
Abstract
This article discusses the treatment of enslaved Africans by the Dutch during the seventeenth and eighteenth centuries. Treatment is interpreted in two ways – morally and medically. Moral treatment is primarily defined by the Dutch Reformed Church and its religious dogmata. Despite the importance of this church in the provision of pastors and comforters of the sick (ziekentroosters), information about its role in providing a religious, moral compass to its members regarding slavery and slave trade is scattered. Medical treatment – both preventive and curative in nature – is discussed as well. The slaves were subjected to abominable living conditions prior to their departure. Although it seems fair to state that these conditions did not improve while sailing westward, for various reasons preventive and curative medical measures were taken by ships' surgeons – and to a lesser extent by comforters of the sick.
The Dutch played a key role in the horrors of the transatlantic slave trade during the seventeenth and eighteenth centuries. The Dutch West India Company (WIC) was one of the major actors in this drama, but there were also private slave ships. Africans were captured in West and Central Africa and brought over to the slave ports controlled by the WIC or European rivals on Africa's west coast. However, the WIC and its European rivals did not control most West African slave ports, only some places at the Gold Coast. From there, enslaved Africans were exported to the New World with the prospect of being enslaved on the various plantations.
This article focuses on the preventive and curative medical treatment of the enslaved Africans traded by the Dutch during the seventeenth and eighteenth centuries. 1 The main question this article addresses is: how did the Dutch medically and morally treat the slaves before, during and after their journey to the American colonies?
We will discuss three phases in chronological order. The first phase comprises the slaves’ lives from the moment of capture until their embarkation on the ships in the West African slave ports setting sail for the New World. The second phase is the so-called ‘middle passage’, the transatlantic voyage from the West African slave ports to the New World. In examining the third phase we will review the slaves’ physical conditions and medical treatment upon their arrival in the colonies and during their deployment on the plantations. We conclude the article with a case study of how slaves were treated – including their medical treatment – in Suriname.
Phase one: Hunting, imprisonment and transport
Between the fifteenth and nineteenth centuries approximately 12–12.5 million African people were enslaved in Africa and subsequently purchased by European slave traders, the vast majority of whom were transported across the Atlantic Ocean to the New World. 2 This enormous supply of enslaved Africans originated from various sources. Some were previously enslaved by local African slaveholders. Others were enslaved by the domestic judicial systems as a punishment for criminal activities, or as a manner of compensation for being insolvent debtors. Another, smaller-scale source of capturing slaves was kidnapping. However, most of the enslaved transported by Europeans were prisoners of war. 3
The enslavement of prisoners of war was dominated by the political and military leaders of African societies, often located deep in the African interior. British pioneer Edward James Glave visited a few of these African societies in the late nineteenth century. In his study, published in 1892, he describes the sight of the slaves who were waiting to be sold to African slave traders: At every village bands of slaves were offered for sale; it would be difficult to give a truthful picture of the suffering endured by the captives in this region. (…) Others sit from day to day with their legs and arms maintained in a fixed position by rudely constructed stocks, and each slave is secured to the roof-posts by a cord knotted to a cane ring which either encircles his neck or is intertwined with his wooly [sic] hair. Many die of pure starvation, as the owners give them barely enough food to exist upon, and even grudge them that. These hungry creatures form indeed a truly pitiable sight (…).
4
Glave's journal dates from a period when Europeans were no longer massively involved in the transatlantic slave trade. Be this as it may, the author provides a distressing description of the treatment of slaves in the villages of their captors. Most slaves in African communities were used for domestic purposes and had a sort of family life with their communities. 5 The position of captives who were sold as slaves to European traders was quite different. According to Glave, the enslaved were locked in chains for days without any food. In combination with diseases like yellow fever, malaria and cholera, their living conditions in the tropical weather of Central and West Africa must have been horrific.
