
Abstract
The implementation of Person-Centred Care (PCC) by primary care teams is complex. Framed through the Quadruple Aim, successful healthcare system redesigns result in improved health outcomes of individuals and populations, reduce costs, and ensure an engaged and productive workforce. However, how can primary care teams achieve the Quadruple Aim? This article provides a learning and performance framework to support PCC through a Team-Based Care (TBC) ecosystem approach. We developed our approach using action research to improve TBC orientations, workshops, and consultations for teams and their leaders in Urgent Primary Care Centres and Primary Care Networks in Canada. This paper provides a synthesis of our experience in the context of the relevant evidence. We aim to share our efforts and acknowledge that our experience is still ongoing and complemented by ongoing improvement activities by others in the TBC ecosystem.
Background
For over half a decade, British Columbia (BC) has embarked on the redesign of primary care services to attain the Quadruple Aim of improved health outcomes for individuals and populations, reduced costs, and an engaged and productive workforce.1,2 This initiative has been supported by a series of position papers and policy instruments, which have clearly featured the need to shift to a team-based model of care.3,4 In BC, Team-Based Care (TBC) is defined as “multiple healthcare providers from different professional backgrounds work[ing] together and with patients/clients, families, caregivers, and communities to deliver comprehensive health services across care settings.” 3
As Learning Consultants at Island Health, between the fall of 2018 and into 2021, we led the orientation of six Urgent Primary Care Centres (UPCCs). In response to the COVID-19 pandemic restrictions, we translated the two-week, in-person orientation to a self-directed on-line course, webinars, and either virtual or on-site simulation depending on the restrictions at the time. In addition to this course, we facilitated eight clinical and five leader (operational and corporate) workshops specifically on TBC, provided informal TBC coaching as opportunities arose, and provided consultation services to two Primary Care Network orientations. Eight-seven participants attended the clinical workshops and over 60 participants attended the leader workshops. Attendees at our clinical workshops included medical, nursing, allied health, and administrative staff. The leadership workshops focused on the operational leaders and their corporate supports (eg, project managers, professional practice consultants, and informaticists).
To improve this TBC work, we leveraged an insider, action-oriented approach to systematically lead practice changes and build our expertise in TBC implementation.5-11 Action research uses iterative cycles of look-think-act to structure engaged, evidence-informed improvement.9-11 After our first two orientations in 2018/19, we organized these experiences into a TBC framework. We structured the framework using a learning and performance perspective that detailed five steps a team and their leaders must work through to acquire and optimize TBC skills. Over the next orientations, we engaged with our corporate partners to create a team-based approach to facilitate the orientation and shifted the focus from training for TBC to training for a person-centred approach. We conceptualized Person-Centred Care (PCC)5,6,12,13 as a person seeking wellness, which is embodied relationally within a TBC ecosystem (a complex system of individuals and organizations). This conceptualization evolved our TBC approach from developing interprofessional competencies to the holistic development of teams to be adaptable, build relationships, engage with their community, promote wellness and prevent chronic diseases, develop and adhere to standards of care, and provide equitable care from birth to death. 14 This work was supported by participating in TBC working groups, reviewing the literature, and attending relevant conferences webinars.
Inspired by the work of Helen Bevan and Goran Henriks’ application of complexity science to change, 15 we identified their concepts of transformational change in our TBC work. This led to the realization that our TBC framework was not a series of steps, but a process of alignment and realignment. Bevan and Henriks describe their approach as rules that can align people with a simple set of easily understood parameters. 15 However, both authors work in a perspective of influence versus authority and we were uncomfortable with the word rules and its command-and-control connotation. Therefore, we chose to use intentions to reflect an alignment to a human-centred approach to learning and unlearning.
Intentions recommended to achieve the goal of person-centred care (PCC) within a team-based care (TBC) ecosystem.
