
Abstract
When youth experience psychosocial difficulties, multiple sectors of care may intervene. The present study examined the prevalence and sociodemographic predictors of multisector involvement related to psychosocial difficulties among adolescents with disabilities. Using a nationally representative sample of 9,230 students who participated in the National Longitudinal Transition Study–2, we estimated students’ rates of involvement in school, health, social service, and juvenile justice sectors and used logistic regression models to ascertain the relations to student characteristics. Students with disabilities were frequently involved with a variety of sectors of care, but schools remain the primary provider. Multisector involvement was commonplace, particularly for adolescents with emotional disturbance or autism. Disability and insurance type consistently predicted involvement of each sector, but other sociodemographic characteristics commonly related to disparities in involvement were not significant in most of our models. Communication and collaboration across systems can support the school-based problem solving and individualized planning for students with disabilities.
Psychosocial difficulties are common among adolescents, and when they occur, one or more sectors of care may intervene in a variety of ways—from receipt of behavioral, psychological, medical, or social work services in a range of settings, to arrest, detention, and monitoring—in response to impaired functioning, inappropriate behavior, or risk. These sectors, including education, health care, social services, and juvenile justice, represent the primary institutions responsible for prevention and intervention services to support children’s and youths’ well-being. Because psychosocial difficulties and treatment needs often increase with age (Merikangas, Avenevoli, Costello, Koretz, & Kessler, 2009), for students with disabilities, understanding multisector involvement may support large-scale efforts to foster communication and collaboration with providers conducive to positive student outcomes. Comorbid psychosocial difficulties and psychiatric disorders are especially common among adolescents with disabilities (see Note 1; for example, Rohde, Lewinsohn, & Seeley, 1991; Simonoff et al., 2008; Willcutt & Pennington, 2000), but we know little about their involvement in sectors of care beyond special education. As such, the present study examined patterns and predictors of multisector involvement among adolescents with disabilities in a nationally representative sample.
Students with disabilities, who currently represent 8.5% of the U.S. student population (U.S. Department of Education, 2015), warrant attention in the discourse surrounding multisector involvement and mental health treatment access given the long-term consequences of inadequate services and broader health care disparities that disadvantage individuals with disabilities (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014). Furthermore, disabilities, psychosocial difficulties, and mental disorders frequently co-occur. Among students with high-incidence disabilities (i.e., emotional disturbance, learning disabilities, other health impairments, speech–language impairments, and intellectual disability), one in five students are identified with secondary disabilities (De Valenzuela, Copeland, Qi, & Park, 2006) and nearly half of students with disabilities may also experience mental disorders (e.g., Matson & Shoemaker, 2009). It is likely many of these youth present with complex behaviors and needs that spur involvement in multiple sectors of care beyond education, but little is actually known about involvement or services received by adolescents with disabilities.
Multiple care sectors provide services for youth with psychosocial or mental health difficulties. Among the most commonly involved sectors are education, health, juvenile justice, and social services (Costello, He, Sampson, Kessler, & Merikangas, 2014), and youth may be involved in sectors simultaneously or sequentially (Dauber & Hogue, 2011). School services may take a variety of forms, including behavioral, psychological, or social work services to provide or facilitate behavioral modification, positive behavior supports, counseling, or other social–emotional interventions (e.g., conflict resolution, crisis management, social-skills training). Health services for psychosocial difficulties may include prevention and intervention services from a variety of mental health providers, including psychologists, behavioral therapists, counselors, psychiatrists, and others. Health services often include pharmacotherapy, or medication management of psychosocial difficulties prescribed by health service providers. In the case of severe difficulties, individuals may receive inpatient treatment in medical or mental health facilities. Social services include a range of governmental services to support individual, family, and community well-being via direct services to prevent or improve health and social problems such as child welfare, youth programs, financial assistance, counseling services, and out-of-home placements (National Association of Social Workers [NASW], 2011). Children and youth may be engaged in this sector as a result of their own behavioral or social difficulties, or as a result of family discord, neglect, or abuse, which is a significant risk factor for psychosocial difficulties. Social workers engage in a range of roles within social services, from case management, assessment and counseling for psychosocial difficulties, and coordination and management of out-of-home placements (NASW, 2011). Services may be provided in home, community, or residential settings.
The juvenile justice system is another common care sector in which adolescents who experience psychosocial difficulties may engage when their behavior violates local laws; involvement ranges from arrest to incarceration and probation or parole, as well as diversion programs that emphasize rehabilitation and treatment. Delinquency is recognized as an outcome of maladaptive adjustment or behavior during interrelated neurobiological and psychosocial processes of adolescence (Barbot & Hunter, 2012; Ezinga, Weerman, Westenberg, & Bijleveld, 2008). Youth with mental disorders and disabilities are at elevated risk for involvement in juvenile justice with estimates as high as 80% of incarcerated youth having a diagnosable disorder or disability (Barbot & Hunter, 2012). Only 15% of detained or incarcerated adolescents receive psychological treatment (Zajac, Sheidow, & Davis, 2015), however, despite legal standards for care referencing treatment options such as pharmacotherapy, treatment for chemical dependency, and adequate mental health services (Zerby &Thomas, 2006).
