
Abstract
The purpose of this study was to investigate the self-perception bias (SPB) in adolescents with attention-deficit hyperactivity disorder (ADHD). The SPB was defined as adolescent underestimation of their learning and behavior problems in comparison to parent- or teacher-reports or a standardized achievement test. The sample comprised 74 adolescents, ages 13 to 18 (40 ADHD; 34 comparison). Compared to adolescents without ADHD, adolescents with ADHD underreported their symptoms and impairment when parent-reports, but not teacher-reports were the indicator of performance. Adolescents with ADHD, however, reported more difficulties in all areas of functioning than adolescents without ADHD. In the sample of adolescents with ADHD, self- and parent-reports of learning problems, but not teacher-reports, were significantly associated with adolescent total academic achievement test score. Adolescents with learning problems as measured by the achievement test, and social problems as rated by parents, reported higher levels of these difficulties than adolescents whose functioning was in the average range; however, adolescents with clinical levels of oppositional behaviors, as rated by parents or teachers, did not report elevated levels of these behaviors. Depressive symptoms were associated with a lower SPB. Implications of these findings for psychologists’ use of self-report measures with adolescents with ADHD are discussed.
School psychologists rely on teacher-report and parent-report rating scales to assess the social and emotional functioning of children who are referred for assessment of potential attention-deficit hyperactivity disorder (ADHD) and often add self-reports for adolescents (Allen & Hanchon, 2013; Pelham et al., 2005). Although commonly-used behavior rating scales such as the Conners Rating Scales (Conners, 2008) and the ASEBA (Achenbach & Rescorla, 2001) have strong psychometric properties, the correlations between self-, parent-, and teacher-reports are often modest (Achenbach, et al., 1987; Izzo et al., 2019). It is therefore important for school psychologists to gain an understanding of the potential biases inherent in the reports from these different sources. The focus of this study is the self-perception bias (SPB) of adolescents with ADHD.
Several terms have been used to describe the SPB construct including positive illusory bias and self-enhancement bias (Colomer et al., 2016). Similar to the SPB, all of these terms refer to overestimation of competence or underestimation of symptoms. The SPB has been extensively researched in children with ADHD. The few studies that considered adolescents suggest that the SPB is still evident during this period (Colomer et al. 2016). Nevertheless, there is considerable variability in findings for two reasons. First, the results of previous studies suggest that the indicator of performance might be an important factor. Adolescent self-reports were more predictive of performance on an objective math task than parent ratings (Chan & Martinussen, 2016), whereas parent-reports were more strongly associated with educational attainment, high school GPA, and vocational performance than were self-reports of young adults with ADHD (Barkley et al., 2002). Although, compared to parent ratings, teacher ratings correlated more strongly with grades (GPA) and impairment (Sibley et al., 2014), inter-rater agreement between teachers on ADHD rating scales is low in secondary school (Evans et al., 2005), and those ratings are subject to rater biases such as teacher sex and age (Schultz & Evans, 2012).
Second, the SPB in adolescents with ADHD may vary by domain. They have been found to overestimate their academic, social, and behavioral competence in relation to parent and teacher ratings (Fefer et al., 2018; McQuade et al., 2011). Bourchtein et al. (2017), however, found that only 47% of adolescents with ADHD had a positive bias in at least one of the academic, social, and behavioral domains, with the remaining adolescents rating themselves accurately relative to parent-report and school grades. Longitudinal studies suggest that, in adolescence, the SPB decreases with regard to self-perceptions of behavioral competence and is mainly evident in the social domain (Bourchtein et al., 2017; Hoza et al., 2010).
