
Abstract
Despite the high prevalence of mental health concerns in university populations, students are unlikely to seek formal help. The current study examined help-seeking behaviors among emerging adults in a university setting using a mental health literacy framework. Responses from 122 university undergraduates were examined. Students ranged in age from 17 to 25 years (M = 20.67 years, SD = 2.03 years). Quantitative data were collected to determine students’ knowledge and use of campus services and to compare students’ awareness and appraisal of common mental health symptoms. Narrative data were collected to identify the key symptoms that are appraised to be “early warning signs” versus “early action signs,” and to identify barriers and facilitators to help-seeking. Mental health symptoms were more likely to be assessed as warning signs than signs warranting action. Lack of knowledge and stigma were barriers to help-seeking, while urging from family and friends, increased knowledge, and confidentiality were identified as facilitators to help-seeking. Emerging adults in a university setting tend to make distinctions between warning and action signs. Although demonstrating good awareness of the signs of declining mental health, students may respond reactively rather than proactively to symptoms.
One third of university students report significant stress and mental health concerns (Adlaf, Gliksman, Demers, & Newton-Taylor, 2001). As approximately 75% of lifetime mental disorders have first onset by age 24 (Kessler et al., 2005), and many disorders have their peak period of incidence during young adulthood (Rickwood, Deane, Wilson, & Ciarrochi, 2005), emerging adulthood represents a particularly susceptible period of the life span. Despite high levels of stress and mental health problems, university students are the least likely population to seek formal help for mental health concerns (Biddle, Donovan, Sharp, & Gunnell, 2007). Researchers have identified several barriers to help-seeking among emerging adults, such as fear of stigma, negative beliefs about help-seeking, preference for self-reliance, and poor recognition of mental health decline (Gulliver, Griffiths, & Christensen, 2010; Rickwood et al., 2005). Given the low rates of help-seeking among university students, the potential for untreated symptoms to worsen and mental health to deteriorate is high.
Mental health literacy (MHL) encompasses both knowledge and beliefs about mental disorders, assisting in their recognition, management, or prevention (Jorm, Korten, Jacomb, Rodgers, & Pollitt, 1997). For the current study, we have incorporated the help-seeking framework proposed by Rickwood et al. (2005) in which MHL aids in the progression through help-seeking stages, and mental health illiteracy presents barriers. Within this framework, the first stage to help-seeking begins with awareness and appraisal that one has a problem. Mental health illiteracy at this stage involves a lack of knowledge about the symptoms of mental disorders, or appraisal that certain symptoms do not warrant concern or help. The second stage involves the expression of a need for help. Negative beliefs about mental illness and help-seeking inhibit progressing through this stage. The third stage of help-seeking involves the knowledge of available help sources. A lack of knowledge regarding potential help sources or the process involved in help-seeking would present another barrier. The final stage of help-seeking culminates with a willingness to access the help that is available. Perceptions and beliefs regarding available services impact progression through this stage. In sum, in order to engage in help-seeking, one must first identify a mental health problem and assess the problem as warranting action, then one must express a need for help, understand how to gain help, and be willing to procure the help which is available.
Past research has supported the theoretical stages of help-seeking. For example, the general construct of MHL has been related to help-seeking intentions. Smith and Shochet (2011) surveyed university students on various components of MHL and help-seeking intentions. Higher levels of MHL were predictive of greater intentions to seek formal help. In particular, knowledge about the helpfulness of interventions, knowledge about confidentiality and affordability of services, and beliefs about mental illness uniquely contributed to participants’ intentions to engage in formal help-seeking. Moreover, MHL deficits among university students have been linked to lower rates of formal help-seeking (Furnham, Cook, Martin, & Batey, 2011; Rickwood et al., 2005; Yorgason, Linville, & Zitzman, 2008).
Although all four stages of the help-seeking framework have been investigated, the first stage, awareness and appraisal, warrants further consideration. Past research has focused on individuals’ knowledge, recognition, and awareness of symptoms (Burns & Rapee, 2006; Lauber, Ajdacic-Gross, Fritschi, Stulz, & Rossler, 2005) while comparatively less attention has been paid to the appraisal of symptoms. The focus on symptom recognition begs the question—does awareness alone influence help-seeking? Progression through the help-seeking stages would seem to rely on the type of appraisal made in the first stage. Young adults may become aware of signs or symptoms that are indicative of a mental health problem (i.e., warning signs); however, unless they appraise the signs or symptoms to be important enough to warrant help-seeking (i.e., action signs), there would be no motive to progress through subsequent stages. For example, a young adult may be aware that prolonged sadness is a warning sign of depression, but could mistakenly appraise the symptom as not warranting attention/action, if she does not understand the risks of untreated depression, does not believe mental health treatments to be efficacious, or does not believe the symptom to be sufficiently serious.
