
Abstract
Parent training (PT) is widely used with families of children with autism spectrum disorder (ASD), and its benefits for young children and their parents have been documented. However, no reviews have examined the use of PT within interventions delivered to older children with ASD or investigated the added benefit of including a PT component in these interventions. Therefore, the purpose of this review is to explore the state of research regarding the inclusion of PT in interventions for school-age children with ASD and to determine the value added to these interventions by including a PT component. Fifteen PT studies examining 622 child participants with ASD were included. Participants, interventions, and the effects of the interventions are described. Overall, studies demonstrated moderately positive effects for interventions that included PT. Importantly, three studies isolating the added benefit of PT demonstrated an effect size (ES) of 0.33, 95% confidence interval (CI) [0.05, 0.61], indicating the value added to interventions by including parents. More research is needed to understand the development of effective PT, its components, and how to best design these programs to benefit school-age children with ASD.
Autism spectrum disorder (ASD), characterized by difficulties with communication and social interactions, begins in early childhood and persists throughout an individual’s life. In addition to social and communication deficits and repetitive behaviors (American Psychological Association [APA], 2013), children with ASD can exhibit a variety of challenging behaviors, including anxiety, self-injury, noncompliance, aggression, and property destruction (Gadow, DeVincent, Pomeroy, & Azizian, 2004). Maladaptive behaviors and skill deficits frequently persist into adulthood, leaving most adults with ASD unemployed, socially isolated, and dependent on their families or other support services (Howlin, Goode, Hutton, & Rutter, 2004). Because of these difficulties, many families seek treatment for their children aimed at reducing the frequency of challenging behaviors and increasing functional skills. These interventions often include a parent training (PT) component.
Rationale for PT
Behavior therapists often provide training to family members to facilitate interventions, whereby parents can become the primary interventionist or a supplement to children’s therapist-driven programming. When parents are able to implement treatments with fidelity, it can result in lasting improvement for children (Vismara, Colombi, & Rogers, 2009). In addition to child outcomes, PT in behavior management and teaching strategies may also help to alleviate some of the stress experienced by family members as they attempt to engage in daily activities and access services for their children (Keen, Couzens, Muspratt, & Rodger, 2010; Minjarez, Mercier, Williams, & Hardan, 2013).
Impact on the Family
In families of children with ASD, parents and other family members experience high levels of isolation, stress, and psychological difficulties. In a survey of parents and caregivers of children with ASD, Dillenburger, Keenan, Doherty, Byrne, and Gallagher (2010) found over 80% of parents described limitations on their families’ social, community, recreation, and leisure activities. Parents also stated they spent decreased amounts of time with their partners and their other children, and 80% of parents said they worried their other children felt neglected and treated unfairly. Further supporting these findings, in a meta-analysis of parent stress, Hayes and Watson (2013) found that parents of children with ASD experience higher levels of stress than parents of typically developing children and those of children with other disabilities. Many parents of children with ASD cite difficulties managing everyday behavior and unmet needs for support and care as sources of stress (Sharpley, Bitsika, & Efremidis, 1997).
Therefore, training parents to cope with ASD symptoms and facilitate the acquisition of necessary skills is important for reducing parent level of stress and to improve treatment outcomes for children. In fact, research has shown PT interventions for parents of toddlers and young children with ASD lead to considerable improvements in parents’ stress, self-efficacy, and mental health (Keen et al., 2010; Minjarez et al., 2013; Tonge et al., 2006).
Benefit of Parents as Therapy Support
Using parents as therapeutic support provides several advantages for children with ASD, as well as for families and interventionists. Behavioral interventions for young children with ASD demonstrate better outcomes when implemented for more hours and over a longer duration (Reichow & Wolery, 2009). When parents are able to implement programming, either as the primary or secondary instructor, it extends the number of opportunities for children to experience an intervention beyond the scope of their contact with teachers and clinicians. Parents’ use of behavioral interventions also facilitates children’s ability to generalize skills to other individuals and settings (Matson, Benavidez, Compton, Paclawskyj, & Baglio, 1996). In a study conducted by Koegel, Schreibman, Britten, Burke, and O’Neill (1982), children with ASD whose parents were trained to implement a behavioral intervention were compared on a series of individual target behaviors to children who received only outpatient treatment. The researchers found that only children whose parents had participated in the training program were able to generalize improvements in appropriate behavior to the home setting. With these findings in mind, PT programs have the potential to facilitate the maintenance of previously mastered skills and behavioral outcomes for children.
