
Abstract
Healthcare organizations engage in continuous quality improvement to improve performance and value-for-performance, but the pathway to change is often rooted in challenging the way things are “normally” done. In an effort to propel system-wide change to support healthy eating, Nova Scotia Health developed and implemented a healthy eating policy as a benchmark to create a food environment supportive of health. This article describes the healthy eating policy and its role as a benchmark in the quality improvement process. The policy, rooted in health promotion, sets a standard for healthy eating and applies to stakeholders both inside and outside of health. We explain how the policy offers nutrition but also cultural benchmarks around healthy eating, bringing practitioners throughout Nova Scotia Health together and sustaining collaborative efforts to improve upon the status quo.
Background
Benchmarking for healthcare quality improvement
Originating in a critique of patient safety, 1 quality improvement in healthcare management has evolved into a diverse field of practice. 2 Organizations engage in quality improvement to improve performance and value-for-performance, but the pathway to change is often rooted in practice—for instance, changes optimized in a specific service area, which can then be scaled (eg, virtual care pilot projects in rural Nova Scotia). 2,3 Continuous quality improvement refers to the idea that quality improvement is a process and requires repeated tests of change. 4,5
Identifying and setting benchmarks has become a critical component of quality improvement measures. 6 Benchmarks are measures that set intra- and inter-organizational performance goals while balancing cost considerations and stakeholder/public expectations. 7 They are essential to achieving the healthcare “triple-aim.” 8,9 Benchmarking can also be considered an active method for quality improvement. 7 For instance, intra-organizational benchmarks can be established in an integrated care pathway development process 10 ; inter-organizational benchmarks such as wait times can support analysis of appropriateness of care. 11
In the following article, we focus on benchmarking in intra-organizational quality improvement through an applied discussion of the Nova Scotia (NS) Health healthy eating policy. As per Ettorchi-Tardy, we will examine benchmarking as a “comparison of outcomes…to stimulate cultural and organizational change within the organizations being compared” (emphases added). 7 Although benchmarking commonly occurs between organizations, we examine this benchmark within NS Health, an organization with a wide variety of facilities, areas of practice, and past histories with healthy eating policies.
In addition, we address gaps in the literature on benchmarks that serve health promotion functions. To date, much healthcare benchmarking research has centred upon inpatient care. 6,12,13 Some authors have examined how healthcare benchmarking and quality improvement can be adopted in health promotion organizations 14 and community settings such as schools. 15 Others have challenged whether or not benchmarking should be applied to health promotion, given benchmarking’s more transactional industrial origins and focus on quantitative metrics, in contrast to the relational issues central to health promotion. 16
However, increasingly, attention has been drawn to the role that healthcare service delivery organizations themselves play in broader population health and health promotion. 17 Health organizations’ internal policies and practices can affect health behaviours well beyond their patient populations and have even been referred to as anchors within their communities. 18 By examining a healthcare organization’s healthy eating policy, we have the opportunity to consider how benchmarking in healthcare can benchmark health for a wider variety of stakeholder audiences.
First, we will provide a brief introduction to healthy eating policies developed in Canada for healthcare organizations. Second, we will describe the governance context and content of the NS Health healthy eating policy. Third, we analyse the NS Health policy as an internal benchmark to influence culture and explain how benchmarking has begun to emerge through Plan-Do-Study-Act cycles following adoption of the policy. Fourth, we conclude with the generalizable lessons from this health promotion example for quality improvement and the potential application of findings in cases of external benchmarking.
Context and setting
Healthcare organization healthy eating policies in Canada
Healthy eating policies are a growing healthcare priority. 18 Diet-related diseases are a leading cause of death and disability in Canada and driver of healthcare costs, 19 making dietary improvement essential to population health promotion. 20 Previously, healthy eating initiatives in healthcare tended to fall within service lines for cardiovascular disease prevention. 21 Over the last decade, hospital healthy eating policies have shifted to focus on the consumer food environment (eg, retail merchandising such as placement, promotion, and pricing) and the information environment (eg, nutrition labelling, sponsorship). Table 1 provides a comparison of major healthcare healthy eating policies in Canadian provinces and territories.