Although valuable knowledge regarding young adults’ help-seeking behavior and MHL has been garnered through past studies, several areas for improvement remain. First, extant research has primarily been aimed at emerging adults’ awareness of symptoms, to the neglect of emerging adults’ appraisal of symptoms. Thus, little is known about the potential importance and consequences of symptom appraisal. Young adults begin to monitor their own health status and make their own decisions about health actions for the first time during emerging adulthood (Rickwood et al., 2005); therefore, they become more reliant than ever on their own judgment, making appraisal a particularly salient issue for this population. Second, symptom awareness and symptom appraisal have typically been grouped together as one general concept (i.e., the first step to the help-seeking process). Consequently, little is known about the potential differences in awareness and appraisal of symptoms. In particular, we are unaware of any research examining university students’ reactions to “warning signs” (that which would indicate a problem), in comparison with “action signs” (that which would actually prompt help-seeking behaviors). Although the knowledge component of MHL may assist young adults in correctly monitoring their health status via warning signs, the belief component of MHL is needed in order to make appropriate decisions regarding health actions via action signs. Third, past research has typically relied on either quantitative or qualitative methodology, while mixed methods designs have been neglected. As the current topic of investigation is relatively unexplored, both quantitative and qualitative methods are needed to cross-corroborate findings as well as provide a rich foundation on which further research can build. The structured format of quantitative methods enhances the breadth of our knowledge by determining global statistics and allowing for future replication. Conversely, the nuanced format of qualitative methods enhances the depth of our knowledge by improving our understanding of individuals’ perceptions and experiences.
In order to establish a firm foundation for research in this new area, the actual voices of emerging adults should be heard, and their opinions sought. Therefore, the four main research objectives include investigating (a) symptoms university students consider to be the most pertinent warning signs, (b) symptoms university students consider to be the most pertinent action signs, (c) differences between awareness and appraisal of symptoms by comparing “warning signs” and “action signs,” and (d) factors (e.g., barriers and facilitators) that potentially influence the decision to act upon awareness and appraisal of symptoms.
Method
Procedure
Prior to beginning the study, approval was obtained from the local institutional review board. Students from a mid-sized Canadian university were recruited. In compensation for their time, students were given the option of receiving 1% credit toward their final grade through the university’s participant pool or entering into a draw for one of two CAD$50 gift certificates to a large box-store. Efforts were made to recruit students across disciplines through presentations in classes across campus; however, participation was higher for those receiving credit (approximately two thirds of responses). The study was completed online using SurveyMonkey.
Participants
A total of 154 individuals completed the survey. Prior to providing consent, participants were informed that incomplete surveys would be considered a withdrawal from the study should more than 20% of questions be left unanswered. Nine participants left more than 20% of questions unanswered and were subsequently removed from the sample. Individuals above the age of 25 were excluded from the sample in order to more accurately represent emerging adults in the university setting. This resulted in the removal of an additional 23 participants. The final sample for this study consisted of 122 undergraduate students ranging in age from 17 to 25 years. Demographic characteristics are summarized in Table 1.
Demographic Characteristics of Sample (n = 122).
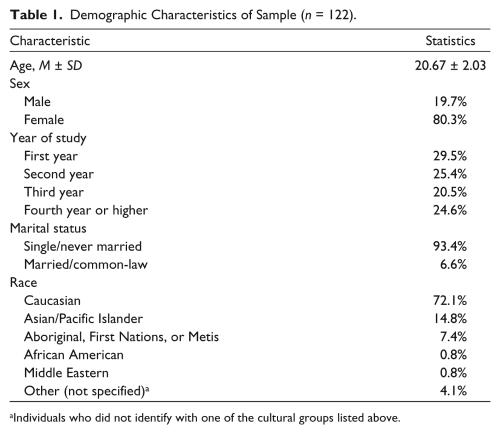
Individuals who did not identify with one of the cultural groups listed above.
Demographic factors are integral to mental health concerns. Socioeconomic variables were not directly queried in the current study; however, the university population from which the sample was sought has previously been examined and compared with national rates. A brief review of these factors allows for a better contextualization of our study’s findings. Demographics were drawn from the Office of Resource Planning, University of Regina (2011a, 2011b). Demographic information from the current sample is described further in the “Results” section.
The average age of undergraduate students in the sampled population is 24 years, slightly older than the national average (22 years). The number of female students is on par with the national average (66% in sampled population, 67% nationally). Although a smaller percentage of students identify as a visible minority (19%) in the studied population compared with the national average (25%), the population of aboriginal students is higher (10%) than the national average (5%). These rates are similar to the demographic of the current sample (see Table 1).