Effects of PT Interventions
Early intensive behavioral interventions for young children that include PT components have been shown to improve the communication skills, cognitive abilities, behavior, and adaptive functioning of children with ASD (Cohen, Amerine-Dickens, & Smith, 2006; Lovaas, 1987; McEachin, Smith, & Lovaas, 1993; Vismara et al., 2009). For example, Remington et al. (2007) studied outcomes for young children with ASD and their parents following a long-term early intensive behavioral intervention including PT. They reported that the children’s gains in cognitive ability, language skills, adaptive functioning, and positive social behavior demonstrated in their first year of participation maintained at the 2-year follow-up.
Similarly, McEachin et al. (1993) conducted a follow-up study of families who participated in an early intensive behavioral intervention when their children were toddlers, in which therapists instructed parents in all treatment procedures so they could continue therapy in the absence of therapists (Lovaas, 1987). The researchers discovered that the higher IQ scores and levels of adaptive functioning achieved by the children in the intervention group were maintained when children were 11.5 years old. Moreover, 47% of the experimental group had made gains substantial enough to be considered “normal functioning” with placement in general education settings, whereas none of the children in the group receiving a less intensive intervention had achieved such gains (McEachin et al., 1993, p. 367).
In addition to interventions that include parents, other studies have evaluated parent-implemented interventions for young children with ASD, in which parents are the sole interventionists, providing individualized interventions following structured PT programs. These studies have described improvements in young children’s language skills (Harris, Wolchik, & Milch, 1982; Smith, Groen, & Wynn, 2000), cognitive abilities (Sheinkopf & Siegel, 1998; Smith et al., 2000), academic skills (Smith et al., 2000), and problem behavior (Wacker et al., 2013). In addition, reviews of parent-implemented interventions for young children with ASD have shown improvements in children’s social and communicative behavior, as well as enhanced parent–child interactions (McConachie & Diggle, 2007; Meadan, Ostrosky, Zaghlawan, & Yu, 2009). These findings highlight the efficacy of early intensive behavioral intervention programs and present favorable outcomes for children who received interventions delivered by parents.
Although multiple reviews have found that parents are capable of learning techniques and facilitating programming (Matson et al., 1996; McConachie & Diggle, 2007; Suppo & Floyd, 2012), most of the literature reviews to date have focused on programs for families of younger children, and no syntheses have evaluated the effects of PT for school-aged children with ASD. This is unfortunate because older children with ASD continue to experience difficulties, and PT may remain necessary to support families and promote positive outcomes as children age. For example, research indicates the language, behavior, and social deficits present in children with ASD persist into adolescence (Ballaban-Gil, Rapin, Tuchman, & Shinnar, 1996; Seltzer et al., 2003). Furthermore, as children progress into adolescence, caregiving challenges have detrimental effects on parents, whose psychological well-being tends to decrease with increased age of their child (Fong, Wilgosh, & Sobsey, 1993).
Previous reviews on this topic also do not isolate the benefit of including parents in interventions delivered to children. In other words, the effects of PT are confounded because it is delivered as a component of a composite intervention and not on its own. In addition, a wealth of literature provides guidance on including parents in interventions for young children with ASD. Studies have used a variety of methods to train parents, including education, modeling, coaching, written materials, and technology, leading to changes in a diverse set of behaviors in young children with ASD. However, the literature supporting similar programs for older children with ASD has received less attention in the literature.
Purpose
As indicated above, we did not identify any systematic reviews that examine the inclusion of PT in interventions for school-age children with ASD. It is currently unclear what techniques are being used to instruct parents of older children with ASD, how parents are involved in interventions, or what child outcomes the programs target. In addition, no reviews have attempted to isolate the benefits of including parents in interventions delivered to school-age children with ASD. Therefore, the primary purpose of this synthesis is to describe the studies in this promising area and to evaluate the added value of including parents in interventions delivered to school-aged children with ASD. Within this review, our subquestions are (a) What is the current state of the literature regarding including PT in interventions delivered to school-age children with ASD; (b) In terms of child outcomes, what is the added benefit of including parents in interventions; and (c) Do the effects of interventions with a PT component vary across different child skill areas or behavioral outcomes?
Method
Following a search of two databases and reviews of PT plus an ancestral search, 16 articles reporting on 15 studies were analyzed in terms of study design, participant characteristics, purpose and characteristics of the interventions, and outcome measures. ESs were calculated for each study and further collapsed into categories. Due to the small sample of studies, effects were not analyzed using inferential statistics.
