
Abstract
Health systems are now organized across England to deliver a more integrated population-based approach, not competing for services, rather collaborating and driving better value for the population from a fixed resource. This approach of health system leadership and collaboration has resulted in governance including a mixed economy of public-private provision but with greater alignment to delivering an agreed set of outcomes and value-based healthcare for the population. This dramatic shift from provider competition to collaboration and integration means a reframing of contracting and partnerships with the independent sector.
Introduction
The National Health Service (NHS) continues to use the private sector in a range of ways for the delivery of services, ranging from cleaning, supply chain, digital, diagnostics, with much of primary care operating as independent contractors to the NHS. These arrangements work best where there is an opportunity for the independent sector to compete and deliver value; it is also evident in more complex service areas such as mental health, where the independent sector is able to offer specialist provision, but this must be through and with other parts of the health and care system, and the future approach to contracting must create collaboration and a focus on quality and value for the population served. Canadian policy development in this area might consider how this contracting approach can be adapted to enable a mixed economy of public and private provision within a provincial publicly funded health system.
Background
In the United Kingdom since the 1980s, successive governments have seen contractual mechanisms to secure services for public sector funded care or service delivery as a route to more efficient and effective public services. As a result, the role of private and voluntary sector organizations in service delivery has increased significantly. In 2008, the De Anne Julius Review suggested that the UK public service industry accounts for over 6% of gross domestic product, generating some £80 billion (bn) in revenue while employing well over 1.2 million people (note 1). In healthcare, NHS England accounts 2018-2019 show a £113bn investment in the purchase of NHS healthcare, £13.7bn is from non-NHS providers, £2.9 million from dentists, £1.9bn from pharmacists, and £16.7bn from general practitioners (GPs) including prescribing. All of this group (representing 30% of the total NHS investment or £35.7bn) include NHS contractors who treat NHS patients under a contract, rather than NHS Trusts, Mental Health, and Community providers (whose assets and liabilities come onto the NHS balance sheet).
This contracting approach has survived different political and policy approaches and has combined with a quasi-internal market approach with separate governance and regulation of purchaser and provider sectors, contractual approaches, and a focus on transactional payment, and savings, also reinforced in European Law on public procurement for services. National procurement of services commissioned by NHS England has delivered 1% or £284.4 million priced savings over 2015 to 2020 (note 2).
The importance of the “NHS contract for NHS services” overrides the corporate form of the provider, this contract determines the service scope, specification, outcomes, and payment, all services to the NHS are provided under a contract, but this varies between Hospital and Community services and Primary Care, where there are dedicated separate contracts for GPs, pharmacists, dentists, and optometrists. This approach raises a fundamental question of how these different contracts come together to drive benefit.
Complexity of driving benefits from contracting
Contracting can help secure benefits in quality, costs, and outcome. Contracting out for non-core services (note 3), for example, where there is a healthy competition for quality and cost but needs reframing for integrated care systems to address challenges this presents. Where service lacks objective or quantifiable measures of the value added by the specific provider, it will be more difficult to price contracts and monitor performance. If services that depend on one another to achieve their outcomes are contracted out to competing organizations, it may be more difficult to incentivize and secure the necessary cooperation between providers. Where a service requires investments in highly specialized physical or human resources, commissioners may find it costly to attract providers, and over time, could be left vulnerable to a provider with excessive market power (see example below on specialized mental health provision). If demand for a service is not known in advance, or subject to unpredictable variation, commissioners may find it costly to incentivize investments and/or may be left vulnerable to “hold-up” situations. These barriers need to be addressed to enable benefits from contracting for integrated care.
Independent sector in the pandemic
Contracts with independent providers during the pandemic to maintain access to cancer surgery for example has worked well where there is a partnership between the local NHS Trust provider and the Independent Sector partner, often with shared consultants working additional sessions in the independent sector and treating priority NHS-funded patients with cancer. Although these services are dependent on wider services for referral and follow-up care, they can be clearly transacted, with discrete outcomes for the intervention; therefore, the benefits of bringing in capacity to deliver access are viewed as outweighing the costs of contracting this capacity.