A similar proportion of students report living with their parents during their studies in the sampled population than nationally (43% and 40%, respectively); however, more students report being employed during their studies (62%), compared with national rates (56%). The most common source of financing for undergraduate students at the current university is from parents, family, or spouse (60%), which is similar to the national average (58%). Thus, although socioeconomic status was not directly examined in the current sample, the population’s characteristics are comparable with that of the national average, with only cultural distinctions.
Measures
Demographic questionnaire
All participants completed a demographic questionnaire querying age, sex, year of study, program of study, ethnic group, and marital status.
Knowledge and Use Questionnaire (KUQ)
A three-item questionnaire was developed to query knowledge and previous use of on- and off-campus mental health services. To calculate a global knowledge score, three questions from the KUQ were summed to represent knowledge of campus mental health services (maximum score of 15 with higher scores indicating higher knowledge). Participants were asked to rate their knowledge of mental health and counseling-related services (rated on a 5-point Likert-type scale); knowledge of how to contact services, if needed (rated on a 5-point Likert-type scale); and knowledge of other source of support counseling on campus (1 point for each source to a maximum of 5 points). Cronbach’s alpha for the KUQ was .73 in the current sample, suggesting good reliability. Responses regarding service use were examined using descriptive analyses.
Attitudes Toward Seeking Professional Psychological Help
The Attitudes Toward Seeking Professional Psychological Help–Short Form (ATSPPH-SF; Fischer & Farina, 1995) is a 10-item self-report measure of attitudes toward seeking mental health care. This measure is a short version of the Attitudes Toward Seeking Professional Psychological Help Scale first developed by Fischer and Turner (1970). Responses to the ATSPPH-SF questions are provided using a 4-point Likert-type scale and higher scores represent more positive attitudes toward seeking professional help. The ATSPPH-SF has previously been reported to have a strong internal consistency of .84 and good test–retest reliability over 1 month, a .80 in a university population (Fischer & Farina, 1995). In the current sample, Cronbach’s alpha was .77.
Perception of Mental Health and Help-Seeking Questionnaire
A series of open-ended questions was asked to gain participants’ perspectives on mental health services. Participants were asked to reflect on (a) what behaviors, problems, or feelings they would consider as warning signs that they should seek help; (b) what behaviors, problems, or feelings would need to be occurring for them to actually seek help; (c) perceived barriers to seeking mental health services; and (d) perceived facilitators to seeking mental health services
Warning and Action Signs Checklist
A list of 18 common signs of mental health decline was compiled. The items included on the checklist were determined through a review of lists of signs and symptoms of mental health impairment available through an Internet search. Two researchers individually conducted searches and then reviewed items to create a comprehensive, yet accessible, list of signs and symptoms. The rationale for this approach was to identify signs and symptoms that would be commonly identifiable to the lay-person should they be seeking information. The list included both symptoms (e.g., hallucinations) and signs of impairments (e.g., growing inability to cope with daily tasks). Participants were shown the list of symptoms twice. In the first instance, participants identified which of the items would be a warning sign that they might need help. In the second instance, participants identified which of the items would need to occur before they actually seek help from a mental health professional.
Study Design
Upon following the link to the study, participants were provided with a description of the procedure and purposes of the study. Once participants provided informed consent to participate, they completed demographic questionnaire, the KUQ, and the ATSPPH-SF. Subsequently, participants responded to the open-ended Perception of Mental Health and Help-Seeking Questionnaire. The Warning and Action Signs Checklist was the final portion of the study completed by participants. The open-ended questions were asked prior to the presentation of the Warning and Action Signs Checklist to ensure that responses were not influenced by being presented a list of symptoms. Quantitative analyses were undertaken with questionnaire results to better understand the relationship between help-seeking and various factors (e.g., beliefs).
In addition to quantitative analyses, qualitative analysis of each open-ended question was conducted. Analysis of the open-ended questions employed a thematic content analysis approach (Dixon-Woods, Agarwal, Jones, Young, & Sutton, 2005). Analysis occurred within each question using a data-driven approach in which no a priori categories were established; rather, emerging thematic categories were examined. Through an inductive process of becoming familiar with the data, generating initial codes, searching for themes, reviewing themes, defining and naming themes, each researcher generated a list of themes for each question through an independent analysis of the total data set (Braun & Clarke, 2006). Pulling from Braun and Clarke’s (2006) definition of a theme, in which “a theme captures something important about the data . . . and represents some level of patterned response or meaning within the data set” (p. 82), potential themes were evaluated based on their relevance to the research questions and the degree to which they were emphasized both across and within participant responses.
