
Abstract
Medication Reconciliation (MedRec) is a proven method of optimizing pharmacotherapy and decreasing incidence of Adverse Drug Events (ADEs); however, consistent and correct execution is often a challenge in the setting of outpatient oncology. Ambulatory chemotherapy patients are particularly susceptible to polypharmacy and ADEs and their medication management is often complicated due to gaps in communication between an increased volume of non-co-located, multidisciplinary, healthcare providers. Acknowledging these challenges, Winchester District Memorial Hospital (WDMH) led an initiative to create an ambulatory chemotherapy MedRec process using behavioural change approaches. Prior to the intervention, ambulatory chemotherapy MedRec at WDMH was conducted informally via an “open-loop” process. Through an iterative quality improvement process which involved understanding and communicating failure points in the transmission of patients’ medication information directly with the frontline medical staff, a practical and sustainable “closed-loop” system evolved, which improved rates to 97.8% overall completion post-intervention.
Why is medication reconciliation important?
Medication Reconciliation (MedRec) is the formal process in which medical records are compiled, transferred, and kept consistent throughout a patient’s journey of care. Chemotherapy patients are prescribed numerous medications, ranging from those for pre-existing conditions, for the direct treatment of their cancer diagnosis, for management of side effects, and post-chemotherapy medication orders. Chemotherapy can also be very dynamic, having to be tailored to patient-specific factors. The best practice would be to have every chemotherapy patient’s medications reconciled successfully, identifying and correcting any concerns or discrepancies and acted upon.
Absent or inaccurate MedRec can pose a risk for oncology patients leading to Adverse Drug Events (ADEs) and Drug Interactions (DIs). Moreover, several chemotherapeutic agents have narrow therapeutic indices where subtle changes in serum concentration can pose the risk of either subtherapeutic dosing or toxic side effects. 1 Furthermore, since oncology patients tend to be older in age, they are more likely to have a higher baseline pill burden due to pre-existing comorbidities, meaning an increased likelihood of DI/ADEs. In 2009, a study found that among patients older than 65 years, 92% were taking a median of five prescribed medications before the start of any cancer treatment. 2 This underlines MedRec’s importance, particularly with this sensitive population.
Rurally unique challenges with MedRec
Medication Reconciliation implementation can be problematic based on setting. Rural hospitals face challenges due to the limited resources available to them. For instance, when consulting urban counterparts, their large volume of patients allows them to have a dedicated pharmacy technician team for MedRec plus software for seamless reconciliation and communication. Most rural hospitals don’t have the volume to justify the projected costs.
Leadership call to action
Leadership throughout Canada has highlighted the need for better systems of MedRec and the need to understand its implementation. A major player in this sector is a collaboration between health leaders, Canadian Patient Safety Institute, Canadian Institute for Health Information, Institute for Safe Medication Practices (ISMP), and Accreditation Canada. 3 In their most recent reports (from 2012), they released communications investigating MedRec in Canada. 3,4 In these reports, in consultation with leaders across the country, MedRec was identified as one of the top three patient safety priorities in every jurisdiction. 3,4 While they acknowledge that the accomplishments to date are significant, they also recognize that the system of MedRec is far from perfect in many organizations and there remains a particularly strong need for rurally focused leaders and research. This positions rural Canadian health organizations such as Winchester District Memorial Hospital (WDMH) as potential leaders in the introduction of a collaborative approach to support MedRec and Quality Improvement (QI) to better serve our rural patient populations.
Objective
The goal of this project was to (1) ensure that a Best Possible Medication History (BPMH) is received for each patient coming to the oncology ambulatory chemo unit and (2) ensure that the medications on this list are taken into account when conducting a DI checkup.