After purchasing the enslaved in the African villages, slave merchants transported them over long distances from the inland villages to the slave auctions or markets located on a part of the West African coast between the Volta River and Benin: the Slave Coast. Most slaves, were bought at the Loango Coast. These long distances were mostly covered on foot. It has been estimated that a typical coffle of slaves would spend eight hours on the road daily, covering roughly 20 miles. It often took months to reach coastal cities like Offra, Ouidah or Jaquin(m) (Figure 1).

An illustration of a coffle, a line of chained slaves making their way to the coast.
![https://chnm.gmu.edu/cyh/archive/fullsize/slave-coffle,-central-africa,-1861-[image]_6a0ca85048.jpg](https://chnm.gmu.edu/cyh/archive/fullsize/slave-coffle,-central-africa,-1861-[image]_6a0ca85048.jpg){kind=link}
Notwithstanding these poor conditions, slave raiders had strong incentives for getting the slaves to the slave markets fast and in the best shape possible. This did not, however, prove an easy task in the tropical regions where lethal diseases were endemic, as were starvation and assault on the slave caravans.
6
Not surprisingly, British Royal African Company agents in early eighteenth-century reports refer to ‘on-the-road slave burial sites’.
7
An eyewitness report provided by one Major William Gray depicts an overall image of the horrors that must have been evident on these journeys through the African inlands. The report unequivocally refers to the dehydration, exhaustion and heat prostration the enslaved were exposed to. Considering the likelihood of a lack of medical aid, one can imagine these travels were a recipe for death and despair. In Gray's words: The men were tied in pairs by the necks, their hands secured behind their backs; the women by their necks only, but their hands were not left free from any sense of feeling for them, but in order to enable them to balance the immense loads of pang, corn or rice which they were forced to carry on their heads. (…) They were hurried along at a pace little short of running. (…) Many of the women were old, and by no means able to endure such treatment.
8
Unlike the WIC, local slave raiders commonly implementing these journeys did not usually keep official or trustworthy records of, for instance, mortality rates among the slaves during these transports over land. Because of the lack of such documentation, little is known about the details of these journeys or the number of enslaved that succumbed before arriving at the coast. 9 Nonetheless, according to Anderson, it is likely that ‘mortality and sickness rates were highest during this first stage of the journey’. 10
The WIC operated almost the entire African West Coast, from the Tropic of Cancer to Luanda (Figure 2). On behalf of the States General in the Dutch Republic and to the benefit of Johan Maurits van Nassau-Siegen (1604–1679), Governor of Dutch Brazil between 1636 and 1644, Michiel Adriaanszoon de Ruyter (1607–1676) captured the fort St. George in Elmina in 1637 and renamed the stronghold Elmina. It is believed that the name ‘Elmina’ derives from the Portuguese Mina de Ouro or gold mine. Elmina became the strongest fortification in West Africa and remained under Dutch rule until 1872. In 1655, De Ruyter recaptured from the English some other Dutch forts, on Goree Islands and some forts at the Gold Coast, but not Elmina. These forts had previously been taken from the Dutch by the English Admiral Robert Holmes. 11 Elmina was notorious for being the WIC's main operating centre in the region. 12 The town of Elmina was founded approximately 700 years ago. The Portuguese first arrived in 1471, trading their gold for salt. In 1482, they began building a fort, St. George, after obtaining permission from the local king, King Caramansa (also known as Kwamina Ansah). In 1637, the Dutch captured this fort. It remained under Dutch rule until 1872. Other notable WIC slave ports on the West coast of the African continent were established on the Gold Coast (current Ghana), the Slave Coast (current Nigeria) and – briefly – in Angola (Figure 3).

‘Negroland' and Guinea with the European Settlements, Explaining what belongs to England, Holland, Denmark, etc. Map published by Herman Moll in 1727.

View at Elmina by Johannes Vingboons, ca. 1670.