Subsequently, through collaborative discussion between both researchers, themes were combined, collapsed, expanded, and renamed until a final list of themes was completely agreed upon. All data were re-examined and applied to the themes to ensure that identified themes appropriately captured the data (Bradley, Curry, & Devers, 2007). Themes were categorized as “primary” or “secondary” consistent with the degree of emphasis placed on the theme by participants. In addition, responses were further categorized and examined based on prior mental health service use; however, no differences in themes emerged when comparing those who had sought services in the past with those who had not sought services. There was high completion rate of the open-ended questionnaire, as 121 of 122 participants provided responses.
Results
Treatment of Missing Data
Prior to beginning the analyses, an examination of missing data was performed. Nine participants had completed less than 80% of the survey. These participants were considered to have withdrawn from the study, as outlined in the consent form, and were automatically removed without further analyses of responses. Patterns of missing data across remaining participants were examined. Missing data were minimal; however, differences in means were examined for each variable between individuals with and without missing data (Tabachnick & Fidell, 2007). No significant differences were found across variables as a result of missing data.
Mental Health Service Use
Among participants, 82% were reportedly aware of the mental health services offered on campus. Frequency of on- and off-campus mental health service use is summarized in Table 2.
Frequency of Mental Health or Counseling Service Access On and Off Campus.

Identification and Comparison of Pertinent Warning and Action Signs
Quantitative results
To address the first two purposes of this study, the frequency of the sample that endorsed each of the symptoms as a warning sign or as an action sign was calculated (see Table 3). All the symptoms, with the exception of “confused thinking” were identified by 50% or more of participants as being a warning sign of mental health concerns. Although several symptoms were endorsed by a large portion of the sample, “prolonged sadness,” “suicidal thoughts,” and “self-harming behaviors” were symptoms that were most frequently identified as a warning sign, with 82%, 81%, and 80% of participants endorsing the symptoms, respectively.
Frequency of Sample Identifying Symptoms as Either a Warning Sign or Action Sign.
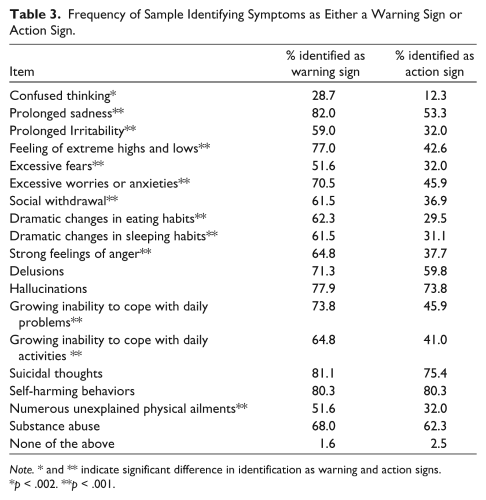
Note. * and ** indicate significant difference in identification as warning and action signs.
p < .002. **p < .001.
Contrary to the high endorsement rates for warning signs, only 6 of the 18 symptoms were identified by more than 50% of participants as symptoms warranting action. In particular, only “prolonged sadness,” “delusions,” “hallucinations,” “suicidal thoughts,” “self-harming behaviors,” and “substance abuse” were symptoms identified as most likely to lead to action.
To address the third purpose of this study, McNemar’s test, a non-parametric test for paired dichotomous data, was used for each symptom. These analyses allowed for identification of significant difference between the number of participants endorsing the symptom as a warning sign and the number of participants endorsing the symptom as an action sign. As multiple comparisons were made, Bonferroni’s correction was used to reduce the risk of Type I error. As a result, comparisons were considered statistically significant when p ≤ .0026 (corrected to allow for McNemar testing on the 19 items, that is, p = .05/19). Significant differences between awareness and appraisal for each sign are highlighted in Table 3.
All symptoms, with the exception of “delusions,” “hallucinations,” “suicidal thoughts,” “self-harming behaviors,” and “substance abuse,” were significantly more likely to be identified as a warning sign than as an action sign. In all cases where significant differences were found between warning signs and action signs, participants were less likely to act on the symptom, despite identifying it as a warning sign. When no significant differences were found, endorsement rates were typically high for both warning and action signs, suggesting that a subset of symptoms are concerning enough to lead to both awareness and appraisal of need for action.
Qualitative findings
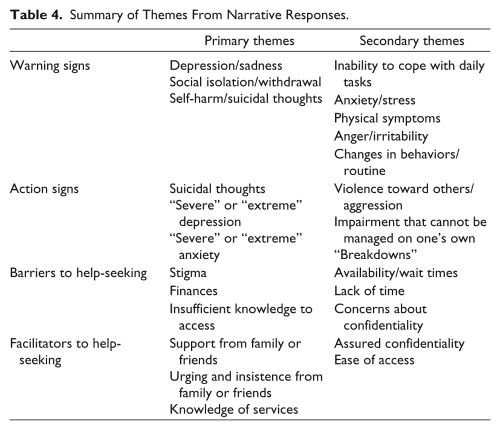
To ensure that no signs or symptoms of mental health decline were overlooked with the checklist, participants were asked to identify warning signs of mental health decline and signs that would motivate action through open-ended questions. Emerging themes are summarized in Table 4.
