
Abstract
This article discusses the emerging role of Artificial Intelligence (AI) in the learning and professional development of healthcare professionals. It provides a brief history of AI, current and past applications in healthcare education and training, and discusses why and how health leaders can revolutionize education system practices using AI in healthcare education. It also discusses potential implications of AI on human educators like clinical educators and provides recommendations for health leaders to support the application of AI in the learning and professional development of healthcare professionals.
Introduction
To build a safer healthcare system, key prerequisites include having “the right equipment, well-maintained and reliable; a skilled and knowledgeable workforce; reasonable work schedules; well-designed jobs; clear guidance on desired and undesired performance; and so on.” 1 Education and training are central to preparing a skilled and knowledgeable workforce. Training refers to learning that is provided to improve performance on the present job, whereas education provides learning to improve performance on a future job. 2 The extent and adequacy of education and training provided to healthcare professionals affects patient safety. Therefore, the education and training of healthcare professionals must be aligned with current and emerging best practices in both learning and healthcare. Thus, Artificial Intelligence (AI) is a particularly critical and hot topic of interest for health leaders.
Although AI has been around for over 5 decades, it is a rapidly emerging area that is actively being integrated in all industries, including healthcare. Canada is quickly becoming a global leader in AI, with 3 AI hubs growing in Montreal, Edmonton, and the Toronto region. While University of Alberta ranks #2 in the worldwide university rankings for AI/machine learning combined, Montreal has the highest concentration of deep learning and researchers in the world, as well as one of the world’s largest deep learning laboratories. 3 Moreover, the Toronto region has the highest number of AI start-ups in the world and has committed over $80 million of funding from companies such as Google and Thomas Reuters to support Toronto’s Vector Institute, an AI research centre. 3 As such, Canada is well-poised to realize the immense potential and promise of AI.
Forbes has predicted that AI for healthcare application will cross $1.7 billion by the end of 2019. 4 Additionally, AI is purported to have significant advantages in supporting learning and student engagement, especially in the workplace setting. The use of AI in the education industry is expected to increase by 47.5% through 2021. 5 At the same time, there is a fear that AI may replace human educators in the coming decade, which could have an impact on roles such as the Clinical Nurse Educator (CNE), medical resident preceptors, and other interprofessional educators. However, AI also has the potential to innovatively support these clinical educator roles, which are currently facing growing workload demands in an increasingly low-resourced, demanding, and complex healthcare environment. In fact, the shortage of frontline healthcare professionals is even forcing clinical educators to fill in the staffing shortage gaps. At present, many clinical educators are being pulled to the bedside to provide direct patient care instead of devoting their time to teach their clinical colleagues the skills and knowledge needed to continuously provide the best possible care to patients. For this reason, it is crucial for health leaders to have an understanding of why and how AI can support educators in the learning and professional development of healthcare professionals in both the post-secondary education and workplace learning domains. As such, this article aligns with the LEADS framework capability of “orient themselves strategically to the future,” in which health leaders “scan the environment for ideas, best practices, and emerging trends that will shape the system.” 6
This article discusses the emerging role of AI in the learning and professional development of healthcare professionals. It provides a brief history of AI and its current and past applications in healthcare education and discusses how AI can be used in healthcare education to better prepare current and future healthcare professionals to provide safe and quality patient care.
Background
While there are many definitions of AI, Marvin Minky defines it as “the science of making machines do things that would require intelligence if done by men.” 7 According to the leading textbook on AI, 8 the definition of AI fits into the following 4 approaches: (1) thinking like a human (eg, decision-making and problem-solving), (2) acting like a human (eg, image and voice recognition), (3) thinking rationally (eg, computational models of perception and reasoning), and (4) acting rationally (eg, artifacts with intelligent behaviours). 8 In everyday life, AI is used in e-mail spam filtering, personal assistants like Siri, Netflix, Google Home, and learning apps like Duolingo. 9 It is important to note that when cutting-edge AI becomes “mainstream” (ie, filtered into general applications), it is often not called AI “because once something becomes useful enough and common enough it is not labeled AI anymore.” 10 Recent computational approaches in AI that are widely used in numerous applications include algorithms, machine learning, and neural networks.