Children (Wiener et al., 2012) and adolescents (Barkley et al., 2002; Sibley et al., 2012, 2017) with ADHD report fewer ADHD symptoms relative to their parents and/or teachers. Consistent with the ignorance of incompetence hypothesis (which postulates that individuals who have poorly developed skills in a given domain are unable to recognize their incompetence in that domain, Kruger & Dunning, 1999), the SPB in children with ADHD has been found to be most evident in their domains of greatest deficit (Hoza et al., 2002, 2004; Volz-Sidiropoulou et al., 2016). Furthermore, co-occurring depressive symptoms are associated with increased accuracy of self-perceptions in children with ADHD (see Jiang & Johnston, 2014, for review). It is unclear, however, whether these findings also apply to adolescents.
The first objective of this study was to determine whether, compared to adolescents without ADHD, adolescents with ADHD would underestimate their inattention, hyperactivity-impulsivity, oppositional behaviors, learning problems, and social problems relative to parent and teacher ratings. The second objective was to investigate the relation of self-report, parent-report, and teacher-report of learning problems with academic achievement as measured on a standardized individual achievement test among adolescents with ADHD. The third objective was to examine whether adolescents with ADHD with deficits in academic achievement (as assessed on a standardized test), social problems (as reported by parents), and oppositional behaviors (as reported by parents and teachers) would acknowledge that they have more difficulties in these areas than adolescents with ADHD who do not have these deficits. The fourth objective was to explore the role of depressive symptoms in the SPB of adolescents with ADHD.
Methods
Participants
The sample for this study comprised 74 participants, ages 13 to 18, 40 of whom had a diagnosis of ADHD (male: n = 23; female: n = 17) and 34 of whom were typically developing comparison adolescents (male: n = 16; female: n = 18). Participants, who resided in the Greater Toronto Area, were recruited through brochures distributed to physicians and mental health professionals who worked with adolescents with ADHD, websites serving individuals with ADHD, local middle schools and secondary schools, and advertisements placed on websites and in community newspapers.
For inclusion in the ADHD sample, participants were required to have a previous diagnosis of ADHD from a physician or mental health professional. Parents and teachers of the adolescents completed the relevant form of the Conners Rating Scales—Third Edition (Conners, 2008) to confirm that the adolescents with ADHD continued to present significant symptoms. ADHD symptomatology was confirmed if a participant was rated within the clinically significant range (T ≥ 70) by one informant and within the borderline or clinical range (T ≥ 61) by the second informant on at least one of the ADHD core subscales (DSM-IV Inattentive, DSM-IV Hyperactive-Impulsive). For inclusion in the comparison sample, participants were required to have no previous or current diagnosis of ADHD or other behavioral disorder and had non-clinical levels of ADHD symptoms (i.e., received a T-score ≤ 60 on both the DSM ADHD subscales of the Conners 3-P according to parent ratings). Participants who scored below a standard score of 80 on a standardized measure of intelligence, or who were suspected of having an Autism Spectrum Disorder, Bipolar Disorder, or Tourette’s Disorder were not included in the sample.
There were no significant differences between adolescents with and without ADHD in the proportion of males and females, Χ2 (1, N = 74) = .80, p = .370, age, t (72) = 0.41, p = .967 (ADHD: M = 15.48, SD = 1.77; Comparison: M = 15.49, SD = 1.44), level of parent education, t (65) = 1.69, p = .096 (ADHD: M = 8.19, SD = 1.47; Comparison: M = 8.81, SD = 1.49), or the proportion who spoke a language other than English at home (ADHD: 55%; Comparison: 26.5%) X2 (1, N = 67) = 1.15, p = .283. Adolescents with ADHD obtained a lower Full-Scale IQ score on the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999), t (72) = 4.99, p < .001 (ADHD: M = 100.07, SD = 7.18; Comparison M = 109.59, SD = 9.18) and higher scores on all of the DSM-IV ADHD subscales of the parent (Inattentive, t (72) = −20.42, p < .001; Hyperactive-Impulsive, t (72) = −12.32, p < .001) and teacher (Inattentive, t (63) = −9.83, p < .001; Hyperactive-Impulsive, t (63) = −6.79, p < .001) forms of the Conners (see Table 1 for means and standard deviations). Among the 40 adolescents with ADHD, 26 (65%) were taking psychostimulant medication and 70% had at least one (parent-reported) comorbid diagnosis (22 Learning Disabilities, eight Anxiety Disorder, three Oppositional Defiant Disorder, and two Mood Disorder). Among the Comparison adolescents, 2 (5.9%) had a parent-reported learning disability.
