
Abstract
Exposure to physical violence is an unfortunate reality for many Canadian youth as it is associated with numerous negative psychosocial effects. The study aims to assist in understanding resilience in rural Canadian youth exposed to physical violence. This is accomplished by identifying the importance of protective factors, as measured by the Resiliency Scale for Children and Adolescents (RSCA), and physical violence exposure, when used together, in predicting disruptive behavior, depression, and posttraumatic stress. Results indicate positive emotional reactivity is more important in protecting youth from developing psychological symptoms than sense of mastery and sense of relatedness. Differences between the effect of hearing reports, witnessing, and being victim to violence as well as differences between male and female youth were found. The study adds to the research on physical violence exposure, protective factors, and internalizing/externalizing problems in rural youth, with implications for implementing school-based programs.
Introduction
Exposure to violence is an unfortunate reality for many children and youth. Children are more likely than adults to be exposed to violence and crime whereas adolescents are more likely to be victims of violence than the general population (Finkelhor, Turner, Ormrod, Hamby, & Kracke, 2009). There are different types of violence exposure. Direct victimization includes assault, sexual assault, child maltreatment, and property victimization, whereas indirect victimization refers to witnessing violence across contexts and environments. In comparing the effects of direct and indirect victimization, findings suggest that direct victimization has more damaging effects (Ward, Martin, Theron, & Distiller, 2007; Weaver, Borkowski, & Whitman, 2008).
There is a great deal of overlap between the different types of violence experienced, as children and youth can be exposed to both direct and indirect victimization (Appel & Holden, 1998; Jouriles & LeCompte, 1991; Ward et al., 2007). For example, many children who are exposed to domestic violence are also victims of physical abuse (Appel & Holden, 1998; Jouriles & LeCompte, 1991). The degree to which youth are exposed to both direct and indirect victimization was revealed in a recent American study (Finkelhor, Turner, Shattuck, & Hamby, 2013). In the nation-wide survey conducted in 2011, both direct and indirect victimization was experienced by 22.4% of the children and youth with more than 41% experiencing a physical assault and 13.7% experiencing caregiver maltreatment (Finkelhor et al., 2013). With few significant changes since the last survey conducted (Finkelhor et al., 2009), the rates were still viewed as being high with complex interrelationships found to exist between the various forms of victimization. The authors concluded, unfortunately, that there is a lack of epidemiological data available on children and youth’s exposure to violence, victimization, and abuse, suggesting the need to address this gap (Finkelhor et al., 2013).
Physical violence exposure has been linked with numerous negative effects with support for a relationship between violence exposure, delinquency, and offending having been found (Brown, Henggeler, Brondino, & Pickrel, 1999; Weaver et al., 2008). Gang membership has been associated with violence exposure, as youth who were either currently or previously involved with gangs reported higher levels of exposure to violence than those with no previous gang involvement (Li et al., 2002).
Violence exposure is also related to alcohol and drug use. After accounting for the effects of demographic variables, as well as parent and sibling substance use, witnessing serious violence was associated with tobacco use, drunkenness, number of illicit drugs used, and drug/alcohol problems (Kliewer et al., 2006). In addition, violence exposure is linked with poor academic performance (Nettles, Mucherah, & Jones, 2000; Schwartz & Gorman, 2003) and negative school outcomes (i.e., high suspension and expulsion rates; Kennedy & Bennett, 2006). In a study of adolescent mothers, cumulative lifetime violence exposure was linked to attention and behavior problems in school, school suspensions, and expulsions (Kennedy & Bennett, 2006).
There appear to be sex differences related to violence exposure. First, male youth are exposed to higher levels of physical violence than female youth (Cooley-Quille, Boyd, Frantz, & Walsh, 2001; Farrell & Bruce, 1997; Hanson et al., 2008; Mendelson, Turner, & Tandon, 2010). Second, there are gender differences in the response to violence exposure. Studies report that males are more likely to experience externalizing problems, such as aggression, whereas females are more likely to experience internalizing problems, such as depression and somatic complaints (Cooley-Quille et al., 2001; Foster, Kuperminc, & Price, 2004; Hanson et al., 2008; Hertweck, Ziegler, & Logsdon, 2010).
However, not all youth exposed to violence develop internalizing or externalizing problems (Fergusson & Horwood, 2003; Richters & Martinez, 1993; Werner & Smith, 1992). Research has consistently found that it is unusual for more than half of the children exposed to risk factors to develop serious disabilities or persistent problems (Rutter, 1985; Werner & Smith, 1992). Such findings support the theory of resilience, which states that there is some form of dynamic process surrounding positive adjustment under challenging life conditions that protects against the negative effects of adversity (Rutter, 1985). Resilience has been described as a process rather than a trait, and to be considered resilient, one must be exposed to a significant threat or severe adversity and attain positive adjustment in spite of the threat or adversity (Luthar, Cicchetti, & Becker, 2000). Alternatively, Masten (2001) suggests that resiliency is a characteristic of normal development and not only relevant to those exposed to adversity.
Prince-Embury (2006) identified three constructs that could be used together as a framework for understanding personal resilience and developed an assessment tool for its measurement. The Resiliency Scale for Children and Adolescents (RSCA, Prince-Embury, 2006) holds the underlying premise that personal resilience is multidimensional rather than a one-dimensional (i.e., resilient or not resilient) or two dimensional (i.e., protective vs. risk) model (Prince-Embury & Courville, 2008b). The RSCA is comprised of three core developmental factors of personal experience: sense of mastery, sense of relatedness, and emotional reactivity and the relationships between these factors (Prince-Embury, 2011, 2013). Sense of mastery is the ability to interact with and benefit from cause-and-effect relationships in the environment (Prince-Embury, 2008a). It includes optimism, self-efficacy, and adaptability. Sense of relatedness is defined as the experience of trust, comfort with others, perceived access to support, and tolerance of differences. Emotional reactivity is the inability to modulate, manage, and tolerate emotional arousal.
