
Abstract
This article highlights a novel approach to professional development, integrating leadership, development and patient-centred health system transformation in the new Fellowship Program in Health System Improvement offered by the School of Public Health at the University of Alberta. Early assessment of the program is also provided.
Introduction
While Canadians have great pride in their health system, its performance lags behind several other countries. 1 While there has been much discussion and literature over the past 3 decades on how Canada’s system could be improved, transformative change has not matched the rhetoric. In its final report, the Health Council of Canada made the case for increased attention to leadership to channel energy and previous reform efforts toward a “ period of faster, more targeted and more effective health system reform that creates the high quality care Canadians expect and deserve.” 2
Schools of Public Health are expected to play an active role in bringing about positive change in both the healthcare system and health status performance through education and research programs. 3 Accordingly, the University of Alberta’s School of Public Health undertook a planning project for an executive development program in health system leadership. The lead author was asked to lead the planning project in view of his experience at executive leadership levels in government, health authority, and the university; his roles as a founding co-chair of the Canadian Health Leadership Network; his involvement in the development of the LEADS framework; and his academic work on comparative health systems. He was supported by a planning team from the School. The planning project involved consultation with health system leaders and universities already providing executive-level educational programs to identify unmet needs. It resulted in The Fellowship in Health System Improvement being launched in fall 2016 with a cohort of 20 participants.
The Fellowship program combines a focus on leadership development and specific program improvement content related to key drivers for health system transformation. System transformation builds on the definition of transformational change which is “a shift in the business culture of an organization resulting from a change in the underlying strategy and processes that the organization has used in the past. A transformational change is designed to be organization wide and enacted over time” 4
The Fellowship program aligns well with the objectives of the Canadian Institute for Health Research Strategy for Patient Oriented Research, which is built on a premise that transformational change requires harnessing research to foster evidence-based decision-making using strong participatory leadership in the health system. 5 It emphasizes the integration of leadership development and research content to drive change.
Leadership development theory and pedagogy
While there is a rich literature on leadership theory, much less attention has been given to leadership development theory and even less to the effectiveness of different leadership development approaches. In a recent review of leadership development, the King’s Fund makes the case that a culture of continuous improvement is most influenced by leadership practices, but there is little evidence on the effectiveness of leadership development programs. 6
The underlying philosophy for the new Fellowship program is that focusing on leadership development must be tied directly to desired heath system transformative change. In developing the Fellowship program, consideration was given to emerging trends in executive education. McNay notes that executive education must take people well beyond their internal management responsibilities and place a greater focus on the external environment. It must provide a leadership development experience that prepares people to deal with an uncertain future. This requires knowledge of the various parts of a business, understanding the interaction among the parts, and the capability to sense new trends, relationships, and opportunities. Programs that focus on action learning have shown promise. 7 This same point was made in an article in the Economist arguing that executive education has to do more than inform—it has to change the way things are done. Executive education that places emphasis on the use of action learning to energize debate within a group is a growing trend to accomplish this. 8
The King’s Fund report noted above lends support to an approach that incorporates a broad system view, a variety of teaching methods, action learning, and a heavy emphasis on working in teams across disciplines and organizational settings. There are three design features of the Fellowship that distinguish the program from others: program perspective, drivers for health system performance, and critical processes to guide the program. a. Program perspective—Four overriding perspectives guide the program: a system-level focus that goes beyond efficiency and effectiveness to include how the health system contributes to the health status of the population; an emphasis on leadership in action through projects undertaken by participants using a person-centred approach; international comparisons of health system and health status performance to identify opportunities for Canada; and the integration of the most recent research on topics through the involvement of leading research experts. b. Drivers for health system performance—The program focuses on four drivers for health system improvement: the political environment and how to effectively align political and administrative imperatives to achieve health system change; using leadership through the LEADS framework
5
to drive health innovation and transformation; how to optimize health human resources in transformative change; and developing a culture of quality.
Each one of these drivers forms the basis of a weekend session theme along with an introductory “big picture” theme that traces the evolution and underlying values of the Canadian system, the importance of social determinants of health in transformative change, and the performance of the Canadian system relative to other countries (Figure 1). The final weekend session theme is on health system transformation where each group presents its action learning project.
c. Critical processes—Three processes are fundamental to the operation of the program: development of the Change Agenda—A document developed annually in consultation with those jurisdictions from where the participants are from. It identifies top priorities in each of those jurisdictions and summarizes them into common themes to guide speakers and assignments. In the past 2 years, moving to a person-centred system has been a dominant theme, so this has shaped assignments and discussions in the program; interaction with health system leaders throughout the program; and the use of experienced health system leaders who serve as mentors in the program.
