
Abstract
Despite the prevalence of mental health problems, society continues to stigmatize and discriminate against people with mental illness and in particular, schizophrenia. Among the negative consequences of stigma, is that some individuals with mental illness internalize negative stereotypes about themselves, referred to as self-stigma, which is associated with a reluctance to seek needed treatment. The challenge to overcome mental illness stigma has led to the development of global anti-stigma initiatives, which effectively engage young people in school-based programs. The present study examines the effectiveness of a single-session anti-stigma intervention with high school youth (n = 254). The findings replicate and extend previous work demonstrating that a brief anti-stigma initiative can produce significant improvements in knowledge, social distance, and self-stigma. Self-stigma was found to be associated with low self-esteem and factors affecting self-disclosure were identified. Implications for school curricula, mental health policy, and future research are discussed.
Reflecting on her high school years a couple of decades ago, Liz recalls that she started hearing voices at about age 14. In retrospect, she acknowledges that “I knew this was not normal” and wonders if others sensed that something was wrong. However, she says, “I hid the problem by avoiding people and spending a great deal of time by myself.”
For Liz, who was later diagnosed with schizophrenia and has been engaged successfully in treatment and psychiatric rehabilitation, it was not a lack of recognition of symptoms that stopped her from seeking help when she was a youth. Rather, it was the sense of feeling embarrassed and self-conscious.
This phenomenon, whereby public stigma surrounding mental illness is internalized, creating a sense of shame, is termed self-stigma. It differs from public stigma, which is the social process whereby people endorse negative stereotypes about a certain group of individuals and then distance themselves from, and limit the rights of, that group (Corrigan & Watson, 2002). The negative effects of public stigma have been studied extensively with findings suggesting that individuals with serious mental illnesses, especially schizophrenia, are often stereotyped as dangerous, unintelligent, and incapable of recovery (Crisp, Gelder, Rix, Meltzer, & Rowlands, 2000). Such stereotypes are thought to lead to discrimination.
Stigma is the most frequently cited barrier that dissuades people from seeking treatment (Corrigan, 2004). Despite considerable advances in both the quality of, and accessibility to a variety of empirically supported treatments, numerous people with mental health issues never pursue treatment (Corrigan, 2004). In fact, in Canada only one third of those who need mental health services actually receive them (Statistics Canada, 2003). Self-stigma in particular, is believed to have negative effects on treatment engagement above and beyond the influence of public stigma (Moses, 2010). However, the direct relationship between self-stigma and a willingness to seek psychological services only recently has been empirically examined (Vogel, Wade, & Haake, 2006; Vogel, Wade, & Hackler, 2007). Research with adults has found that although the awareness and endorsement of public stigma initially contributes to the experience of self-stigma (Bathje & Pryor, 2011), it is self-stigma that is the more proximal indicator of an individual’s willingness or reluctance to seek professional help (Vogel et al., 2007). Unfortunately to date, there has been a remarkable absence of investigations with adolescent samples assessing self-stigma of seeking help beyond some recent pilot work by Yau, Pun, and Tang (2011). Self-stigma is considered the least researched topic in the area of stigma and help seeking (Schomerus & Angermeyer, 2008), yet it has potential to be of crucial importance for our understanding of the experience of teens who are first experiencing symptoms of mental illness. To our knowledge, the current research is the first study to examine adolescent self-stigma about seeking help in conjunction with exploring a classroom-based intervention for reducing self-stigma in high school students.
The Importance of Engaging Youth to Combat Stigma
Overall, public and self-stigma have adverse effects on the early detection, treatment, rehabilitation, and quality of life of individuals with mental illness. The pervasiveness of mental illness stigma and the underutilization of mental health services has led to the development of a number of global mental health promotion and anti-stigma initiatives, which are currently working with youth in school-based programs to combat mental illness stigma (e.g., Pinfold et al., 2003; Pinfold, Stuart, Thornicroft, & Arboleda-Flórez, 2005; World Psychiatric Association [WPA], 1999), and to enhance youth’s willingness to seek treatment (e.g., Rickwood, Cavanagh, Curtis, & Sakrouge, 2004; Wilson, Deane, Marshall, & Dalley, 2008).