Winchester District Memorial Hospital
Winchester District Memorial Hospital is a rural teaching hospital in southeastern Ontario and serves a geographical area of 50,000 patients. The WDMH Brian Hough Chemotherapy Unit is a six-chair and one-bed unit that serves as a level 4 satellite oncology clinic in partnership with The Ottawa Hospital Cancer Centre. As a satellite unit, WDMH has fewer oncology-related resources than urban centres but can provide ambulatory facilities and support for the administration of low-risk to high-risk intravenous systemic treatment coordinated by a remotely available oncologist and an onsite physician with appropriate training in oncology. The unit’s 2016-2017 clinical volumes included 89 new systemic therapy patients initiated.
Initial practice description
Prior to 2014, WDMH had an informal process for MedRec for ambulatory oncology patients. During the first visit, the nurse would ask patients about their home medications. Patients would either communicate the list verbally or written (meaning there was no guarantee that the list was the BPMH). Subsequently, the nurse would verbally communicate the list to the chemotherapy pharmacist.
The burning platform that led to our work was discrepancies noticed between the patient’s medication list received from the nurse versus the one documented by medical oncologists on their progress note. Many of the discrepancies were associated with missed potential DIs that could result in either supra- or subtherapeutic chemotherapy levels. Supratherapeutic levels of chemotherapy levels can lead to many adverse reactions including neutropenia. Noticing the missed potential DIs, the team questioned whether these were contributing to the incidence of neutropenias they observed. Because of the multifactorial nature of chemotherapy-induced neutropenia, it is very hard to quantify this contribution; however, it is known that bettering MedRec systems does result in decreased incidence of DIs and should consequently eliminate this factor from the causative reasons for neutropenia.
Upon further investigation, it was discovered that there were many inadequacies in the “open-loop” system. Nursing and pharmacy staff observed local challenges impacting both the completion and communication of MedRec and resolved to engage clinical stakeholders with the aim of introducing a new closed-loop approach. The leadership team supported and identified MedRec for ambulatory oncology patients as an area that needed improvement.
Practice innovation
In 2014, the frontline nursing and pharmacy staff discussed the current process and identified areas for improvement. The rollout of the interventions was carried out in multiple PDSA cycles (PDSA stands for Plan, Do, Study, Act). It is a common tool seen in QI initiatives and is short for iterative cycles of planning the changes to be made (Plan), implementing the changes (Do), observing and studying what happened (Study), and making additional changes (Act).
PDSA-1 included the following interventions: Faxing community pharmacies requesting completion of a “MedsCheck,” a comprehensive medication review, funded by the Government of Ontario. Replies from retail pharmacies are received by the hospital pharmacy where the hospital pharmacist conducts comprehensive DI checkups based on home medications and chemotherapy. The results of checkups are then discussed with primary care providers (PCPs) and/or community pharmacists if there are DIs. The resulting changes in medication are then communicated to the patient and documented in the Electronic Medical Record (EMR) for the oncologist to see before entering their next order.
The results of PDSA-1 (refer to Table 1) triggered PDSA-2 which included: Modification in the MedsCheck request form based on input from key stakeholders. The modifications concentrated around two points: To ensure that the reply from the community pharmacy is faxed back to the nursing unit, not to the hospital pharmacy. This allowed identification of requests that didn’t receive replies. The form included an updated chemotherapy regimen which aimed at making community pharmacists aware of the medications the patient is receiving in the hospital. Modification in workflow and documentation (Figure 1). Staff education using a guiding sheet and education tracking plan.