Literature Search
We first established eligibility requirements for articles that would be considered for inclusion in the review. Our selection criteria were developed based on the definition of PT described by Bearss, Burrell, Stewart, and Scahill (2015) and the inclusionary criteria used in previous reviews of PT programs for children with ASD (e.g., Brookman-Frazee, Stahmer, Baker-Ericzen, & Tsai, 2006; Schultz, Schmidt, & Stichter, 2011). Articles must have (a) been published in English, peer-reviewed journals; (b) been experimental or quasi-experimental in nature, which included both studies with a control group and single-case designs; (c) included training parents as a component of the intervention, with a description of PT program characteristics, such as degree of parental involvement, strategies used to instruct parents, and/or content of the training (e.g., studies mentioning the use of PT without describing either the topic, instructional strategies, or dosage of PT were excluded); (d) included children with ASD (diagnosed with ASD, autism, autistic disorder, pervasive developmental disorder–not otherwise specified [PDD-NOS], high-functioning autism [HFA], or Asperger disorder, as reported by the authors) aged 6 to 17 years as participants, with a mean age between 6 and 17 years or disaggregate findings by age and/or disability category so that only those meeting our criteria could be included in our analysis; and (e) reported quantitative child outcome data from a direct assessment or parent, child, or teacher report. Studies including diagnostic status, disorder severity, or clinical improvement as the sole outcome variable were excluded, given the secondary nature of these clinician report measures. In addition, studies must have been published in or after 1987, coinciding with the publication of the Diagnostic and Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-III-R; APA, 1987), which removed the infantile ASD diagnosis, included a more expansive definition of ASD, and established a checklist of diagnostic criteria. Studies must also have been conducted within the United States. Those carried out in other countries were excluded due to the cultural nature of parenting and perceptions of disability, and the influence of cultural differences on the success of PT (Santarelli, Koegel, Casas, & Koegel, 2001).
Studies were located in three ways. We conducted “all text” searches of two databases, ERIC ProQuest and PsycINFO, using the terms ASD and parent training or parent-mediated or parent-implemented or parent education. In line with our research questions and interest in the value added by including parents in interventions delivered to children, studies in which parents were the sole interventionists were excluded. Results were restricted to articles published in scholarly, peer-reviewed journals. PsycINFO search options were used to limit results to those reported in experimental articles with study participants aged 6 to 17 years. The database searches yielded a total of 377 possible studies. After examining article abstracts using our inclusion criteria and eliminating duplicate results, 82 studies remained.
Next, we reviewed the full-text articles to examine whether they met the inclusion criteria. Through this process, 67 articles were excluded for the following reasons: Twenty-nine articles were excluded because they did not describe studies conducted exclusively within the United States. Twenty-three studies included a sample with a mean age less than 6 years, and did not disaggregate their findings by age. Nine studies were excluded because researchers used parents as the primary interventionists, rather than including parents in interventions delivered to children. One study (George, Oriel, Blatt, & Marchese, 2011) included participants with various disabilities and did not disaggregate results according to disability category, and one additional study (Elder, 1995) included individuals displaying “autistic features” rather than with ASD diagnoses. Four articles were not evaluations of interventions including PT, but rather summarized findings from studies already included in the review (Farmer et al., 2012), outlined the characteristics of children receiving community mental health services (Brookman-Frazee, Taylor, & Garland, 2010), or described the piloting of a newly developed outcome measure used in a PT program evaluation (Handen et al., 2013; Johnson et al., 2009). From the original corpus, 15 studies met the final inclusion criteria. Using the same procedures, all searches were repeated by two coders, who reviewed the potential articles to evaluate whether each study met the inclusionary criteria. Coders agreed on the inclusion and exclusion of all potential articles.
Subsequently, we examined studies within the reference lists of previous reviews that evaluated PT interventions for children with ASD (Bearss et al., 2015; Brookman-Frazee et al., 2006; Matson, Mahan, & Matson, 2009; Patterson, Smith, & Mirenda, 2012; Schultz et al., 2011; Suppo & Floyd, 2012). Last, we conducted an ancestral search by examining the reference lists of the studies to be included in the review. These searches contributed one additional study, resulting in a final corpus of 16 articles. Given that two articles reported on multiple group comparisons and three articles described additional variables from studies already included in the analysis (combined into one study for the purposes of this review), in total the review includes 15 unique comparisons. Although we had intended to include studies with single-case designs, no such studies included a PT component in an intervention delivered to children by clinicians; all reported on parent-implemented interventions and consequently do not contribute to understanding the benefit of including PT in interventions conducted with children with ASD. Therefore, all 16 articles in this review employ designs with experimental and control groups.