Implementing such interventions during adolescence is strategic for three major reasons. First, research has shown that young children generally have poor knowledge of mental illness and their associated stereotypes; they do, however, seem to already possess stigmatizing attitudes as evidenced by tendencies to avoid people with mental illness (Wahl, 2002). These stigmatizing attitudes often fully emerge by puberty and solidify in adulthood (Hinshaw & Stier, 2008). Therefore, anti-stigma programs that target youth are thought to be strategic in that they influence young minds before prejudicial attitudes, beliefs, and behaviours towards mental illness become entrenched. Second, the likelihood of the onset of most serious mental illnesses peaks during late adolescence and early adulthood (Rickwood, Deane, Wilson, & Ciarrochi, 2005). Whereas intervening early when symptoms of mental health issues first emerge can lead to better outcomes and even complete recovery, delays in early detection have been equated with a worse overall outcome, especially for serious mental health issues such as schizophrenia (Perkins, Gu, Boteva, & Lieberman, 2005).
Third, in spite of their vulnerability to the onset of mental illness, research has shown that the majority of young people do not seek appropriate help (Rickwood et al., 2005). For many youth, the fear of being stigmatized by peers is a major barrier for seeking professional help for mental health concerns (Rickwood et al., 2005). Given that research with adults has found self-stigma to be a proximal indicator of help-seeking intent, it is of particular relevance to understand self-stigma among youth and the role it may play in fostering a reluctance to seek treatment, so as to develop ways to target this critical issue in school-based interventions.
School-Based Anti-Stigma Programs: Strategies to Combat Stigma
According to social psychological literature, three approaches are generally used to combat stigma: protest, education, and contact. The first of these, protest—a reactive strategy that aims to suppress stigmatizing attitudes about mental illness–is generally ineffective at reducing stigma (Corrigan & Penn, 1999). In contrast, education—a proactive strategy that involves challenging the myths of mental illness with factual information in order to enhance mental health literacy—has been found to be fairly effective (Corrigan & Penn, 1999). The third approach used in anti-stigma programs is contact. This involves dispelling negative beliefs about mental illness through direct in vivo interactions with mental health consumers. Contact appears to be the most promising approach to stigma change and can augment the effects of education (Corrigan & Penn, 1999). National and international studies of brief school-based educational workshops have shown that contact can increase mental health literacy and produce lasting positive changes in the reported attitudes of youth towards mental illness (Pinfold et al., 2003). However, there remains a clear need for examination “of treatment, educational programs, and other interventions targeted towards reducing self-stigma” (Vogel et al., 2006, p. 335).
Evaluating Change in Public and Self-Stigma
Education is an important and effective anti-stigma strategy as research has shown that people who have more accurate knowledge of mental illness are generally less likely to stigmatize mental illness (Faulkner, Irving, Paglia-Boak, & Adlaf, 2010). The need for stigma reduction programs that specifically target knowledge about schizophrenia among youth was elucidated by a recent Canadian study conducted by Faulkner et al. (2010) involving more than 3,000 high school students. In their study, nearly one third of student respondents did not know what schizophrenia was. Moreover, 17.7% of those students who were aware of the illness believed that people with schizophrenia are likely to be violent. Educational interventions have been recommended to dispel the misperceptions about mental illness and violence and other similar myths, as these overestimations largely dominate public perception and foster stigmatization (Torrey, 2011). Fortunately, previous research suggests that brief anti-stigma programs can significantly improve basic factual knowledge of schizophrenia among high school students (Pinfold et al., 2005).