When the enslaved Africans arrived at the WIC slave ports their fates varied considerably. All slaves were stored like commodities, awaiting transport to the New World. The living standards during this period were largely determined by the type of accommodation they were kept in. Some were kept in barracks especially designed for the temporary confinement of slaves. These barracks were called barracoons. To reduce the risk of escape some were kept in underground facilities called truncks. Most were held in the dungeons of forts or compounds called ‘slave castles’. 13
The enslaved were separated from their loved ones upon arrival at the slave forts as men and women were housed separately. They typically stayed in these types of accommodations for a few weeks. However, in some instances it took months before they embarked on the ship that would take them to the other side of the ocean.
As most of the slaves were bought along the West African coast and then ‘stored’ in the slave ships, not in the trade castles, the conditions must have been abhorent. There were no toilet facilities available. Instead, a canal in the floor would carry away the excrement to a lower level of the floor, where it would accumulate and serve as the perfect brewing place for bacteria and viruses. As David A. Johnson states in the Historical Encyclopedia of World Slavery: ‘These festering holes were confined, hot and poorly ventilated’. 14
Many enslaved Africans fell ill with small pox and dysentery. Malaria also played a role, as it is considered to be an endemic disease in most of these coastal locations. 15 As a result, the rate of mortality among the enslaved was directly correlated with the time spent in these accommodations awaiting transatlantic transport. 16 The longer the enslaved were kept in these dungeons and truncks, the greater the chance was of an epidemic disease breaking out and claiming many lives. Even if the main purpose of these castles was to store the slaves, these ‘warehouses of Black humanity’ 17 also served the purpose of breaking the warrior spirit of the male slaves in particular, making them easier to handle by the time they boarded the ships.
Phase two: the Middle Passage
Living conditions on board
When the time had come for them to depart for the Western Colonies, the slaves were shaven and branded. The men and children were stripped of their clothes completely; the women were given a piece of cloth to protect at least part of their dignity. On board, the male slaves were chained to prevent them from attempting to escape by jumping overboard and swimming back to the shore. Usually, the crew chained two slaves together at the ankles and the wrists. 18
At night, the slaves would sometimes be chained to the ship as well as to each other. The male slaves slept on the ‘tweendeck (tussendek). 19 The women and children were separated from the men and slept at the sconce (schans). 20 The sconce was also referred to as the hoerengat (whores’ spot), from which one can infer that even though it was strictly prohibited for the captain and crew to have sexual relations with the female slaves, it happened frequently. 21
Reports vary on the size of these sleeping quarters and the available space per slave – after all, the size of the sleeping quarters was defined by the size of the ship and the number of slaves it carried. Moreover, information about the space for slaves on board WIC ships is highly speculative. Nevertheless, we may assume that the slaves were packed together very tightly, because transporting more slaves increased the chances of profit. M.A. van Andel stated that the tussendek (’tweendeck) usually had a width and length of 7.5 metres and a height of 1.5 metres and housed approximately 200 slaves, whereas the schans (sconce), which slept 150 slaves, had a width and length of 5.5 metres and a height of 2 metres. 22 Balai states that not much is known about the space per slave on Dutch slave ships, but he describes the situation on board English and Danish ships. On average, male slaves had a space of 180 by 40 cm, with a standing height of 170 centimetres. In order to carry more slaves per ship, the sleeping quarters were split into two levels, reducing the height per slave to roughly 70 cm. Slaves lived in this way for at least a month, usually two, and in extreme cases for up to four months. 23 However, sources for the WIC regarding the interior of slave ships do not exist. Most historians (including Balai) use the archives of the Middelburgsche Commercie Compagnie as a proxy.