Coding Procedures
Articles were initially coded for nine study elements. Design described whether participants were randomly assigned to treatment and control groups (1 = quasi-experimental design, 2 = experimental design). Child participants included numerical descriptors such as number of participants; age range; mean age; and percentage diagnosed with autism, ASD, Asperger disorder, HFA, and PDD-NOS. Purpose of the intervention described the treatment administered to child participants, whereas topic of PT indicated the purpose of the treatment given to parents (1 = social functioning, 2 = communication, 3 = emotion identification or regulation, 4 = behavior change, 5 = adaptive functioning, 6 = medication trial). Codes regarding purpose and topic were developed after reviewing each article, and detailed definitions of these codes are available from the primary author upon request. Each study was numerically coded using continuous variables in terms of duration (weeks), frequency (sessions per week), and intensity (minutes per session) of PT. Format of PT described the delivery of PT sessions (1 = individually with parent or family, 2 = group) and sessions attended indicated how many PT sessions were actually attended by parents. Treatment integrity described whether and how the researchers measured parents’ adherence to PT when intervening with their children (0 = no, 1 = informally measured, 2 = formally measured). Outcome described the variable assessed by each measure (1 = social functioning, 2 = communication, 3 = emotion identification or regulation, 4 = behavior change, 5 = adaptive functioning), which was coded independently of an intervention’s purpose because studies often assessed outcomes indirectly related to the principal purpose of the intervention. These codes were developed after reviewing the outcomes measured in each study and collapsing them into categories. Definitions of each outcome category are available from the primary author upon request. Data source indicated the method by which information was obtained on each measure (1 = direct assessment or observation of child, 2 = parent report, 3 = child report, 4 = teacher report, 5 = treatment program staff report). Studies in the final sample were coded by two raters. Initial interrater reliability across all studies was 98.6%. All discrepancies were resolved during coding sessions, with reconciled codes used in all subsequent analyses.
ES Calculation
ESs were calculated as the standardized mean difference between treatment (t) and control (c) groups. Therefore, only dependent measures presented using means and standard deviations were included. We used the standard formula for Cohen’s d by subtracting the control mean from the treatment mean and dividing by the pooled standard deviation. All ESs were calculated using Comprehensive Meta-Analysis (CMA) software (Version 2; 2014).
Analysis
First, an ES (Cohen’s d) was calculated for each dependent measure. Then, ESs for each outcome category within each study were calculated. When studies included more than one dependent measure per outcome category, the ESs for all dependent measures were averaged. Next, ESs for outcomes within each study were collapsed to calculate an overall study ES. Finally, using the CMA software, all standardized mean differences were scaled to Hedges g to account for small sample sizes, which is the ES used in all subsequent analyses. ESs were calculated for each of the three types of intervention by averaging the overall ESs for each study within an intervention category. Furthermore, ESs for each outcome were collapsed within intervention categories to estimate an effect of each intervention on particular outcomes. In meta-analytic research, the next step would typically be to analyze mediating variables to explain the significant variability using Hedges (1982) equivalent to the ANOVA or modified weighted regression (Hedges & Olkin, 1985). However, these analyses are not appropriate in this review given the small number of studies. Therefore, we examined our research questions via a descriptive examination of weighted means and CIs, provided that each category consisted of at least two ESs.
Publication Bias
We conducted two analyses to test for publication bias, including Orwin’s (1983) fail-safe N, which indicates the number of unpublished studies with insignificant mean ESs that would need to be included in an analysis in order for the cumulative effect to become trivial. We also constructed a funnel plot and conducted Egger’s test (Egger, Smith, Schneider, & Minder, 1997) to detect possible asymmetry within the group of studies included in our analysis. Orwin’s (1983) fail-safe N indicated 28 unpublished studies with a mean ES of 0.00 would need to be included in the analysis to reduce the observed ES to 0.20. Egger’s test (Egger et al., 1997) resulted in a two-tailed p value of 0.16, indicating symmetry exists in the funnel plot and that there is no significant publication bias in the studies included in our analysis.
Results
Results are presented in four sections. First, the participants and interventions used in each study are described. Second, the added benefit of PT is analyzed, including effects by child outcome. Last, overall effects and effects by outcome are analyzed by type of intervention. See Table 1 for detailed information regarding all studies included in the review, and see Table 2 for mean ESs, standard errors, and CIs.
Studies Including Parent Training Interventions for School-Age Children With ASD.

Note. ADHD = attention-deficit/hyperactivity disorder; AS = Asperger syndrome; ASD = autism spectrum disorder; HFA = high-functioning autism; HFASD = high-functioning autism spectrum disorder; NR = not reported; PDD-NOS = pervasive developmental disorder–not otherwise specified; PT = parent training; RUPP = Research Units on Pediatric Psychopharmacology.