The strategies of contact and education have also been implemented to reduce behavioural discrimination against people with serious mental illness. In stigma research, social distance, which is defined as an individual’s self-reported willingness to engage in relationships of varying levels of intimacy with a person who has a stigmatized identity, is the most frequently used proxy measure of discriminatory behaviour (Lauber, Nordt, Falcato, & Rossler, 2004). In Canada, research has found that 67% of high school students would feel ashamed if others knew that someone in their family was diagnosed with schizophrenia and nearly as many would be disturbed to be in the same class with someone with this diagnosis (Faulkner et al., 2010). Fortunately, research has also demonstrated an inverse relationship between contact and discriminatory behaviours towards people with mental illness. In fact, personal contact has been identified as the single most influential factor in changing stigma (Couture & Penn, 2003) and it is most effective when it involves mental health service recipients sharing with others their personal experience about their illness (Corrigan & O’Shaughnessy, 2007). Likewise, combining education and contact has also been fruitful in reducing discriminatory behaviours towards people with mental illness (Pinfold et al., 2003, Pinfold et al., 2005; Schulze, Richter-Werling, Matschinger, & Angermeyer, 2003).
Recently, school-based mental health promotion programs have begun to address students’ willingness to seek help. Preliminary research suggests that programs which enhance knowledge about mental disorders and their treatment and incorporate contact, show promise in increasing a youth’s readiness to seek help (Rickwood et al., 2004; Wilson et al., 2008). However, to our knowledge, only one study to date has directly assessed the effects on self-stigma; this pilot research (Yau et al., 2011) found that reducing self-stigma was possible when youth were provided contact with people who have mental illness on a horticultural farm vocational setting. Until now, there have been no studies that provide a sense of the potential prevalence of self-stigma among Canadian high school youth or any investigations of the effects of classroom-based contact interventions on self-stigma.
Investigating the effectiveness of programs that use contact and education in tandem to reduce mental illness stigma and enhance help-seeking behaviour is an important goal. Equally pressing, however, is the need to extend previous research by identifying factors that predict vulnerability to self-stigma and its relationship with the failure to seek psychological help. Previous research indicates that younger undergraduate students are more likely to self-stigmatize (Shechtman, Vogel, & Maman, 2010) and that college men experience greater self-stigma for seeking professional help compared with women (Bathje & Pryor, 2011; Shechtman et al., 2010; Vogel et al., 2006, 2007). Additionally, recent meta-analytic research with adults indicates that certain psychosocial variables predict heightened self-stigma, particularly low self-esteem (Livingston & Boyd, 2010); to our knowledge, few studies have formally investigated whether low self-esteem is associated with elevated self-stigma in youth. As well, social desirability, a phenomenon by which some people respond in socially acceptable ways, is a frequently cited limitation of anti-stigma program research as it can produce under-reporting of stigma and self-stigma; the effects of impression management needs to be considered more thoroughly (Corrigan & Shapiro, 2010).
The current study examined the efficacy of a single-session anti-stigma presentation designed for high school youth in reducing public and self-stigma towards mental illness. It was hypothesized that the anti-stigma initiative, which combines education and contact with a mental health consumer, would be effective in significantly enhancing knowledge, and reducing social distance and self-stigma. Second, the present study aimed to address a major gap in the literature by identifying factors associated with self-stigma in youth that are most responsive to change following an anti-stigma initiative, as well as their susceptibility to social desirability response influences.
Method
Participants
Five secondary schools in the Hamilton Wentworth District School Board region participated in this study. Participants were 282 male and female high school students in Grades 9 to 12 who attended one of eight identical anti-stigma presentations between October 28, 2011 and December 2, 2011. Only participants who completed all the measures were included in the analysis. There were no exclusion criteria. The study sample consisted of 254 high school students (female: 68.1%). Students averaged 16.8 years of age (SD = 1.15 years), with more than half in Grade 12 (51.2%), and a subset of students in Grades 9, 10, and 11 (6.7%, 9.1%, and 33.1% respectively). The majority of participants (71.8%) were White and spoke English as their first language (83.9%).