The slave traders knew that they could not let the slaves stay in their quarters for the entire duration of the journey. Temperatures in the tussendek and schans could reach 40°C, which caused dehydration and made slaves more vulnerable to diseases. Additionally, the slaves would often be sleeping in their own excrement as it was practically impossible to reach a ‘toilet’ (which was usually just a barrel) when chained to another slave. Sometimes, slaves would even be sleeping next to a dead body – if the slave they were chained to had passed away during the night, it would not be discovered until the next morning. 24 Therefore, captains were instructed to ‘air out’ the slaves daily – weather permitting. The slaves’ shackles were removed, and they had to wash themselves with sea water and a mix of fresh water, lemon juice, brandy and palm oil. If their hair had grown out, it would be shaven off again to prevent lice and fleas. 25
In the meantime, the slaves’ quarters were rinsed with seawater and hot vinegar. In addition, the sleeping quarters were smoked out using incense and jeneverbeziën (juniper berries), or using a hot bullet placed in a pot with tar. 26 This was done to remove the bad air, which was believed to cause disease, since the slaves’ sleeping quarters were badly ventilated, if at all. The tussendek was ventilated by two hatches: the voorluik (hatch in the front) and the grootluik (big hatch), but these could only be opened if the weather allowed. The schans was usually ventilated by four very small port holes that allowed for little ventilation. 27 In his Verrichtingen (1769), ship’s surgeon David H. Gallandat lamented this lack of airflow, stating that there is nothing worse for the health than bad air and that slave traders should make it a priority to provide adequate ventilation. However, he also noted that these traders were preoccupied with earning as much money as possible. Therefore, he thought it unlikely that they would be willing to make the considerable investment required to refit the ships to improve ventilation. 28 Nonetheless, Gallandat's treatise on the treatment of slaves on board slave ships is based on his experience on slave ships from the Province of Zeeland in the second half of the eighteenth century, not from the WIC ships that stopped trading in enslaved Africans in the 1740s.
Preventive medicine
To further ensure the ‘cleanliness’ of the slaves’ quarters, the floors were scrubbed daily. Usually, the crew assigned this task to the slaves. This practice reduced the risk of infectious diseases in two ways: the ship and the slaves’ sleeping quarters would be cleaned, removing possible causes of infection, and the slaves would perform physical activities such as cleaning and repairing the ship, which were believed to protect them from falling ill, 29 as the German poet Heinrich Heine wrote in his 1854 poem ‘Das Sklavenschiff’: ‘Durch etwas Luft, Musik und Tanz Läßt sich die Krankheit heilen’. 30
Other forms of activity included singing and dancing – often songs in the slaves’ native languages. This was believed to improve both the physical and psychological well-being of the slaves, as surgeon Gallandat wrote in his ‘slavers’ guide’ Noodige verrichtingen voor de slaafhandelaren. 31 It indicates that he recognised and appreciated the psychological aspect of disease and health, in addition to the other, more physical, preventive measures. 32 It is uncertain, however, to what extent musical activities were stimulated or allowed and whether the dancing had its intended effect, as it was not uncommon for the slaves to be forced to take part in this activity, threatened by the use of the ‘cat with the nine tails’, a whip. 33
Cleaning the sleeping quarters of the slaves, providing ventilation in the sleeping quarters, ‘airing out’ the slaves and forcing them to wash can all be described as measures taken to prevent disease. In the ancient world, preventive medicine had been described by – among others – Hippocrates of Kos (c. 460 to c. 370 BC) and Galen of Pergamum (c. 129–216 AD), who both had a slightly different approach to the concept of preventive measures. Hippocrates argued that the natural environment of an organism could influence or threaten its health, focusing on the external causes of disease. Contrarily, Galen put more emphasis on the lifestyle and other ‘non-natural’ causes of disease, such as food and drink, exercising and resting, sleeping and emotions, including both external causes of disease and internal resistance to developing illness. 34
After a period of disinterest, preventive medicine enjoyed a resurgence as an academic discipline in the sixteenth century. To a somewhat lesser extent, this resurgence carried on into the seventeenth and eighteenth centuries, translating into preventive measures. Both Hippocrates’ and Galen's views of preventive medicine can be seen in these preventive measures taken by slave traders. Treatment on board WIC ships was bad in comparison with that on board private slave ships in the second half of the eighteenth century as slave mortality decreased after the 1740s.