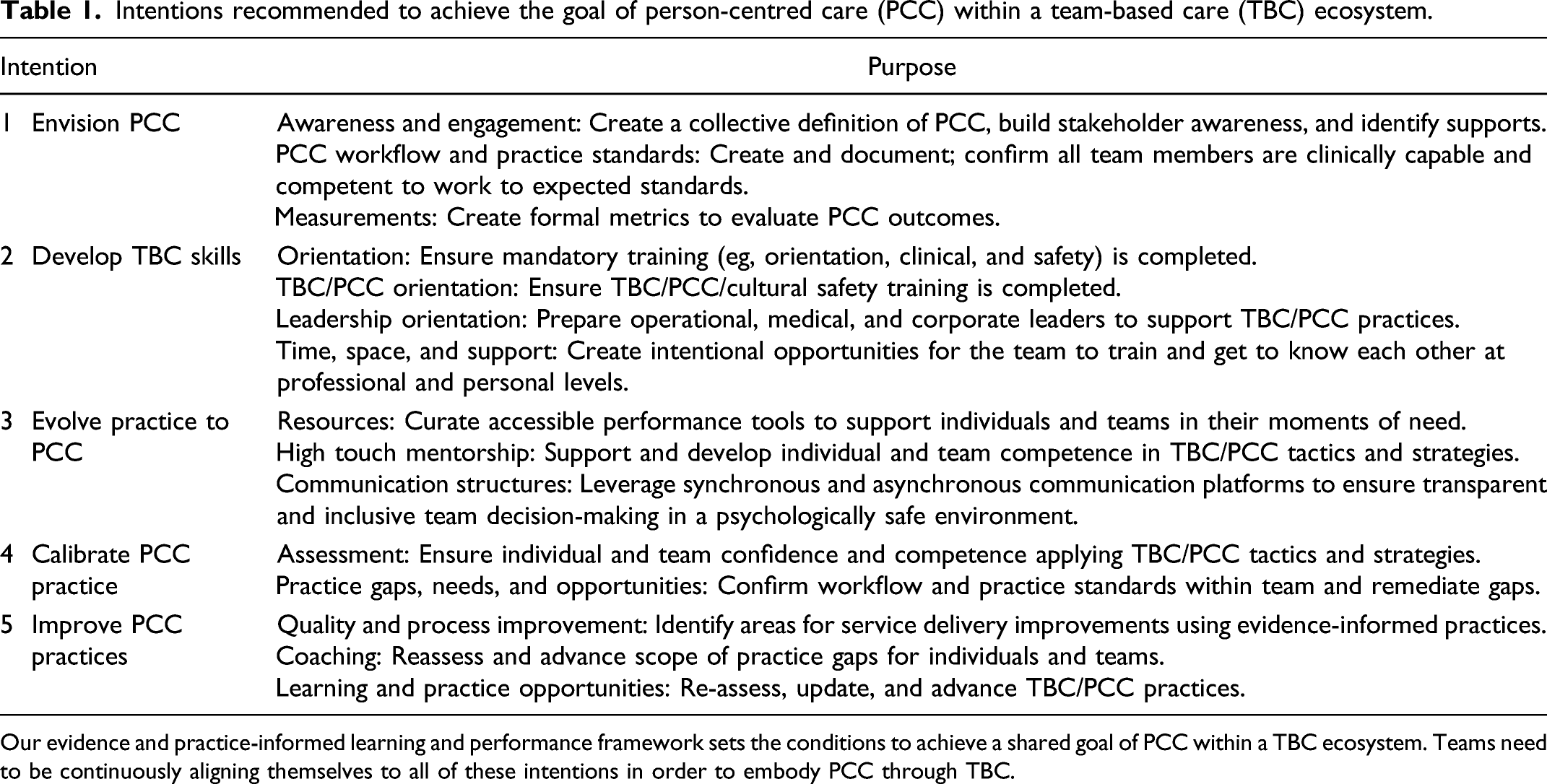
Our evidence and practice-informed learning and performance framework sets the conditions to achieve a shared goal of PCC within a TBC ecosystem. Teams need to be continuously aligning themselves to all of these intentions in order to embody PCC through TBC.
Intention 1: Envision PCC
Foundational to functioning ecosystems are the shared goals of individuals and organizations. Bevan and Henriks describe the importance of identifying a group’s guiding light, which in turn enables the members to move coherently together and in the same direction. 16 Despite the numerous TBC definitions available, the team must actively define and agree on the meaning of their TBC definition and co-create a shared vision for PCC.
With an ecosystem approach, the first step to envisioning PCC is to identify who belongs on the team (the boundaries or containers of the TBC ecosystem). We defined the primary care team to include the entire clinical, administrative, and leadership personnel providing services from the medical clinic. We defined the PCC team to include the public member and their carers accessing the services of the primary care team and other community service providers/resources. Corporate leaders involved in creating TBC structures and spaces (eg, executives, project managers, facility designers, professional practice consultants, and Indigenous wellness advisors) were identified as the teams critical to supporting the ecosystem. We addressed some of the logistical challenges of bringing together a diverse group of stakeholders by thoroughly mapping our TBC ecosystem (see Figure 1) and identifying formal and informal methods to bring stakeholders together, ensuring equitable (note that we are not saying equal) participation and maximum transparency of decisions made. This approach facilitated engagement of upstream decision-makers with their downstream effects.