Studies have confirmed the three-factor structure (Prince-Embury & Courville, 2008a) and the use of the RSCA for female and male youth between 9 and 18 years old (Prince-Embury, 2013; Prince-Embury & Courville, 2008b). Research has found strong correlations between sense of mastery, sense of relatedness, and emotional reactivity and internalizing and externalizing problems (i.e., depression, anxiety, and disruptive behavior; Prince-Embury, 2008a). Preliminary results examining the relationship between the RSCA and child self-reports of bullying and victimization have found sex differences to exist, with emotional reactivity being positively correlated for males and sense of mastery and sense of relatedness negatively correlated for females (Prince-Embury, 2013). Replication of these results is suggested as a small sample was drawn from children 9 to 14 years of age (Prince-Embury, 2013). The RCSA has also been reported to be a useful tool for understanding, assessing, and enhancing resilience in the school setting (Prince-Embury, 2008b, 2011, 2013).
Purpose
The purpose of this study is to determine whether sex, personal protective factors (measured by the RSCA), and physical violence exposure (measured by the Children’s Report of Exposure to Violence) are predictive of internalizing or externalizing problems (measured by the Beck Depression Inventory, Beck Disruptive Behaviour Inventory, and Child PTSD Symptom Scale) in rural Canadian adolescent youth. Physical violence is defined as a deliberate act intended to cause physical harm against a person (Cooley, Turner, & Beidel, 1995). These acts include beating (i.e., punching, kicking, or biting someone so badly that they were hurt), chasing or threatening, robbing or mugging, and shooting or stabbing another individual. This study did not discriminate between the environment in which the violence occurred (i.e., home, school, or neighborhood) and sexual violence was not examined.
There is a lack of empirical research on physical violence exposure in the rural Canadian adolescent population. The majority of studies on physical violence exposure have been conducted in the United States (Finkelhor et al., 2009; Finkelhor et al., 2013; Shukla & Weisner, 2013) or in countries exposed to war or extremely high violence rates (Barbarin, Richter, & deWet, 2001; Kliewer et al., 2006; Ward et al., 2007). Nevertheless, physical violence remains a very real problem among children and youth in Canada (Statistics Canada, 2001, 2005). Considering adolescents are at a greater risk for violence (Wolfe, Jaffe, & Crooks, 2006) and more likely to be victims of violence than the general population (Finkelhor et al., 2009), a focus on adolescent youth is needed. The present study, then, is an important first step in exploring the problem of rural adolescent physical violence exposure in Canada.
Method
A total of 162 participants were included in the analyses, of which 55% were male and 45% were female (see Table 1). Participants ranged from 16 to 18 years, with the majority (90%) between the ages of 16 and 17 years. Data were collected from the five schools that volunteered to participate, two from one division and three from another. The schools in the two divisions are located in smaller communities with populations between 900 and 5,500 people.
Participant Demographics.
The Children’s Report of Exposure to Violence (CREV) is a self-report survey that was used to measure the level of physical violence exposure (Cooley et al., 1995). The three subscales of this measure made up the three modes of violence explored: hearing reports, witnessing, and being victim to violence. The questions do not differentiate between physical violence experienced in the home, school, or neighborhood. The survey consists of 32 items, 29 of which are rated on a 5-point Likert-type scale, ranging from 0 (never) to 4 (everyday). The CREV has been used with participants up to 18 years old (Cooley-Quille et al., 2001) and has good test–retest reliability (r = .75), internal consistency (α = .78), and evidence of construct validity (Cooley et al., 1995).
The RSCA (Prince-Embury, 2006) was used to measure protective factors. The RSCA is a self-report survey composed of three scales that measure the protective personal characteristics: sense of mastery, sense of relatedness, and positive emotional reactivity. The Sense of Mastery Scale and the Emotional Reactivity Scale consist of 20 items, whereas the Sense of Relatedness Scale consists of 24 items. All three scales are rated on a 5-point Likert-type scale, ranging from 0 (never) to 4 (almost always), which results in total scores ranging from 0 to 80 for the Sense of Mastery and Emotional Reactivity Scales and 0 to 96 for the Sense of Relatedness Scale. High scores on the Sense of Mastery and Sense of Relatedness Scales are associated with higher levels of resilience and low scores on the Emotional Reactivity Scale are associated with higher levels of resilience. The Emotional Reactivity Scale was reverse-scored and referred to as positive emotional reactivity (i.e., the ability to modulate, manage, and tolerate emotional arousal) for ease of interpretation. All three scales of the RSCA have good to high test–retest reliabilities (ranged from r = .79 for Sense of Mastery to r = .88 for Emotional Reactivity), high to excellent internal consistency (ranged from α = .85 for Sense of Mastery to α = .95 for Emotional Reactivity), and evidence of construct validity (Prince-Embury, 2006, 2013; Prince-Embury & Courville, 2008a).
The internalizing and externalizing problems explored were depression, disruptive behavior, and posttraumatic stress disorder (PTSD) symptoms. Depression and disruptive behaviors were measured with the Beck Depression Inventory for Youth (BDI-Y) and the Beck Disruptive Behaviour Inventory for Youth (BDBI-Y), respectively, from the Beck Youth Inventories Second Edition for Children and Adolescents (BYI-II; Beck, Beck, Jolly, & Steer, 2005). The scales consist of 20 items rated on a Likert-type scale, ranging from 0 (never) to 3 (always). Total scores for each scale range from 0 to 60. Higher scores are associated with higher levels of depression and disruptive behaviors. Both scales have high to excellent internal consistency (α ranging from .86 to .96) and good to excellent test–retest reliabilities (r ranging from .74 to .93) for all age groups and genders, as well as evidence of validity (Beck et al., 2005).
PTSD symptoms were measured with the Child PTSD Symptom Scale (CPSS; Foa, Johnson, Feeny, & Treadwell, 2001). The CPSS was designed to assess PTSD symptom severity in children and youth between the ages of 8 and 18 (Foa et al., 2001). Evidence supports the CPSS as a reliable and valid instrument (Foa et al., 2001). It has very good to excellent internal consistency (α ranging from .70 for the Arousal subscale to .89 for the total score), moderate to excellent test–retest reliability (kappa = .55 for symptom diagnosis and between .63 and .84 for symptom severity scores) for the overall scale and three subscales, very good convergent validity with another measure of PTSD (r = .80), and satisfactory divergent validity (Foa et al., 2001).
Correlation analyses were used to determine whether the protective factors and physical violence exposure were significantly correlated with the internalizing and externalizing problems. Multiple regression was used to determine whether protective factors (sense of mastery, sense of relatedness, and emotional reactivity) and modes of physical violence exposure (hearing reports, witnessing, or being victimized) predicted disruptive behavior, depression, or PTSD symptoms. The aim was also to identify differences in the predictive power of the protective factors and modes of physical violence exposure. Subscales of the CREV were used instead of total violence exposure to determine whether one of the subscales more strongly predicted the internalizing/externalizing problems.