Cleaning the environment of the slaves and smoking out the bad air is an example of limiting exposure to a bad and unhealthy environment, as described by Hippocrates, while forcing the slaves to wash themselves and perform physical activity was meant to improve health and lift the slaves’ spirits, which are both ‘non-natural’ causes of disease as described by Galen. In fact, most ‘non-natural’ causes described by Galen were addressed by the preventive measures taken on board. For example, food was an important factor for the health of both the slaves and the crew. Slaves received the same meals as the crew, consisting mainly of beans and groats. This food was issued twice per day. The beans and groats were mixed with bacon, pepper and palm oil to make the meal slightly more appealing. Three times per week the slaves would receive scheepsbeschuit (rusk; ships’ biscuit), together with some brandy and tobacco. AS perhaps the most famous manifestation of disease prevention on board ships, fresh fruit would be bought in Africa to combat scurvy, usually oranje-appelen (oranges) and limes. 35
This dietary addition was based on the findings of the British naval surgeon James Lind. In 1747, he recorded in his experiments that lemons and limes helped to prevent and cure scurvy. Six years later, in 1753, Lind published his findings in his Treatise of the Scurvy. However, it took the Admiralty until 1795 to make the issue of lemon juice on board compulsory. It is interesting to note that, despite the success of his experiments, Lind did not believe that scurvy was simply the result of a diet lacking fresh fruit. He believed that, for any disease, multiple causes could be identified – and therefore, a disease could have multiple cures as well. This opinion was not uncommon during the eighteenth century. For example, other texts from the eighteenth century acknowledged that lemons could prevent scurvy, but also suggested the use of vinegar, malt, tea and sugar. 36
The amount of protein and vitamins that the slaves received was not enough to keep their bodies sufficiently healthy. Most of their meals consisted mainly of carbohydrates. The reason for this was quite simple: beans and groats could be stored rather easily, while meat and other fresh food perished quickly. The slave traders did try to prevent the food from rotting. Gallandat wrote in his Noodige verrichtingen that the barrels used to store the food had to be treated with sulphur fumes to prevent them from getting infested with insects. 37 Nonetheless, the food would spoil if the journey took longer than expected. In case of delay, the slaves and crew were put on rationing, which caused mortality to rise.
Controlling the quality of food was not the only problem. Dutch water was of relatively good quality, and it could last the slavers for at least their journey to Africa. Eventually, however, it would turn bad and the slavers had to use water collected in Africa. This water was often contaminated with insects, parasites and bacteria: it caused fevers, dysentery and Guinea-worm infections. Ideally, the water would be boiled before use to kill possible sources of infection, but boiling water daily for all the slaves and crew was simply not feasible. Instead, drops of vitriol, sulphur or vinegar were added to the water. 38 Bacteria and other microbiota in the water supply were not the only threat. Gallandat acknowledged that rats and mice posed a problem as they brought diseases and recommended that cats be taken on every journey. 39
The capacity of the ship limited the amount of water that could be brought on the journey, so slaves were given carefully measured amounts of water during the day, which ammounted to roughly 1.5 litres of water per person per day. This was only half of the 3 litres that one should drink in the tropical climates of Africa and the Western Colonies in order to avoid dehydration. Because of the lack of water, slaves became more susceptible to diseases: their tongues swelled up and their eyes became sunken. The surgeon on board usually interpreted this as an ‘inborn melancholy’ and treated it with purging medication – a treatment that did more harm than good. 40
At this point, it is important to note that even though these rules existed, and the slavers worked to keep the slaves relatively healthy, the slaves were never extended any courtesy out of love or respect. Dutch slavers did not consider slaves as human beings, despite their remarks that they did not treat their slaves worse than the Portuguese, English and French treated theirs, and that their ships were cleaner than their competitors’ ships. 41 They saw them as cargo, as armazoen, which would earn them money, and it was in their own best interest to keep them healthy and alive, as a guarantee for a greater return on their initial investment. Postma states that buying a slave in Africa in the eighteenth century would cost a slaver roughly 130 guilders, whereas in the Americas a slave would sell for 300 guilders. This was a sufficient incentive to try to keep as many slaves alive as possible. 42 However, the prices of buying and selling slaves fluctuated in the seventeenth and eighteenth centuries.