Estimates of sector involvement vary depending on the population and definition. For instance, results of the 2008 National Survey on Drug Use and Health indicated that approximately 11.8% of all adolescents received mental health services via their schools, 12.7% via specialty mental health providers, 2.9% via medical providers, and 5.3% in multiple sectors simultaneously (SAMHSA, 2009). In addition, approximately 7% of adolescents were prescribed psychotropic medications (National Center for Health Statistics, 2015), but rates are 2 to 3 times higher among adolescents with disabilities, suggesting elevated behavioral and mental health needs compared with peers without disabilities (Sullivan & Sadeh, 2015). Yet, some district data suggest only 7% of students with disabilities receive school-based mental health services through their individualized education programs (IEP; Santiago, Kataoka, Forness, & Miranda, 2014), compared with nearly 13% of students in the general population who are reported to receive school-based mental health services (SAMHSA, 2009). Other population estimates derived from the National Comorbidity Survey–Adolescent Supplement (NCS-A) in the early 2000s suggest that as much as a quarter of students receive some form of mental health services in schools while 30% to 50% receive services outside of schools, although adolescents with diagnosed disorders may actually have lower rates of services across sectors (e.g., Costello et al., 2014; Tegethoff, Stalujanis, Belardi, & Mainlschmidt, 2014).
Estimates of access to psychosocial treatment in the general population indicate unmet needs are widespread (Costello et al., 2014). The NCS-A indicated approximately 13% of adolescents have at least one Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) mental disorder (Merikangas et al., 2010), yet as many as 80% of such individuals received no mental health services in any sector of care (Jensen et al., 2011). Furthermore, most adolescents demonstrate several years of complex interrelated mental health, behavioral, school, and family problems before they are treated (Anderson, Wright, Smith, & Kooreman, 2007), and there are additional gaps in service related to individuals’ sociodemographic characteristics (Gyamfi, 2004; Power, Eiraldi, Clarke, Mazzuca, & Krain, 2005). In particular, girls and individuals from racial/ethnic minority, rural, uninsured, or low-income households are less likely to receive mental health services (Gyamfi, 2004; Howell & McFeeters, 2008; Power et al., 2005). Higher parent education is associated with lower rates of psychiatric disorders, but higher rates of service utilization (Howard et al., 1996). Thus, individuals with greater propensity for mental health problems and greater need of prevention and intervention services do not sufficiently receive them. These gaps in service access present challenges for educators because untreated psychosocial difficulties negatively affect school performance (Suldo, Gormley, DuPaul, & Anderson-Butcher, 2014). Perhaps unsurprisingly, schools are often the initial delivery point and primary provider of services for youth with psychosocial needs (Costello et al., 2014; Franklin, Kim, Ryan, Kelly, & Montgomery, 2012), yet few educational professionals are appropriately trained or positioned to assist students given limitations of preservice training and shortages of personnel (Cummings, Wen, & Druss, 2013; Stormont, Reinke, & Herman, 2011).
In addition, and possibly due in part, to high rates of comorbid conditions, adolescents with disabilities are at elevated risk for a variety of negative educational and psychosocial outcomes, including suspension, underachievement, school failure, dropout, incarceration, and low rates of independent living and financial stability (Kohli, Sullivan, Sadeh, & Zopluoglu, 2015; Lee & Jonson-Reid, 2009; Loe & Feldman, 2007; Newman et al., 2011; Pandiani, Schacht, & Banks, 2001; U.S. Department of Education, 2015). Multisector, multiagency collaboration may attenuate these risks (Chrvala & Bulger, 1999), as research suggests it bolsters both academic and psychosocial outcomes (Anderson, 2011), and can enhance access to needed services among youth involved in juvenile justice (Zajac et al., 2015). Collaboration is also consistent with the Individuals With Disabilities Education Act (IDEA), wherein evaluation procedures and services rendered for special education needs must be comprehensive and individualized, and should involve individuals with relevant knowledge of a student’s needs, thus necessitating, for some students, the inclusion of providers from other sectors in evaluation and planning. Understanding the multisector involvement of adolescents with disabilities is one step toward improving broader efforts to improve collaborative endeavors to support the diverse needs of students with disabilities. The present study examined rates and sociodemographic predictors of multisector involvement in a nationally representative sample of adolescents with disabilities. Because of the policy emphasis on and potential value of multidisciplinary collaboration in appropriately individualizing assessment, intervention, and transition planning (Johnson, 2004), findings on patterns in students’ multisector involvement can enhance our understanding of the complexity of students’ support needs and help inform practices to bolster inclusion of appropriate participants in multidisciplinary processes, thus enhancing school teams’ efforts to provide effective collaborative services.