Previous research ordered the variables using hierarchical multiple regression (see Brown et al., 1999; Ozer, 2005; Youngstrom, Weist, & Albus, 2003). The present study performed stepwise multiple regression analyses for two reasons. First, the RSCA and subscales of the CREV have not been used in this area of research. Through stepwise multiple regression, the amount of variance accounted for by each variable can be explored at the same time as the other variables rather than using theory to order the variables into the regression (Tabachnick & Fidell, 2007).
Two sets of multiple regressions were run for each criterion variable. The first set used stepwise regression with the total sample to determine the amount of variance accounted for by each predictor variable. The second set was separated by sex and run using standard regression due to the relatively small number of cases with respect to the number of predictor variables, as suggested by Brace, Kemp, and Snelgar (2010). Dividing the sample resulted in a small sample size for each sex and a decrease in power. Therefore, a p value of .10 was used to decrease the chance of Type-II errors. A p value of .05 was used for regressions that included the total sample. Age was not included considering the majority of participants fell between 16 and 17 years.
Results
Descriptive statistics revealed that the participants were exposed to high rates of physical violence. Almost all (99%) had heard about at least one act of physical violence in their life, with 73% witnessing at least one act of violence, and 58% reporting being victim to at least one act of violence. A large percentage of adolescent youth (78%) were exposed to physical violence as a witness or victim one or more times. Interestingly, half (51%) of the sample were both witnesses and victims of physical violence, with another 21% reporting to be only witnesses and 6% only victims.
Of all the violent events that were witnessed, seeing someone you know being beaten up was the most common, with more than 60% witnessing this occur. The second most common event was seeing a stranger being beaten up. A number witnessed someone being shot or stabbed (14% witnessed a stranger and 12% witnessed someone they knew) and a few even reported being a victim of a shooting or stabbing (6%). The most common event that adolescent youth were victimized by was being chased or seriously threatened (42%), followed by being beaten up (38%).
Correlations between all predictor and criterion variables are found in Table 2. All three protective factors were significantly correlated with all three types of exposure to physical violence. All were small to moderate negative correlations. The total and subscale (Hearing Reports, Witnessing, and Victim) scores of the CREV were all moderately and positively correlated with disruptive behavior, depression, and PTSD symptoms. Of the internalizing/externalizing problems, disruptive behavior had the largest correlation with total physical violence exposure and each subscale of the CREV, with the exception of Hearing Reports, which was more strongly correlated with depression. PTSD symptoms had the smallest correlations with the total and subscale scores.
Correlations Between Variables.
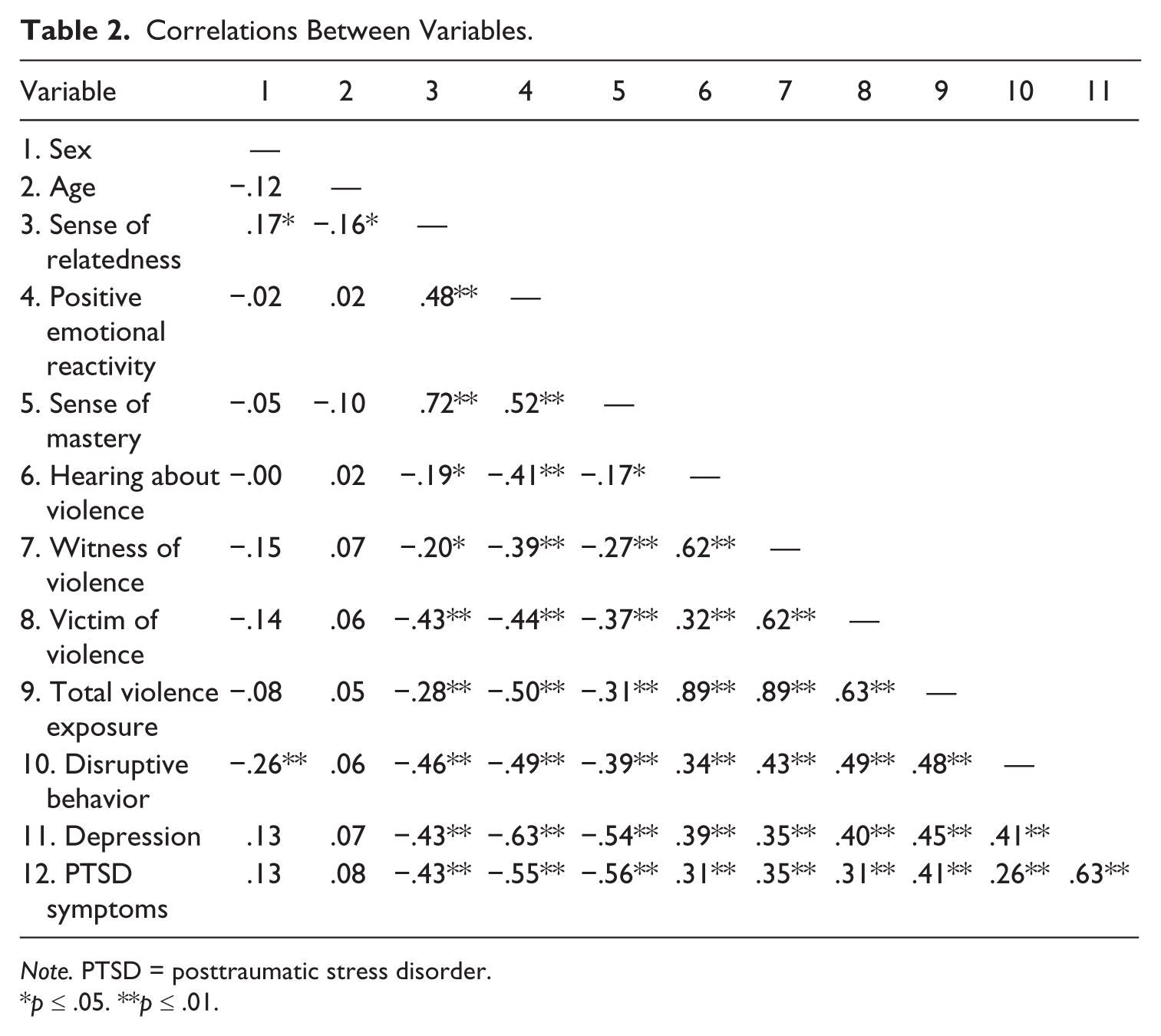
Note. PTSD = posttraumatic stress disorder.
p ≤ .05. **p ≤ .01.
