steps before the start of the play sessions (range: 0.93–1.0). Teachers completed an average of 76% of the identified prompt items during the play sessions (range: 0.49–1.00). Tier 3 fidelity varied based on the classroom and the type of strategy used. Teachers’ mean fidelity for structural strategies that occurred across the entire routine was 70.4% (range: 10.7 %–90.6%) for one target child and 97.2% (range: 93%–99%) for the second target child; this type of strategy was not included in the third child’s plan. Implementation fidelity for structural component strategies that occurred once or twice in the routine was higher for the two children from the same classroom (92.7%, 100%) but lower (66%) for the child from the second classroom.
Classroom Outcomes
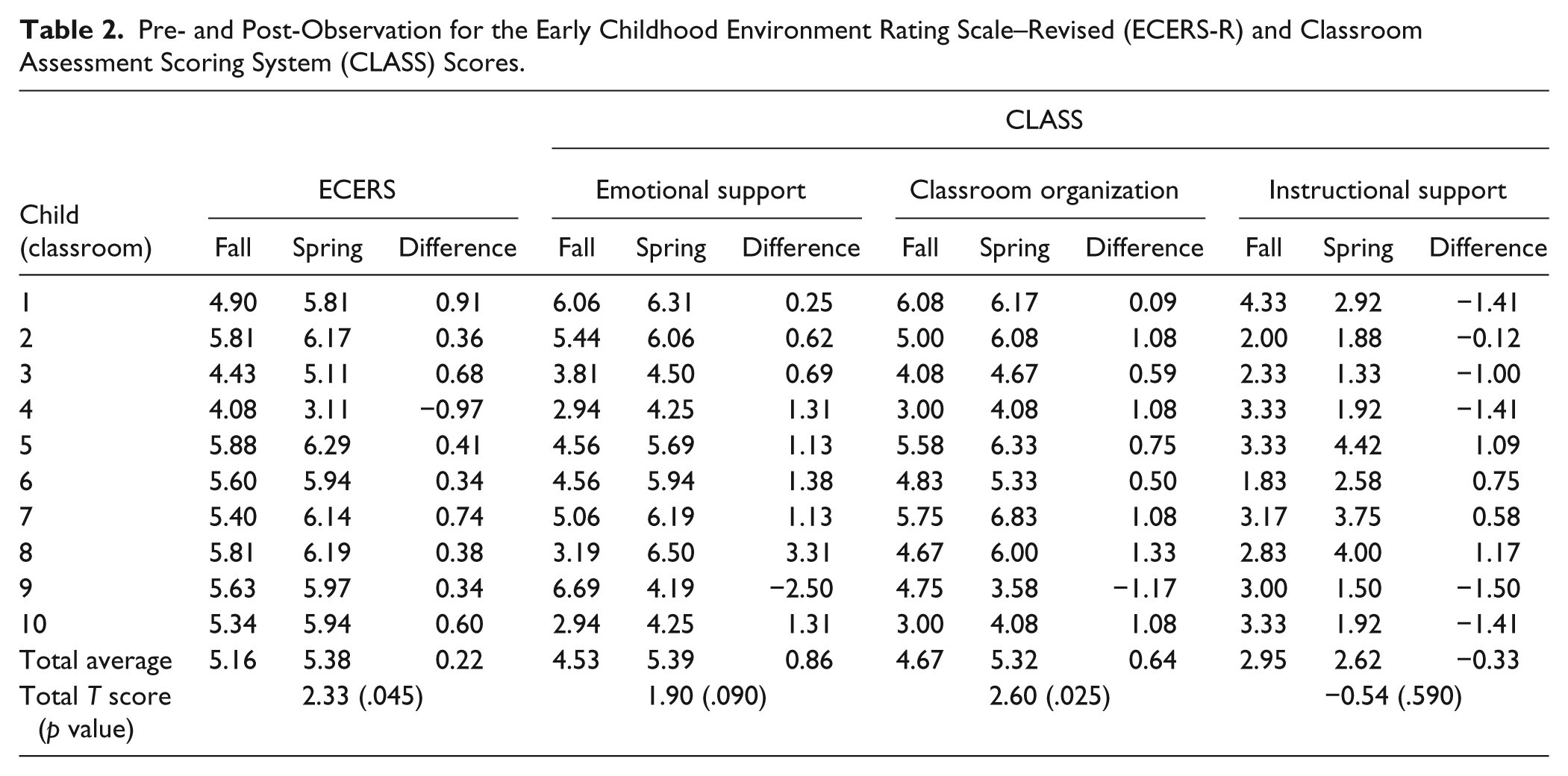
Table 2 presents CLASS and ECERS-R pre- and post-test scores for the 10 HS classrooms participating in the SCIP project. The CLASS results indicate that all classrooms demonstrated gains in the classroom organization domain. T tests were conducted on the mean differences between the fall and spring observations across all classrooms. For classroom organization, there was a significant difference between average pre- and post-observation scores at the p < .5 level (t = 2.26, p = .025, d = 0.28). There was no significant pre- and post-observation difference for emotional support (t = 1.90, p = .090, d = 0.14) or instructional support (t = −0.54, p = .590, d = −0.17). ECERS-R total scores showed improvement in nine of the 10 classrooms. The total scores at the pre-observation averaged 5.16. This score significantly increased at the post-observation to 5.38 (t = 2.33, p = .045, d = 0.13). One classroom had a decrease in their ECERS-R score.