15
TBC Ecosystem. We define ecosystems as a complex network of interacting persons, organizations and agencies, and their environment. This figure represents some of the interactions of the many individuals and organizations in the TBC ecosystem, forming its complex relationship matrix. This figure is not exhaustive and does not contain other important elements of the ecosystem, such as the social determinants of health, the various cultures and sub-cultures among the groups, values, and beliefs systems, as well as the infrastructures (eg, physical and psychological spaces and electronic health records), processes (eg, care pathways and workflows), and mechanisms (eg, policies and incentives). In practice, we imagine our TBC ecosystem like a matryoshka doll with the person seeking wellness at the centre. Wrapped around that person supporting them are the primary care team and community resources. Wrapped around the primary care team supporting them are corporate and governance supports.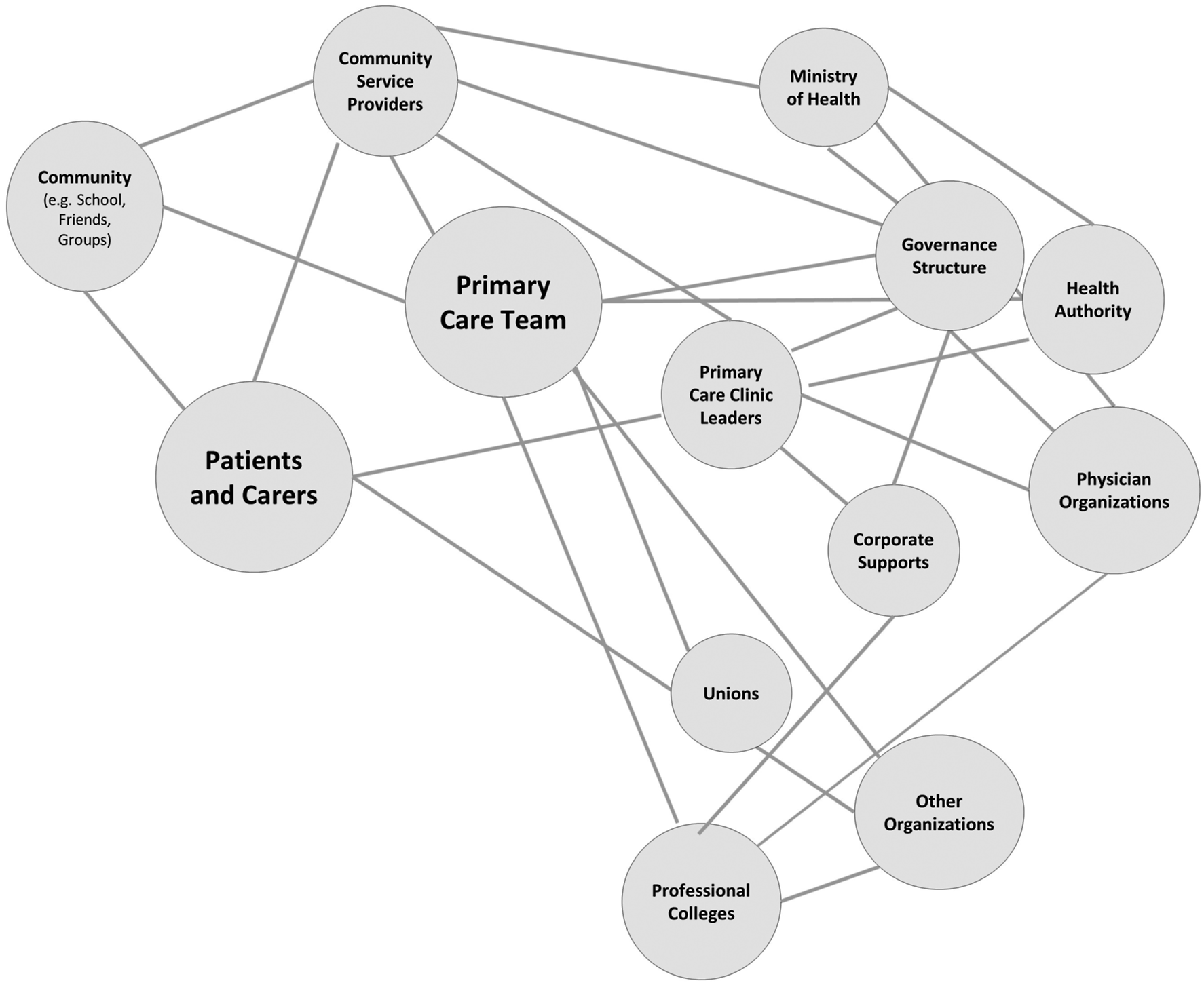
Complexity thinking tells us that envisioning PCC will not be a linear process because it reflects the diverse perspectives of various systems (see Figure 1).5,16 But it is an important activity because it supports the development of an agreed upon governance structure that will “meaningfully measur[e] the provision of patient-centred team-based care.”14 (p.13) Formal measurements, that are aligned with desired outcomes, will promote team adaptability to meet the demands of PCC. 17 These measurements can include health outcomes (eg, reduction in medications, emergency department visits, screening, and follow-up activities), stakeholder satisfaction (eg, services provided, wait times, appropriateness of referrals, and staff retention), and organizational measures (eg, engagement and quality improvement activities, financial health, and information management). Efforts must be made to ensure it is meaningful across stakeholders and hierarchies and can foster improvements and change through frontline ownership. 17
Intention 2: Develop TBC skills
As facilitators, our support is focused on providing foundational TBC training and training on the related, but essential, concepts that support PCC.14,18,19 We have been fortunate to be included at the onset of project planning and to be allotted dedicated orientation time. We structured the orientation to provide essential clinical, safety, and team-based care training. We leverage UBC’s TBC on the Run, 20 which is based on the Canadian Interprofessional Health Collaborative (CIHC) National Interprofessional Competency Framework 21 as foundational training, provide self-directed learning, and deliver customized workshops. While feedback has been overwhelming positive and comments indicate that attendees are eager to implement TBC and PCC, we recognize that implementing these practices is challenging. Working in complexity requires embodying new mental models, which cannot be achieved by just taking a course.6-8,13,17 Without new mental models, we have witnessed primary care clinical and leadership teams devolving to traditional practices such as triaging all visits through a physician and assigning patients to panels based on their medical history.