Numbers of completed and non-completed MedRecs post PDSA 1 and 2
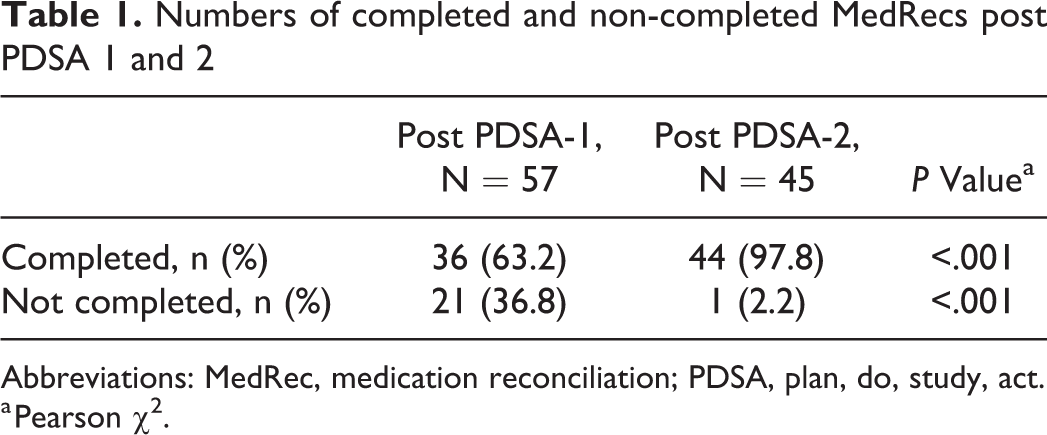
Abbreviations: MedRec, medication reconciliation; PDSA, plan, do, study, act.
a Pearson χ2.
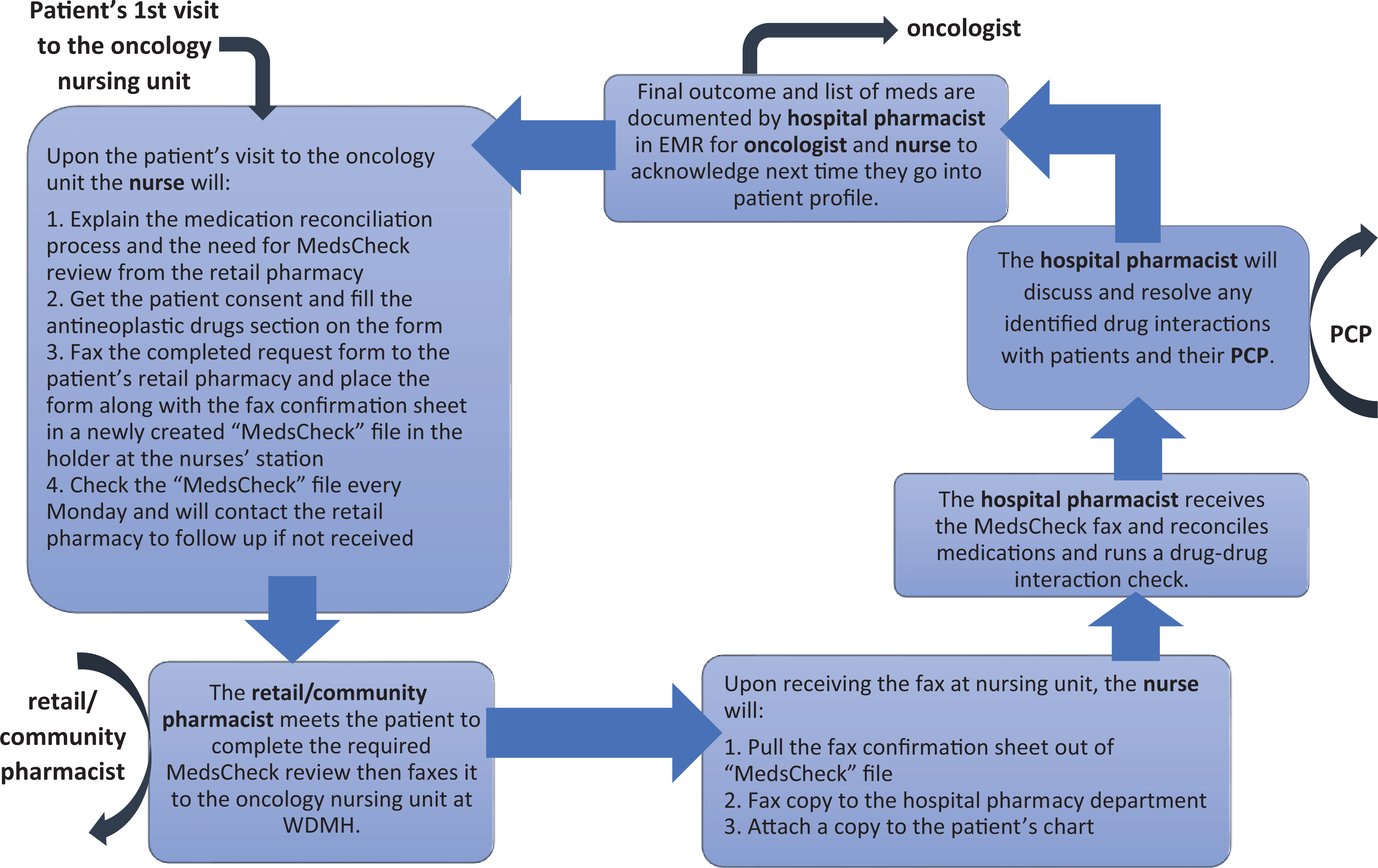
New workflow for MedRec process at WDMH. The nurse does these steps every time a patient is started on a new chemotherapy regimen, not just solely at the first chemotherapy appointment. MedRec indicates Medication Reconciliation; PCP, primary care providers; WDMH, Winchester District Memorial Hospital.
Although closed-loop MedRec is more reliable and less human resource intensive when there are adequate IT capabilities, those IT capabilities were not available at the time of this study.
Approach used
The “WDMH Quality Improvement Framework” was created collaboratively between WDMH leadership and stakeholders and after extensive investigation and consideration identified “Front Line Ownership (FLO) 5 ” and “The Influencer Model 6 ” as its main models. Whenever it is possible, these two models are used to guide QI studies.
Frontline ownership
Frontline Ownership is a QI approach that engages staff to empower them to creatively develop solutions to challenges they face each day and to create sustainable changes utilizing a sense of ownership, not buy in. 5 This is done by choosing frontline staff who becomes heavily involved in the project, in this case both a pharmacy and chemotherapy champion. They became leaders for the intervention roll outs including the education of fellow staff. 5
The influencer change model