Means and Standard Deviations of T-Scores on the Conners-3, CBCL, and YSR, and of Parent-Self and Teacher-Self Discrepancy Scores.
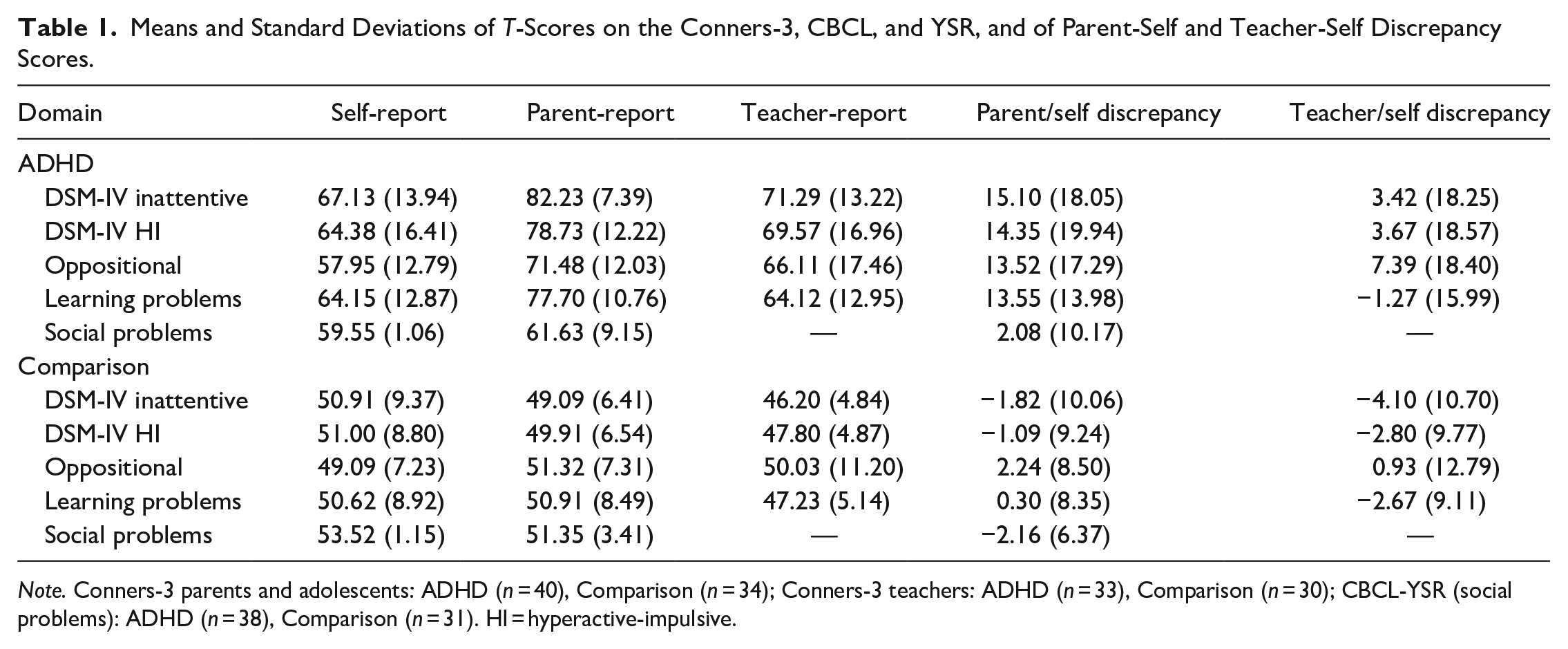
Note. Conners-3 parents and adolescents: ADHD (n = 40), Comparison (n = 34); Conners-3 teachers: ADHD (n = 33), Comparison (n = 30); CBCL-YSR (social problems): ADHD (n = 38), Comparison (n = 31). HI = hyperactive-impulsive.