A comparison of major healthy eating policies in Canadian provinces and territories
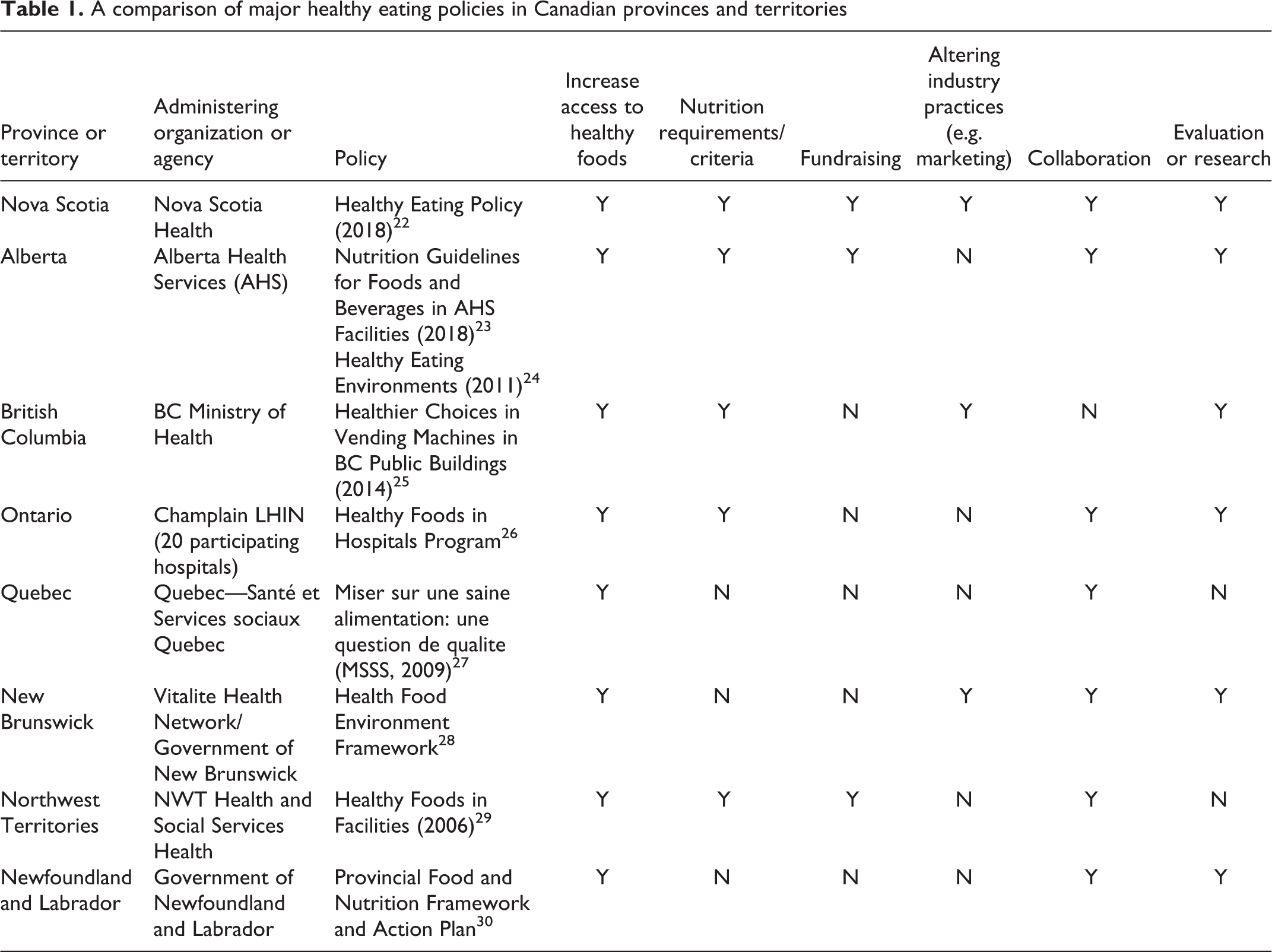
Some jurisdictions have cross-cutting policies that cover public institutions. For example, the Northwest Territories policy deals with nutritious and affordable food and beverage options in schools, recreation centres, and government buildings. Other policies target specific consumer environments to encourage upstream food supply reformulation, such as the BC vending machines policy.