Algorithms are at the centre of AI. In fact, it can be said that the history of AI is the history of increasingly efficient/elegant algorithms. 9 A notable example is Google PageRank, which ranks the importance of a web site. As a subfield of AI, machine learning refers to “getting computers to act without being given every step in advance.” 9 As such, algorithms “learn what to do.” It includes supervised learning, unsupervised learning, and reinforcement learning. Examples of machine learning include self-driving cars and natural language processing. Artificial neural networks are AI algorithms that are “based on the structure and functions of biological neural networks (ie, animal brains) that might be applied in advanced supervised, unsupervised, or reinforcement learning.” 9 For example, artificial neural networks have been trained to identify faces in moving crowds of people.
Brief history of AI in education
Dating back to the 1920s, AI has a rich history in education and is referred to as AI in Education (AIED). Figure 1 illustrates the historical timeline of AIED, demonstrating the iterative improvements in AIED over time. The earliest “teaching machines” supported learning and immediate feedback, serving as a personal tutor for students. 9 However, these machines were not adaptive (ie, they did not adapt to individual student needs). In the 1950s, teaching machines led to the development of adaptive teaching machines known as Self-Adaptive Keyboard Instructor (SAKI), which adapted to the learner’s performance and presented tasks accordingly. 9 Several iterations of SAKI led to the development of Computer-Aided Instruction (CAI) systems in the 1960s and 1970s. Computer-aided instruction marked the introduction of educational technology tools, such as user forums, e-mail, remote screen-sharing, and multiplayer games. 9 However, due to issues of cost and poor accessibility, CAI systems were not widely adopted. 9 In 1970, AI was first implemented into CAI in a PhD thesis; this became known as Intelligent Tutoring Systems (ITSs). 9 This marked a significant milestone in the history of AIED.
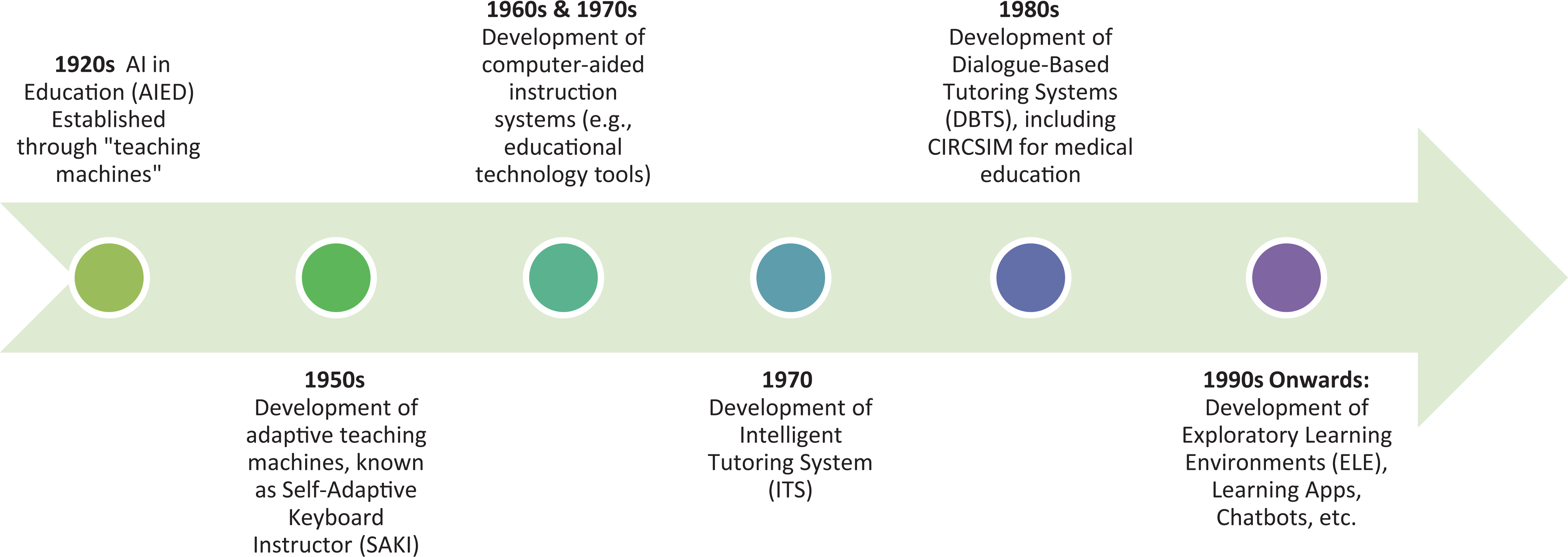
Timeline of AI in education.