Pre- and Post-Observation for the Early Childhood Environment Rating Scale–Revised (ECERS-R) and Classroom Assessment Scoring System (CLASS) Scores.
Child Outcomes
Table 3 presents child outcome data for the children participating in Tiers 2 and/or 3 of the three-tiered model of PBIS. Ten children participated in the Tier 2 SPSI intervention. Complete SSRS and CBCL data are available for nine participants; one child relocated from the schools before post-teacher ratings were conducted. All nine children showed significant increases in social skill abilities (t = −4.24, p = .05, d = 0.65) and showed significant decreases in problem behavior as rated by their teachers (t = 4.11, p = .05, d = 0.67) on the SSRS.
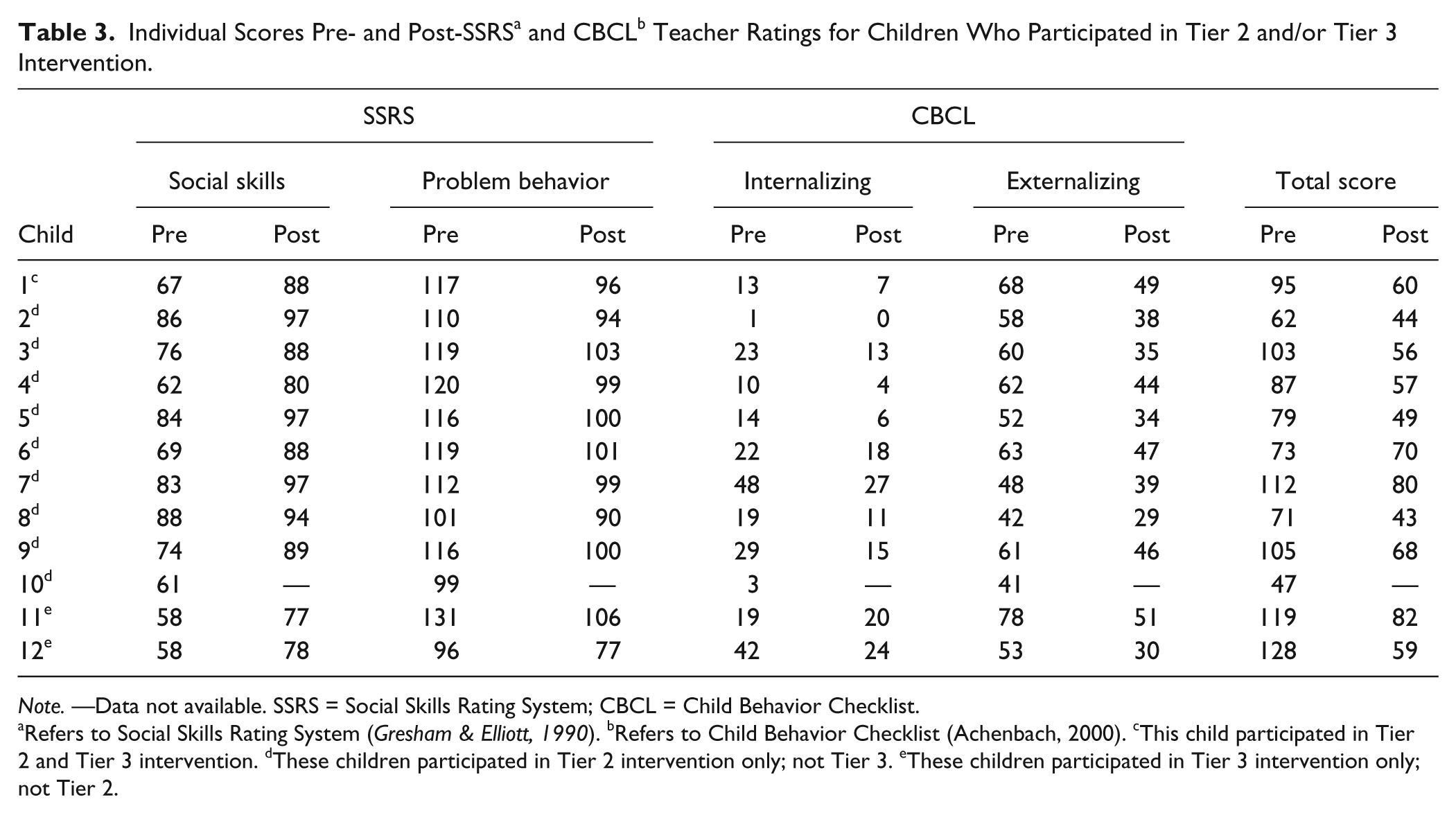
Note. —Data not available. SSRS = Social Skills Rating System; CBCL = Child Behavior Checklist.
Refers to Social Skills Rating System ( Gresham & Elliott, 1990 ). bRefers to Child Behavior Checklist (Achenbach, 2000). cThis child participated in Tier 2 and Tier 3 intervention. dThese children participated in Tier 2 intervention only; not Tier 3. eThese children participated in Tier 3 intervention only; not Tier 2.
CBCL results for the nine participants showed overall decreases in internalizing, externalizing, and total problem behavior. Internalizing behavior did not significantly decrease from pre- to post-intervention (t = 1.43, p = .08, d = 0.12). Externalizing behavior, however, did significantly decrease from pre- to post-intervention (t = 4.01, p = .05, d = 0.67). The total mean difference in total problem behavior as reported by the CBCL was also significant (t = 3.34, p = .05, d = 0.60). All children showed decreases in problem behavior according to teacher report on the CBCL.