Two provinces have comprehensive healthcare healthy eating policies, integrative of the food environment. The policy by Alberta Health Services looks at food and beverages offered, optimizing the availability of nutritious choices, but also looks at promotions, marketing, and an overall culture of healthy eating. Similar to NS Health, Alberta is the only other province whose policy centres upon supportive environments. In 2009, Nova Scotia’s Capital Health (now NS Health Central Zone) was the first health authority in Canada to establish a comprehensive organizational healthy eating policy and strategy. 18 However, the standard, or benchmarks, of a supportive eating environment within health institutions has not been well defined, which makes it difficult to compare inter-organizational healthy eating policies and engage in inter-organizational benchmarking. Therefore, we will focus on the benchmarks and benchmarking (intra-organizational) of the NS Health healthy eating policy.
Nova Scotia Health
In 2015, NS Health amalgamated to one health authority, becoming the largest provincial health authority in Atlantic Canada, responsible for delivering healthcare services to 923,598 provincial residents 31 through 10 hospitals, 8 ERs, and 135 community locations. 32
Prior to amalgamation, five of the nine regional authorities had their own healthy eating polices. Each policy defined healthy eating differently and differed in scope, resulting in a patchwork. For example, in 2009, the aforementioned Capital Health was an early adopter of a healthy eating policy. 18,33 Their policy focused on promoting health and wellness through measurable standards for food retail settings, cafeterias, and vending machines. In contrast, the Colchester East Hants Health Authority targeted healthy eating within occupational health and safety 34 but did not mandate nutritional standards when serving food and beverages at internal and external events. 22
Three years after amalgamation, NS Health adopted a new healthy eating policy, resembling elements of former regional policies, while embracing a new population health approach. 22 This policy replaced the five former policies and integrated updated nutrition evidence, federal guidance, and best practice (see Figure 1) across all NS Health facilities.
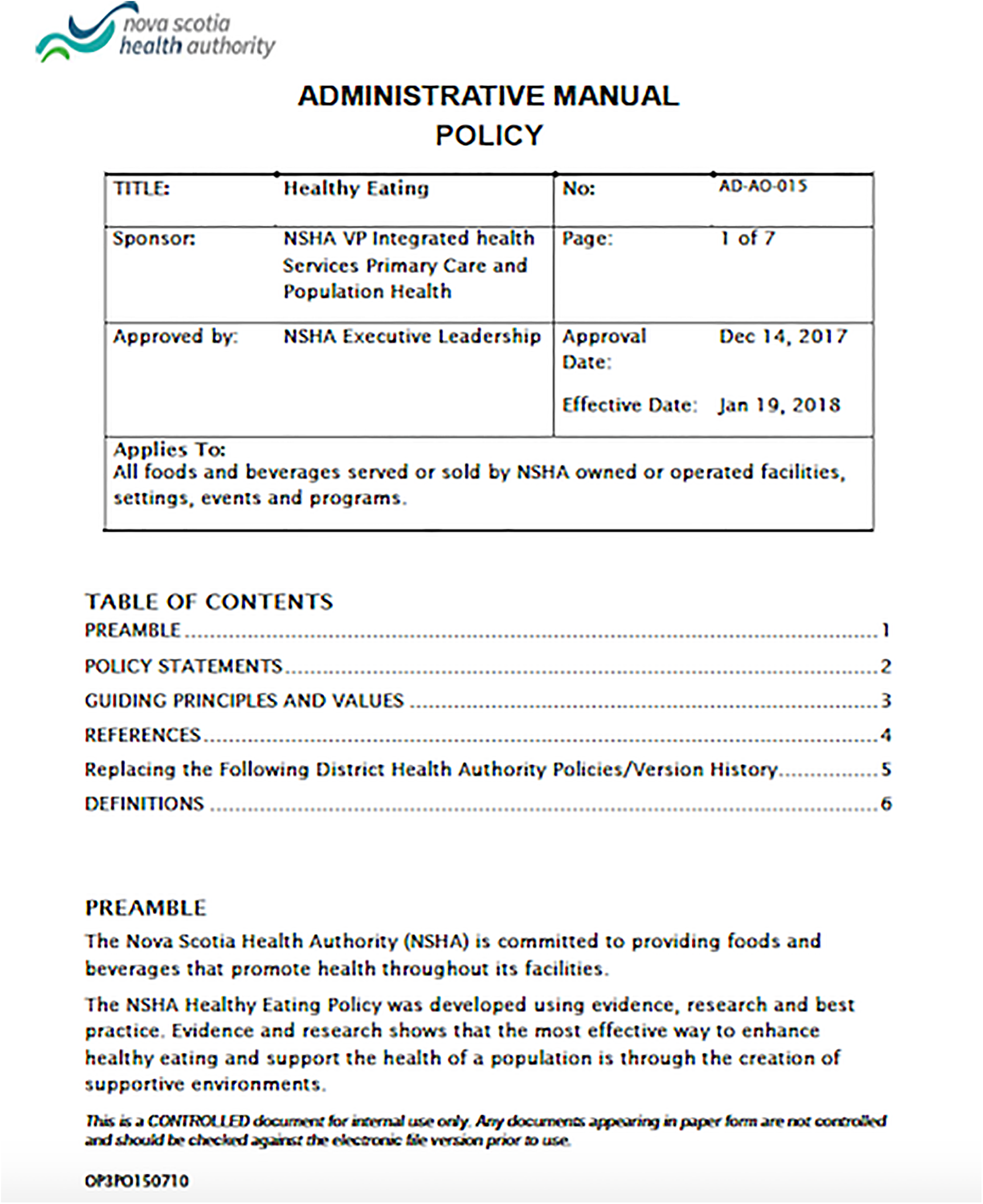
The NS Health healthy eating policy.