Method
Data Source and Sample
This study entailed secondary analysis of the National Longitudinal Transition Study–2 (NLTS2), a nationally representative longitudinal study of adolescents with disabilities served under the IDEA. The U.S. Department of Education sponsored the study to describe characteristics, experiences, and long-term outcomes of adolescents with disabilities from 2000 through 2009 (SRI International [SRI], 2000). The study involved approximately 11,280 adolescents who received special education services, were 13 to 16 years old, and in at least the seventh grade in 2000. The NLTS2 featured a complex sampling scheme of youth stratified by disability, region, and local education agency size and wealth to ensure national representativeness, with oversampling of low-incidence disabilities to ensure adequacy of participation for subgroup analyses (Valdes et al., 2006). Although the age of the data may moderate the sample’s representativeness of the current cohort of adolescents with special needs, the NLTS2 provides the most current large-scale data available on this population and allows comparison with population estimates for mental health needs and treatment of U.S. adolescents (e.g., NCS-A 2001–2004; National Longitudinal Study of Adolescent to Adult Health 2001, 2008), providing for identification of potential disparities affecting adolescents with disabilities.
Five waves of NLTS2 data collection occurred every 2 years for 10 years. Sample weights developed to account for the complex sampling design effects and attrition are detailed elsewhere (SRI, 2008; Wagner, Kutash, Duchnowski, & Epstein, 2005). The analytic sample here consisted of 9,230 students. The cross-wave weighting variable, wt_ANYPY, was used to estimate the U.S. population of adolescents with disabilities who received services related to mental health during high school (N = 2,000,570) as variables were drawn from multiple instruments and waves (as discussed below in measures). The unweighted frequency counts and weighted proportions of the population for other sociodemographic characteristics are shown in Table 1. The mean age of participants was 15.25 years (SD = 0.03 years) at the first wave.
Sociodemographic Characteristics of Adolescents With Disabilities in 2001 (n = 9,230; N = 2,000,570).
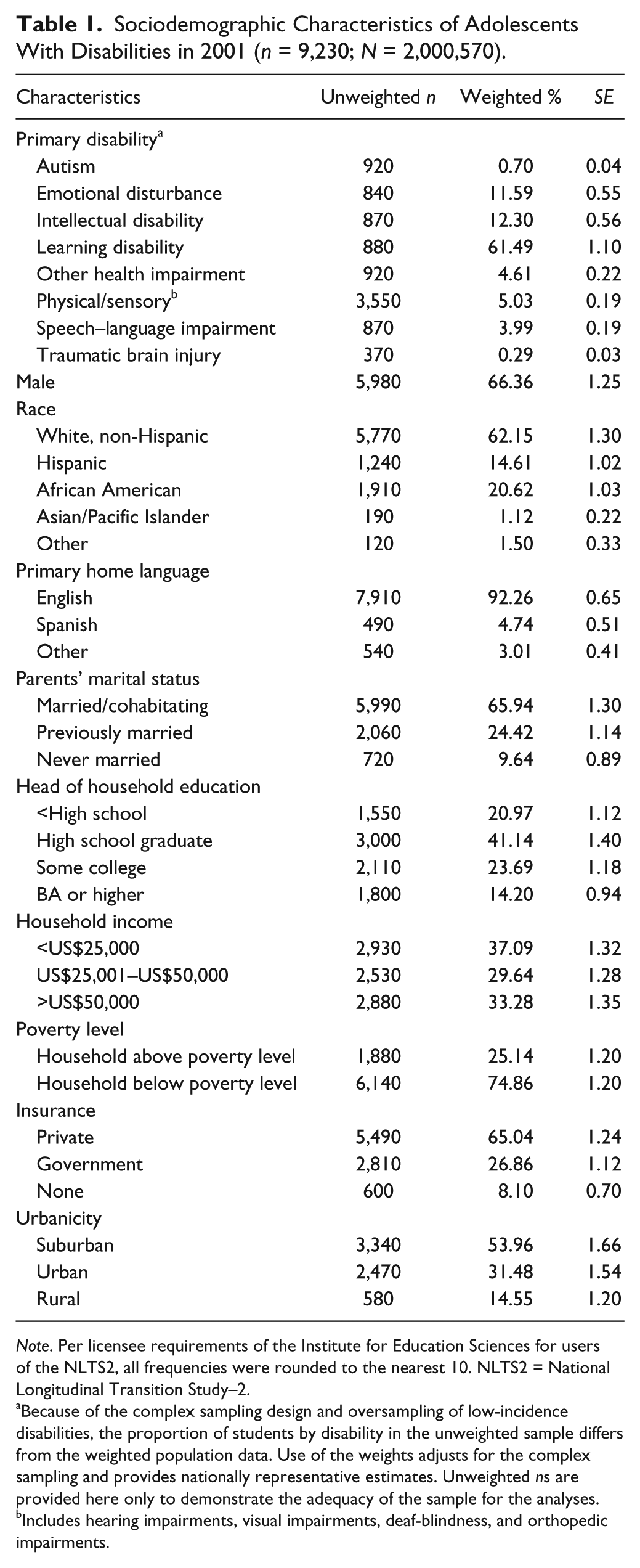
Note. Per licensee requirements of the Institute for Education Sciences for users of the NLTS2, all frequencies were rounded to the nearest 10. NLTS2 = National Longitudinal Transition Study–2.