The initial analysis sought to determine whether the protective factors (sense of relatedness, sense of mastery, or positive emotional reactivity) and the different modes of physical violence exposure (hearing reports, witnessing, or being victim) were significant predictors of disruptive behavior when used together. The results indicate that sense of relatedness, witnessing violence, and positive emotional reactivity are important predictors of disruptive behaviors (see Table 3). When analyzing the total sample with stepwise regression, 39% of the variance was accounted for in the final model, F(3, 132) = 27.60, p < .001, with sense of relatedness, witnessing physical violence, and positive emotional reactivity identified as significant predictors of disruptive behavior. Sense of relatedness was the strongest predictor and accounted for 24% of the variance in disruptive behavior with an additional 12% of the variance accounted for by witnessing violence. Positive emotional reactivity accounted for an additional 3% of the variance. Thus, high scores in disruptive behavior were associated with high scores in witnessing physical violence and low scores in sense of relatedness and positive emotional reactivity.
Stepwise Multiple Regression Predictions.
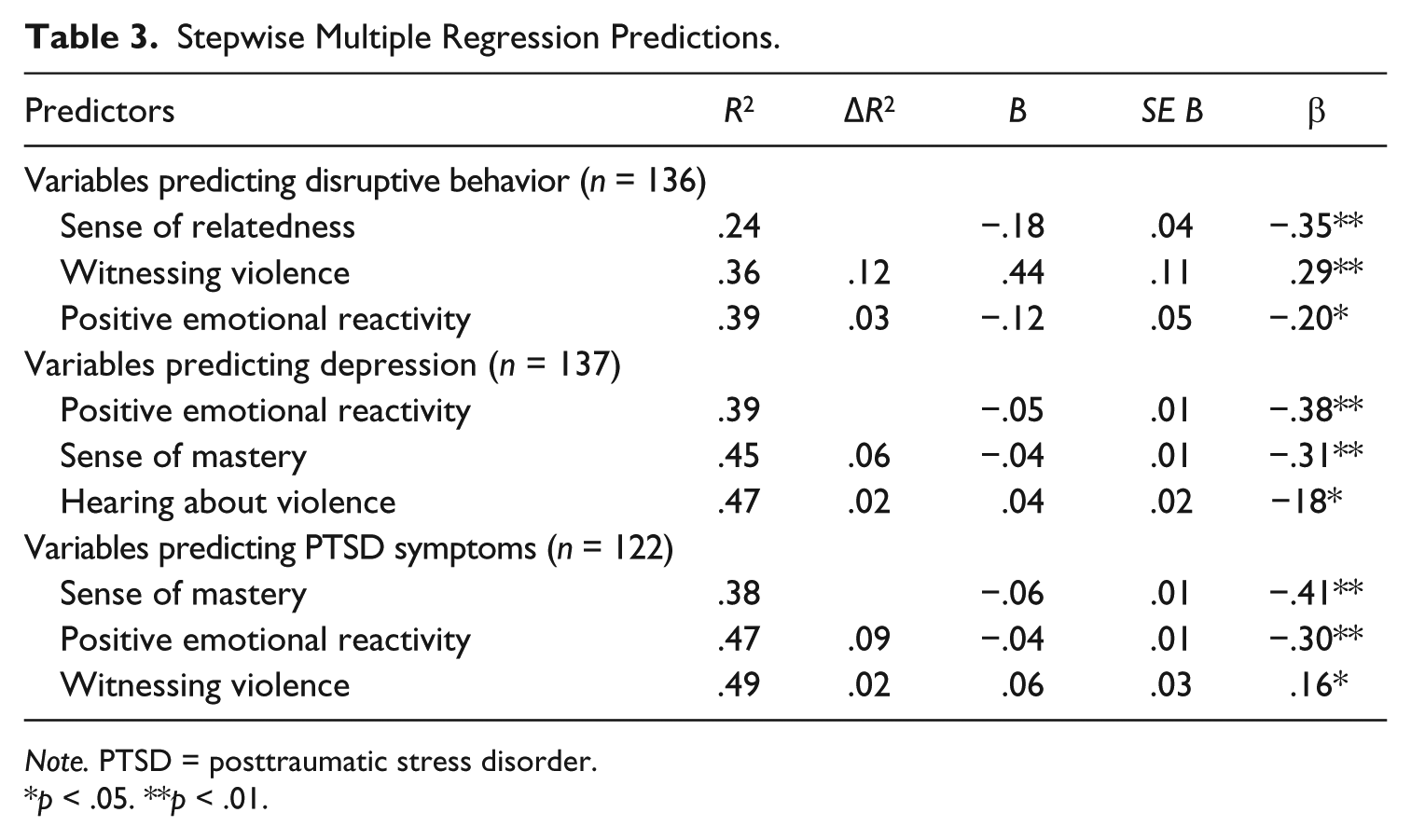
Note. PTSD = posttraumatic stress disorder.
p < .05. **p < .01.
After splitting the sample by sex, the regression revealed some interesting sex differences (see Table 4). Only 36% of the variance in disruptive behavior in males was accounted for by the predictor variables, F(6, 69) = 6.57, p < .001, whereas 52% of the variance was accounted for in females, F(6, 53) = 9.56, p < .001. For the males, the only significant predictor of disruptive behavior was hearing reports of physical violence, with higher levels of disruptive behavior associated with hearing more reports. Conversely, for females, sense of relatedness and being a witness of violence were significant predictors of disruptive behavior. High levels of sense of relatedness and low levels of witnessing violence were associated with lower levels of disruptive behavior. The strongest predictor according to the β value was witnessing violence, followed by sense of relatedness.
Standard Multiple Regression Predictions for Disruptive Behavior by Sex.