Effect Sizes by Dependent Variable Category and Overall.
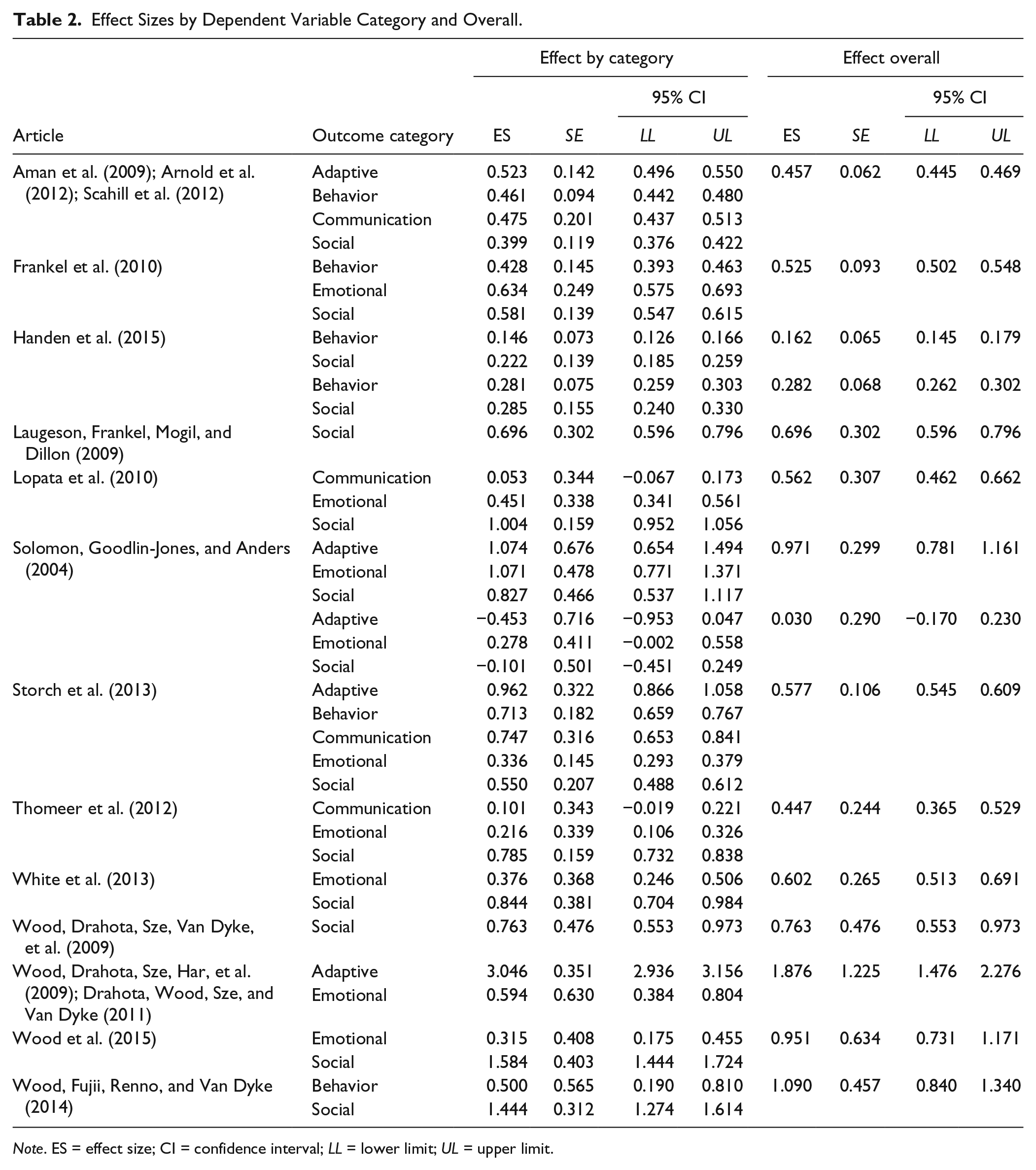
Note. ES = effect size; CI = confidence interval; LL = lower limit; UL = upper limit.