Nightingale Hospitals were also established via national contracts, which rapidly repurposed private sector conference facilities for either critical care or step-down care. The private sector provided the facilities management and infrastructure, and the NHS provided the operational care.
Choice and capacity
The NHS has had a range of initiatives over the recent history to increase choice and capacity which appears to work best through and with the local NHS healthcare partnership, and with fixed price services or marginal rates rather than full price.
The “Any Qualified Provider” contract was developed in 2012 to stimulate choice and build new capacity in priority areas such as mental health and community services and create a level playing field between NHS providers and non-NHS providers. Providers qualify for the service area on a fixed price, which is offered to patients by GPs under patient choice; selection is therefore on quality not price.
The NHS continues to contract for Diagnostics capacity to supplement key pathways, of note was the national positron emission tomography/computed tomography procurement to bring in additional capacity. The first phase was priced at a cost per case, and growth at 10% resulted in poor value for money. Subsequent phases offered through NHS led bidder and partnership and marginal rates which provided better integration and value.
Although these examples demonstrate the ability to increase capacity and choice, it needs balancing with the significant downside of this market-based approach where providers decide which services they will offer and the population they serve.
Canadian policy-makers may consider how best to include private sector capacity in the recovery of healthcare access after the pandemic within a health authority-managed relationship that provides consistent quality, outcomes, and value approach.
A lack of population-centred provision
In the United Kingdom, the Mental Health and Learning Disability/Autism population has got independent sector provision for some of the most vulnerable patients. For all adult and children’s, specialized mental health services around 32% (note 4) is provided by the Independent Sector; however, in some key service areas, the independent sector is the major provider of services: children’s and adolescent eating disorders 65%, psychiatric intensive care is 64%, and low secure 85%. These services are provided by very few providers. A review of these services has identified fragility in staffing, challenges in maintaining the quality of care and some providers leaving the marketplace due to economic factors. The contracting of these services to independent sector providers therefore needs greater oversight due to the needs of patients; the long-term outcomes, patient experience, and quality measures; and the need for a population and whole pathway approach for this segment of the population. Later in this article, we describe the Mental Health Provider Collaborative as a response to this problem of oversight and coordination.
Population health management approach for future PPP arrangements
The NHS has recently published a long-term plan which set out a vision for integrated care systems enabled with a “Removal of the counterproductive effect that general competition rules and powers can have on the integration of NHS care” (note 5).
After 30 years of the purchaser-provider split and targets mostly focussed on waiting times, it is understandable that at times we forget that the NHS is a universal healthcare service which is underpinned by seven principles of the NHS Constitution (see Table 1) (note 6).
NHS Constitution Commitments
Source: The NHS Constitution, England
Achieving these standards (or similar standards in Canada) requires active intervention by health leaders.
In England, there has been a commissioning role that has operated at this interface between the population and the provider, using contractual, organizational level payment for the activity delivered. This can result in multiple commissioners working with the same providers, and a lack of population or pathway focus to driving improvement (see Figure 1).

Commissioners contracting with same providers.
There is a shift now toward a role of a strategic commissioning function to address these problems and offering four leadership roles.
First orientate the system to work in populations. This is not just geographical areas; it should also be defined by need, so all people: at the end of life; requiring urgent care; or who are frail. The Bridges to Health 1 being piloted by NHS England is such an approach. The schematic below highlights the need for population segments, across tiers of care and population size (see Figure 2).
