
Abstract
As more people became infected with the SARS-CoV-2 virus, it was anticipated that 10-20% of these individuals would develop a post-viral illness that would affect their ability to work and participate in daily activities and reduce quality of life. To support these patients, Unity Health Toronto opened the Outpatient Post-COVID Condition Rehabilitation Program in June 2021, with the aim of teaching patients how to manage their ongoing symptoms, and to maximize their independence and function. The program incorporated a multidisciplinary, patient-centred approach that leveraged group education and a virtual platform to allow patients from across Ontario to learn from one another and share experiences. Over the two years of the program, the multidisciplinary team continuously adapted to the new research on Long COVID and evolving needs of patients. This article will outline the development and evolution of the program.
Background
As more people became infected with SARS-CoV-2 in 2020, many in the scientific community predicted a second pandemic of post-viral illnesses.1,2 Unity Health Toronto, a network of two acute care and one post-acute rehabilitation hospitals, recognized the need for post-COVID-19 rehabilitation and expanded services to assist patients with a post-COVID condition, commonly known as Long COVID (LC), transition to independence at home. In May 2021, Unity Health drafted a briefing note to Ontario Health outlining the rationale for an Outpatient Post-COVID-19 Condition Rehabilitation Program, citing evidence that persistent post-COVID symptoms were impacting individuals’ health, functioning, and finances. 3 At that time, the National Institute for Health and Care Research in the United States stated that in the absence of research guiding LC-specific treatments, interventions should draw from “expert consensus and evidence from other conditions.” 4 New York’s Mount Sinai Health System opened the first multidisciplinary post-COVID centre just months into the pandemic, 5 but in early 2021, there were few hospital-based LC rehabilitation programs in Canada open to external referrals. Internationally, the Leeds Teaching Hospitals NHS Trust developed a multidisciplinary rehabilitation pathway that incorporated in-person and virtual care. 6 The Unity Health proposal drew from available guidance and existing models.
Based on Unity Health’s Intensive Care Unit (ICU) admissions and international statistics regarding individuals most susceptible to severe COVID-19 infections,7,8 the expectation was that most patients needing rehabilitation would be older adults who had required hospitalization. The initial program model did not meet patients’ needs because (1) the majority were working age and had experienced only mild or moderate acute infections, (2) high referrals to the program led to long waits for service, and (3) traditional progressive rehabilitation did not adequately address the multisystem, chronic, episodic nature of the condition. The present article describes the program’s two-year evolution from a traditional progressive rehabilitation model to one emphasizing self-management and based in a group therapeutic education framework. We will highlight lessons learned and provide recommendations for future program planning, research and advocacy.
Program Model #1
The Unity Health Outpatient Post-COVID Condition Rehabilitation Program opened to physician referrals in June 2021, with no catchment area
The program accepted patients experiencing new or persisting symptoms more than 8 weeks after presumed or confirmed COVID-19 infection and not attributable to another cause. The allied health team included full-time Occupational Therapy (OT), Physiotherapy (PT), and Social Work (SW), and part-time (.4) Registered Dietician (RD) and (.6) Speech-Language Pathology (SLP). Physiatry (MD) was available for consults and could refer outside the program to other medical specialities (e.g., neurology, cardiology, and psychiatry). A Patient Flow Coordinator (PFC) reviewed and triaged referrals. Community Health Navigators (CHNs) collected Patient-Reported Outcome Measures (PROMs) by telephone at intake, discharge, and 6 months post-discharge, supported by a Research Assistant. Standardized PROMs rated fatigue (Functional Assessment of Chronic Illness Therapy (FACIT-4) – Fatigue Scale) 9 ; functional status (Post-COVID Functional Status Scale – PCFS) 10 ; physical and mental health-related quality of life (EQ5D - 5L) 11 ; and self-efficacy in chronic illness (PROMIS - Self-Efficacy). 12
Patients completed four weekly one-hour virtual group education modules on managing common physical, cognitive, and emotional symptoms of LC. All patients were assessed by OT and PT. Internal referrals for SLP, RD, and SW could be made by team members based on identified needs (e.g., mood, cognitive communication, and nutrition). Clinicians could refer to the program MD or suggest a specialist referral to a patient’s Primary Care Practitioner (PCP)
Outcomes of Program Model #1
In January 2022, program staff met to review the model in response to data collected and to patient and clinician experiences. Three key themes emerged:
Referral numbers and demographics
In the first 6 months, the program received an average of 30 referrals per month from within and outside the Greater Toronto Area. This suggested insufficient rehabilitation options for patients in outlying communities
Evolving understanding of LC
At intake
Consistent with information shared in the scientific and patient communities at that time, 14 patients reported receiving new diagnoses or exacerbations of pre-existing conditions including dysautonomia, migraines, asthma, diabetes, and autoimmune disorders. Many reported an episodic pattern of Post-Exertional Symptom Exacerbation (PESE): severe fatigue and worsening of other symptoms with physical, cognitive, or emotional exertion, similar to Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). 15 Clinicians noted that assessment or treatment sessions sometimes triggered episodes of PESE.