Participants
Collectively, the 15 studies included a total of 622 child participants (M = 41.47, SD = 29.66), all diagnosed with ASD, but sample sizes were generally small. Of the 15 studies, only six included samples of 40 or more participants. All studies reported including participants diagnosed with autism or ASD, Asperger disorder, HFA, and PDD-NOS. Two studies (Frankel et al., 2010; Wood, Drahota, Sze, Van Dyke, et al., 2009) did not report the percentages of participants diagnosed with each disorder, but the remainder of the participants were mostly children diagnosed with ASD or autism (40.0%), PDD-NOS (27.5%), and HFA (27.1%). Given that studies must have included participants with a mean age between 6 and 17 years, participants across all studies ranged from 4.0 to 17.0 years old (M = 12.5).
Interventions
Of the 15 interventions delivered to children, most were described as social skills training (n = 6) or cognitive behavioral therapy (CBT; n = 6). Social skills programs focused on behaviors such as friend-making, conversation skills, and social etiquette, whereas CBT interventions tended to focus primarily on emotional regulation, coping skills, and identification of emotions. However, CBT interventions often also included aspects of social skills training, such as perspective-taking and friendship skills. Three studies were medication trials, investigating the effectiveness of risperidone or atomoxetine. Interventions were delivered for a range of 10 to 24 weeks, with 1 to 25 sessions per week, for 60 to 90 min per session. As described by the researchers, studies targeted participants social/emotional adjustment (n = 5), social skills (n = 4), problem behavior (n = 3), adaptive skills (n = 2), or emotional identification/regulation skills (n = 1).
The purposes of PT interventions mirrored the purposes of the interventions delivered to children and were delivered for similar durations. PT sessions took place between 0.71 and 1 time per week, most for 60 to 90 min. Studies used between one and nine strategies to instruct parents. Where no strategies were mentioned, the PT program was coded as including only lecture and/or discussion, as this is the most general PT strategy and is routinely included in all PT programs. Strategies used to instruct parents included lecture and/or discussion (n = 14), homework assignments (n = 7), providing written materials (n = 5), data collection instruction (n = 5), practice and/or role-play (n = 3), watching videos (n = 3), home visits (n = 3), phone calls (n = 2), and feedback and/or in-situation coaching (n = 1). PT interventions were typically provided in a one-on-one setting with the parent or family (n = 9) as compared with being offered in a group format (n = 6). Four studies included the actual number of PT sessions attended, reporting about an 85% attendance rate, on average. No studies included formal measures of treatment integrity for parent implementation of strategies learned.
Added Benefit of PT
The three studies that examined the added benefit of PT, in that they compared groups of children receiving an intervention plus PT to groups of children receiving the intervention without PT (Aman et al., 2015; Arnold et al., 2012; Handen et al., 2015; Scahill et al., 2012), included 252 child participants, collectively. Handen and colleagues (2015) reported two unique studies, comparing a medication and PT group to a medication only group and a placebo plus PT group to a placebo only group. Scahill and colleagues (2012) examined data on an additional variable from participants in the Aman et al. (2009) study, and Arnold and colleagues (2012) conducted a follow-up of the same participants. Therefore, the Handen et al. article was considered as containing two studies, and the Aman et al., Arnold et al., and Scahill et al. articles were considered as reporting on one study. Across the three studies, whereas child participants received either medication, placebo, or no medication, parents participated in PT on behavior management strategies following the Research Units on Pediatric Psychopharmacology (RUPP) Autism Network model, which offered between 9 and 17 individualized sessions of PT, 60 to 90 min in length, over 10 to 24 weeks, including lecture and discussion, practice, role-play, written materials, coaching, data collection instruction, video models, homework assignments, home visits, and follow-up phone calls. Studies obtained an overall ES of 0.33, 95% CI [0.05, 0.61] in the comparison of interventions delivered to children with and without PT components. Only one of these studies examined the impact of PT on communication skills and adaptive skills, so aggregated comparisons were not possible for these outcomes. However, all three studies reported on social skill improvement and emotional identification and regulation outcomes, demonstrating an ES of 0.32, 95% CI [0.04, 0.60], on social skills and an ES of 0.33, 95% CI [0.04, 0.61], on emotional identification/regulation skills.
Effects by Intervention Type
Social skills training programs
Studies evaluating the effects of social skills training programs (n = 6) obtained an overall ES of 0.53, 95% CI [0.25, 0.82]. Effects were also estimated for each outcome area. Studies (n = 6) demonstrated an ES of 0.67, 95% CI [0.39, 0.96], for social skills. In the area of emotional identification/regulation, studies (n = 5) obtained an ES of 0.49, 95% CI [0.18, 0.80]. However, a unique effect for the PT programs in these interventions cannot be determined, given that the effects are confounded with the interventions delivered to the participants, and comparisons are made with control groups who received treatment as usual, not the intervention minus PT.