Summary of Themes From Narrative Responses.
Warning signs
Analysis of responses revealed that participants were able to independently identify several symptoms that might be indicative of a problem. In particular, three primary themes emerged. First, participants shared that depression and sadness warned them of a need for help regarding their mental health. As one participant reported, Feelings of anger, sadness, emptiness, extending for long periods of time. These kinds of feelings may ultimately lead to depression and if I was concerned about that then professional help may be very useful to me at such a time.
Second, participants reported that thoughts or attempts of self-harm or suicide would also be significant warning signs that assistance with their mental health was necessary. Third, participants identified social isolation and withdrawal from their family and friends to be warning signs of mental health concerns, such as identified by one participant who articulated that “disconnect from family, friends and loved ones” would be cause for concern.
Overarching the specific warning signs identified was the notion that change in routines or behaviors was a central indicator of mental health decline. This is exemplified by one participant who stated, “If myself, or others in my life noticed significant changes to my life regarding moods and actions such as depressed mood or grades falling.”
Action signs
Participants were similarly asked to identify behaviors, problems, or feelings that would have to be occurring for them to actually seek help for their mental health. Although specific symptoms were identified, an overarching theme across responses was the level of severity and duration of symptoms. Participants frequently used terminology such as “severe” or “extreme.” For instance, consistent with this idea of severity, one participant stated, If I was feeling extremely depressed or anxious for an extended period of time and it was caused by things that usually do not bother me/ or if I did not know the origin of my feelings I would want to seek mental health.
Suicidal ideation was a common theme across participants as a symptom that would cause participants to take action. For instance, one participant wrote “having hateful/suicidal thoughts” would cause him to seek out help. Moreover, participants reported that violence or aggression toward others, impairment that cannot be managed on one’s own (i.e., no social supports, interference with daily life, can no longer cope with symptoms alone), and “breakdowns,” would be alarming enough for them to utilize mental health services.
Factors That Influence Help-Seeking Behaviors
Quantitative findings
Consistent with the fourth purpose of this study, specific factors that predict actual help-seeking were examined. In particular, the influences of attitudes toward psychological help and knowledge of counseling services were examined. To better understand the role of these variables on help-seeking, a hierarchical multiple regression was performed. The predictors of interest were attitudes toward seeking psychological help, as measured by the total score on the ATSPPH-SF, and knowledge of university counseling services, as measured by the total score on the KUQ. Help-seeking behaviors were assessed by using the participants’ reported frequency of access of university counseling services as the dependent variable. This dependent variable was selected for several reasons. First, given the university population, the free services available on campus are likely the most accessible services for individuals seeking help. Second, the specific role of knowledge of this service on use of the service was of interest. Using frequency scores for broader access of mental health services would overlook the specific relationship between knowledge of counseling services and use of counseling services.
Given findings from previous research suggesting that demographic characteristics influence use among university students (Nam et al., 2010; Yorgason et al., 2008), the influences of age and sex were controlled for by entering these variables first (Step 1). Next, ATSPPH-SF and KUQ total scores were entered in Step 2. Finally, frequency of access of counseling services was entered as the dependent variable. Age and sex explained 5% of the variance in service use. After entering ATSPPH-SF and KUQ scores in Step 2, the model explained 28% of the variance in campus counseling service use, F(4, 113) = 10.98, p < .001. The addition of these measures in Step 2 explained an additional 23% of the variance in service use, after controlling for age and sex, R2 change = .23, F change (2, 113) = 18.22, p < .001. In the final model, only knowledge of counseling services was statistically significant (β = .48, p < .001). These results suggest that service use is impacted by knowledge of counseling services and attitudes toward health care providers; however, when examined more closely, knowledge of counseling services has the greatest effect on services use, and is the only factor that makes a unique statistically significant contribution to services use. The regression results and standardized regression coefficients (β) are summarized in Table 5.
Results of Regression Examining Influence of Attitudes and Knowledge of Access of Counseling Services on Frequency of Counseling Services Access.