Measures
Conners Third Edition (Conners-3, Conners, 2008). The Conners-3 is a norm-referenced measure commonly used to screen for ADHD in children and adolescents and to assess symptoms and behaviors that often co-occur with ADHD. Items have a 4-point scale from 0 to 3. Adolescents (CSR-3), parents (CP-3), and teachers (CT-3) of the adolescents completed the Conners. The DSM-IV ADHD, the Oppositional and the Learning Problems scales were used to establish the presence of a SPB. The internal consistency in our sample of the scales used in this study was high (Cronbach alphas of the DSM-IV ADHD scales range from .92 to .95 for parent and teacher report and .85 to .89 for self-report; Cronbach alphas of the Oppositional and Learning Problems scales range from .84 to .93 for parent and teacher report and .76 to .80 for self-report). Test–retest reliability of all of the scales on the Conners-3 is adequate (Conners, 2008).
Child Behavior Checklist (CBCL) and Youth Self-Report (YSR) Forms (Achenbach & Rescorla, 2001). The CBCL and YSR are well-established measures that assess the frequency and intensity of behavioral and emotional problems exhibited by children and adolescents. On the 113-item CBCL and 112-item YSR, parents and adolescents, respectively rate the occurrence of behaviors at the present time or within the past 6 months using a scale from 0 to 2. Both parent and adolescent forms demonstrate adequate to high internal consistency for the subscales (i.e., CBCL: .72–.94; YSR: .67–.95) and adequate to high test–retest reliability (i.e., CBCL: .82–.94; YSR: .67–.89). The Social Problems and Anxiety/Depression scales were used in the analyses for this study. The Cronbach’s alphas in our sample were .84 for CBCL Social Problems, .86 for CBCL Anxiety/Depression, .70 for YSR Social Problems, and .78 for YSR Anxiety/Depression.
Woodcock-Johnson Test of Achievement-Third Edition (WJ-III ACH; Woodcock et al., 2001). The WJ-III ACH is a comprehensive standardized measure of academic achievement, with high internal consistency (.88) and test–retest reliability (.89). The core Reading, Writing, and Mathematics subtests (Letter-Word Identification, Passage Comprehension, Spelling, Writing Samples, Calculation, and Applied Problems) were administered.
Procedures
This study was approved by the University of Toronto Research Ethics Board. Individual testing sessions with adolescents were conducted by graduate students in school and clinical child psychology. Prior to the testing sessions, parents of adolescents provided demographic and medical information about their child and completed the CP-3. Each testing session began by obtaining consent and/or assent. Sessions occurred in a private room. Adolescents were medication-free on the day of study participation. The CT-3 was mailed to teachers, and the CBCL was mailed to parents, who completed them and returned them by mail.
Data Analyses
Parent/adolescent and teacher/adolescent discrepancy scores were computed by subtracting adolescent self-report T-scores from parent/teacher T-scores on the Conners-3 and the Achenbach (CBCL/YSR) subscales. A higher subscale discrepancy score is indicative of a higher SPB. Multivariate (MANOVA) and univariate analyses of variance (ANOVA) were conducted to examine the presence of a SPB and to compare absolute self-perceptions. Adolescents with and without deficits in the different domains were compared using t-tests of independence. Pearson correlations were computed to examine the relationships between the variables.