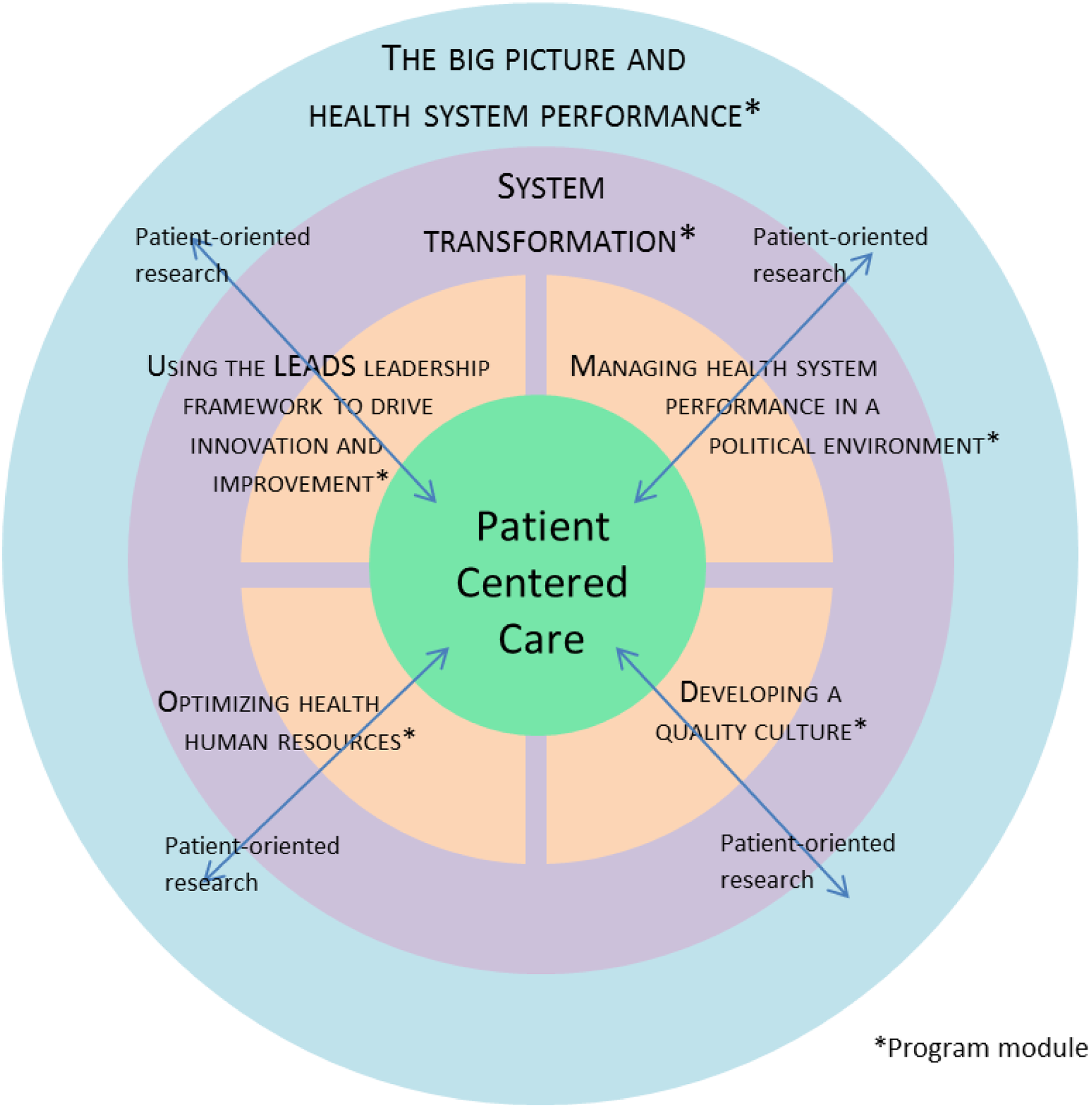
Conceptual framework for the fellowship program.
The Fellowship program integrates several different approaches to learning over a span of 9 months with 6 intensive weekends that alternate between Banff and Edmonton. The sessions involve interaction with leading researchers, persons who have held significant leadership roles, and current leaders in the Canadian system and from other countries. The list of speakers used in the program for 2016-2017 is included in on-line appendix A.
Both plenary sessions and discussion sessions are used. Participants are placed in four groups to ensure a diversity of provincial experiences, professional disciplines, and roles in the health system. Each group is guided by a mentor who has had significant leadership experience in the health system and academic mentors with strong methodological expertise in health systems and health policy research. Mentors collectively bring experience in roles as deputy minister, chief executive officer, assistant deputy minister, health agency vice-president, professor, and research leader.
The International Ideas Marketplace is a key component of the weekend sessions and has been included to stretch the thinking of participants beyond what is currently happening in Canada. On a rotational basis, each group reviews current literature on the module theme from one of the reference countries—Australia, the Netherlands, New Zealand, Sweden and the United Kingdom—to identify ideas and strategies that should be considered in Canada. Of those countries, only Australia has a federated political system like Canada. However, the evolution in the two countries has taken different trajectories since the formation of the federations. 9
A Leadership Health System Transformation Prospectus is created by each group as a culminating step for each weekend session to integrate learnings from readings, speakers, and group discussions. The intent of this prospectus is to advance a strategy to improve performance of the Canadian system by identifying critical implementation steps and the leadership imperatives to make this happen.