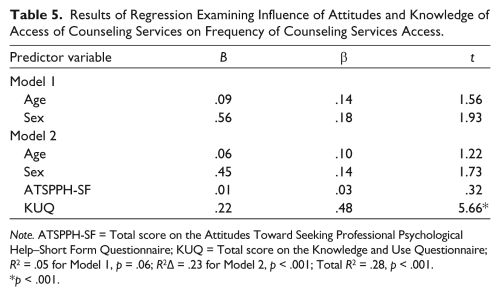
Note. ATSPPH-SF = Total score on the Attitudes Toward Seeking Professional Psychological Help–Short Form Questionnaire; KUQ = Total score on the Knowledge and Use Questionnaire; R2 = .05 for Model 1, p = .06; R2Δ = .23 for Model 2, p < .001; Total R2 = .28, p < .001.
p < .001.
Qualitative findings
The fourth purpose of this study was to provide a comprehensive examination barriers and facilitators to formal help-seeking through open-ended questions. The themes that emerged through these analyses are summarized in Table 4.
Barriers to formal help-seeking
One of the most significant barriers to accessing mental health services was the stigma attached to using such services. A frequently identified and strongly emphasized theme by participants was that they felt a certain level of “shame,” “judgment from others,” and general “embarrassment” if they were to access mental health services. As one participant noted, “Shame of not being able to deal with issues myself.” Another participant commented, “The stigma that mental illness is a weakness would prevent me. I wouldn’t want to be seen as weak or vulnerable.”
Inadequate knowledge of practical facets of services, such as how to access services or cost of services was a broad theme across responses. Specifically, though the university counseling services are free to students, results revealed that not all students were aware of the free mental health services available on campus as they identified constraints on finances as a critical barrier to accessing mental health services. In addition, participants mentioned that they had insufficient knowledge regarding which mental health services were available on and off campus. The lack of knowledge of practical aspects of services appeared to be a large deterrent, as exemplified by one participant who identified “not knowing where to go or how to schedule appointments” as a significant barrier to accessing needed mental health services.
Facilitators to formal help-seeking
Support was strongly emphasized as a facilitator to treatment. For instance, one participant stated “the support and encouragement of friends and family would contribute to me accessing services.” In addition to support, participants commented that urging and insisting from their family or friends that they seek help would facilitate access to services. Consistent with this theme, one participant commented, “Family members and friends voicing concerns over my current state of mental health,” while another noted, “Having a friend or family member telling me I needed to go” would facilitate accessing mental health services.
Many participants reported that additional knowledge of services (i.e., location, how to access, the process of therapy, information about counselor, etc.) would facilitate their access to services. This was exemplified by one participant who commented, “Increase in knowledge of services available!! I did not know that the [University] provided such services.”
Concerns over confidentiality and visibility (i.e., likelihood that others will know you are accessing services) when accessing in-person services, and steps to increase confidentiality were highlighted as a second important theme. Participants noted that assurance that the mental health services provided would be confidential and services were easily accessed (i.e., affordable, short wait times, private location) would be key facilitators to using mental health services. Suggestions to decrease visibility of those accessing services from the public were commonly made by participants. For example, one participant suggested that the campus counseling center be relocated to a more innocuous location in order for students to not be readily identified as attending mental health services. Recommendations such as allowing for online booking of services were also made in order to enhance students’ confidentiality.
Discussion
High prevalence of mental health concerns coupled with strong reticence to seek formal help renders university students a target population for mental health professionals’ attention and intervention. Emerging adults who attend university may be hampered in their help-seeking by a lack of MHL, which inhibits progression through the help-seeking process. The current study targeted the comparison of symptom awareness (identifying warning signs) with symptom appraisal (identifying actions signs), sought to elucidate students’ perspectives on the most pertinent warning and action signs, as well as identified which factors influence acting upon these appraisals. Utilizing a combination of quantitative and qualitative methods allowed for both breadth and depth of knowledge.
Relevant Warning and Action Signs
It could be argued that any symptom which indicates a mental health problem should automatically warrant action. Based on this logic, warning signs and action signs should be appraised in a near identical fashion. On the contrary, students perceived warning signs to be quite distinct from action signs. The majority of signs and symptoms from the list with which students were presented were appraised to be a warning sign, but not something that would prompt help-seeking. Similarly, when asked to independently generate warning signs of mental health problems, students were able to identify the more subtle symptoms of mental health concerns, such as impairment in daily activities, social withdrawal, and changes to patterns of behavior. Despite having a good sense of which behaviors/problems are signs of mental health decline, only the most severe of symptoms (i.e., suicidal thoughts, hallucinations) were equally appraised to be both a warning and action sign. When asked to generate action signs that would prompt them to seek help, students placed more emphasis on the severity of symptoms. Although “depression/sadness” was one of the primary warning signs identified in students’ narrative responses, “severe or extreme depression” was one of the primary action signs. In addition, the responses unique to action signs all include some element of blatancy. When symptoms become apparent to others or difficult to hide, students seem more likely to seek help.