Three children received Tier 3 intervention. One of these children (Child 1, see Table 3) also participated in Tier 2 so her SSRS and CBCL results are not repeated. Child 11 and Child 12 (see Table 3) showed an increase in social skills and a decrease in problem behavior as measured by the SSRS. For the CBCL, internalizing behavior, externalizing behavior, and total problem behavior scores decreased tremendously from pre- to post-intervention.
Social Validity
Seven teachers completed an evaluation of the consultation and of the three-tiered model of PBIS procedures. All seven teachers reported that each tier of intervention was either “easy” or “very easy” to use. Teachers also rated the benefits to children of the overall three-tier model of PBIS used by the SCIP project and of each intervention. The mean rating for the benefits of the overall model was 4.6 with similar ratings for Tier 1 (M = 4.8), Tier 2 (M = 4.7), and Tier 3 (M = 4.5). Ratings were also positive with regard to the support teachers received from their SCIP consultant with a mean rating of 4.9. Finally, teachers were asked to rate the ease of taping in the classroom. The majority of teachers reported that it was easy (n = 5); one teacher reported that the task was “very easy” and one as “neither easy nor difficult.” In addition to rating aspects of the three-tiered model of PBIS, teachers were asked to provide suggestions for improvement. Only one teacher responded by suggesting that videotaping would be easier if there was a third person to assist with the rest of the class. This is important for future investigations. Five teachers provided positive comments. Illustrative comments included “I am very pleased with the changes in my class” and “. . . every classroom should [get] a chance to experience SCIP.”