When we looked to the literature, Schottenfeld et al. suggested the goal of TBC training should not follow a competency approach but instead focus on building teams who can work together in egalitarian ways and communicate as a single entity. 18 They suggest, along with others, that TBC training should emphasize information sharing practices, build team flexibility, and normalize the concept that patients are team members. Therefore, we evolved most of the orientation training from role-based towards team-based training and adjusted the focus to building professional adaptability and connecting the team to each other and to their TBC ecosystem of corporate supports and community resources.8,17,18,22 We have learned that for teams to adapt and flex their professional roles in response to a person’s care needs and to share accountability for that care across a team, their work must be anchored to standards of care.17,19,23
Our orientation training now uses interdisciplinary facilitation techniques. We also evolved the training from a single event at orientation to a multi-prong approach that includes TBC workshops for leaders and their corporate supports and post-training resources. Our most recent work has been focused on fostering an adaptive space for leadership development to sustain practice change in non-hierarchical ways.7,17,24 Our TBC training continues to be a moving target and in our next iterations, we hope to improve physician engagement with the training and include community members (aka patients).
Intention 3: Evolve practice to PCC
Once the foundational training is complete, the primary care team must apply this learning and implement TBC practices to support PCC as a team and as individual professionals. Mental models of service delivery and practices of standardization must evolve to the provision of PCC, which emphasizes equity, wellness, and collaboration within a TBC ecosystem.5,6,13,17 This evolution, which we see as a significant directional change away from transactional care delivery, requires the embodiment of risk as a shared responsibility and relationships as key to healing.25,26 The structures that support standardized care (eg, workflows, algorithms, role clarity, and fee-for-service) need to be replaced with care pathways that optimize roles. As Tuckman and others identified, we are finding that any mental models that run counter to the principles of TBC and PCC will now surface and will require renewed attention.27,28 Therefore, local leaders play a critical role in shepherding practice change and must ensure a psychologically safe space for the team and stakeholders to reflect, negotiate, develop, adjust, and finesse the contradictions and tensions of this evolution.7,15,17,24,29
As TBC facilitators, we have emphasized to leaders and team members that clear parameters for communication need to be proactively set that support this negotiation while also supporting positive team formation. Check-ins and actioned responses are the foundation of an adaptable and culturally safe TBC ecosystem. Check-ins create a safe space because they enquire whether colleagues felt heard in the conversation and whether there is agreement on the current approach. Actioned responses are the in-the-moment adaptations, which indicate that the team is listening and willing to adapt. 22 They are practiced during structured team reports, warm handovers, daily huddles, and ad hoc case conferencing.19,30,31 Written communication channels (eg, visual boards, charting or electronic medical records, protocols, order sets, and meeting minutes) can also be included to support meaningful, asynchronous participation in decisions. When done well, this activity will create a sense of belonging among all team members and the communication techniques can be applied to improve PCC.