The evolving scientific literature and patients’ experiences categorized LC as a chronic illness, with fluctuating symptoms and severity consistent with other episodic and post-viral illnesses such as ME/CFS. 16 In this context, clinicians, patients, and PCPs initially had unrealistic expectations for complete rehabilitation and recovery, making discharge more challenging.
Program and system gaps
The usual model of care, with the PCP coordinating recommendations from medical specialists, often did not meet the needs of patients with LC, a condition in which one symptom might represent a dysfunction in more than one system (e.g., cardiac, respiratory, and immune). 17 Few specialists had experience with LC at that time, and waitlists were lengthy and patients were often sent back to their PCP with normal test results and little to suggest other than to exercise their way back to health, a recommendation with the potential to cause harm for those with PESE. 18 Understandably, PCPs and patients often expected the program to provide specialized medical care and case coordination. Many patients’ complex concerns were outside the scope of the allied health team. Patients felt validated by meeting others with this new condition during the introductory modules and suggested including formal peer support.
Because of patients’ relatively young age, they frequently required documentation for medical or disability leave, income support programs, and employment or academic accommodations. Many insurers and employers expressed disbelief in the medical basis for symptoms. This was a significant source of stress and fatigue for patients, and clinicians invested time and effort to provide evidence-based documentation.
Program Model #2
Comparative summary of program models.
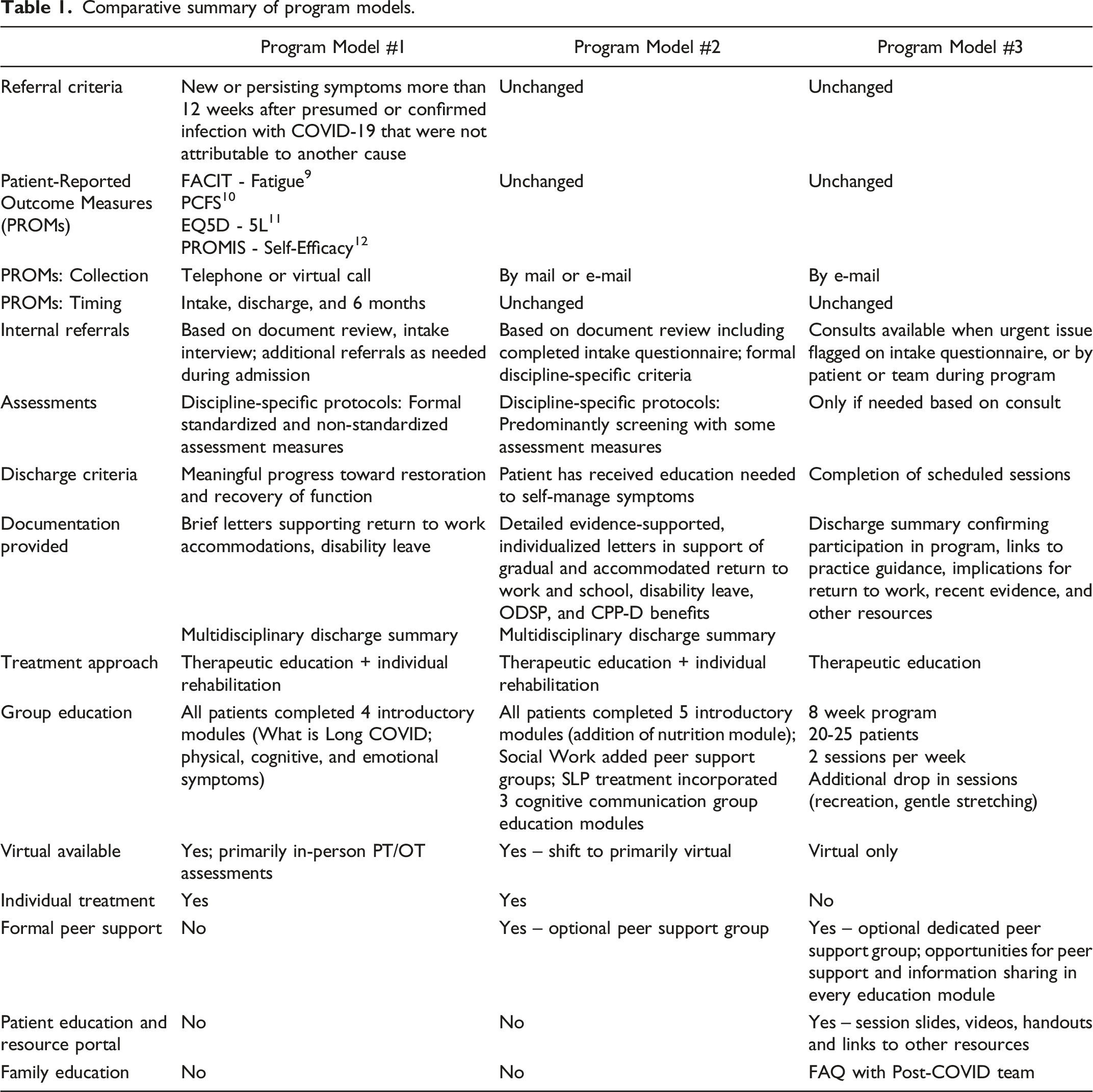
Program Model #2 was implemented in April 2022. Rehabilitation goals and discharge criteria were explicitly aligned with chronic illness self-management and stabilization of symptoms rather than targeting a return to baseline. To set realistic expectations for patients and referring physicians, the referral form outlined program goals, resources, and discharge criteria. Most sessions shifted to virtual care to accommodate patients living outside the local area, those with work or childcare obligations and those who needed to minimize the risk of PESE. To ensure appropriate, timely internal referrals, patients completed intake questionnaires that included discipline-specific referral criteria. Collecting PROMs via e-mail prior to starting the program reduced the resources required for CHN calls.