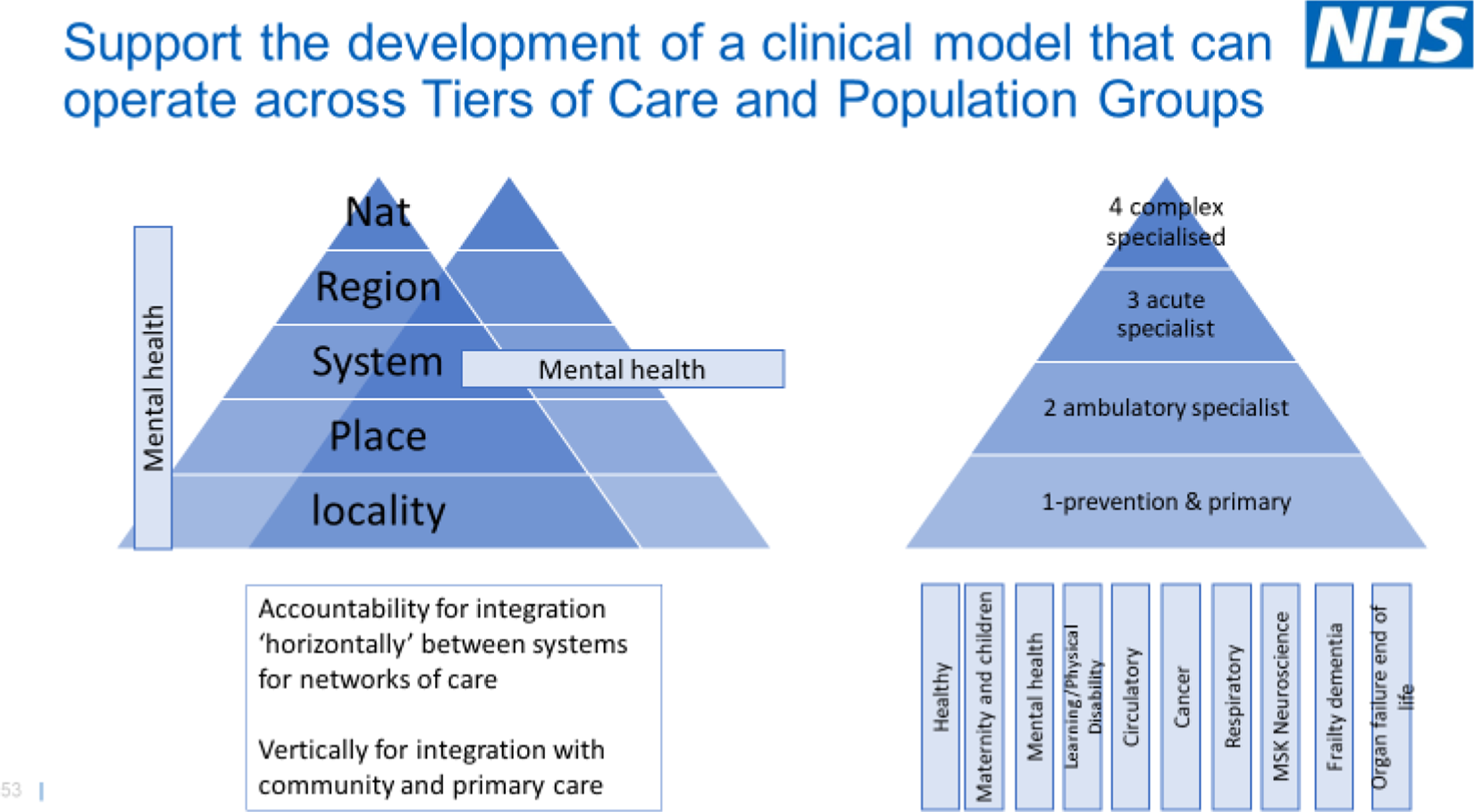
Commissioning for populations.
Second, for each of these population segments, there should be a clear aim and defined outcomes. Third, there must be some deliberative allocation of resources to the population segments by the strategic commissioner based on need and fairness, not on historical activity.
Finally, the strategic commissioner needs to balance learning and accountability. They need to enable and maximize learning with clinical leadership networks, analytics, measurement, benchmarking, collaborative improvement, and knowledge management. But at the same time, a strategic commissioner needs to hold system providers to account. The role of commissioners was set out in the NHS long-term plan “commissioners will become leaner, more strategic organizations that support providers to partner with local government and other community organizations on population health, service redesign and implementation” (note 7).
Canadian policy-makers may consider how these four roles feature in health authority management and accountability arrangements.
How can this strategic commissioning approach work across both public and private sectors?
The contractual and accountability frameworks now available to commissioners will support this revised approach, which enables contracting for standards and outcomes, for population needs, and for natural geographies. This next section broadly covers these approaches and addresses the issue of how the public and private sectors will operate within this framework.
This population approach, together with a set of clear principles for a more strategic approach to commissioning, is now being adopted across the English healthcare systems using consistent process and principles.