Results
SPB for ADHD Symptoms, Learning Problems, Oppositional Behaviors, and Social Problems
The MANOVA conducted with the parent/adolescent discrepancy scores on the Conners-3 subscales was significant, Wilks’s λ = .71, F4,69 = 6.97, p < .001, η2 p = .288. Compared to adolescents without ADHD, adolescents with ADHD underestimated their difficulties on the DSM-IV Inattentive (F1,72 = 23.62; p < .001; η2 p = .247), DSM-IV Hyperactive-Impulsive (F1,72 = 17.21; p < .001; η2 p = .193), Oppositional (F1,72 = 12.01; p = .001; η2 p = .143), and Learning Problems (F1,72 = 23.44; p < .001; η2 p = .246) scales; they also underestimated their social difficulties on the Social Problems scale of the YSR (F1,67 = 4.07; p = .048; η2 p = .057) compared to parent ratings on the CBCL. The MANOVA conducted with the teacher/adolescent discrepancy scores on the Conners-3 was not significant Wilks’s λ = .92, F4,58 = 1.28, p = .289, η2 p = .081. Means and standard deviations of the discrepancy scores are shown in Table 1.
Adolescent, Parent, and Teacher Estimations of Academic Achievement
As shown in Table 2, in the sample of adolescents with ADHD, the correlations between Total Achievement on the WJ-III and self-report and parent-report of learning difficulties on the Learning Problems subscale of the Conners-3 were negative and significant. Self-report was negatively correlated with all of the subscales of the WJ-III with the exception of Letter-Word Identification, parent-report was negatively correlated with the reading and mathematics subtests, and teacher-report was negatively correlated with reading comprehension and spelling.
Pearson Correlations Between Academic Achievement on the WJ-III and Self-Report, Parent-Report, and Teacher-Report of Learning Problems on the Conners-3 in Adolescents With ADHD.
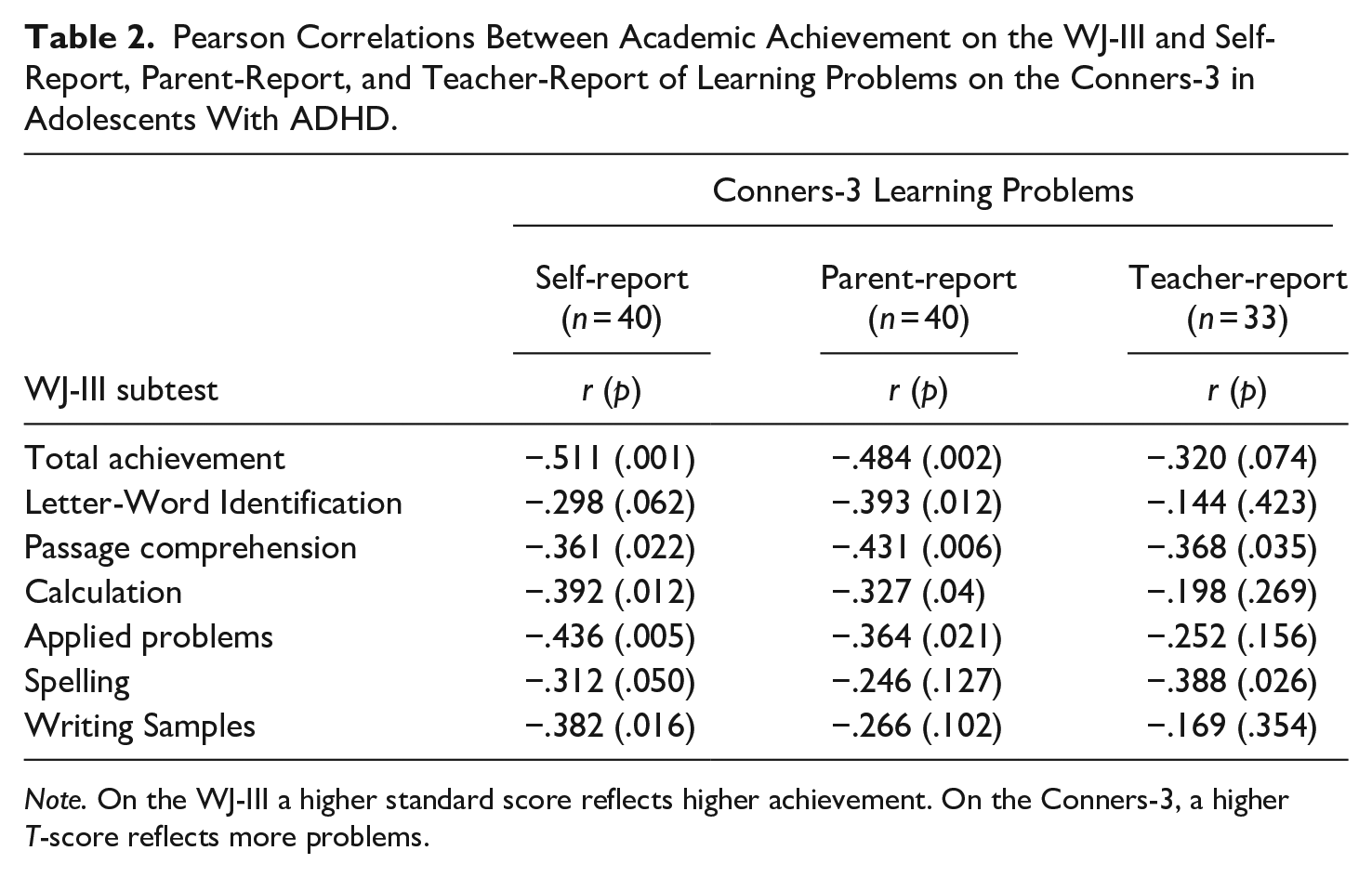
Note. On the WJ-III a higher standard score reflects higher achievement. On the Conners-3, a higher T-score reflects more problems.
Awareness of Specific Deficits