Measures
Factual knowledge of schizophrenia
Factual knowledge regarding schizophrenia was measured using the WPA’s (1999) Myths and Facts About Schizophrenia Questionnaire, which consists of nine statements representing common beliefs about schizophrenia; higher scores indicate greater knowledge. Cronbach’s α = .16 in pretest and .56 in posttest. There are some concerns with the WPA questions in terms of adequacy as a psychometric instrument, which were addressed to some extent in statistical analyses (see the Results section).
Social distance
The social distance scale used in this study was a slightly modified version of a 12-item scale developed for secondary school students (Schulze et al., 2003), adapted to a 4-point Likert-type scale ranging from 1 (definitely agree) to 4 (definitely disagree). Items describe intended behaviour towards people with schizophrenia; higher mean scores indicate greater desire for social distance. Cronbach’s α = .82 in pretest and .87 in posttest.
Self-stigma of seeking help (SSOSH)
The SSOSH scale (Vogel et al., 2006) was used as the measure of self-stigma. The 10-item self-report scale assesses concerns about the loss of self-esteem a person would experience if they decided to seek help from a mental health professional. For instance, “I would feel inadequate if I went to a therapist for psychological help.” Responses are made using a 5-point Likert-type scale ranging from 0 (strongly disagree) to 4 (strongly agree). Higher scores indicate a greater tendency to self-stigmatize treatment. Cronbach’s α = .78 pretest and .84 posttest.
Familiarity with mental illness
An eight-item revised version of the Level of Contact Report, adapted for use with adolescents, was used to assess prior experiences with mental illness (Corrigan et al., 2005). Higher scores indicate greater familiarity with mental illness.
Rosenberg self-esteem scale
The Rosenberg self-esteem scale (Rosenberg, 1965) is a well-validated 10-item measure of self-esteem. Higher total scores are indicative of higher self-esteem. Cronbach’s α = .90.
Social desirability
Social desirability was assessed using Ballard’s (1992) Scale 1 short version of the well-validated Marlowe-Crowne Social Desirability Scale. Higher scores represent a greater tendency to respond in a socially desirable manner. Cronbach’s α = .63.
Procedure