Commissioning cycle
These principles and overall approach apply to each level of geography (in Canadian context, region or sub region might be a province or health authority, see Figure 3).
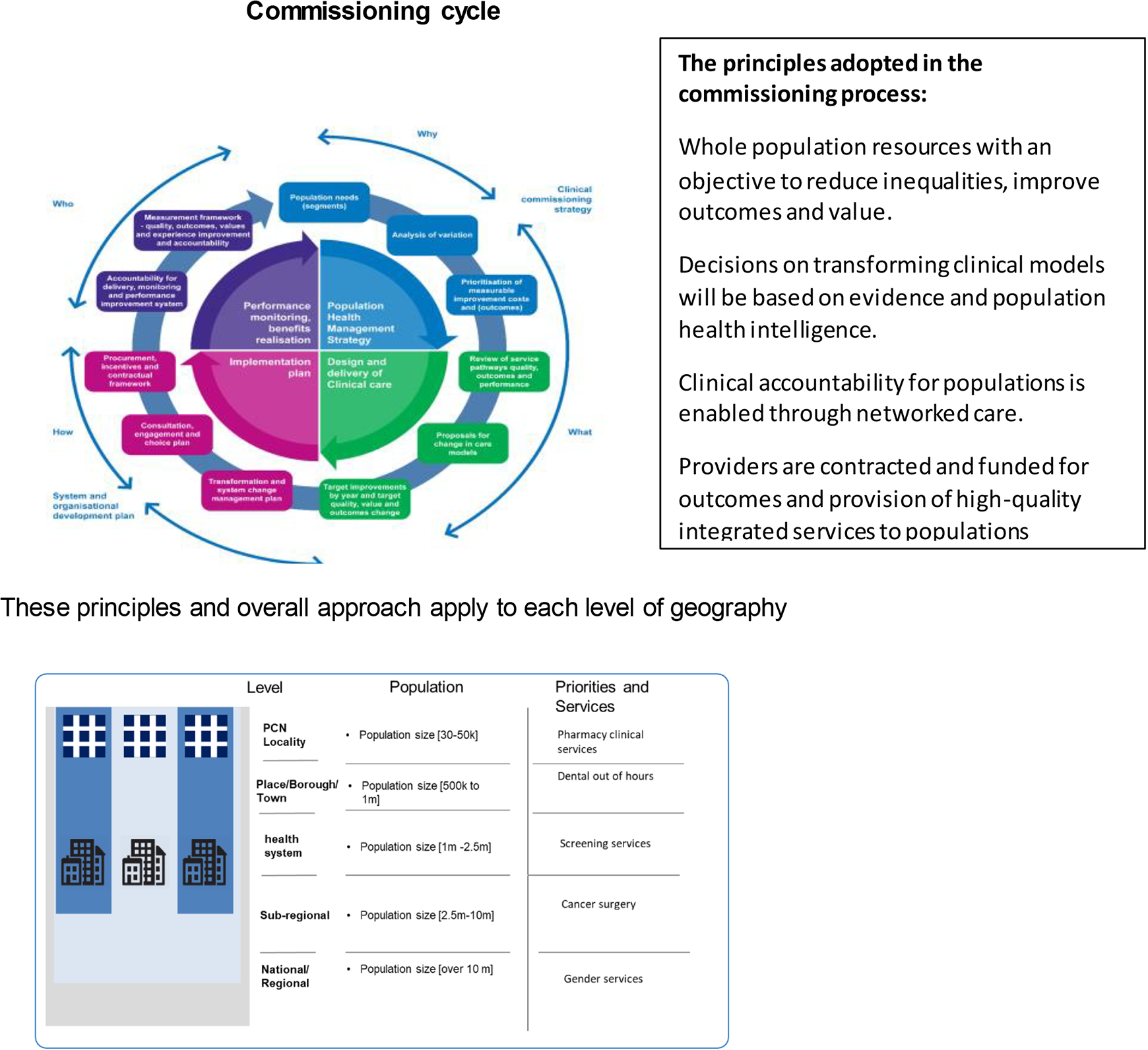
Strategic commissioning process and principles.