The MANOVA comparing absolute self-report ratings of adolescents with and without ADHD was significant, Wilks’s λ = .64, F5,68 = 7.56, p < .001, η2 p = .358. Adolescents with ADHD perceived themselves as having more problems on the CSR-3 DSM-IV Inattentive (F1,72 = 33.19; p < .001; η2 p = .316), DSM-IV Hyperactive-Impulsive (F1,72 = 18.14; p < .001; η2 p = .201), Oppositional (F1,72 = 12.82; p = .001; η2 p = .151), and Learning Problems (F1,72 = 26.67; p < .001; η2 p = .270) scales than adolescents without ADHD. They also reported that they had more social problems on the YSR than did adolescents without ADHD (F1,72 = 15.17; p < .001; η2 p = .174). Means and standard deviations are shown in Table 1.
As classified on the WJ-III-ACH, low achieving (standard scores < 85 on one or more subtests) adolescents with ADHD (n = 27; M = 67.78, SD = 12.33) obtained significantly higher T-scores on the CSR-3 Learning Problems scale than adolescents with ADHD who were average achievers (standard scores ≥ 85 on all of the subtests, n = 13, M = 56.62, SD = 10.82), t (38) = −2.78, p = .008, d = 0.96. Similarly, as classified on the CBCL, adolescents with scores in the Clinical range (T ≥ 70) on the Social Problems subscale (n = 11; M = 64.55, SD = 5.79) had higher self-report T-scores on the YSR Social Problems subscale than adolescents whose scores on the CBCL Social Problems subscale were in the average range (T ≤ 60; n = 16; M = 58.00, SD = 8.65), t (25) = −2.19, p = .038, d = 0.89. The self-reports on the CSR-3 Oppositional scale of adolescents with ADHD who had scores in the Clinical range on the Oppositional scale of the CP-3 (n = 15; M = 58.84, SD = 12.95), however, did not differ from those whose scores were in the average range on the CP-3 (n = 8; M = 53.63, SD = 8.86), t (31) = −1.06, p = .299, d = 0.47. Similarly, on the CSR-3 Oppositional scale, adolescents with ADHD who had scores in the Clinical range on the Oppositional scale of the CT-3 (n = 15; M = 61.67, SD = 16.28) did not differ from those whose scores were in the average range on the CT-3 (n = 16; M = 55.56, SD = 10.53), t (29) = −1.25, p = .222, d = 0.45. Only 15% (6/40) of adolescents with ADHD reported clinical levels of oppositional behaviors compared to 37.5% (15/40) of their teachers and 62.5% (25/40) of their parents.