This model is based on the theory that all actions have numerous environmental influencers. 6 There are six key areas of influence which can be used effectively to change a person’s behaviour. These areas are personal motivation, personal ability, social motivation, social ability, structural motivation, and structural ability. At least four of these sources of influence have to be successfully addressed for a person to change their behaviour. We used components of this model, for example, personal ability and motivation were addressed using an educational plan and medication discrepancies reports. Social motivation was utilized by engaging all stakeholders and having a frontline champion. Finally, structural ability was achieved by a clear and easy-to-follow process being created (refer to Figure 1).
Evaluation
Two equivalent audits after each PDSA-1 and -2 measuring: Eligible patients (Criteria: Ontario resident, valid Ontario Health Card, currently taking a minimum of three prescription medications for a chronic condition); Completed MedRec request forms; MedsCheck request forms with fax confirmations to the retail pharmacy and back to WDMH; and Status of the MedRec at the time of the audit (complete/incomplete).
Timeframe summary
PDSA-1 took place between December 2014 and March 2015.
The post PDSA-1 data were a retrospective chart audit of 57 newly started oncology patients who were enrolled in chemotherapy treatment at the clinic between January and August 2016.
PDSA-2 took place between November 2016 and March 2017.
The post PDSA-2 data was an equivalent audit of 45 oncology patients seen and treated in the chemotherapy unit from July 2017 to September 2017.
Results
The post-PDSA-1 audit shows 63.2% completion, showing success of the newly created process and a big jump from having no process. The post-PDSA-2 cycle showed a further significant increase in completed MedRecs with 97.8% completion (refer to Table 1 and 2).