The introductory group education modules were updated to reflect new research. Patients could access a limited number of 1:1 consultations with clinicians, and SW and SLP groups provided peer support and more efficient information delivery. Individual sessions were offered by telephone for patients without internet access or unable to tolerate the sensory load of virtual sessions.
All disciplines emphasized self-management (e.g., compensatory cognitive strategies). Goals included increased stabilization of symptoms, function, and health self-efficacy, a sense of control which for those with chronic illness correlates with improved physical and emotional well-being and quality of life.19,20 The team screened patients for patterns of PESE and followed ME/CFS recommendations centred on pacing and energy conservation strategies rather than graded exercise therapy.
Letters for PCPs, insurers, and income support included patient-specific recommendations, education about LC as a chronic episodic illness, and links to evidence and resources. To increase community expertise, team members presented on LC and the program to the local community health network, provincial Legal Aid clinics, and physician and allied health professional groups. The program collaborated with a community organization offering virtual peer support to patients after discharge.
Outcomes of Program Model #2
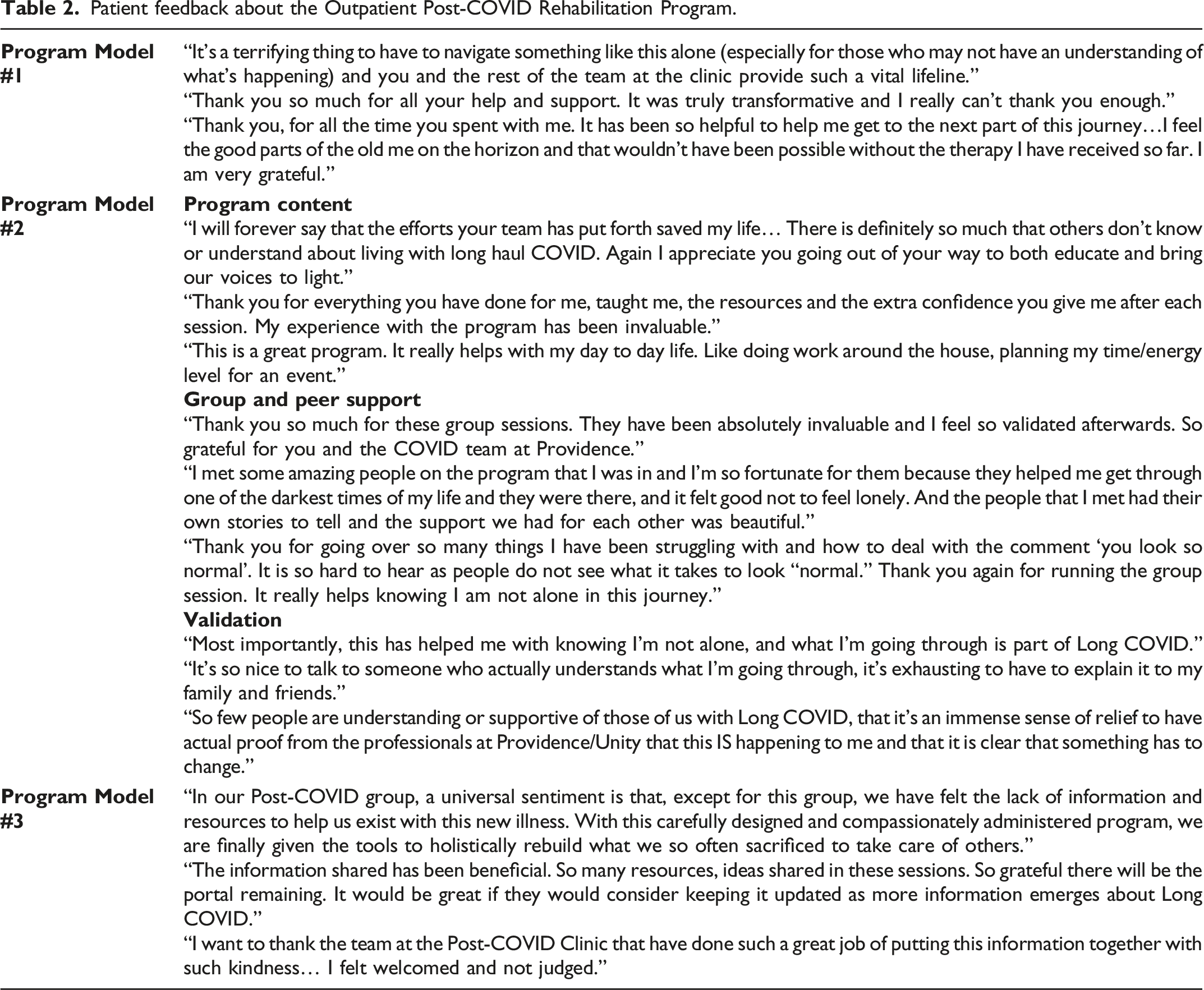
Patient feedback about the Outpatient Post-COVID Rehabilitation Program.
Few reported complete recovery. On admission, 74% of patients identified return to work/school as a goal; available discharge data indicated that 26% reported returning on at least an accommodated basis. Return to leisure was a goal for 94% of patients; by discharge 37% had resumed leisure activities to some degree.
The primary factor leading to a second, more radical, program revision was continued high demand, with up to 200 patients accepted and waiting for service for 12-20 weeks despite the initial program changes.
Program Model #3