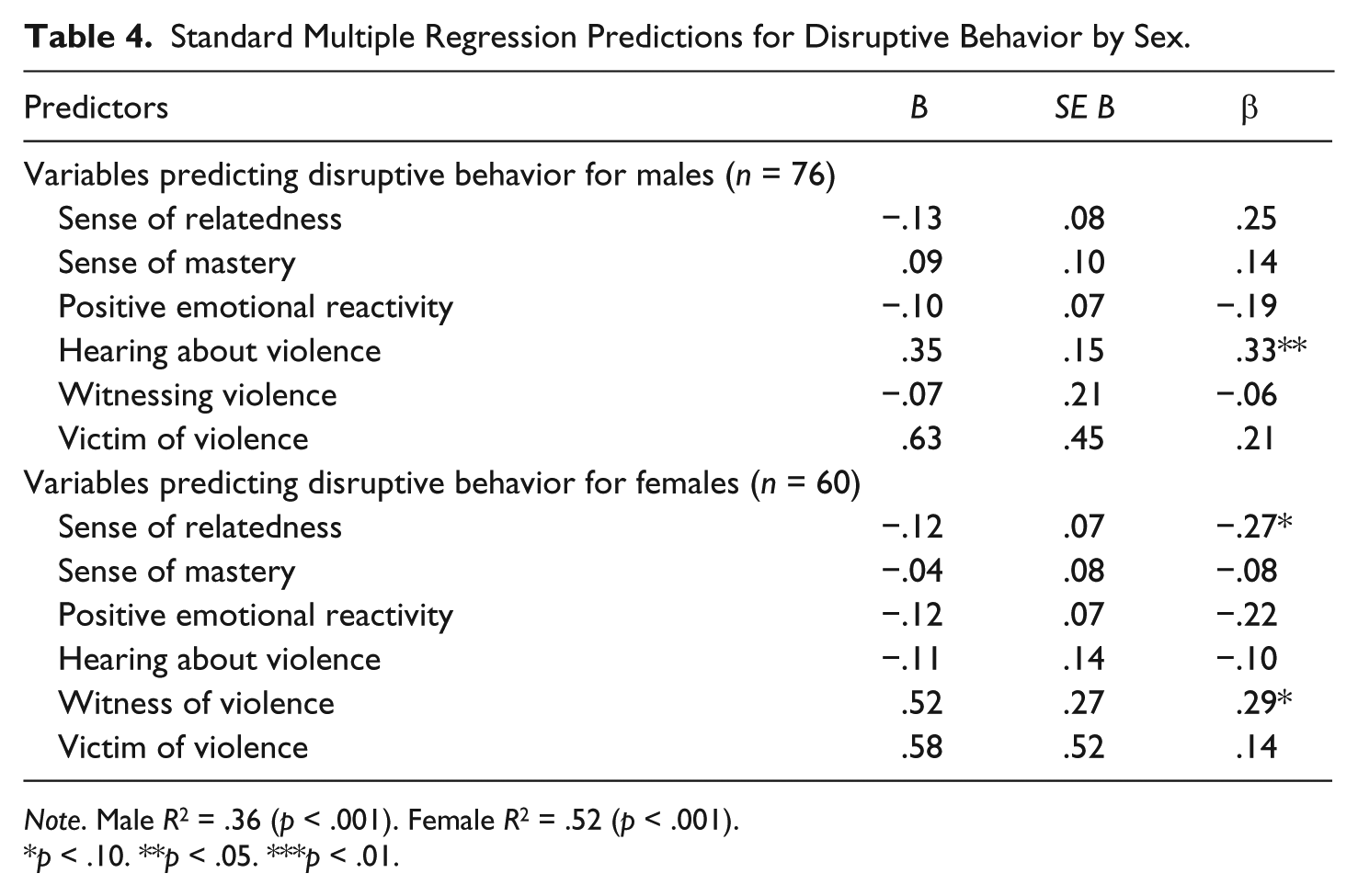
Note. Male R2 = .36 (p < .001). Female R2 = .52 (p < .001).
p < .10. **p < .05. ***p < .01.
This study also sought to determine the importance of the protective factors (sense of relatedness, sense of mastery, or positive emotional reactivity) and the different modes of exposure to physical violence (hearing reports, witnessing, or being victim) when used together to predict depression.
For the total sample, positive emotional reactivity, sense of mastery, and hearing reports of violence were significant predictor variables (see Table 3). Thirty-nine percent of the variability in depression was accounted for by positive emotional reactivity. An additional 6% of the variance was accounted for by sense of mastery and another 2% was accounted for by hearing about violence, resulting in a final model that accounted for 47% of the variance in depression, F(3, 133) = 41.57, p < .001.
Once the sample was divided by sex, positive emotional reactivity was the only significant predictor for both males and females (see Table 5). Again, more variance was accounted for in the female regression at 54%, F(6, 52) = 8.73, p < .001, than the male regression at 46%, F(6, 69) = 8.38, p < .001.
Standard Multiple Regression Predictions for Depression by Sex.