SCIP consultants provided feedback on aspects of the training and consulting process that worked well and suggestions for improvement. One of the major points highlighted with regard to what worked well was the use of videotapes for consulting. Consultants reported that teachers appreciated the value of observing their teaching on videos to identify factors affecting child behavior and to see child progress over time. Consultants also felt the time they spent in the classrooms to learn firsthand about the challenges the classroom staff faced, and to model strategies and to provide support to address these challenges, were critical with regard to relationship building and teacher buy-in to the use of the three-tier model of PBIS. Consultants also noted that the use of a consistent ABC–PTR problem-solving process across all tiers of intervention, which allowed intervention strategies to be tailored to each classroom’s specific needs, was also positively viewed. Teachers valued their role in providing input in this process and the importance that the SCIP project placed on responding to teacher feedback. Last, consultants reported that it was an asset that all project consultants had classroom experience as this assisted in building camaraderie, respect, and trust with classroom staff.
Consultants indicated that although child behavior improved across all tiers, additional consulting related to each tier may be needed for maximum impact. Consultants also emphasized that some classrooms had most Tier 1 strategies in place, and suggested incorporating a needs assessment or developing criteria to determine whether a classroom did not need Tier 1 training and could begin with Tier 2 implementation.
Discussion
In the current study, classroom and child outcomes, intervention fidelity, and teachers’ and consultants’ feedback were examined following the implementation of a three-tier model of PBIS. This model included the use of a consistent ABC–PTR problem-solving approach across all three intervention tiers and the implementation of SPSI as a targeted Tier 2 intervention. In this section, we describe implications for practice, limitations, and areas for future research.
Intervention fidelity varied across teachers with higher fidelity found in teachers who held graduate degrees (i.e., master’s degrees) or had more years of classroom experience. This finding occurred for all three intervention tiers. Possible explanations for these results include procedures that were too complicated for teachers new to the profession or teachers who had little knowledge on educational terminology provided in preservice college programs, a lack of administrative support, or teachers experiencing burnout from job-induced stress (Ransford, Greenberg, Domitrovich, Small, & Jacobson, 2009).
Results indicated that the three-tier model was effective in improving classroom quality as evidenced by a statistically significant change in the average standard score for both (a) the classroom organization domain on the CLASS and (b) the ECERS-R. Classroom organization changes on the CLASS led to a small effect, but no effect was found for the ECERS-R (Cohen, 1988). Other studies have reported an increase in the use of PBIS practices following program implementation, which reflect program improvement (Fox & Hemmeter, 2009; Frey et al., 2010; Muscott, Pomerleau, & Szczesiul, 2009). For example, Fox and Hemmeter (2009) found that early childhood teachers and program teams in Iowa made progress in the implementation of the Teaching Pyramid model as measured by the Teaching Pyramid Observation Tool (TPOT) and the Early Childhood Benchmarks of Quality. Muscott et al. (2009) noted that early childhood programs that participated in PBIS implementation in New Hampshire increased their implementation of preventative features of PBIS as measured by the School-Wide Evaluation Tool (SET). The results of this study are promising as they confirm that improvements can be demonstrated using standardized classroom quality measures.
The three-tier model of PBIS also resulted in positive outcomes for children. Children who received targeted Tier 2 and 3 interventions had statistically significant decreases in average standard scores for externalizing and total problem behavior on the CBCL. Internalizing scores on the CBCL had no effect whereas externalizing score and total CBCL score changes had a medium effect finding (Cohen, 1988). These findings are consistent with child observation data we report elsewhere that demonstrated reductions in children’s problem behavior following implementation of each intervention tier (e.g., Snell et al., 2012). The results are also consistent with PBIS implementation studies that have documented significant decreases in children’s problem behavior in programs that reliably collected behavior incident data (e.g., Muscott et al., 2009). We also found that children’s social skills as measured by teacher ratings on the SSRS significantly increased from the pre- to post-assessment, leading to a medium effect size (Cohen, 1988). This finding is noteworthy, as the three-tier model of PBIS implemented by the SCIP project did not directly target SSRS social skill areas (e.g., cooperation, empathy, assertion, etc.). Child observation data reported elsewhere (Stanton-Chapman et al., 2014) increased for nine out of ten children in interactive play behavior, which was the focus of the Tier 2 SPSI intervention. Other PBIS implementation studies have found medium to large effect size improvements in children’s social competence as measured by teacher ratings using Early Screening Project measures of children’s adaptive behavior and social interaction (Feil et al., 2009).