Because of the complex sampling design and oversampling of low-incidence disabilities, the proportion of students by disability in the unweighted sample differs from the weighted population data. Use of the weights adjusts for the complex sampling and provides nationally representative estimates. Unweighted ns are provided here only to demonstrate the adequacy of the sample for the analyses. bIncludes hearing impairments, visual impairments, deaf-blindness, and orthopedic impairments.
Procedures
The NLTS2’s extensive procedures are detailed elsewhere (SRI, 2000; Wagner et al., 2005). In short, parents provided consent and all procedures were administered by trained personnel. This study utilized NLTS2 measures for student and family sociodemographic characteristics, disability classification, and involvement in school, health, social services, or juvenile justice related to psychosocial difficulties. These data were collected via computer-assisted telephone interviews with parents, paper questionnaires completed by parents and school personnel, and reviews of school records. Prior studies involving reverse record-check methodology demonstrate that parents are reliable reporters of their children’s health-related treatments (Bussing, Mason, Leon, & Sinha, 2003; Pless & Pless, 1995). Data were accessed under a restricted data user license from the Institute of Education Sciences, and the present study was approved by the university’s institutional review board.
Measures
Multisector services
IEP data and parent reports were used to identify the sectors in which their student was involved based on identified services or engagement generally related to psychosocial difficulties: behavioral, psychological, psychiatric, pharmacological, and social work services, as well as arrest and detention. Student cases were dichotomously coded for involvement in the school, health, social service, and juvenile justice sectors if any type of treatment or involvement within it was indicated such that a 1 indicating the student was involved in the sector of care while in high school. We created a categorical variable to assess the total number of sectors involved during high school by summing the sector variables.
Students were coded as involved in the school sector if school program data drawn from the IEP by teacher respondents indicated they had a behavior management program (nprXD3b_06 where X indicates either Wave 1 or 2); behavioral intervention or specialist’s services (nprXD7d); mental health services, counseling, or psychiatric care (nprXD7h); or social work services (npr1D7m); or if the parent indicated the student received mental health services (npXH1b_c) or social work services through the school or district (npXH1b_e). Students were coded as involved in the health sector if the parent reported psychological or mental health services, counseling, or therapy (npXH1b_c) excluding those provided through the school or district; if the parent reported the student took medications for “attention, behavior, activity level, moods” (npXB7c); or if the parent indicated the student had lived in a mental health facility in the previous year (npXA5c_09, npXA5d_09). Students were coded as having social service sector involvement if the parent reported that the student received social work services (npXH1a_e), excluding those provided by the school or district, or if parent indicated out-of-home placement in foster care (npXA5c_04, np1LiveWith) or a group home or assisted living center (np1A5c_07). Students were coded as having juvenile justice involvement if the parent reported that the student had lived in a correctional facility (npXA5c_10) and using the NLTS2 composite variable for arrest, detention, parole, and probation (npXCrimJustice).
Disability
Students’ disabilities were identified from the primary disability on record in the district-provided data (np1DisNum). The analysis included autism, emotional disturbance (ED), intellectual disability (ID), learning disability (LD), other health impairment (OHI), physical/sensory disabilities (a combination of hearing impairments, visual impairments, deaf-blindness, and orthopedic impairments), speech–language impairments (SLI), and traumatic brain injury (TBI).
Sociodemographics
Child and family sociodemographic characteristics were taken from parent interview data that included a continuous measure of the student’s age in 2001, a dichotomous variable for sex (w1_Gend2), and categorical classifications for race/ethnicity (non-Hispanic White, Hispanic, African American, Asian/Pacific Islander; from variable w1_Eth6), primary home language (English, Spanish, other; np1A4b), parents’ marital status (never married, married/cohabitating, previously married; np1K6b), household income (<US$25,000, US$25,001–US$50,000, >US$50,000; w1_Incm3), insurance status (private, government, none; np1HealthIns), and urbanicity (suburban, urban, rural; w1_Urb3).