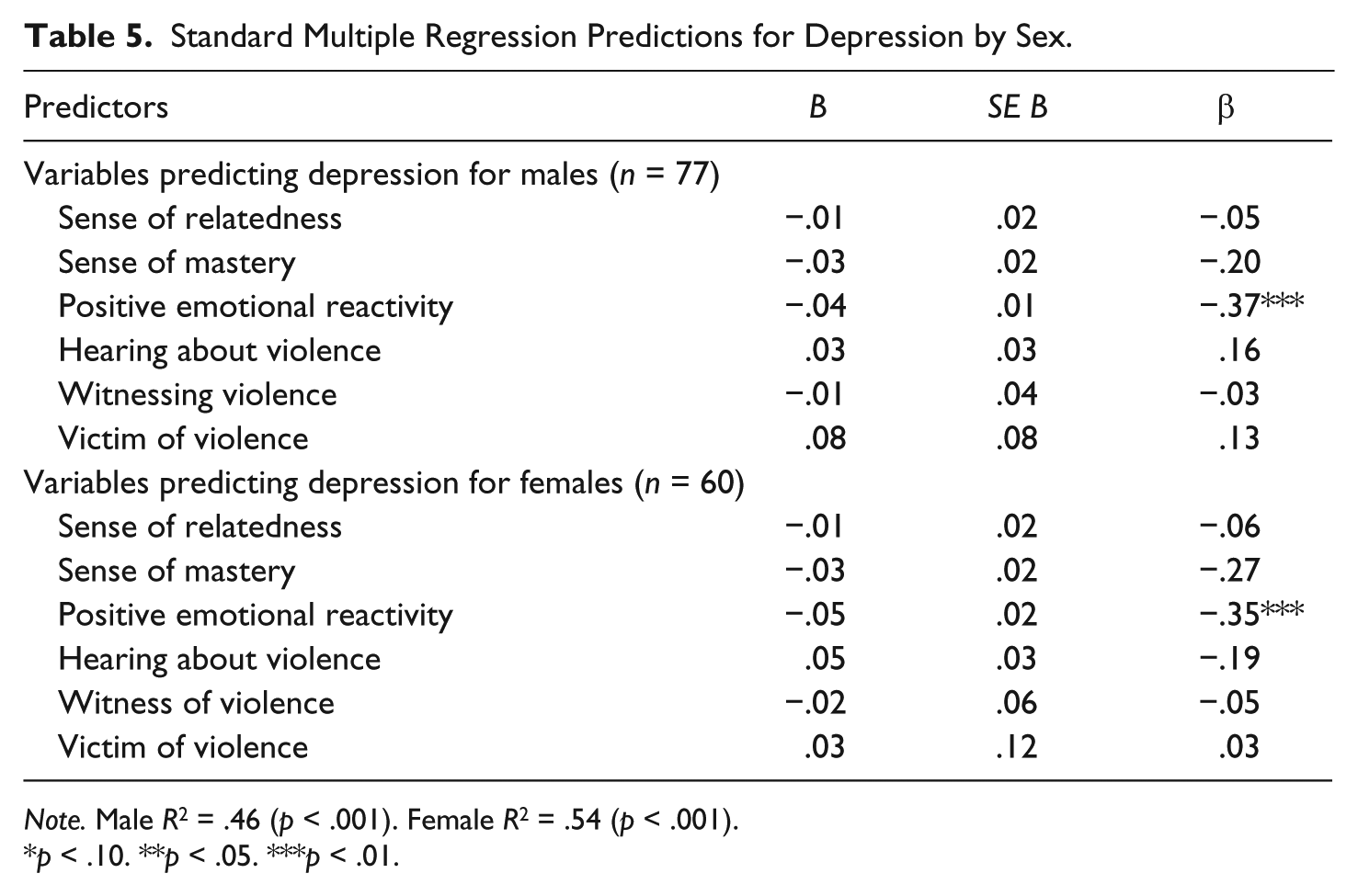
Note. Male R2 = .46 (p < .001). Female R2 = .54 (p < .001).
p < .10. **p < .05. ***p < .01.
Finally, this study sought to determine the importance of the protective factors (sense of relatedness, sense of mastery, or positive emotional reactivity) and the different modes of exposure to physical violence (hearing reports, witnessing, or victim of violence) when used together to predict symptoms of PTSD. Sense of mastery, positive emotional reactivity, and witnessing violence were found to be significant predictors of PTSD symptoms in the stepwise regression (see Table 3). Sense of mastery accounted for 38% of the variance in PTSD symptoms, positive emotional reactivity accounted for 9% of the variance, and witnessing violence accounting for an additional 2% of the variance, resulting in a final model that accounted for 49% of the variance in PTSD symptoms, F(3, 118) = 37.90, p < .001.
Regressions run for each sex revealed that for males, 40% of the variability in PTSD symptoms was accounted for by the predictor variables, F(6, 60) = 5.69, p < .001, compared with 65% of the variance for females, F(6, 46) = 14.97, p < .001 (see Table 6). Sense of mastery and positive emotional reactivity were found to be significant predictors of PTSD symptoms for males as well as for the females. According to the β value, sense of mastery was the strongest predictor for males and sense of mastery and positive emotional reactivity were equally predictive of PTSD symptoms for females. However, for females, witnessing violence and being a victim of violence were also significant. As exposure to these types of physical violence increased, so did PTSD symptoms.
Standard Multiple Regression Predictions for PTSD by Sex.
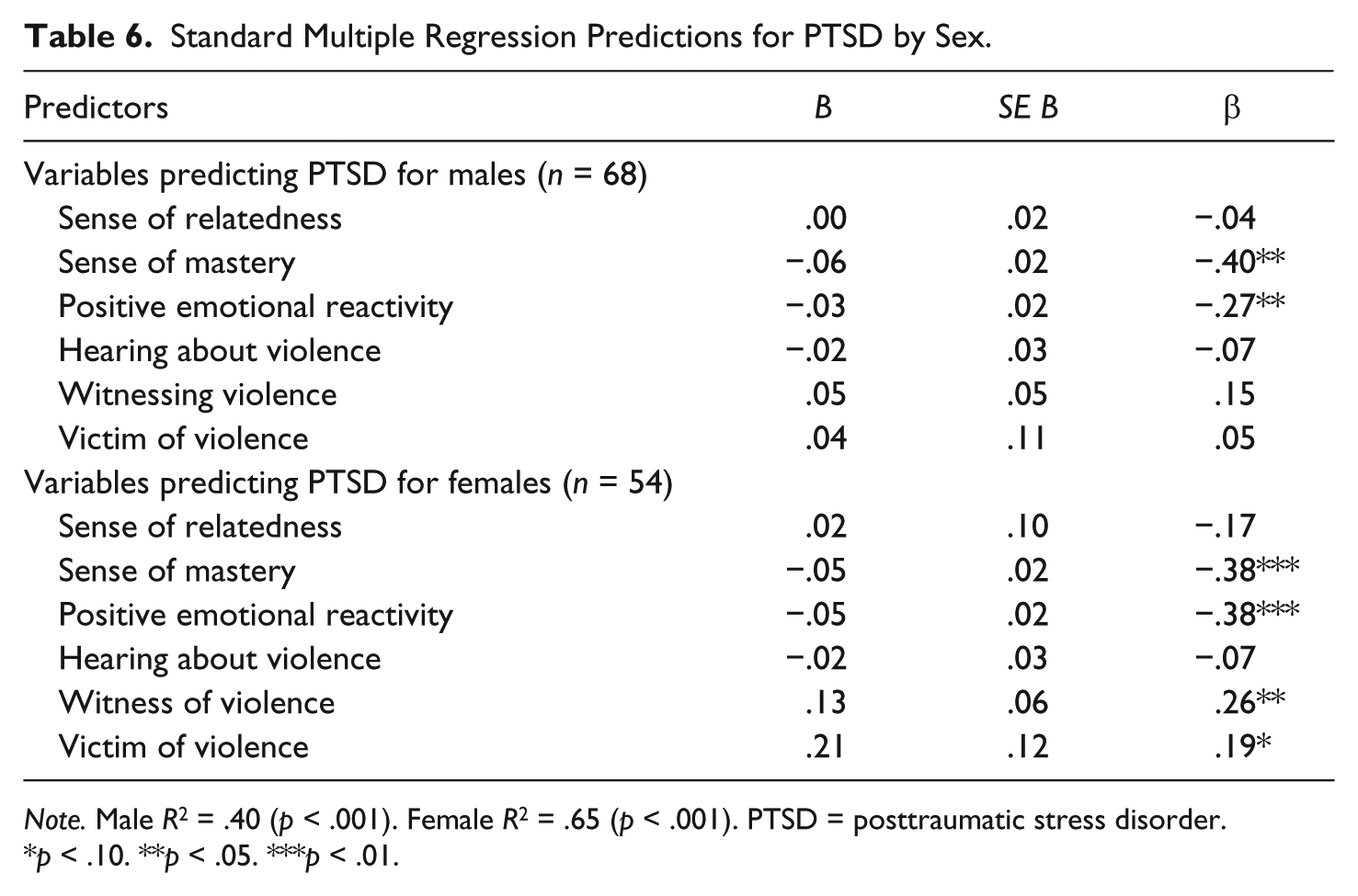
Note. Male R2 = .40 (p < .001). Female R2 = .65 (p < .001). PTSD = posttraumatic stress disorder.