High schools in the Hamilton Wentworth District School Board region were invited to participate in the study and Grade-9 to -12 teachers from interested schools were contacted to schedule a time for the 75-minute interactive presentation on mental illness. Teachers distributed an information brochure and written informed consent form to students or to their guardian(s) for students who were younger than 18 years. Written informed consent was obtained from all participants prior to attending the presentation. Participants were not offered any form of compensation. These procedures were approved by York University’s Research Ethics Board, as well as by the E-Best research committee of the Hamilton Wentworth District School Board.
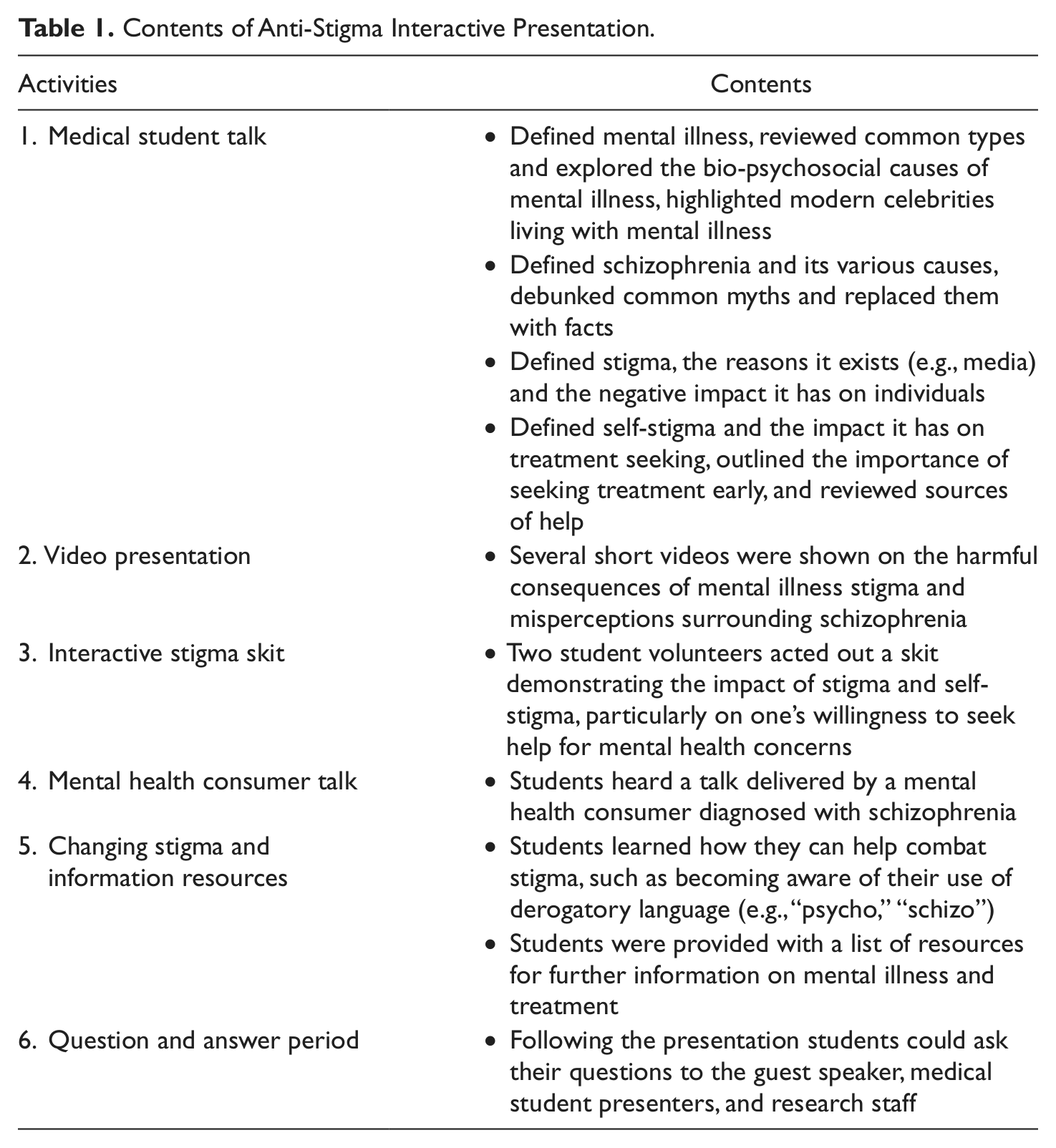
The presentation (see Table 1) and pre- and postpresentation data collection occurred during regular school hours in either a classroom or auditorium setting with the highlight being an autobiographical talk delivered by a woman with schizophrenia. She described her journey of recovery including her ongoing struggles with stigma and feelings of shame about seeking help.
Contents of Anti-Stigma Interactive Presentation.
Results
Social Distance and Knowledge About Schizophrenia
High school students demonstrated adequate basic knowledge of schizophrenia at baseline, with the average total score being approximately 7 out of 9 factual knowledge items answered correctly (M = 6.79, SD = 1.31). Following the anti-stigma presentation the average total score increased further to approximately 9 out of 9 items answered correctly (M = 8.82, SD = 0.59). Analyses were conducted to determine if this improvement was significant. Initial analyses determined that the assumption of normality was violated, likely because of the negative skew of the distribution of postpresentation knowledge scores where a ceiling effect was observed. Therefore, change scores were calculated from the pre- and postpresentation knowledge scores. Examination of the knowledge change score data resulted in a normal approximation. A simple sample t test assessed the expected mean change in factual knowledge of schizophrenia (M = 2.03, SD = 1.38) and the change was found to be significant, t(247) = 23.26, p < .001, 95% confidence interval (CI) = [1.86, 2.20]. Further review of mean item responses revealed that two false beliefs were prevalent among students prepresentation, namely the belief that people with schizophrenia have a split personality (53.1%) and the belief that people with schizophrenia are likely to be violent (31.7%).