Intelligent tutoring systems are the most common application of AIED; they are “adaptive, instructional systems that attempt to emulate the well-known benefits of one-on-one human tutoring.” 11 As such, ITSs support “learning by doing” through guidance and explanations, as well as pointing out errors and adapting curriculum to meet individual learner needs. 11 Dialogue-Based Tutoring Systems (DBTSs) are a version of ITS. Interestingly, one of the earliest DBTSs was developed in the 1980s for medical education; the DBTS was called CIRCSIM, which used one-to-one tutorial dialogues to help first-year medical students learn about cardiovascular physiology dealing with the regulation of blood pressure. 9,12 As a tool designed to strengthen medical students’ problem-solving, CIRCSIM required learners to “explore in depth, better understand, and consolidate what they had already learned.” 9
In more recent history of AIED, Exploratory Learning Environments (ELEs) were introduced. In contrast to the step-by-step approach of ITS and DBTS, ELEs encourage learners “to actively construct their own knowledge by exploring and manipulating elements of the learning environment.” 9 Other modern developments of AIED include language learning apps, chatbots, learning network orchestrators, collaborative learning, student forum monitoring, and continuous assessment. 9 Additionally, automatic writing evaluation is an AIED support that provides automatic feedback (formative or summative) on student writing submitted to the system. 9
Benefits of AI in education
In various industries, there have been numerous benefits reported for AIED, especially in the use of ITS. However, there is a dearth of literature on the quantifiable cost savings or learner effectiveness (eg, satisfaction, learning, change in behaviour, etc) of using AIED as an educational intervention. This reflects a larger gap in research on the effectiveness of technology-based educational interventions, overall. While AIED requires further examination using rigorous learning evaluation methodology, the key benefits of AIED are discussed subsequently.
Essentially, the goal of an ITS is “to emulate the benefits that a well-trained human tutor provides to students, by interpreting student answers and appropriately responding in order to encourage elaboration.” 13 In statistical quality control, an ITS known as STCEQ has been found to provide a friendly learning environment embedded with real problems and a virtual subject matter expert and tutor 14 ; the tool provides learners full control of interaction, allowing them to choose or ignore tutor recommendations, as well as review previous interactions (eg, performance, tutorials consulted). 14 Cognitive tutors (ie, interactive learning environments) are another AIED tool that have been researched at Carnegie Mellon University and were found to increase learner interactivity by providing a problem-solving environment, tutorial guidance (through yes-no feedback in a step-by-step manner, specific feedback for commonly occurring errors, and next-step hints), and adaptive problem selection based on the learner’s performance in solving problems with the tutor. 15
In the field of linguistics, ITS has been leveraged to develop “virtual” humans who engaged in dialogue with learners to help them learn new languages 16 ; these virtual humans have been used to train tens of thousands of people in the military, government, business, education, and non-governmental organizations. 16 The virtual humans help provide learners with extensive conversational practice in learning a new language and continually monitor the learner’s application of communication skills to assess their mastery of the language. 16
The “politeness” of ITS tools is another area that offers benefit in AIED. In the high school setting, a “polite” ITS (ie, an ITS that provided polite feedback and hints to learners) was implemented; the polite characteristics of the ITS were found to benefit more “needy” students (ie, those who made the most errors). 17 This highlights the critical importance of an ITS’ “soft” skills.