Reasons for lack of completion of MedRecs reported in post PDSA-1 and 2 audits
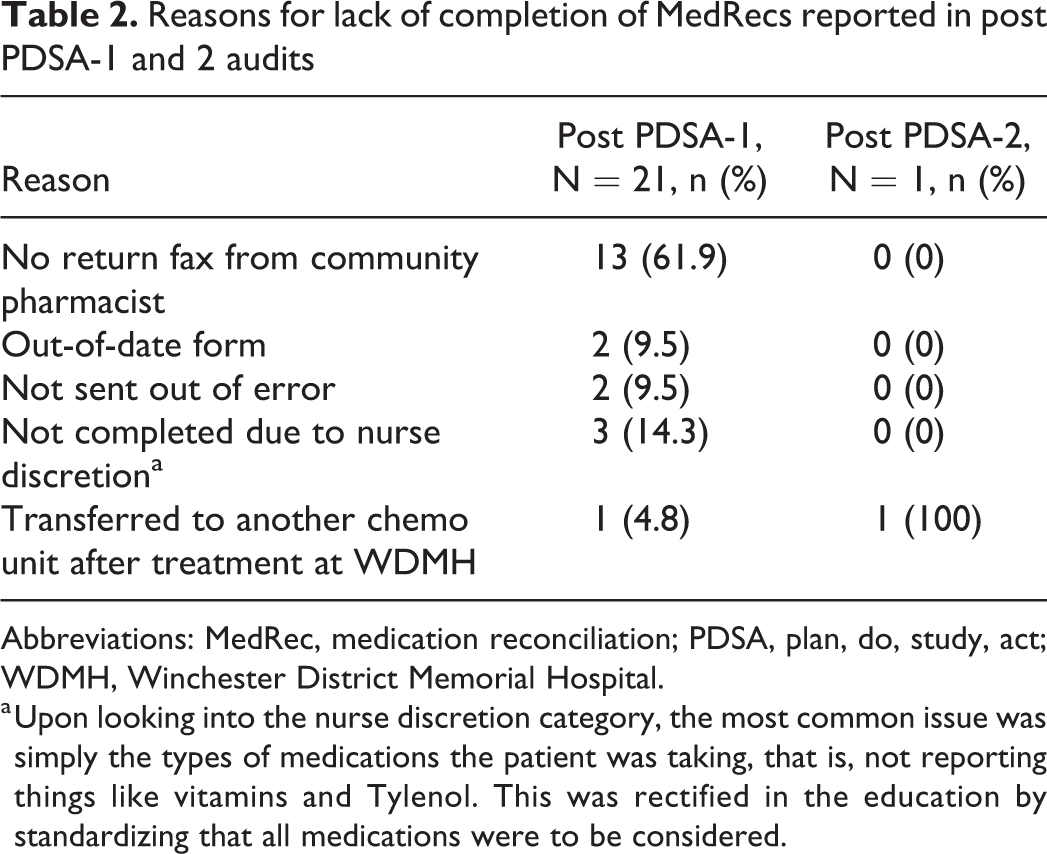
Abbreviations: MedRec, medication reconciliation; PDSA, plan, do, study, act; WDMH, Winchester District Memorial Hospital.
a Upon looking into the nurse discretion category, the most common issue was simply the types of medications the patient was taking, that is, not reporting things like vitamins and Tylenol. This was rectified in the education by standardizing that all medications were to be considered.
A review for the documentation in the EMR (the final step in the “closed loop”) revealed that in 17.8% of the cases, there was no traceable documentation by hospital pharmacists although the MedRec was completed. Despite the success of this frontline QI team, this slight unanticipated lack of documentation resulted in lowering of the outcome and highlights a need to modify the future audit to include the DI checkup findings.
The team regularly discussed any potential problems that arose from the new processes. At the hospital pharmacist and nursing levels, there were no significant changes in their daily workflow or workload. From the retail pharmacy level, there was an increase in workload, yet this increase was perceived positively due to being compensated by the “MedsCheck” program funding formula.