Contracting agreements that enable this approach
There are effectively two forms of contract that may enable integration and collaboration, one that encourages providers to work with each other across a specific speciality or program, reducing unwarranted variation and managing the population together for equitable access, through a collaboration with a “lead provider.” The second enables integration in geography, or place, between different providers from primary care, community through to acute and tertiary care, with either an integrated care provider contract or alliance agreement (which overlays individual NHS service contracts).
Mental Health Provider Collaboratives are an example of this. These are currently being formed across the English health system. They comprise of both NHS and Independent Sector providers within a single collaborative for a regional area. These providers agree with the lead provider for a service/speciality area which is then designated as the contractual lead, receiving the funding for the entire service, and manages a range of subcontracts across the region. This lead provider is responsible for achieving consistent standards and ensuring quality and access to care. This is achieved through clinical leadership and a clinical network operating between the different entities within the collaborative to manage care standards. The inclusion of independent sector provision was an important objective for these collaboratives, ensuring patients receive high-quality care and can move easily between providers (see Figure 4).
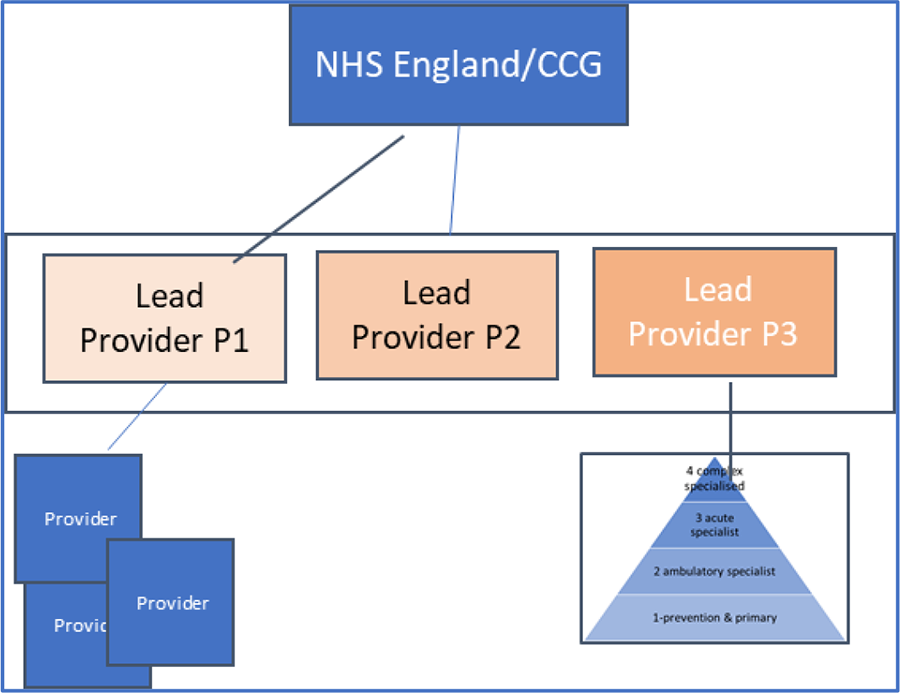
Collaborative contracting with lead provider.
Integrated Care Provider Contract is also a new contract that enables primary care (GP services) contracts under GMS (note 8), PMS and APMS to be integrated into a single larger scale place-based service contract with a patient list. This contract can then also be used to provide an umbrella for NHS services provided by local hospital community services and social care all under the same single agreement. This can also include independent sector provision and care providers.
A variation of this is an Alliance Agreement which wraps around existing contracts; it is not a service contract but offers aligned objectives and agreed priorities for delivering services with incentives aligned to this agreement.
Primary Care Networks, although well understood in Canadian health systems, are new in the NHS. These have a network agreement that enables practices to work on a range of enhanced services for the population, to develop workforce plans and digital transformation.
Conclusion
Public-private partnerships in the United Kingdom have often been related to acute hospital care and access to surgery. This article however describes a wider scope of how the NHS can contract with providers across primary care to mental health areas. The article has illustrated the challenges in determining the mix of provision and complexity and interdependency of services elements makes traditional activity-based contracting less effective. The article concludes with the movement toward population-based approaches to commissioning and contracting that encourages this collaborative outcomes-based approach.