The program team collaborated on the second revision, which again benefited from Unity Health patient and clinician experiences, as well as information shared by clinics providing LC services internationally. While guidance around targeted treatment remained incomplete, there was early evidence in the LC literature for peer support. 21 Given expanded scientific knowledge of the chronicity of LC, the team drew on evidence supporting a group therapeutic education framework for individuals with chronic illnesses,22-24 and for the use of virtual platforms for patient education. 25 Program Model #3 (Table 1), launched May 2023, was a virtual group therapeutic education program that aimed to address wait times as well as other themes identified earlier, while meeting the key rehabilitation goals: increasing self-efficacy, stabilizing symptoms, and improving function.
Referral sources and patients were clearly informed regarding the program format and that the PCP would continue to be responsible for care. Two cohorts of 20 to 25 patients could be admitted each week, to a maximum of eight cohorts running concurrently.
Outline of virtual group education sessions in Program Model #3.

aSessions on dysautonomia/POTS, breathing not offered as program had no PT at this time.
bOriginal four introductory education sessions.
Patients could use a secure e-mail address to share questions or feedback not easily addressed in a group setting. If a concern was identified during intake, a group session, or via e-mail, a consult with one of the clinicians was offered. The general discharge letter included a program description, LC education, and links to reliable sources of physician guidance, evidence, and return to work resources. Patients could share this with employers and insurers as needed. In response to patients’ suggestions, the portal was made publicly searchable to allow community access to program resources (https://unityhealth.to/patients-and-visitors/covid-19/outpatient-post-covid-condition-resources/).
Outcomes of Program Model #3 and program closure
Again, without allocated resources to prompt completion of repeat PROMs, there was limited outcome data; however, patient feedback regarding the program and the portal was largely positive (Table 2). The group therapeutic education model was in place for only three months before funding lapsed.