Cognitive behavioral therapy (CBT)
Studies evaluating CBT interventions (n = 6) obtained an overall ES of 0.91, 95% CI [0.52, 1.30]. In the analysis of individual outcome categories, the six CBT intervention studies demonstrated an ES of 0.67, 95% CI [0.39, 0.96], on social skills and five studies indicated an ES of 0.49, 95% CI [0.18, 0.80], on emotional identification and regulation skills. As mentioned above, effects for the PT portions of these interventions cannot be estimated.
Discussion
The purpose of this review was to examine the inclusion of PT within interventions for school-aged children with ASD. We identified and reviewed a total of 15 articles published between 1987 and 2016. The majority of child participants were diagnosed with autism or ASD, and the mean age of participants was 12.5 years. Interventions directed at children took place for between 5 and 24 weeks, typically in 60- to 90-min sessions, delivered about once per week, with some interventions offering as many as 25 sessions per week. Generally, PT was part of these interventions for one 60- to 90-min session per week. Unfortunately, not all studies included specific information regarding the extent to which parents were involved in interventions, and no studies described treatment integrity on the part of the parents. However, where reported, the degree of parental involvement varied widely across studies. For example, Lopata and colleagues (2010) asked parents to participate in only five PT sessions, and the actual instructional activities in which parents participated are not described. In contrast, Aman and colleagues (2009) offered parents 17 PT meetings involving nine different instructional activities.
PT sessions included between one and nine strategies to instruct parents. Overall, instructional strategies used were of low intensity and required little parental engagement. Across all studies, the most common instructional strategy used in PT was lecture and/or discussion. High-intensity strategies, such as feedback, in-situation coaching, and practice or role-play were used less frequently. Unfortunately, comparisons between studies including different PT components were not possible given the small sample size. However, other research indicates strategies used to teach parents have varying effects on parents’ skills and children’s outcomes. For example, in a meta-analysis of PT for parents of children with behavior problems (Kaminski, Valle, Filene, & Boyle, 2008), studies of programs using different strategies to teach parents demonstrated varying ESs. In terms of improving parenting skills and behaviors, studies including manuals (ES = 0.38), homework assignments (ES = 0.39), role-playing (ES = 0.45), and practicing with one’s own child (ES = 0.91) led to different results.
Most PT interventions were conducted in a one-to-one setting, and interventions were primarily aimed at changing social/emotional adjustment, social skills, problem behavior, or adaptive skills. This finding is similar to those of other reviews (Bearss et al., 2015; Patterson et al., 2012; Schultz et al., 2011), which found PT tended to focus on alleviating the core symptoms of ASD, such as communication, socialization, and behavior. Similarly, in a review of single-case design studies of PT for families of children with ASD (Patterson et al., 2012), most studies concentrated on social skill and communication outcomes. The studies included in these previous reviews focused on interventions for children younger than 5 years old, indicating that similar skills are being targeted in programs intended for both young and older children with ASD. Several studies in the current review, however, focused on children’s emotional identification and regulation skills, reflecting an area in which older children’s deficits may prove more critical than for younger children with ASD.
Where reported (n = 4), attendance rates at PT sessions were generally low, with parents attending about 85% of training sessions offered. Considering that parental attendance was rarely reported and bearing in mind the potential value of PT, we consider the rate of parental attendance problematic. In addition, in the three studies isolating the effects of including parents in interventions, described by Aman and colleagues (2009) and Handen and colleagues (2015), over 20% of families withdrew from treatment, many citing burden due to participation and lack of efficacy. Similarly, in a review of PT programs for families of children with ASD, Matson et al. (2009) noted significantly high dropout rates. Given that parent perceptions regarding the effectiveness of PT programs is linked to dropout rates (Forehand, Middlebrook, Rogers, & Steffe, 1983), the design of PT procedures that parents feel are efficient, effective, generalizable, and easily fit into families’ lifestyles and routines is especially critical to parental participation. Furthermore, no studies in the current review included formal measures of parent treatment integrity. Previous research, however, suggests treatment integrity is widely variable, which may affect the success of PT. For example, Patterson et al. (2012) found that of the single-case design studies reviewed that included direct measures of parental treatment integrity, rates varied from 20% to 100%.
Across the studies isolating the added value of PT interventions (n = 3), a mean ES of 0.33 was obtained, indicating a small positive effect on children’s outcomes. In addition, for studies isolating the benefit of PT, effects on social skills (ES = 0.32) and emotional identification and regulation skills (ES = 0.33) were small but positive, suggesting that parental involvement in interventions continues to have the potential to change these outcomes as children age. Notably, these ESs represent the value added to effective interventions by including parents, and not a comparison between interventions with PT and no treatment. These findings suggest including a PT component in interventions for school-age children with ASD may improve children’s outcomes beyond what would be expected following the same interventions without PT.