A repeated measures analysis of covariance was conducted on pre- and postsocial distance towards schizophrenia scores with social desirability entered as a covariate. Analyses revealed a significant change over time in total social distance scores, F(1, 237) = 13.3, p < .001,
Self-Stigma of Seeking Help
Pre-intervention self-stigma levels in the high school student sample (M = 26.7, SD = 6.3) were found to be most comparable to those young adults not seeking treatment services (M = 27.3, SD = 6.6) in the SSOSH validation study (Vogel et al., 2006); whereas levels obtained following the intervention (M = 23.6, SD = 7.2) were most comparable to those individuals who were found to be willing to seek help if needed in the SSOSH validation study (M = 24.3, SD = 6.1). Using a cutoff score of 34 (1 SD above the Vogel et al. [2006] validation study mean) to categorize self-stigmatizing individuals, it was found that 12% of the high school sample showed significant levels of self-stigma, which was reduced to 8.8% following the intervention, reflecting a 27% improvement.
A repeated measures analysis of covariance was conducted on self-stigma of seeking help with self-stigma scores at both pre- and postpresentation entered as the dependent variables. Sex and ethnicity were entered as fixed factors. Age, familiarity with mental illness, self-esteem, and social desirability were entered as covariates.
Pillai’s F-trace statistic was reported as the Box test of equality of covariances was violated (p = .017). Results from the multivariate test showed a trend towards significance, V = .01, F(1, 223) = 2.32, p = .129,
Furthermore, the multivariate test found that the observed reduction in self-stigma scores from pre- to postpresentation interacted significantly with age, V = .02, F(1, 223) = 4.66, p = .032,
There was also a significant interaction obtained between familiarity with mental illness and time, V = .03, F(1, 223) = 6.07, p = .014,
In terms of between-subjects effects, a significant effect was found for self-esteem on self-stigma, F(1, 223) = 10.85, p < .001,
Finally, a significant between-subjects effect of social desirability on self-stigma was observed, F(1, 223) = 10.85, p < .001,
Discussion
Self-stigma was identified as a key obstacle to seeking help for mental health concerns among high school youth. A target group of about 12% of secondary school students in the sample was identified as having significant self-stigma at levels that would be considered a barrier to help seeking for mental health concerns. To our knowledge, the impact on self-stigma of a single-session anti-stigma presentation combining education and contact with a mental health service recipient has not been examined thus far in high school youth. The results of the current study suggest that classroom-based interventions are effective in producing beneficial reductions in self-stigma. Postpresentation levels of self-stigma among the high school youth were comparable to scores found among young adults in the Vogel et al. (2006) normative study who were interested in seeking help if needed, which suggests that the demonstrated improvements are in fact meaningful. Taken together, the current findings replicate and now extend to a classroom setting previous pilot research that had examined an experiential intervention with an international sample (Yau et al., 2011).
The current findings also support other research (Pinfold et al., 2005) by demonstrating that brief school-based stigma reduction programs can effectively enhance mental health literacy of serious mental illness, as well as reduce social distance towards mental illness, and schizophrenia in particular. Importantly, providing accurate information and hearing an autobiographical testimonial from an individual with serious mental illness dispelled the false belief held by a third of students in our sample that people with schizophrenia are violent. As well, reductions in behavioural discrimination against those with mental illness may help sensitize students to not only be more aware but also accepting and supportive of peers who struggle with mental and emotional concerns.
A secondary goal of the study was to identify risk factors associated with greater levels of self-stigma. Factors identified include younger age, lack of familiarity with mental illness, and low self-esteem. These results mirror findings in the literature with college and university samples but extend them to Canadian high school youth. However, the present study failed to replicate other findings suggesting that male college students showed greater self-stigma than their female counterparts. Further research is recommended to examine the extent of sex effects, as well as the influence of culture and ethnicity on self-stigma of seeking treatment.