Lessons learned
A total of 844 patients were served by the Unity Health program. Two years of program planning, implementation, and revision provided important lessons that can be applied to future programs and clinical research for individuals with LC or similar chronic and episodic conditions.
Virtual group platform and peer support
Utilizing a virtual group model made the program more accessible to patients who were working, providing care at home, outside Toronto or too debilitated to attend in-person. Chronic conditions are often misunderstood and isolating, 26 but patients found support in the groups and learned from peers’ lived experiences. The patient portal allowed patients to review session information and to share with care partners and Healthcare Providers (HCPs).
Validation
The importance of validation was a repeated theme across the life of the program. Patients described the burden of having their symptoms and experiences dismissed by family, friends, and HCPs. As evidence for the pathophysiological mechanisms underlying LC accumulates, this is a reminder to HCPs of the inadequacy of care that dismisses what is not yet understood.
Patients are the experts of their illness
At a time when little was known about LC, the team came to understand the breadth and severity of the illness through interactions with patients. Collaboration between patients and clinicians led to program revisions that improved care and honoured the patients’ experiences.
Advocacy
The program provided self-advocacy tools, but the severity of LC symptoms makes it unrealistic for patients to persevere with these tasks alone. There remains limited awareness of chronic and episodic disabilities in the insurance and vocational rehabilitation fields. Some individuals are refused leave and suffer severe health and quality of life impacts; others who remain off work could return if given accommodated schedules or responsibilities. Inadequate social and income supports can result in food, housing, and financial insecurity. A new condition like LC demands advocacy in the community, government, healthcare and public and private insurance systems to support patients’ ongoing care, participation in work and family, and quality of life.
Impact on program staff
Staff were impacted by factors affecting all those providing healthcare during the COVID-19 pandemic. In addition, there were emotional burdens associated with working with individuals diagnosed with a new condition, facing threats to employment, finances, and relationships. The program closure was a source of moral distress for the staff. Countering these burdens were the meaningful inclusion of staff in program revisions; clear, honest, and timely communication from managers; ongoing positive feedback from patients; and daily opportunities for team collaboration and support.
Program and system gaps
The final program model could not address all the complex medical, mental health and social support challenges, or fulfil requests for individualized documentation. It was challenging for facilitators to monitor the emotional well-being of patients as some did not comment during sessions. Adequately funded programs should provide meaningful peer support and therapeutic education, but be able to address individuals’ complex medical needs, mental health concerns, or threats to food and housing security. Offering the recorded modules and program materials on the portal may have increased access for shift workers or those with precarious work, but future programs should consider flexible scheduling options. Providing service and materials in multiple languages would further increase access.
System wide, improved access to speciality LC care and medical specialists is needed; at present, the onus is on PCPs and walk-in clinics to coordinate complex care, educate patients, and provide detailed documentation for employers and insurers.
Finally, there were insufficient resources to pursue the outcome data necessary to support the need for and benefits of LC care.
Research opportunities
Research into the pathophysiology and multisystem impacts of LC will hopefully lead to targeted treatments and medications; in the meantime, there are opportunities to evaluate rehabilitation approaches to the impairments and devastating functional impacts of LC. The present paper describes the unexpected evolution of a rehabilitation program rather than outcomes of clinical research, but lays groundwork to prospectively study the effectiveness and feasibility of model components, for example, the optimal balance of virtual and in-person care or of individual and group intervention. Future clinical research should also evaluate interventions beneficial in other illnesses that target individual symptoms such as PESE, shortness of breath, and brain fog.
Conclusion
Beginning in 2021 when little was known about LC rehabilitation, the Unity Health program team adapted care by incorporating patient and clinician experiences and evidence from the LC and chronic disease literature. The final program model, a virtual group therapeutic education series, accommodated high referrals while providing peer support and symptom self-management strategies. Continued advocacy is needed to address multiple persisting gaps in healthcare, insurance, social support, and vocational rehabilitation systems.
Footnotes
Acknowledgements
This program was a collaboration between the remarkable patients who shared their experiences, and a resilient and compassionate team of professionals: Kelly Tough, OT Reg.(Ont.); Dr. Albert Cheng, MD, FRCPC; Dr. Ashley Verduyn, MD, FRCPC; Lori Brady, PT, MSc, PT, MHSc, CHE, PMP; Aruba Adnan, BSc, Cassandra Chan, RD; Leigh Ann Gray; Erin Leneeuw, BA; Christina Lee, BSc, PT; Nicole Luinenburg, RD, Monica McCullagh, BA (Hons); Irene Nicolakis, MSc, PT; and Dione Romero, MSW, RSW.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional Review Board approval was not required.