In the healthcare setting, an ITS known as BRCA Gist has been found to be suitable and beneficial for deep learning about genetic breast cancer risk. 13 Compared to simply being given information, learning is more effective and deeper when learners talk to an ITS that facilitates communication with facial expressions, simulated facial movements (ie, animation or video with sound), voice inflection, and conversational phrasing. 13 This depth of learning is the result of learners being required to express causal and functional relationships instead of just mechanically applying procedures. 13 Another study found that applying emotion regulation strategies in ITS may produce more optimistic emotions in learners and better learning gain resulting from increased cognitive flexibility that allows the learner to discover new ideas and possibilities. 18 Further, ITSs provide a greater range of medical cases and are not bound by place and time; instead they provide learners immediate feedback that can simulate a normal apprenticeship experience. 19 As such, the ITS dynamically supports case selection that adapts to learner mastery, focusing learning time on cases that have the highest learning value for individual learners. 19 As a form of “performance trainers,” these ITSs or cognitive tutoring systems have consistently been found to achieve higher performance than learning in a traditional classroom alone. 19
Clearly, AIED holds significant promise across industries, which require additional research to measure the full extent of benefits realization for organizations. While AIED has myriad applications and significant potential for supporting the novel education and training of healthcare professionals, its current adoption has been limited and varied, as discussed in the subsequent section.
Current role of AI in healthcare professionals’ education
Despite the rich and early history of AIED in medical education, its application in the education of healthcare professionals in Canada has generally been limited; most studies examine the use of ITS in medical education in the United States. Some exemplary healthcare applications of AIED are outlined in Table 1. In general, there is a paucity of literature on the use of AIED in nursing and allied health education, especially interprofessional education and the continuing professional development of healthcare professionals.
AIED applications in healthcare education
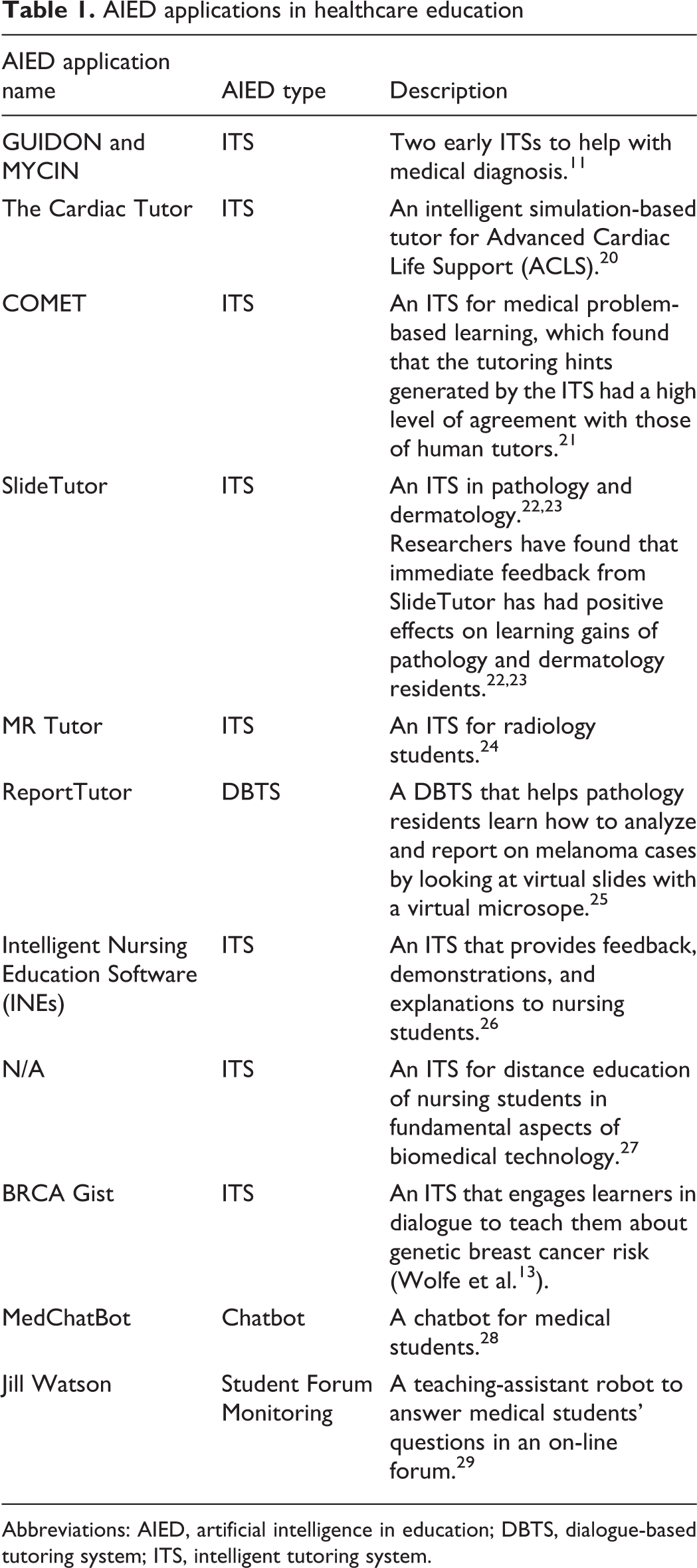
Abbreviations: AIED, artificial intelligence in education; DBTS, dialogue-based tutoring system; ITS, intelligent tutoring system.
While there is some evidence of the use of AIED applications in healthcare learning, the topic of AI and its applications have rarely been introduced to date into healthcare professionals’ education. Surprisingly, this is especially the case in medicine where AI is making rapid advancements. According to Dr. Vijaya B. Kolachalama, assistant professor of medicine at Boston University School of Medicine, “Technology without physician knowledge of its potential and applications does not make sense and will only further perpetuate healthcare costs.” 