p < .10. **p < .05. ***p < .01.
Discussion
The rates of physical violence exposure in this rural Canadian sample were higher than that found by Sullivan, Farrell, Kliewer, Vulin-Reynolds, and Valios (2007). In their rural American sample, 50% of youth were exposed to violence as a witness or victim one or more times, compared with 78% of this sample (Sullivan et al., 2007). However, the American study was drawn from Grade 6 students, with the younger age likely accounting for the difference.
When the results of a comparable age group in the National Survey of Children’s Exposure to Violence are examined (Finkelhor et al., 2013), it is found that American youth (i.e., both urban and rural) in the 14- to 17-year age range experienced rates of indirect victimization (i.e., witnessing violence) comparable to those found in the present study. For example, this study found that 73% of the participants reported witnessing at least one act of violence in their life. Similarly, Finkelhor et al. (2013) reported 71.5% of adolescents witnessed an act of violence in their lifetime.
The protective factors associated with low levels of internalizing/externalizing problems do not appear to differ between males and females. Emotional reactivity was an important predictor of disruptive behavior, depression, and PTSD symptoms, whereas sense of mastery was an important predictor of depression and PTSD symptoms. Sense of relatedness was only important in the prediction of disruptive behavior. These results support past research by Prince-Embury (2008a, 2013), which found emotional reactivity to be more strongly related to psychological symptoms than sense of mastery and sense of relatedness. The ability to regulate one’s emotional reaction and recover when upset seems to be important in protecting individuals exposed to adversity from developing internalizing and externalizing problems.
Future research should explore whether the protective factors studied provide a buffer against the negative effects of physical violence exposure. If the protective effect exists, it would be interesting to learn whether it follows a similar pattern to the results found here, with positive emotional reactivity protecting against disruptive behavior, depression, and PTSD symptoms with sense of mastery protecting against depression and PTSD symptoms, and with sense of relatedness protecting against disruptive behavior. It would also be interesting to explore whether these protective factors buffer against other problems associated with physical violence exposure, such as gang membership, drug use, or academic difficulties.
On their own, the correlations suggest that physical violence exposure is associated with internalizing/externalizing problems, supporting much of the previous research on violence exposure (Benhorin & McMahon, 2008; Gorman-Smith & Tolan, 1998; Myers & Thompson, 2000; Weaver et al., 2008; Youngstrom et al., 2003). More specifically, the consistent relationship that violence exposure has been found to have with PTSD (Cooley-Quille et al., 2001; Ozer, 2005) and disruptive behavior (Benhorin & McMahon, 2008; DuRant et al., 2000; Weaver et al., 2008) would be supported further, and the inconsistent relationship between depression and violence exposure would be clarified (Gorman-Smith & Tolan, 1998). However, results suggest that the relationship between these variables are more complicated and need to take sex into account.
Hearing reports, but not witnessing or being victim to physical violence, was identified as an important predictor of depression. This finding adds to the mixed results found in the literature. Previous research focused on exposure to violence in general (Cooley-Quille et al., 2001) or the difference between witnesses and victims of violence (Fitzpatrick, 1993), but did not include hearing reports of violence. It is possible that previous studies that did not find a link between violence exposure and depression (Cooley-Quille et al., 2001; Hanson et al., 2008) may have found different results if hearing about violence was explored.
It is unclear why this relationship occurs when more direct experiences with physical violence do not predict depression. One potential explanation is that individuals with higher depressive symptoms see the world through a negative filter, and therefore, negative events such as violent incidents might be exaggerated or more salient in their memory than those with less depressive symptoms. A recent study by Cammack, Lambert, and Ialongo (2011) provides further insight. The researchers broke their sample into four groups based on participants’ level of community violence exposure and level of perceived neighborhood violence. Their results revealed that among those with low community violence exposure, those with high perceived neighborhood violence were more anxious, depressive, and aggressive than those with low perceived neighborhood violence. It is possible that in the present study, those who reported hearing about many physical violent incidents, also perceived their neighborhood as being more violent than those who reported hearing about fewer violent incidents, which supports the explanation described above. Holding the perception that there is a high risk of physical violence may be more related to depression than actual experience with violence.
Surprisingly, for males, witnessing and being a direct victim of physical violence did not improve the prediction of any of the internalizing/externalizing problems explored in this study, suggesting that exposure to violence does not predict disruptive behavior, depression, or PTSD symptoms in males. This raises the question of whether exposure to physical violence has a different impact on males than females or whether an unknown factor led to non-significant results.