NS Health healthy eating policy
The 2018 NS Health policy falls under the service mandate of NS Health Nutrition and Food Services, with advisory support from a Steering Committee comprised of a Senior Director, Nutrition and Food Services directors and leadership, dietetic and nutrition practitioners, communications, and representation from the Foundation and Auxiliaries, patient and family advisory, and external research.
The policy applies to all food and beverages sold or served at NS Health facilities, events, or functions and draws an explicit evidence link between food, nutrition, and downstream health outcomes. The policy is aligned with other jurisdictional frameworks on healthy eating, including the federal Healthy Eating Strategy and Canada’s Food Guide. 35 Its explicit purpose is the creation of supportive food environments, which according to best practice is one of the most effective ways to influence health (see Figure 2). 22
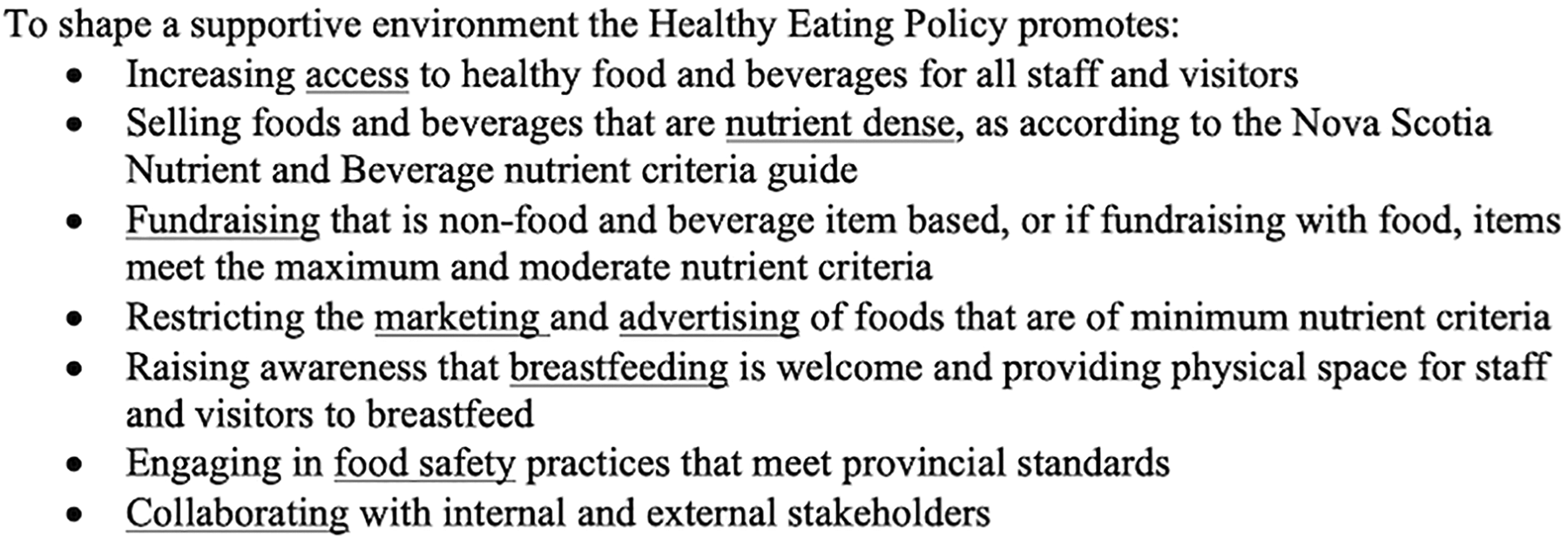
Excerpt from the NS Health Eating Policy, 2018, defining supportive environments.