Analyses
Statistical analyses were performed with the SPSS Complex Samples Module (SPSS version 20.0) which uses Taylor Series adjustments to precisely estimate standard errors, necessary given the NLTS2’s complex sampling design. Response rates varied by instrument and section such that the unweighted subsample for school program survey data on school services was 5,270, whereas approximately 9,000 cases had data from the parent questionnaire on services elsewhere. Using Complex Samples Module, weights and replicate weights were applied to account for the design, attrition, and nonresponse. Regression analyses excluded cases with missing values after weighting.
Rates of sector involvement by type and frequency were estimated using cross-tabulations. Given our interest in determining the relations of student characteristics to involvement in various sectors, which were dichotomous outcomes, multivariate logistic regression models were used to estimate the relations of sector involvement to students’ disability and sociodemographic characteristics, adjusting for age. The regression analyses simultaneously included all disability and sociodemographic correlates. The assumptions for logistic regression are less restrictive than ordinary least squares regression. Appropriate use of logistic regression requires a binary or logistic outcome (i.e., predicting occurrence, rather than nonoccurrence of an event), independent observations, large samples (>50 cases per independent variable), and that all relevant variables are included in the model (Spicer, 2005). Although the latter point cannot be assured, predictors were selected based on significance in studies of the general population, and all predictors were dichotomous or categorical to meet the assumption of linearity of the independent variables and log odds. The general multivariate logistic regression model is expressed as follows:
where
Results
Our purpose was to describe patterns and predictors of multisector involvement among adolescents with disabilities. We begin by reporting descriptive statistics for involvement in sectors of care by disability (see Table 2). Then, we describe the results of the multivariate logistic regression analysis for adolescents’ use of each type of service (see Table 3).
Rates of Sector Involvement by Disability Type.

Note. ED = emotional disturbance; ID = intellectual disability; LD = learning disability; OHI = other health impairment; SLI = speech–language impairment; TBI = traumatic brain injury.
Data on services within the school sector were primarily drawn from the school program survey completed by teachers, which had a much lower response rate than the parent questionnaire data from which health, juvenile justice, and social service data were drawn. Unweighted ns reflect cases with valid data on the applicable items (i.e., not including skipped items or nonresponse). bIncludes hearing impairments, visual impairments, deaf-blindness, and orthopedic impairments.
Correlates of Sector Involvement Among Adolescents With Disabilities.
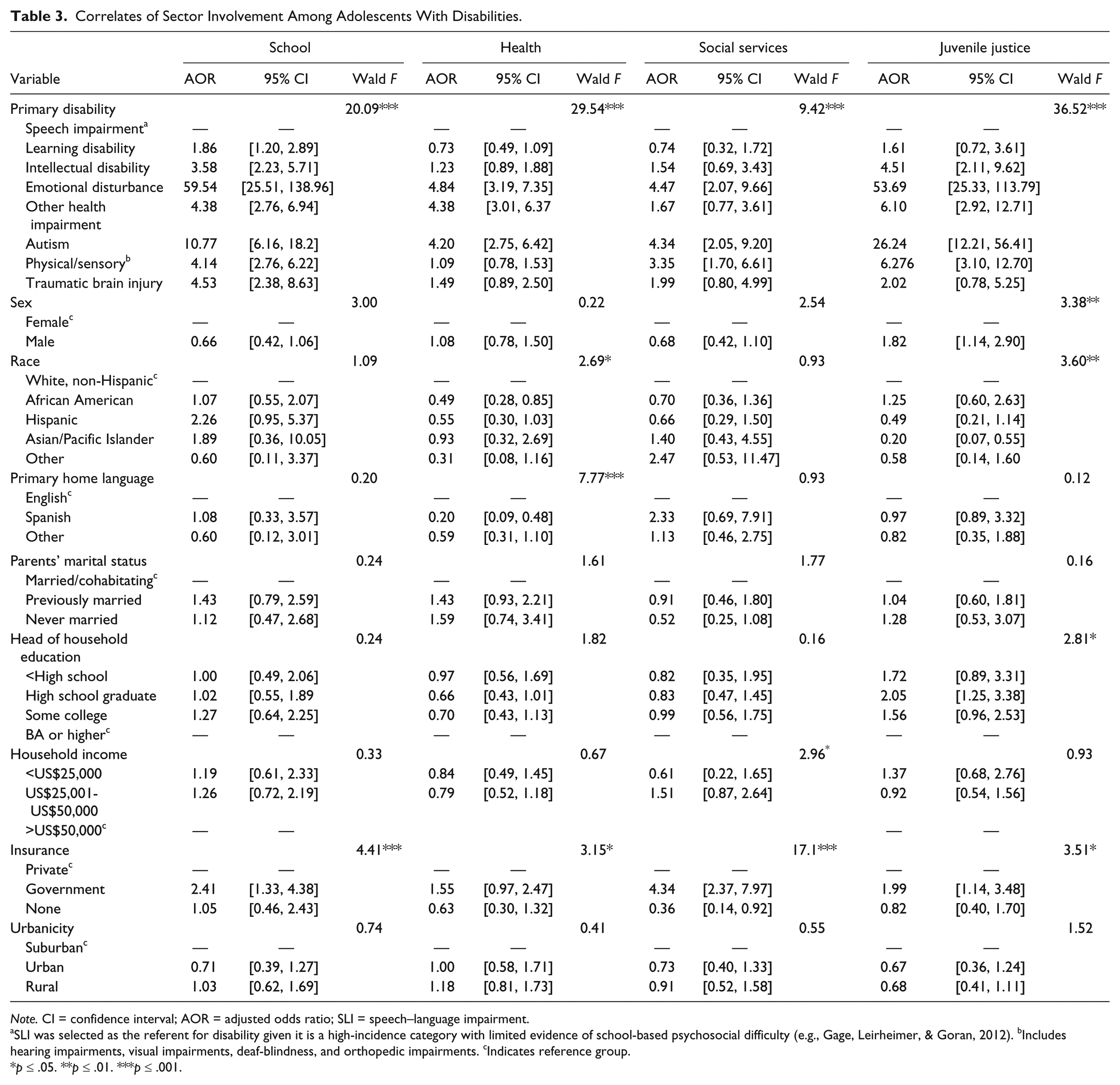
Note. CI = confidence interval; AOR = adjusted odds ratio; SLI = speech–language impairment.
SLI was selected as the referent for disability given it is a high-incidence category with limited evidence of school-based psychosocial difficulty (e.g., Gage, Leirheimer, & Goran, 2012). bIncludes hearing impairments, visual impairments, deaf-blindness, and orthopedic impairments. cIndicates reference group.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Multisector Involvement by Adolescents With Disabilities