For individuals who need more support in adopting these practice shifts, coaching, buddy shifts, and deliberate training opportunities need to be made available. 32 For teams that desire improved functioning, we have been invited to facilitate activities and have used a variety of facilitation techniques that also support team building, including simulation, 33 Primary and Community Care (PACC) Mapping, 34 Liberating Structures, 35 Appreciative Inquiry, 36 and Process Mapping. 37 We have also recommended cultural improvement training from British Columbia’s Patient Safety & Quality Council (BCPSQC) 38 and activities that make time and space for the team to just have fun together. Leaders and organizers must be intentional about ensuring the physical space comfortably supports the activity. When appropriate, primary care teams can also intentionally expand the boundaries of their physical clinic walls and invite their TBC ecosystem (eg, community members, service providers, corporate supports, and governance members) to join their conversations.
Intention 4: Calibrate PCC practice
Once the team has had time to negotiate and practice, sometime between three and six months, we recommend planning a formal check-in. It is critical to seek meaningful internal and external feedback to ensure care delivery is calibrated to the expected practices and outcomes conceived prior to implementation (the PCC vision) as well as intentionally evolve practices and resources to address any opportunities or issues.7,17 Benchmarking care delivery is important because strong team dynamics can result in groupthink and hide blind spots and biases, which can derail the adoption of TBC and PCC. We recommended formal measurements be collected by the governance structure described in our first intention. At the clinic level, context-rich metrics can also be collected that can be used to locally calibrate and improve practices.
At the local level, stakeholders, community members, and team members will often have in-the-moment and anecdotal feedback on satisfaction. This informal feedback can be formally collected for analysis. 19 Quantitative data can be extracted from electronic charts and correlated with qualitative satisfaction data. Compliance with TBC and practice standards can be monitored through chart audits and skill testing. The team can also address practices that are overly complex, inefficient, fragmented, or underdeveloped and the effectiveness of communication and support structures. One of the strongest measures of success is patient and staff satisfaction with PCC practices. Other measures may be less obvious—such as implementing new hiring practices aligned with the team-based, person-centred care model. 14 Every three to six months, sufficient data should be available for analysis and action. Whatever data are collected, efforts must be made to ensure that it can be translated into a format that is timely and useful for actioning change.8,17
Intention 5: Improve PCC practices
We believe that as TBC facilitators, a measure of our success is when the team takes full ownership of their PCC practices. 19 Therefore, this intention supports continuous quality improvement and the building of a learning culture.8,11,39 Activities in this intention include the more complex, TBC ecosystem opportunities and issues like service and infrastructure gaps, scope of practice optimization, team composition, team dynamics, and so on.19,22,26
Although foundational training in these areas is widely available, teams must often identify novel opportunities to advance their practices. As mentioned earlier, some organizations like the BCPSQC, 38 professional organizations,40,41 or the Institute for Healthcare Improvement 42 may provide advanced supports. When advance supports are not available, creative activities like site visits, community engagement, conferences, and engaged action research could be leveraged. Access to an experienced TBC facilitator could also provide customized consultation services. 24 Presenting and publishing these activities are also important contributions to the body of knowledge on TBC and PCC.
Conclusion
PCC embodied relationally within a complex system, or ecosystem of individuals and organizations, requires multi-faceted nurturing to sustain. Our five intentions are the result of iterative, action-oriented research across multiple TBC implementations using a learning and performance perspective. As we attended to parts of the ecosystem, we also acknowledge the various leaders and teams who also engaged in parallel with local activities that directly supported TBC implementation in other ways. Achieving the Quadruple Aim through team-based care requires the replacement of traditional practices with complexity models that support PCC. From this viewpoint, TBC training is not an event for primary care teams but a process of building a shared goal of PCC within a TBC ecosystem.