An integral part of the program is the LEADS reflection, which is done on an individual basis with the mentor. The process starts with the LEADS self-assessment 10 that identifies each person’s leadership strengths and developmental needs. Following each weekend, a conversation takes place with the mentor on how the participant is using knowledge and skills gained in the program to apply new approaches in their leadership within their current work setting.
Prior to each weekend session, a list of required readings is made available. Given the busy schedules of program participants, most of the assignments are designed to be completed during the weekend session. The exception is the major Action Learning Project carried out by each group over the duration of the program.
The Action Learning Project provides an opportunity for each group of participants who have diverse backgrounds and career experience to undertake a transformative project linked to the Change Agenda. The project is undertaken over a span of 8-9 months and must have at least one sponsor organization that appoints an executive leader to guide the project and commits to having the project presented to its senior leaders in that organization. It is intended to develop strategies including leadership requirements and initial steps toward an implementation plan that will provide a transformative approach to a real-world issue. These projects must take a big system view and involve at least two sectors that impact health status/outcomes, including sectors outside the conventional health system that will integrate learnings from the program. The four ALPs in 2016-2017 and the sponsoring organizations were: embedding a palliative approach into Alberta’s Primary Healthcare (Alberta Health Services); strengths and supports for mothers to have a conversation with community (to reduce infant mortality in Indigenous populations; Interior Health Authority, BC); integrating primary and social care (Alberta Health); and suicide prevention for First Nation Youth in rural and remote Northern Saskatchewan communities (Ministry of Health in Saskatchewan and Health Quality Council in Saskatchewan).
All of these projects (on-line appendix B) were transformative in that they put forward approaches that were major departures from the current practices and took a broad health system approach noting changes that should be made in several parts of the existing system. In all cases, the sponsor organizations have responded positively to the recommendations contained in the final reports and provided indications of intent to incorporate many of the ideas into follow-up strategies. On-line appendix B provides an overview of the four projects in the past year. For the coming year, each of the four ALPs incorporates a person-centred approach, with one specifically looking at patient engagement in the development of performance measures.
All resources and communication for the program are made available using the learning system at the University of Alberta, known as eClass, and each participant is encouraged to develop a portfolio of their work using Mahara software, a support learning system that allows individuals to record all their work and allows for the sharing of information among participants.
Through a strategic alliance with the Canadian College of Health Leaders, participants who complete the program and become Fellows can pursue an accelerated track to achieve their Certified Health Executive (CHE) designation. For persons already holding the CHE designation, the strategic alliance provides an opportunity to use the ALP project as a platform to achieve the Fellow of Canadian College of Health Leaders designation.
The first cohort of the Fellowship program consisted of 20 participants who came from Québec, Ontario, Saskatchewan, Alberta, and British Columbia, including some who worked at the national level. The participants had a broad range of backgrounds both in terms of their roles in the system and professional backgrounds. This included physicians, pharmacists, an engineer, epidemiologist, physiotherapists, and nursing leaders. Roles included persons holding senior positions at the operational levels with health authorities, policy roles within government, regulatory agencies, quality councils, and research organizations
Early assessments of the program
Since only one cohort of 20 participants has completed the program, only early results are available. A debrief with the first cohort as a group and follow-up interviews with each participant were documented. They provided important insights, including some areas where the program can be enhanced: There was unanimous support for the structure of the program. The big system perspective and international experience was highly valued. The calibre of speakers was regarded as exceptional and the opportunities to interact with well-known leaders was seen as an exceptional experience. The mentorship model was highly praised as it provided direction but allowed groups to work through issues. The participants identified their expanded understanding of the larger health system, the ability to take ideas back immediately to their respective work settings, and the added sense of self-confidence that the program gave them as enhancing their leadership capabilities.
Several areas where the program could be enhanced have now been incorporated into the program for the second cohort which is now underway. These included having a better integration of leadership development within each module, reducing the reading list, providing more opportunities for participants to tailor some of their assignments more directly to their current work settings, and refining the expectations of the ALP, so that it becomes more oriented as an executive-level action document rather than an academic paper.
Next steps
The experience from the first cohort has demonstrated significant promise for the Fellowship program and fine-tuning is now taking place to improve the program for the second cohort that commenced in fall 2017. Persons completing this program will constitute a community of leaders, and the intent of the School is to keep these people engaged and allow their participation in parts of the program on an ongoing basis. The ultimate test will the extent to which these people can truly exert leadership to improve the performance of the Canadian health system as a patient-centred system.
Footnotes
Supplemental material
Supplementary material for this article is available on-line.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.