30 As such, there is a need to move all healthcare professionals from the information age to “the age of AI.” 31 This can be facilitated through applications of AIED in the post-secondary and workplace settings for healthcare education, which holds significant potential to improve learning effectiveness (eg, more individualized, deeper, and lifelong learning) and job satisfaction for educators (eg, reduction in education workloads, more positive attitudes toward a workplace that is committed to supporting ongoing and personalized learning, etc), thereby further enabling conditions for better patient care and safety. Further, to effectively “kill two birds with one stone,” there is currently a unique opportunity to apply AIED in the introduction of AI as a topic into the healthcare education of students and professionals. The next section describes how health leaders can apply current trends in AIED for this purpose.
Recommendations for health leaders
Healthcare organizations have the potential to revolutionize education system practices and platforms using AIED in healthcare to improve learning effectiveness, reduce costs and clinical educator workloads, and enhance employee job satisfaction. To best support the learning of professionals based on current and future trends in AIED, we recommend the following strategies for health leaders to apply in their organizations:
Assess and increase organizational awareness and knowledge of AI and AIED through formal and informal education (eg, webinars, lunch and learns, articles, social media) of healthcare professionals. These initiatives should focus on the benefits of AI and AIED (eg, increased learning effectiveness, reduced clinical educator workloads, potential for cost savings). Earlier this year, we introduced the topic of AI to our departmental team members as a part of Forbes’ Top 8 Health Care Predictions for 2019. 4 Through a group discussion and follow-up survey, our team members had the opportunity to reflect on the predictions and suggest ideas and opportunities for applying them to our Learning and Performance Support Department. This exercise motivated several team members to learn more about AI and its implications for healthcare and our work, which furthered our capability of “orienting [ourselves] strategically to the future.” 6 Further, the exercise inspired us to (1) do more research on AIED as a part of our departmental goal to “Advance Learning [Best Practices],” (2) purchase books on AIED for our departmental library to enhance our collective understanding of AIED as a team, and (3) prepare this publication to spread awareness of the current and future potential of AIED in healthcare. Throughout this process, we were surprised to learn that AI is not necessarily a brand new buzzword in healthcare; instead, AIED has very humble roots in healthcare education, which demands celebration and increased awareness. Understanding the successful history of AIED applications is a significant facilitator for increasing its application and adoption in today’s complex and fast-changing healthcare learning environment.