The policy goes beyond physical locations
It is applicable to all NS Health social and built environments in which food and beverages are served: food retail and food services settings across the province, including cafeterias, coffee shops, and vending machines; special events and catering; associated procurement; and staff-specific consumption in healthcare settings as well. These social and built environments vary across the province, in communities ranging from urban centres to rural villages. This broad conceptualization of the food environment is consistent with other institutional contexts such as schools and shows that healthy eating is more than what we eat—it is how, why, when, and where eating occurs. 35 The policy explicitly states its intent to shift food “culture” towards healthier eating by engaging stakeholders throughout the system 18 and moving away from healthy eating as a “cafeteria policy” or “nutrition policy.”
Notably, the policy takes a food systems approach, addressing the pathway from farm to table. It also considers food waste and sustainability, including the ecological footprint of procurement, prioritizing food that is locally grown or combination meals cooked from scratch ingredients and prepared in site kitchens.
The policy reaches beyond food as an individual choice
The policy reinforces that food choices are more than the combined choices of individuals alone. It names NS Health as the “leader” to create a supportive environment, establishing avenues to implement further evidence-based programs and interventions under the auspices of the policy. The nutrition standards associated with the policy are based on province-wide nutrient composition guidelines within the Nova Scotia Food and Beverage Nutrient Criteria, also adhered to by public schools, recreation centres, and daycares. 36
The policy accommodates both exceptional and everyday circumstances
In comparison to the earlier patchwork of regional policies, the new policy addresses routine service delivery as well as special circumstances where performance standards might be needed. For instance, while past regional policies contained exceptions, the new policy is inclusive of all events under the auspices of the health authority—from a retirement celebration to an auxiliary fundraiser.
Healthy eating and quality improvement
Healthy eating policy and benchmarking
The following section will explore two specific aspects of intra-organizational benchmarking based on the criteria and definition by Ettorchi-Tardy: to set a standard for healthy eating culture, and second, how it prompts tests of change.
First, the policy is clear that a culture of healthy eating must be cultivated through practices of all individuals engaged through NS Health mandate—from executives to clinical service and support managers, frontline care and service providers, volunteers, patients, and visitors. These stakeholders have different priorities and roles when it comes to food decision-making. For example, a hospital foundation may raise money through catered events; clinical practitioners may be customers at the cafeteria; retail workers make decisions through everyday stocking and cooking operations. Yet a supportive food environment requires aligned efforts by each of these individuals and service teams.
Bringing together frontline practitioners to build consensus and manage change is a key aspect of benchmarking. 4 The involvement of practitioners relies on lived experience and knowledge at the patient or staff level and sets up the process of quality improvement for a greater orientation to the specific changes to practice that need to be implemented. 4,5,37
By creating a Steering Committee that features experienced interdisciplinary and frontline representation from diverse teams across the province, NS Health has attempted to create a forum for advancing a cultural conversation. The committee flattens the management hierarchy and gives voice to those with differing responsibility and power in the organization. In meetings to date, discussion has featured practical observations about “junk food hot spots” to concerns about being labelled “food police” among those responsible for monitoring and measuring implementation of the policy. The design of the policy has served as a guide for deliberation: to challenge the way things are done, comparing what is to what could be, and to ask “how can this be done better.” 38
Second, the NS Health healthy eating policy embeds principles of health promotion within a quality improvement implementation paradigm. The Plan-Do-Study-Act cycle (Shewhart or Deming cycle) 16,37 is a way of ordering tests of change to organizational practice within quality improvement. The cycle involves an assessment of the problem (Plan), followed by a change in practice (Do) and analysis of the outcome (Study) to informs future practice (Act).
Accessibility, comprised of affordability and availability/variety of healthy products, is a key part of the healthy eating policy and provides an opportunity to integrate healthcare organizational (cost) and health promotion (equitable access) considerations. Price promotions to encourage purchasing of healthier options have been a growing area of food environment research, 39 becoming increasingly relevant to concerns of nutrition managers. A workplace survey had also been carried out with retail food services employees, prior to implementation of the policy, where staff shared the perception that healthy foods within the cafeteria were “too expensive.” Healthcare organizations are different from other retail food operators in that they may be able to operate on a “break-even” rather than profit motive. This is the case for NS Health, which used this capacity to establish a linked standard operating procedure to the healthy eating policy explicitly targeting affordability and accessibility for consumers—who might be staff at different compensation grades or diverse patients and visitors.