SPB and Depressive Symptoms in Adolescents With ADHD
Self-reported depressive symptoms were negatively correlated with the SPB defined as the discrepancy between parent- and self-report of inattention (r (40) = −.327, p = .039), the discrepancy between parent- and self-report of hyperactivity/impulsivity (r (40) = −.376, p = .017), and the discrepancy between self- and teacher-report of inattention (r (34) = −.404, p = .016). Self-reported depressive symptoms were not significantly correlated with the SPB when it was defined as the discrepancy between teacher- and self-report of hyperactivity/impulsivity (r (35) = −.244, p = −139). Parent-reported adolescent depressive symptoms were significantly correlated with the SPB when it was defined as the discrepancy between self-report and teacher-report of inattention (r (34) = −.404, p = .016), and the discrepancy between self-report and teacher-report of hyperactivity/impulsivity (r (34) = −.356, p = .039). Parent-reported adolescent depressive symptoms were not significantly correlated with the SPB when it was defined as the discrepancy between self-report and parent-report of inattention (r (38) = −.285, p = .083) and self-report and parent-report of hyperactivity/impulsivity (r (38) = −.200, p = .228).
Discussion
Although adolescents with ADHD had a SPB when discrepancies were calculated between self-reports and parent-reports of ADHD symptoms, learning problems, oppositional behaviors, and social problems, they did not consistently underestimate the extent of their difficulties. First, the SPB was not evident in relation to teacher-reports. Second, the correlation between their self-appraisals of learning problems and their total score on an individual standardized achievement test was high (r = −.51). Third, they reported higher levels of ADHD symptoms, oppositional behaviors, learning problems, and social problems than did adolescents without ADHD. Fourth, adolescents with ADHD who were low achievers or who had parent-reported social problems were typically aware of their difficulties. On the other hand, adolescents with ADHD whose parents or teachers reported that they had clinical levels of oppositional behaviors typically did not acknowledge their difficulties in this domain. Fifth, among adolescents with ADHD, adolescent depressive symptoms were associated with a lower SPB. There are several factors that might contribute to these inconsistencies, some of which pertain to adolescent characteristics, others to parent and teacher characteristics, and others to methodological issues in the measurement of the SPB.
Adolescent Characteristics
The data on adolescents with ADHD in the current study and in studies by Chan and Martinussen (2016) and Hoza et al. (2010) suggests that, consistent with Harter’s (2012) developmental theory, individuals with ADHD become more accurate during adolescence. Bourchtein et al. (2017) found that despite having a positive bias in the social domain, adolescents with ADHD recognized their problematic social functioning. It is possible that in adolescence, teens with ADHD become more capable of the self-reflection required for accurate appraisals of competencies and difficulties.
Adolescents with ADHD perceived themselves as having more difficulties in all of the domains measured than typically developing adolescents and their perceptions of their difficulties in the academic and social domains were similar to those of parents, teachers, and results of standardized achievement tests. However, although over one-third of teachers and almost two-thirds of parents reported that the teens with ADHD had clinical levels of oppositional behaviors, only 15% of these adolescents indicated that their oppositional behaviors were in the Clinical range. Taken together, these results do not support the ignorance of incompetence hypothesis regarding the SPB being more evident in the most impaired domains (Hoza et al., 2004), but, similar to children with ADHD (Jiang & Johnston, 2014), suggest that among adolescents with ADHD, the SPB might be associated with oppositional behaviors. Consequently, in adolescence, the relationship between ADHD and overestimation of competence or underestimation of problems may decrease, while the relationship between oppositional behaviors and overestimations of competence or underestimations of problems may remain stable. This might occur because the combination of ADHD and oppositional behaviors is associated with higher levels of social impairment including difficulties with the social-perspective taking that contribute to accurate self-appraisals (see Bora & Pantelis, 2016 for review). It is also possible that contextual factors such as a deviant peer group (Kofler et al., 2015) or inconsistent parenting (see Wiener, 2020, for review) may be risk factors for the higher SPB in adolescents with co-occurring ADHD and oppositional behaviors.