Table 2 presents adolescents’ rates of involvement by sector type and number of sectors involved. Across all data sources, reports indicated approximately 54% were involved in at least one sector, with 23% involved in multiple sectors. Of students with disabilities for whom IEP data were provided, a subset of the total sample, 72% received services for psychosocial difficulties, but there were substantial missing data for school services, precluding estimation of the percentage of all adolescents with disabilities who received psychosocial services in the school sector. Data provided by parents indicated that a substantial portion of youth were involved in the health sector (30%), followed by juvenile justice (13%) and social services (7%).
Rates of involvement varied substantially by disability category and were highest among students identified with ED (98%), autism (88%), TBI (80%), and ID (77%). More than half of students identified with autism (60%), OHI (58%), and ED (57%) were also involved in the health sector. Social service involvement was most common among adolescents identified with autism (19%), ED (18%), and physical/sensory disabilities (16%). Students identified as ED were the most likely to be involved in juvenile justice (36%), followed by students identified with OHI and TBI (14%) and LD (11%). Students identified as SLI were the least likely to be involved in any sector related to psychosocial difficulties; 62% had no sector involvement reported. Overall, just less than a quarter of all students with disabilities were involved in multiple sectors, with elevated rates most common among students with ED (61%) and autism (46%). More than one in five students with ED were involved in three or four sectors.
Correlates of Sector Involvement
Disability and sociodemographic correlates of sector involvement are presented in Table 3. The models correctly classified between 70% (school services) and 94% (social services) of cases. Involvement in each sector was consistently predicted by disability type, consistent with the patterns discussed above, as well as by insurance status. Students who received government insurance were most likely to be involved in all sectors relative to students with private insurance, whereas students with no insurance were less likely to be involved in the health, social service, and juvenile justice sectors. Sex predicted only juvenile justice involvement as boys were more likely to be arrested, detained, paroled, or incarcerated than girls (AOR = 1.82). Race predicted health sector involvement, as all racial minority students with disabilities were less likely to be involved in the health sector than White students (Wald F = 2.69, p < .05). Likewise, students from non–English-speaking households were less likely to receive health services (Wald F = 7.77, p < .001). Race also predicted juvenile justice involvement, with Black students with disabilities more likely to be involved (AOR = 1.25) and all other racial minority groups less likely to be involved than White students (Wald F = 3.60, p < .01). Juvenile justice involvement was also predicted by parent education, as students whose parents had less than a college degree were more likely to be involved (Wald F = 2.81, p < .05).
Discussion
Individuals with psychosocial and mental health challenges may engage in a variety of service sectors when they experience psychosocial difficulties that manifest in inappropriate or maladaptive behaviors or functioning. Most common are school, health, social services, and juvenile justice sectors that provide prevention, intervention, punitive, or rehabilitative services. Nationally representative studies have offered insight into service sector involvement of the general population and among adolescents with diagnosed psychiatric conditions (e.g., Costello et al., 2014; Merikangas et al., 2010; Tegethoff et al., 2014), but few studies have considered the experiences of youth with disabilities despite high rates of comorbidity and need. The present study used a nationally representative sample of adolescents with disabilities to provide population estimates of involvement in multiple sectors of care and relations to sociodemographic characteristics.