The current study also found that lower self-stigma towards seeking help was associated with greater social desirability. It is hypothesized that self-reported levels of self-stigma were actually an underestimate of students’ true experience in this case. Students who scored highest on the social desirability measure may also be those who are most likely to hide any distress since having symptoms of mental illness is not “socially desirable.” The tendency to ‘hide’ distress, and in turn, to avoid seeking necessary help through a ‘cover’ of positive self-impressions has important implications for teachers, since it may impede the detection of at-risk students. Fortunately however, the anti-stigma intervention remained effective in reducing self-stigma of seeking help, even after accounting for the influence of social desirability, providing hope for students whose distress is less apparent.
Relevance for Education and Policy
There are key implications for high school curricula and mental health policies. The presence of self-stigma among high school students suggests that mental health education needs to be integrated directly into classroom studies as a way of reaching out to this vulnerable group. High school mental health studies should integrate contact with a mental health service recipient into the classroom alongside basic education about early signs and signals of mental health problems; such contact serves not only to foster tolerance but also may enhance appropriate opportunities for self-disclosure of help-seeking needs. Professional development for educators needs to provide information about the prevalence and nature of self-stigma as an under-recognized barrier to seeking treatment—that is, self-stigma may be under-reported and concealed due to shame—as well as provide training and resources to teachers for when a student fails to ask where to turn for help even when it seems to be required. The recommendation that opportunities need to be built into the curriculum for direct contact with a speaker who has mental illness requires not only changes to high school curricula but also to hospital and community mental health policies; there is a need for the development and increased funding for training programs for individuals with mental illness to develop their speaking skills and support their participation in classroom teaching. Forming collaborative partnerships in the planning and delivery of classroom sessions with individuals who have mental health concerns could have a positive impact on both the learning experiences of young people and the morale of mental health service users. It is crucial that high schools create or facilitate these opportunities for personal contact between students and people with mental illness since such approaches have been consistently shown to reduce stigma and now have been shown to be effective in reducing self-stigma.
Although the current results are encouraging, there are several limitations that should be noted. As with many other studies exploring the effectiveness of school-based anti-stigma programs among youth, it was not feasible to include a no-intervention control group. A follow-up assessment was also not conducted in the current research. Evidence from other studies assessing anti-stigma programs with youth suggest that improvements in knowledge, attitudes, and behaviours towards individuals with schizophrenia and other mental illnesses may be maintained in the short term (Pinfold et al., 2003), but generally dissipate over the longer term. Future studies should conduct long-term follow-up. In addition, the nature of the relationship between heightened self-stigma and lowered self-esteem, in particular, needs to be explored further including examination of the role of personality factors that may be associated with vulnerability to self-stigma.
Conclusions
Teaching about mental illness routinely involves basic instruction in factual information about symptoms but such knowledge delivery approach alone does not address a key problem that emotionally troubled high school youth may recognize that something is wrong yet nevertheless still conceal their inner struggles and not seek treatment. The current study identified that about one in eight high school students experience self-stigma, in which they feel a sense of shame about expressing aloud mental health concerns and feel self-conscious about seeking help. It was determined that a classroom-based presentation which incorporates contact with a mental health services recipient can produce significant reductions in self-stigma. Furthermore, the contact-based educational approach served to reduce social distance, that is, feeling more comfortable being around people with mental health concern; such findings suggest potential for sensitizing peers to be able to reach out to their fellow students rather than ostracize them. Low self-esteem, younger age, and lack of familiarity with mental illness were among the factors associated with self-stigma but more research is needed to explore self-stigma vulnerability issues in youth. Consideration should be given for incorporation of contact-based presentations into standard curriculum practice.
Footnotes
Acknowledgements
Thank you to Dr. Kathy Short and E-Best, the students, teachers, and principals of participating secondary schools from the Hamilton Wentworth District School Board. Thank you to the McMaster University medical student presenters and Liz for sharing her story.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a small grant from the Community Social Vocational Research CSVR Foundation to fund an honorarium for the mental health speaker. Gordon L. Flett was supported by a Canada Research Chair in Personality and Health.