The remaining studies, which included PT as part of a multicomponent intervention, were categorized as either social skills (n = 6) or CBT (n = 6) interventions. An effect for the PT component in the social skills training and CBT intervention studies cannot be determined, given that the effects are confounded by the interventions delivered to children and comparisons are made with control groups who received treatment as usual, not the intervention minus PT. However, comparisons can be made between these studies and other studies of similar programs. A meta-analysis of 69 afterschool social skills programs for children and adolescents indicated an ES of 0.34 for programs using recommended social skills training practices (Durlak, Weissberg, & Pachan, 2010). This effect is slightly smaller than the ES of 0.53 obtained from the social skills studies with PT components included in this review. The social skills program meta-analysis by Durlak et al. (2010) also indicated an ES of 0.19 on positive social behaviors, compared with the studies in this review, which demonstrated an ES of 0.67 on social skills. In addition, a meta-analysis of psychotherapy techniques for children and adolescents (Weisz, Weiss, Han, Granger, & Morton, 1995) demonstrated an ES of 0.57 for CBT interventions, whereas the studies of CBT with PT in this review obtained an ES of 0.91. These findings suggest that including PT within these interventions may be more effective than the interventions delivered to children alone. However, the comparison meta-analyses above did not focus on children with ASD, and more research is needed to understand the benefit of including a PT component in social skill and CBT interventions for older children with ASD.
Limitations
There are several limitations to this review and meta-analysis. First, only 15 studies met our criteria for review, making comparisons among and between study variables difficult. For example, comparisons of studies using different populations and various PT instructional strategies were not possible given the small sample size. The small number of articles also meant studies with differing intervention characteristics were collapsed into one category as we looked for commonalities among studies. For example, social skills interventions employ a wide range of curricula and instructional strategies, but collapsing them into one category was the most reasonable decision for the purposes of this review. Despite the small sample of studies, however, our findings are strengthened by the fact that the combined studies included 622 participants.
Second, we did not use indicators of methodological quality as criteria for analysis. However, the small sample of studies and lack of detailed information provided regarding the characteristics of interventions would have made such an approach problematic. In addition, no included studies measured treatment fidelity of parents’ implementation of the skills and behaviors taught during PT, making interpretation of the findings difficult. Similarly, the extent to which parents were involved in interventions was widely variable and often unclear, further complicating the interpretation of our findings. It is also important to recognize ASD as a spectrum, in that the participants included in this analysis likely display a variety of characteristics and degrees of impairment. Therefore, it is inappropriate to make a generalized statement regarding the effectiveness of PT interventions for school-age children with ASD based on these findings. In addition, we did not contact authors or experts in the field to locate articles for inclusion, nor did we include gray literature in our analysis. However, we conducted two analyses to test for publication bias, concluding there was no significant bias in our analysis.
Implications and Recommendations for Future Research
There are several practical implications from this analysis. First, results indicate that PT may be a worthwhile component to include in interventions for families of school-aged children with ASD. However, given the small number of studies on the topic, additional research is needed to evaluate the effectiveness of these programs, especially in terms of the added benefit of PT over interventions delivered only to children. Second, given the moderate rates of parental attendance at PT sessions, additional research is needed to understand factors related to the lack of adherence to treatment and how to design the most efficacious PT programs to encourage continued parental participation. To this end, previous PT research recommends the development of PT programs that address families’ needs through providing culturally and linguistically sensitive interventions that consider parent stress and other contextual variables as barriers to parental participation and fit into families’ lifestyle and daily routines (Steiner, Koegel, Koegel, & Ence, 2012). Similarly, it is currently unclear which PT components have the largest effect on child outcomes. Last, future research should incorporate measures of parent treatment integrity, as no studies in this review included such measures, and differing levels of parent treatment integrity may contribute to varying outcomes of PT interventions across studies.
Existing research has documented the value of PT for young children with ASD and their parents. However, we located relatively few studies of interventions for older children with ASD that included a PT component. In addition, limitations in several of the included studies (e.g., small sample sizes, lack of parent treatment fidelity data, and limited descriptions of PT procedures) make it difficult to draw firm conclusions regarding the value of including a PT component in interventions for school-age children with ASD. Future researchers should design studies to more definitively address the benefits of including a PT component for this population of learners and related issues such as whether the developers of interventions perceive PT as less valuable as children age or whether parents are less willing to participate in interventions when their children reach school age.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.