Multisector Involvement
Schools are the primary sector of care for adolescents with disabilities, as has long been true for the general adolescent population (e.g., Burns et al., 1995; Costello et al., 2014). Earlier research suggested that most youth received services by providers outside of the health sector and most commonly through schools (Burns et al., 1995; SAMHSA, 2009); this is also the case for adolescents with disabilities. Adolescents with disabilities are more likely to be involved in multiple sectors of care than the general population at the same time (Costello et al., 2014). Although rates of health and social service sector involvement were roughly commensurate with population estimates for adolescents generally and those diagnosed disorders (Costello et al., 2014; Tegethoff et al., 2014), our findings indicate higher involvement in juvenile justice. As in the past (Burns et al., 1995), multisector involvement was most common among students with ED and autism, but multisector involvement also typified the experience of approximately one sixth of adolescents with disabilities compared with one tenth of the general population (SAMHSA, 2009). Comparisons must be made with caution, however, because sectors were defined slightly differently in each study. Future research should consider the relations of special needs, diagnoses, and other relevant characteristics to sector involvement using uniform definitions.
Even with relatively high rates of services and multisector involvement, prior research would suggest many students still have unmet needs. Future research with adolescents with disabilities should consider needs relative to access and actual services received, as access alone does not indicate youths’ needs are being met (Jonson-Reid, 2011). For instance, that approximately one in six adolescents with autism and ED were not engaged in any sector may suggest inadequate care or that needs are met through other providers. Researchers should also explore the extent to which common barriers and facilitators of mental health service seeking and utilization (e.g., cost, awareness, stigma, attitudes toward help-seeking; Alegria, Green, McLaughlin, & Loder, 2015; Gulliver, Griffiths, & Christensen, 2010) apply to adolescents with disabilities, and whether there are group-specific mechanisms that affect access and involvement. Analyses of effectiveness and return-on-investment can inform service provision and coordination. Future research should also explore contextual factors, such as policies and infrastructure, which may moderate the relationship between needs and receipt of services.
Correlates of Sector Involvement
This study suggests that for adolescents with disabilities, sociodemographic disparities in access do not characterize school-based services but are common in other sectors as seen in other subpopulations (Costello et al., 2014). Insurance was most consistently related to involvement, likely an indicator of the importance of Medicaid in schools and more broadly. Student and family demographic and socioeconomic characteristics were not consistently related to sector involvement of students with disabilities, although there were racial differences in the health and juvenile justice sectors. Notably, there do not appear to be widespread socioeconomic disparities in sector involvement of adolescents with disabilities, whereas research on mental health parity often shows individuals with low-income have less involvement (e.g., Gyamfi, 2004).
Implications for Practice and Policy
When youths’ psychosocial needs are appropriately supported, their chances of educational success increase (Anderson, 2011). The high rates of involvement of students with disabilities in school-based psychosocial services and in other sectors suggest a high need for support and highlight the need to ensure provision of effective services. Often, school-based services are primarily a gateway to other sectors, rather than themselves supporting improved outcomes (Tegethoff et al., 2014). For adolescents with disabilities, however, schools are the primary provider, underscoring the need to ensure students’ access to school psychologists, social workers, and other school mental health providers and to keep student-to-provider ratios at levels that allow for appropriate provision of intervention and consultation services. School personnel can capitalize on the robust and growing body of research for effective school-based mental health services with high return-on-investment that also support academic outcomes (Suldo et al., 2014). The present results suggest a need to invest in such services to support students with disabilities as most receive one or more behavioral, mental health, or social work services in schools, and many have needs substantial enough to engage in multiple sectors.
Educators can expect that at least one in three adolescents with disabilities are involved in a sector of care outside of school for psychosocial difficulties or risk. Local education policy and practice for individualized services should reflect these trends. For instance, more than a third of adolescents with ED were involved with the juvenile justice system; because of the likelihood of their continued involvement as they move into adulthood and resultant detrimental outcomes, collaboration to support rehabilitation and reduce recidivism is warranted (Maschi, Hatcher, Schwalbe, & Rosato, 2008). Research indicates collaboration and data sharing can improve access to mental health services and bolster outcomes for such youth (Zajac et al., 2015).