Consistent with findings from several studies with children (see Jiang & Johnston, 2014 for review), in the current study adolescent depressive symptoms as reported by parents and adolescents were associated with a lower SPB for ADHD symptoms in adolescents with ADHD and the correlations remained significant even when the reporter of adolescent depressive symptoms was not one of the reporters of adolescent ADHD symptoms.
Parent and Teacher Characteristics
The discrepancy between parent and adolescent reports might be associated with challenges that the parents experience including their parenting stress (Wiener et al., 2016), their own ADHD symptoms (Wiener et al., 2016), and depression (Biondic et al., 2019; Theule et al., 2013). Moreover, parents spend less time with their children during the adolescent period and for that reason they may be less aware of their behaviors. It is also possible that parents have a negative bias toward their teens’ behaviors due to the influence of previous experience.
Teachers typically come into contact with more adolescents than parents, which may help normalize their perceptions of their students with ADHD. The lower correlation between teacher ratings of learning problems and achievement, however, suggests that teacher ratings may also not be the best indicator of adolescent competence and difficulties. One possible reason is that students in secondary school typically have different teachers for each subject and teachers may teach more than 100 different students in a semester.
Methodological Factors
The limitations of the current study illustrate the methodological confounds in measuring the SPB in much of the previous research (De Los Reyes & Kazdin, 2004; Jiang & Johnston, 2016; Owens et al., 2007) and may affect the interpretation of the results. First, parent and teacher reports were used to classify adolescents as ADHD or typically developing, as an indicator of extent of the teens’ difficulties when measuring the SPB, and as a measure of depressive symptoms. The only area where there was a performance measure of adolescent functioning was academic achievement. As discussed above, the assumption that parent and teacher reports of functioning are objective indices of the teens’ actual symptoms may be fallacious as shown by the findings in the current and other studies (Chan & Martinussen, 2016; Jiang & Johnston, 2016; Swanson et al., 2012;) that children and adolescents with ADHD are relatively accurate appraisers of their performance on standardized achievement tests or laboratory tasks. Second, because the discrepancy scores used to calculate the SPB range between large negative values and large positive values, the comparisons may obscure important individual differences. Third, without data on the characteristics of the teachers, parenting stress, and parent psychopathology, it is not clear whether factors other than the adolescents’ behavior is influencing their reports. It is therefore important in future research to examine whether these parent and teacher factors influence the presence or magnitude of the SPB in adolescents with ADHD.
Relevance to the Practice of School Psychology
The results of the current study have implications for school psychologists who use standardized behavioral rating scales to assess the ADHD symptoms, impairment, and problem behaviors of adolescents. The results suggest that, with the possible exception of self-reports of oppositional and other externalizing behaviors, school psychologists who are diagnosing ADHD should give credence to adolescent self-report using standardized rating scales assessing ADHD.
School psychologist should also be aware that there is considerable variability in the magnitude of the SPB. Although adolescents are typically aware of their ADHD symptoms, learning and social problems, adolescents whose parents and teachers view them as having high levels of oppositional behavior frequently do not acknowledge their difficulties in this area. In contrast, depression may partially explain why some adolescents with ADHD do not have a SPB. Consequently, school psychologists should investigate possible depression when adolescents do not underestimate the extent of their problems compared to parent and teacher ratings. In conclusion, the current study provides additional support to the contention that assessments should be multi-source and multi-method (e.g., Pelham et al., 2005), and that clinical judgment should be used in interpreting the findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Social Sciences and Humanities Research Council of Canada (410-2010-1763). In addition, a mobility grant (E-2016-30) for C.C. was received from Universitat Jaume I.