Results from the CLASS assessment showed significant improvements in the average score on the Classroom Organization subscale; however, significant increases for Emotional and Instructional Support subscales were not observed. These results are not surprising given the item content within the subscales. The Classroom Organization subscale has items that focus on behavior management, productivity, and instructional learning formats. The three-tier model of PBIS used by the SCIP project targeted all of these skills in its training materials and procedures. However, we did not address all skills assessed in the emotional support (e.g., encouraging children to talk and share their ideas) and instructional support domains (e.g., providing children with opportunities to use analysis and reasoning in their approach to problems). We believe that, without key components in place (e.g., classroom organization including rules and routines), behavior problems whether severe or minor can prevent quality instruction from happening.
Limitations, Implications, and Conclusion
The following limitations need to be mentioned when one evaluates the three-tier model of PBIS implemented by the SCIP project. The first limitation involved the scheduling of training and consultation to allow assessment across all three intervention tiers. Various school constraints (i.e., special classroom activities, field trips, teacher illnesses, workshop requirements and vacations, school testing requirements, school closings due to weather) resulted in a limited amount of time to test each intervention tier within an academic year. These time constraints only allowed testing of the Tier 1 universal problem-solving approach with the most problematic routine in each classroom and to test the Tier 2 SPSI intervention with the child from each classroom who had the most significant social skill difficulties. Ideally, Tier 1 and 2 interventions would continue to be used as needed. A second limitation involves the measurement of workshop and consulting fidelity and pre–post assessment data collection. Consultants used a checklist to measure the extent to which they adhered to the manualized workshop and consulting fidelity procedures. Project staff evaluated classroom quality prior to and after intervention using the CLASS and ECERS-R. In both of these cases, reporter bias is a major concern, as agreement checks were not conducted to verify these self-reported data. A third limitation is the simple data analytic plan utilized in the current study. Future work should use more sophisticated analyses exploring mediating and moderating variables as appropriate for larger samples.
The practical implications of the three-tier model of PBIS implemented by HS classrooms participating in the SCIP project lie in the combined results of the classroom and child outcome measures, intervention fidelity, and teachers’ and consultants’ feedback. This model is an example of a comprehensive approach that includes universal and targeted interventions implemented by classroom staff with various skillsets in typical HS programs. Although more data are needed on the maintenance of program and child effects over an extended period, the data described here and in child observation data from separate evaluations of each tier of intervention (e.g., Snell et al., 2012; Stanton-Chapman et al., 2014) are encouraging and add to the expanding database supporting the value of the three-tier model of PBIS.
Furthermore, classroom staff evaluated the procedures as effective in improving problem behavior and social skills, worth the time and effort, and easy to implement, and were likely to recommend to others. Classroom staff and consultant feedback also suggested that the training and consulting procedures used by the SCIP project were effective. The use of a consistent ABC–PTR problem-solving process for all three intervention tiers coupled with the use of videotapes during consulting sessions was highlighted as an effective feature that promoted teachers’ involvement and growth. Further research is needed to investigate the benefits of these unique features. In addition, the incorporation of a needs assessment as other PWPBS models have done (Fox & Hemmeter, 2009) may be valuable in individualizing training for classrooms.
Consultants and teachers reported that they appreciated the value of observing teachers’ instruction on videos to identify factors affecting child behavior and to see child progress over time. We advocate for the use of videotapes to not only reflect on lesson plan details, but also reflect on how lesson plans and teacher behaviors influence child behavior. Reflective analysis of the teacher’s verbal behavior (i.e., what is said to particular children), the teacher’s paralingual behavior (i.e., intonation, speaking pace, and volume), and the teacher’s nonverbal behavior (e.g., body posture, eye contact, use of gestures) may be useful in determining what may have led to a change in a child’s behavior.
As HS programs address the need to promote children’s healthy social emotional development and prevent problem behavior, the three-tier model of PBIS holds promise as a comprehensive approach that early childhood programs can implement to address all children’s needs. HS programs have limited resources, and intervention intensity must be matched to the severity of the problem behavior and social skill difficulties. As HS programs make important decisions regarding intervention selection, a three-tier model of PBIS provides a hierarchy of prevention and intervention strategies with intervention intensity matched to children’s needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The research reported here was supported by the Institute of Education Sciences, U.S. Department of Education, through Grant R324A080016 to the University of Virginia. The opinions expressed are those of the authors and do not represent views of the U.S. Department of Education.