This distinction between warning and action signs suggests that university students in the emerging adult age group are reactive rather than proactive in regard to mental health concerns. Students’ appraisal that only the most severe symptoms, such as hallucinations and suicidal thoughts, should prompt action is particularly worrisome. Delaying treatment until symptoms are extreme makes intervention more difficult and recovery less likely (Kisely, Scott, Denney, & Simon, 2006; Rosenkranz & Muller, 2011). Furthermore, as symptoms increase, intentions to seek help tend to decrease, making delayed help-seeking all the more problematic (Rickwood et al., 2005). Students’ tendency to wait until symptoms are extreme before seeking formal help may contribute to the increasingly high prevalence and severity of mental health problems among this population.
Barriers and Facilitators to Help-Seeking
Several factors were identified that might influence responding to one’s awareness and appraisal of symptoms. The importance of knowledge to help-seeking was identified in both the regression results and qualitative findings. Students reported insufficient logistical information (e.g., location, fees) as well as procedural information (e.g., who is eligible, what to expect in treatment) as barriers to taking action.
Although the quantitative results indicated that beliefs/attitudes about help-seeking are not predictive of help-seeking, the qualitative responses suggested that certain beliefs/attitudes do play a role. This discrepancy is likely due to the way in which beliefs and attitudes were queried in the two methods. The specific attitudes/beliefs presented in the questionnaire were not necessarily the same attitudes/beliefs that emerged in the open-ended qualitative responses.
Stigma is one such attitude/belief that students indicated as a particularly important barrier to seeking services. In fact, students indicated that increasing the secrecy of help-seeking would help limit stigma, and thus, would facilitate seeking services. Stigma as a barrier to help-seeking has been widely discussed in past research (Eisenberg, Downs, Golberstein, & Zivin, 2009; Livingston & Boyd, 2010), and widely targeted in mental health initiatives and awareness campaigns (Stuart, 2008). The current results suggest that the many forms of stigma (e.g., shame, fear of judgment from others, self-stigmatizing attitudes) remain a major impediment to the receipt of mental health services. Students recommended several logistical changes, such as online booking of appointments and housing campus services in an allied health center rather than in a separate distinct area, that could be implemented to delimit anticipated stigma.
Students also identified support and insistence from family or friends as major facilitators to accessing mental health services on campus. This finding is consistent with past research, which has identified social support or encouragement from others as a primary facilitator among young people seeking help (Gulliver et al., 2010).
Conceptual Model of MHL and Help-Seeking
Although models of help-seeking have been previously proposed (e.g., Rickwood et al., 2005), they do not sufficiently capture the distinction between awareness and appraisal identified in the current study. Results suggest that awareness and appraisal are distinct processes, and that they should be recognized as such when considering emerging adults’ understanding of mental health symptoms. To better capture this distinction, a conceptual model, based on integration of the qualitative and quantitative findings, is proposed in Figure 1. This model highlights the distinction between awareness and appraisal, as well as the progression toward help-seeking that is impacted by barriers and facilitators identified through our results. Following the same process from awareness to action, the quantitative and qualitative findings allow for proposed recommendations to improve MHL and access to services.
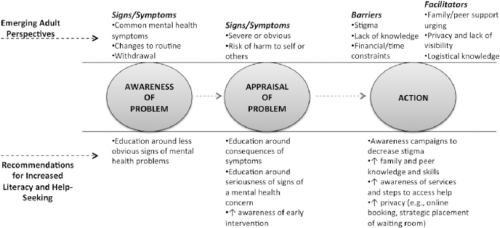
Conceptual model of mental health literacy and help-seeking in university students.
At the stage of awareness, quantitative and qualitative results suggest that students have a good sense of which behaviors or symptoms are “warning signs” of a mental health concern. A subset of more subtle signs of mental health decline, such as irritability and changes to sleep and eating, were less frequently identified as warning signs. Increased education around the less obvious, yet equally pertinent signs could improve awareness across students.
Both the quantitative and qualitative results support the notion that emerging adults appraise symptoms as problematic when they are severe or obvious markers of mental health problems (e.g., suicidal ideation, hallucinations). Similarly, when they perceive themselves as at risk for harming themselves or others, symptoms are appraised as warranting action. Paralleling these findings, we propose that education of the consequences of symptoms, and the benefits of early intervention, even for less obvious symptoms may result in increased help-seeking. Professionals and educators should consider promoting awareness about the implications of failing to seek help in response to warning signs. Moreover, instruction on accurately appraising mental health symptoms should be incorporated into the education system curriculum. If instruction was provided during school-aged years, people may be better prepared to take health-related action in emerging adulthood.