Assess the current state of AIED in your organization. Learning/education teams should evaluate the effectiveness of current learning technologies used in their organizations. This will help to determine the potential for piloting AIED applications, as well as serve as an opportunity to do a rapid SWOT (Strengths, Weaknesses, Opportunities, Threats) analysis of your organization’s learning infrastructure. In this assessment, you may consider if there are (1) any current learning technologies in your organization that include AI, (b) learners in your organization who have used AIED in their prior training (eg, medical or nursing school) or learning outside of the workplace, and (c) any learning technologies that learners prefer to use which are not currently supported by your organization.
Pilot AIED applications (eg, ITS, DBTS, chatbots, collaborative learning) across medical, nursing, and allied health specialties. In addition to enhancing learning outcomes in a cost-effective way, AIED applications may be effective in supporting the role of human educators, such as CNEs, preceptors, and peer mentors. It should be noted that AI is not anticipated to replace human educators; instead, the role of human educators will continue to evolve and eventually be transformed to effectively and efficiently use their time and expertise. 9 For this reason, there is a critical need to explore how AIED can be leveraged to support the workload of clinical educators to ensure their time and energy can be better allocated to reaching more learners in more meaningful ways (ie, using technology to supplement and support the capacity of human educators).
Collaborate with other healthcare organizations, AIED designers, and post-secondary institutions to design, develop, and evaluate AIED applications that meet the learning needs of the healthcare workforce. For example, Google offers a free chatbot creator called DialogFlow, which laypeople can use to develop chatbots. 32 Quick reference guides, frequently asked questions, workplace coaching, and mentoring may be a potential area to explore using chatbots. Essentially, cross-sector partnership is pivotal to developing, adopting, and optimally using AIED applications that enhance learning outcomes, improve learners’ and educators’ job satisfaction, reduce costs, and ultimately improve the quality and safety of patient care.
Monitor AIED trends to ensure that healthcare organizations are applying the best learning practices to support healthcare professionals’ education. As leaders, keeping our eyes and ears open for learning trends just beyond the horizon is key to preparing, recruiting, and retaining the healthcare workforce of today and tomorrow.
Conclusion
Although AI has had a long history in education, its adoption is generally limited in the education of healthcare professionals in Canada. At the same time, there is a need to move healthcare professionals from the information age to the age of AI. To strategically orient themselves and their organizations to the future, health leaders should (1) assess and increase organizational awareness and knowledge of AI and AIED; (2) assess the current state of learning technology and AIED in their organizations; (3) pilot AIED applications across medical, nursing, and allied health specialties; (4) collaborate with other healthcare organizations, AIED designers, and post-secondary institutions to design, develop, and evaluate AIED applications and their benefits realizations (eg, learning effectiveness, cost savings); and (5) monitor AIED trends. All in all, AIED holds significant promise for improving learning effectiveness, employee job satisfaction, and healthcare costs. For health leaders, the time is now “to AIED healthcare learning” today and tomorrow.
Footnotes
Acknowledgment
The authors wish to thank Ken McFarlan, Manager/Librarian at Island Health, for his much appreciated support with conducting the literature review for this article.