Keeping this in mind, it should come as no surprise that the surgeon was one of the highest-paid people on board. Earning between 28 and 36 guilders per month, he came second only to the captain, who earned 50–60 guilders per month, 43 and the pastor, who was not only the religious ‘helmsman’, but also the moral compass on board. 44 The salaries of the captain and the pastor were almost equal, although the captain had more opportunities to acquire a substantial extra income. 45
Curative medicine
Reports on mortality rates of slaves on board of WIC ships differ but range from 12 to 19%. Counter-intuitive as it may seem, the communis opinio is that a higher number of slaves on a ship does not translate into higher mortality rates. A longer duration of the voyage, however, does seem to correlate with a higher mortality, mainly because of a lack of food near the end of the journey. A total overview of ships, deaths and death percentages based on Postma's findings can be found in Table 1. 46
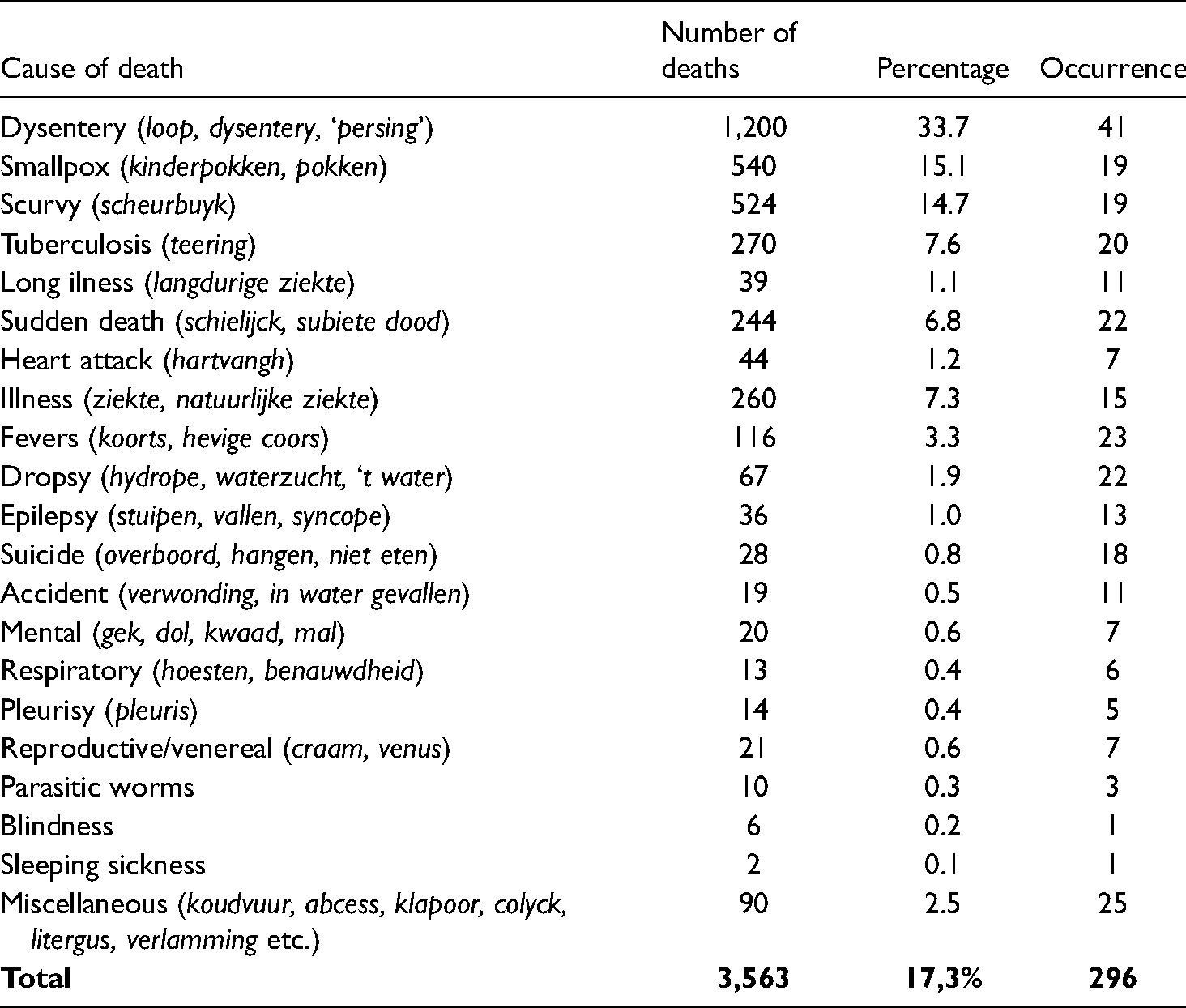
Causes of death on 42 voyages (total number of slaves in sample, 20,653; total deaths 3,563 (17.3%), n = 42)
An average mortality rate of 16% is higher than the mortality of free sailors on the Dutch or United East India Company (in Dutch: Vereenigde Oostindische Compagnie, VOC) ships – it has been calculated that between 1620 and 1780 mortality rates amongst crew arriving in Asia ranged from 6.2 to 16.8% with an average of 10.3% – but one must keep in mind that VOC voyages usually took three times longer than WIC voyages, so it seems safe to state that the mortality per month was higher for slaves. 47 According to several authors, among others Emmer and Postma, this relatively high mortality rate could partially be attributed to inexperienced slavers. Preferring a smaller, more experienced crew over a larger, incompetent one implied raising sailors’ wages to attract a better and more experienced labour force. In addition, Muller and Haaf suggest screening candidate sailors for general health and motivation, using orphans who were more accustomed to a poor, unvaried diet – and even using old VOC ships to slowly accustom the sailors-to-be to the conditions on board before they departed. 