Our informal observation of patient experience could be grouped into two categories. The first, being the majority, were patients who felt grateful to the unit for catching things potentially missed by their healthcare provider as well as for going the extra mile to communicate to their circle of care to close the loop. The second category, a minority of cases, felt that doing a MedRec at the pharmacy was an added burden and thus weren’t able to do it.
Discussion
Introducing this “closed-loop” process enhanced the MedRec for ambulatory oncology patients at WDMH. After completing this project, we now know that we appropriately completed MedRec in 97.8% of cases within two PDSA cycles. While not measured within our own institution, there is a fair amount of literature showing the outcomes of an improved MedRec system, including reductions in medication errors such as omissions, duplications, dosing errors, DIs/ADEs and other side effects, unnecessary and/or repeat hospital visits, as well as preventing delays in treatment. 3,4,7
We believe our implementation led to successful results as our strategies were lined up well with the ISMP’s 2012 leadership reports mentioned earlier. Within this, their summits and survey of MedRec leaders’ reported key themes and success factors to optimize MedRec, which we echoed in our study.
3,4
These include: Leadership support: MedRec was identified to be a priority for QI by our leadership team early on. Interprofessional engagement: We included internal collaboration between chemo nurses, hospital pharmacists, administrative and leadership staff, research, and family/caregivers as well as externally with retail pharmacists, primary care providers, and oncologists. Engagement was also achieved through using frontline champions. Culture: Sustainable culture changes were achieved through using validated models such as FLO and Influencer. Education and training: We created a comprehensive staff education plan and materials delivered by frontline champions. Tools and resources: Many tools/resources stemmed from this initiative such as the workflow and posters created, champions to ask questions to, and the creation of “MedsCheck” request form. Measurement: The use of multiple PDSA cycles allowed us to collect data and track the improvements over time.
While themes and success factors are important, few real models for MedRec have been well described, especially regarding rural environments. It is often difficult to draw comparisons to literature as each institution utilizes strategies most effective to them, the majority of which are urban centred. However, considering that many limitations are shared by rural hospitals, we believe that our MedRec system is one of the first that could be transferrable to other rural institutions who are facing similar challenges. Our strategy of engaging others who might be funded to do the job such as engaging the retail pharmacies to do “MedsChecks” achieved a credible and reliable method of reconciliation that didn’t require significant funds/human resources, advanced technology, or a high level of direct contact between the interfaces of healthcare (all challenges faced by rural organizations).
WDMH’s interests include contributing to the quality of rural research through building capacity. Consequentially, we developed a structured means of carrying out improvements that could be adopted by other rural organizations. We identified a common issue here in that we sometimes return to previous behaviours. Because the potential cultural resistance associated with implementing new processes can often be a barrier to sustainability, we opted to use a validated framework to ensure sustainability. This includes FLO, which is intended to create a culture of ownership that will sustain the behaviours developed by the QI interventions. 5 We also avoided the common mistake of relying on education as the main force to change behaviour. Instead, we imported the “Influencer” model of change and maintained four sources of behavioural change. 6 Research suggests that this model is 10 times more likely to produce significant, sustainable behavioural change. 6 These two models in addition to PDSA cycles are paramount to sustainable improvement. We believe these ideas are generalizable to many different QI initiatives and organizations. By developing rurally conscious QI models that have proved to be successful, it allows us to share these tools and resources for all healthcare facilities to use and benefit from.
Conclusion
This study showed that upon addressing inefficiencies using a QI framework, the MedRec system increased in both accuracy and efficacy while promoting internal sustainability, working within the resource constraints typical of a rural hospital. We believe that through our descriptions, this model could be replicated within a similar environment, thereby providing a means for other rural centres to provide optimal treatment to chemotherapy patients in addition to supporting their own QI endeavours.
Footnotes
Authors’ note
Data is available from the corresponding author upon reasonable request. This QI study received an administrative review and REB exemption was granted by WDMH ethics board.
Acknowledgments
The authors would like to acknowledge the cooperation of the chemotherapy unit and the pharmacy unit staff in the study hospital.