Participants identified several barriers and facilitators that might intervene between appraisal and action. As discussed, stigma, lack of a knowledge, and financial/time constraints were detrimental to access, while support, as well as a guarantee of privacy supported help-seeking. Several recommendations emerged from these findings, as well as directly from the participants’ recommendations. Continued work to decrease stigma on campuses remains needed. In addition, mental health professionals and educators should also consider promoting logistical and procedural knowledge of formal help-seeking. Given that participants suggested that parents and peers played a big role in their help-seeking behaviors, education geared toward providing skills in assisting a loved one in seeking services could be useful. Finally, implementing changes that allow for increased privacy of clients accessing service may encourage students to seek help.
Reflection on Cultural/Institutional Context
The participants in the current study consisted of university students in a mid-sized western Canadian university and the results reflect on the general university culture in several ways. First, participants gave the impression that the university atmosphere is not conducive to, or supportive of, formal help-seeking for mental health concerns. This is in line with past research indicating that components of campus culture (e.g., lack of marketing of mental health services, over-valuation of physical health, and under-valuation of mental health) can dissuade students from help-seeking (Chen, 2013). Second, participants strongly asserted that mental health stigma is still very much alive within the Canadian university culture. These findings are consistent with past research proposing that mental health stigma is particularly widespread within university settings (Golberstein, Eisenberg, & Gollust, 2008). As peer influence is highly important to identity formation and decision making in emerging adulthood (Seiffge-Krenke & Beyers, 2007), perceptions of peer beliefs and the experience of social pressures are integral to help-seeking within this culture (Goodman, Peterson-Badali, & Henderson, 2011).
Third, participants indicated that mental health knowledge is lacking in this institutional context. As those emerging adults who are attending university are often assumed to be more educated and advantaged (i.e., higher socioeconomic status) than their non-university student peers, this finding is particularly disconcerting. Nevertheless, MHL would have to be examined in a non-university population of emerging adults in order to extrapolate the current findings to diverse cultural, socioeconomic, and institutional contexts.
Limitations
Several limitations to this study should be acknowledged. To begin, the majority of the sample was female and Caucasian. As noted, the sampled population is similar on demographic variables to institutions across Canada; however, the population sample includes a higher rate of aboriginals and lower overall rate of visible minorities. This demographic distribution may have uniquely influenced responses in the current study. The small number of participants within minority groups did not allow comparisons between cultural group. Consequently, certain cultural influences on help-seeking (e.g., underutilization of formal supports among minority students; Kuo, Kwantes, Towson, & Nanson, 2006) may not be represented in the current results.
Similarly, our sample is most representative of a middle-class socioeconomic status and may not generalize to emerging adults in alternate socioeconomic strata. Moreover, data collection was limited to one university, and the majority of students in the sample were enrolled in kinesiology, psychology, and nursing. As a result of the sample limitations, our findings may not be generalizable across different universities and among all university students. The purpose of our study was to gain an enhanced understanding of the MHL of emerging adults in the university setting; therefore, further research is needed to examine whether there is variation in MHL across different universities and students in diverse disciplines.
In addition, the checklist used to determine students’ perspectives on warning signs versus action signs was simplistic, in that it did not provide contextual details about their decision making. For example, the checklist did not allow for participants to indicate the degree of symptoms that would warrant action, or certain situations in which symptoms would warrant action. Another limitation of the checklist method is the potential for participants to interpret symptoms differently. For example, one student’s definition of “substance abuse” may not be the same as the next student’s definition.
Conclusion
Emerging adults in the university setting approach mental health concerns reactively rather than proactively. Students tend to view the majority of mental health symptoms as warning signs of a problem but not as a prompt to actually seek help. Although students demonstrated good awareness of the signs of declining mental health, they lacked awareness regarding when to seek help. Students also self-reported that lack of knowledge and concerns regarding stigma impacted their willingness to seek help from available campus mental health services. In order to improve university students’ help-seeking behaviors, initiatives to develop MHL at the appraisal stage of the help-seeking process by increasing knowledge and decreasing stigma are necessary. The current study contributes to the theoretical underpinnings of MHL by highlighting the importance and implications of symptom appraisal in the help-seeking process.
Future research should extend the current study by investigating symptom awareness and appraisal in more culturally diverse samples. In addition, future research should examine potential influences on students’ awareness and appraisals of symptoms, such as context (life stresses, time of semester, etc.), compounding of symptoms, among others. As well, garnering a greater understanding of students’ personal definitions of various mental health symptoms would provide insight into their awareness and appraisal behaviors. Similarly, differentiating the appraisal process for one’s own symptoms in comparison with others’ symptoms (e.g., peer, partner) would further clarify the interrelationship between MHL and help-seeking among emerging adults. Finally, in order to provide more empirical support for the importance of symptom appraisal to subsequent help-seeking, future research should compare the help-seeking actions of emerging adults with varying symptom appraisal abilities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.