For males, hearing reports of physical violence seemed to be associated with symptoms of psychopathology, more specifically, depression and disruptive behavior. However, the relationship with disruptive behavior remains unclear. Research suggests that females view physical aggression as less acceptable than males (Pepler & Craig, 2005) and have different moral reasons for understanding why aggression is wrong (Murray-Close, Crick, & Galotti, 2006). Females are more likely than males to view physical aggression as morally wrong because it could harm someone, whereas males are more likely to view physical aggression as a matter of social convention or personal choice (Murray-Close et al., 2006). Therefore, it is possible that as males hear more stories about violent incidents, they begin to view these types of behaviors as socially acceptable and, consequently, are more likely to engage in them. In addition, it was found that the females who did believe physical aggression was a matter of social convention were also more likely to engage in aggressive behavior than the females with other moral reasoning for understanding why aggression is wrong (Murray-Close et al., 2006). Thus, females may not be as influenced by stories of physical violence because they are less likely to view physical aggression as a matter of social convention. Nevertheless, those who do, may be just as likely as males to view aggression as socially acceptable with repeated exposure to stories of physical violence.
As this study relies heavily on correlation analysis, the opposite could also be true. It may be that males who engage in disruptive behaviors also take part in story telling about violent incidents, seek out such information, or have increased awareness of these types of stories, whereas females, because of differences in socialization, are not as preoccupied with violence. Regardless of whether the disruptive behavior leads to hearing more reports of violence or hearing more reports of violence leads to more disruptive behavior, research consistently suggests that males are more likely to engage in aggressive or violent behaviors (Crooks, Scott, Ellis, & Wolfe, 2011; Jagers, Sydnor, Mouttapa, & Flay, 2007), be exposed to physical violence (Cooley-Quille et al., 2001; Hanson et al., 2008; Mendelson et al., 2010), and hold accepting beliefs about aggression and violence (Murray-Close et al., 2006).
Females who witness a high level of physical violence might follow a similar path toward disruptive behavior as described for males who experience hearing about high levels of violence. Female disruptive behavior could be influenced by the amount of times they witnessed violent incidents, or conversely, because they are more disruptive, they are more likely to witness violence. It is unclear though, why hearing reports of violence but not witnessing violence would predict disruptive behavior in males.
Finally, being victim to physical violence was only found to be important in the prediction of PTSD symptoms in females. These results further complicate discrepancies found in past research. Much of the older research has found a relationship between direct and indirect violence exposure and PTSD symptoms (Fitzpatrick & Boldizar, 1993; Martinez & Richters, 1993; Osofsky, Wewers, Hann, & Fick, 1993). In the present study, both witnessing and being victim to physical violence predicted PTSD symptoms for females, whereas for males, neither direct nor indirect violence exposure predicted PTSD symptoms. These results are in line with a study by Hanson et al. (2008) which found that females who experienced violence were more likely than males to meet PTSD criteria.
Furthermore, previous research has found women with a history of childhood sexual abuse to be at risk of further abuse (Pope, 1999; Sachs-Ericsson, Blazer, Plant, & Arnow, 2005). Other types of violence (i.e., sexual) were not explored in this study; therefore, it is unknown whether previous sexual abuse was a confounding variable that influenced the relationship between violence exposure and PTSD symptoms for females.
Interestingly, in the present study, disruptive behavior and depression were more highly correlated with violent victimization than PTSD symptoms. Yet, being victim to physical violence was only important in the prediction of PTSD symptoms. These results suggest that there may be a third confounding variable responsible for the relationship between disruptive behavior, depression, and violent victimization. Previous research found that being a victim of violence was important in the prediction of other internalizing and externalizing problems; however, the protective factors that include sense of mastery, sense of relatedness, and emotional reactivity were not considered (McGee, 2003). Perhaps these protective factors or one of the other modes of violence exposure are responsible for the relationship often found between victimization and internalizing/externalizing problems other than symptoms of PTSD. Future research should explore interactions between protective factors and exposure to physical violence to better understand these relationships.
Educating youth on the realities associated with physical violence might help them better understand the potential negative effects and decrease the number who approve of aggression as a social response and perceive positive outcomes for using aggression. Education on the effects of violence is also needed so that witnesses and victims of violence become aware of their risk of getting caught in the cycle of violence.
Future preventative programming should focus on building skills related to the protective factors explored in this study. Emotional reactivity was important in the prediction of disruptive behavior, depression, and PTSD symptoms. Therefore, as Prince-Embury (2008a, 2013) suggests, interventions should focus on improving children and youth’s emotional reactivity to help individuals become less sensitive and more able to deal with and recover from negative emotions. In addition to improving one’s emotional reactivity, interventions directed at decreasing PTSD symptoms could also include strategies that increase one’s optimism, self-efficacy, and adaptability, as it was found that sense of mastery was important in the prediction of PTSD symptoms. Similarly, interventions directed at decreasing disruptive behaviors could also include strategies that increase one’s experience of trust, comfort with others, perceived access to support, and tolerance of differences, considering sense of relatedness was important in the prediction of disruptive behaviors.
Prince-Embury (2011, 2013) also describes how the RSCA can be used as an assessment tool of personal resilience in the school environment. By assessing students’ sense of mastery, sense of relatedness, and emotional reactivity, they can be screened for their strengths as well as risk for developing problems such as disruptive behavior, depression, and PTSD symptoms. Preventative programming could then be provided to those students or classrooms most at risk. This type of intervention may help to bridge the gap in mental health services available to rural youth given the high levels of violence exposure found in this study. Preventative programming and school-based interventions access a large number of youth and in a cost and time efficient manner. Prince-Embury (2008b) provides examples of school-based interventions that foster positive emotional reactivity, sense of relatedness, and sense of mastery. As well, inclusion of personal protective factors that can be targeted in school-based programs fits with the approach suggested by the Mental Health Commission of Canada. Some of the strategies advocated include focusing on the prevention of mental illness, promoting mental health in school, reducing disparities in risk factors and access to mental health services, and strengthening the response to needs of diverse communities (Mental Health Commission of Canada, 2012).
The study is limited by the small sample size for the number of predictor variables. Furthermore, only one domain of resilience (i.e., emotional resilience) was measured. Future research should explore the predictive power of the different modes of physical violence, sense of mastery, sense of relatedness, and emotional reactivity on other domains of resilience (i.e., academic, social, etc.) as suggested by Luthar et al. (2000).
In conclusion, this study adds to the body of research examining relationships between physical violence exposure, protective factors, and internalizing/externalizing problems. Few studies have explored these relationships in rural or in Canadian samples. This study does both. Nevertheless, owing to the dearth of research available and the high rates of violence exposure experienced by youth, a more concerted and systematic effort is advocated to address the gaps that exist.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received financial support from the Social Science and Humanities Research Council Joseph Bombardier Canada Graduate Scholarship.