The NSH’s Nutrition and Food Services team has also begun to experiment with retail merchandising efforts that integrate price promotions to incentivize healthier choices. A PDSA cycle “makes it easier for previous practice to be discontinued and innovations to be accepted, implemented and spread throughout the healthcare organization.” 37 Rather than implementing these best evidence practices simultaneously throughout the province, price modifications were first identified by staff and then tested incrementally. Further, partnering with academic research partners (our team of co-authors), NS Health has evolved these tests of change to evaluate the impact of targeted pricing changes (increase in price for less healthy options, decrease in price for healthier options) in combination with placement (healthy and unhealthy alternatives side by side) and promotion (large pull-up banners marketing healthier items) strategies, through analysis of point-of-sales (POS) data.
Sales data represent a valuable administrative dataset within healthcare organizations and food environments research. It is typically used for supply management, but the nutrition literature has demonstrated the value of in-depth sales data analysis as an important proxy measure for dietary outcomes. 40 The NS Health policy has catalyzed the development of both internal and external expertise to evaluate sales data. The findings from the initial evaluation will inform the next cycle of testing and facilitate a comparison of sales outcomes between sites.
Discussion and implications for future practice
This paper describes the NS Health healthy eating policy and its role as a benchmark to shift the food environment towards one that is supportive of healthy eating for staff, families, and entire communities within NS Health. Benchmarking within healthcare systems is a method of practice within quality improvement that often focuses on comparing clinical indicators between organizations; however, it is also used for intra-organizational or system-wide evaluation. 7,41 Benchmarking for health promotion, and specifically nutrition promotion, is a newly evolving area of study, primarily studied within schools. For instance, Biggs et al recently used a process map to analyse the quality of a nutrition primary prevention program in Australian schools. In Nova Scotia, researchers have also assessed policy adherence to nutrition policies in schools from an implementation perspective. 42 Yet as we have discussed in this paper, NS Health has demonstrated that healthcare healthy eating policies can become an important exemplar for benchmarking for health promotion purposes. Furthermore, the internal benchmarking process initiated by the NS Health healthy eating policy has highlighted emergent areas for future research in this area.
Novel data collection: Benchmarking within health promotion can be challenging because the indicators and goals are often focused “upstream” on concepts like empowerment, resilience, and here culture. 16 These changes may be difficult to measure using traditional benchmarking methods. Collecting qualitative data, or in our case, establishing deliberative forums, and creative use of administrative data (eg, POS data) are just a couple of promising approaches.
Ongoing improvement is critical: An upfront investment is required in quality improvement to demonstrate value and cost-effectiveness. As we have discussed in this essay, healthy eating policies, because of their organization-wide impact, can support diverse managers and frontline staff alike to adopt processes to evaluate practices within and across teams. 16,43 This must be done with some care, since engaging in tests of change, without controlling for context or confounders, may oversimplify findings. 44
Systems approach: Healthy eating policies are designed for internal impacts within the organization, yet due to their harnessing of food systems, integrate community impacts as well. 16 Since there is skepticism among some scholars and practitioners that quality improvement leads to practical changes, critics may suggest quality improvement may simply pave the path to cost containment rather than the health of a patient or community 16,45 —in essence, the opposite of a systems shift. A food system lens integrated into healthy eating policies can help healthcare organizations refine their understanding of healthcare service delivery beyond service lines. It can alert staff and decision makers to the broader opportunities for society-wide change.
Conclusion
In this article, we have explored the NS Health healthy eating policy as a benchmark for creating supportive environments to promote health. The policy emphasizes the importance of the food environment and its impact on improving diets at a population level. The policy brings NS Health stakeholders together and prompts tests of change to shift towards a culture of healthier eating.
Benchmarking in healthcare is not yet well understood outside of clinical care. In health promotion, the definition of the population and methods can diverge from the traditional quality improvement literature and present challenges when trying to “fit” health promotion within the traditional quality improvement approach. 16 Healthy eating policies can serve as a bridge for healthcare organizations to consider the pathways to enacting supportive environments for changing population health.