Providers from the health, social service, and juvenile justice sectors may make valuable contributions when planning individualizing supports and services. Special educators or other support personnel should proactively ascertain the need for collaboration as many adolescents with disabilities—and 45% to 60% students with autism and ED—are involved with multiple sectors and providers. Thus, the observed patterns here suggest the need for targeted communication and collaboration with some systems for youth with specific disabilities. Involvement in multiple systems is associated with increased risk of poor long-term outcomes, perhaps because it is indicative of pervasive and severe difficulties (Dauber & Hogue, 2011). This risk warrants attention to communication and collaboration across systems to support students’ well-being and enhance the cohesion, efficiency, and effectiveness of the services provided (Anderson, 2011). Fragmented, one-size-fits-all, categorically based (as opposed to need-based) approaches ignore the multidimensionality and complexity of youth’s needs and may hinder positive outcomes.
Communication and collaboration across systems can facilitate problem-solving and intervention processes when students are involved in multiple sectors of care. Outside providers’ participation may range from an ad hoc basis, wherein members of the school team request and share information during assessment and planning processes, to more formal involvement as members of students’ multidisciplinary evaluation or IEP teams. Providers can share information on youths’ needs and services to inform the assessment process and enhance the social validity and coherence of service plans across sectors. For example, a students’ case manager can solicit information about sector of involvement; coordinate meeting logistics to promote participation of family members, the student, and members from various sectors; lead discussion of processes, roles, and responsibilities; provide orientation to identification of needs, goals, and action steps; and ensure proper documentation throughout processes such as evaluations for eligibility and IEP, intervention, and transition planning (for more detailed discussion in the context of wraparound services, see Bruns & Walker, 2008). Outreach and referrals to families may facilitate access to other sectors of care where students demonstrate needs for support beyond the school environment or school providers’ capacity (Green et al., 2013).
In educational systems interested in a systematic approach to collaboration, a systems of care (SOCs) approach has been shown to bolster collaboration and improve educational and mental health outcomes (Anderson, 2011). SOCs is a framework for organizing a continuum of mental health services, and are intended to support youth with complex, long-term needs who can benefit from coordinated, sustained intervention (Anderson et al., 2007), of which many adolescents with disabilities qualify. Furthermore, the guiding principles of the team-based SOC framework—services should be strength based, goal directed, family driven, community based, and culturally competent—are consistent with the spirit of IDEA and can be integrated into or designed to extend students’ IEPs (Anderson et al., 2007). SOCs have been found to enhance professionals’ communication and collaboration across sectors, and foster improve educational and mental health outcomes of participating students (Anderson et al., 2007). SOCs may also facilitate adolescents with disabilities’ requisite transition planning given the importance of ongoing communication, information sharing, joint planning teams, and collaborative service planning and delivery to supporting students’ postschool outcomes (Johnson, 2004). A related approach is wraparound services intended to promote services in the least restrictive environment through multidisciplinary team coordination, family assistance, and development of support networks, which can be especially beneficial in reducing recidivism among youth involved in juvenile justice (Zajac et al., 2015) and improving psychosocial outcomes of children and adolescents with emotional and behavioral disorders (Suter & Bruns, 2008).
Limitations and Future Directions
This study provides insight into multisector involvement of adolescents with disabilities but is not without limitations. Although the NLTS2 allowed for national estimates for adolescents across the range of disabilities served through special education, an advance over typical use of small convenience samples, the analyses should be replicated for the current population and with administrative data. The population estimates here indicate contact with various sectors and providers but not the nature of the involvement, quality, or effectiveness of services, or relations to specific needs. Other limitations are related to the structure of the NLTS2 instruments, which may underestimate involvement. The NLTS2 survey did not capture all possible means of engaging in the various sectors addressed here (e.g., short-term psychiatric holds; mental health services by providers not mentioned here). In the case of mental health and social work services, the parent questionnaire first asked about receipt, then receipt in schools such that it was not possible to determine who received these services both in and out of school. In addition, the questions regarding social work services were nonspecific in that they did not permit identification of the setting or nature of services provided. We classified social work services within the social service sector because this is the primary context in which social workers are employed, but they may also work in a variety of other sectors (U.S. Bureau of Labor Statistics, 2015). Furthermore, it is possible that the estimates of multisector involvement were biased by nonresponse, particularly by the lower response rate of educators who completed the school program data from which IEP services for psychosocial difficulties were drawn compared with the data obtained from parents. Nonetheless, measures of involvement and frequency here are relevant to educators and policymakers as they suggest high rates of multisector involvement related to some disabilities and point to a need to be responsive to this involvement in efforts to support these students.
Conclusion
Multidisciplinary collaboration is considered essential to improving health and reducing disparities, two major areas of concern for individuals with disabilities throughout the life span (Chrvala & Bulger, 1999). Although schools are a primary sector of involvement related to psychosocial difficulties among adolescents with disabilities, many of these students are involved in multiple service sectors. Communication and collaboration across systems can support the ongoing problem-solving and intervention processes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Robert Wood Johnson Foundation (New Connections Award 69589), awarded to Amanda L. Sullivan. The content of this article is solely the responsibility of the authors and does not represent the views of the Foundation. We are grateful for the support.