48 These preventive measures could, in theory, also be used for slaves. As mentioned above, the screening of possible slaves did occur, but other measures such as getting them slowly accustomed to seafaring were probably too time consuming to implement.
It is interesting to examine the possible causes of death of slaves on board WIC ships, alongside presenting and interpreting harsh, matter-of-fact mortality figures. These causes of death include diseases that are very typical for sailors, such as dysentery, but also indigenous diseases that the slaves or crew brought on board. Postma collected records of death causes among slaves from 42 different voyages. A summary of these records can be found in Table 1. 49
The accuracy of this list should be examined critically. When it came to infectious diseases, ship surgeons in the seventeenth and eighteenth centuries were ignorant at best and thoroughly misinformed at worst. They had been trained to deal with trauma, such as ulcers, amputations and wounds, and much less with vague symptoms such as lethargy, diarrhoea and fever, and they often did more harm than good. In fact, Gallandat criticised the ignorance amongst Dutch surgeons, lamenting the disinterest his peers showed in the publications of physicians such as Salomon de Monchy. 50
Regardless of Gallandat's criticism, there is no doubt that dysentery (loop or rode loop), a type of gastroenteritis characterised by the occurrence of diarrhoea, which could be mixed with blood, was an important cause of death among slaves. Despite attempts to separate sick slaves from healthy ones, dysentery had a tendency to spread quickly. This, of course, affected both slaves and crew, resulting in 1,200 deaths in 42 journeys. Figure 4 shows an excerpt from the journal of Petrus Couperus, surgeon on board the slaving ship Eenigheyt, who diagnosed a slave with buikloop (diarrhoea). 51
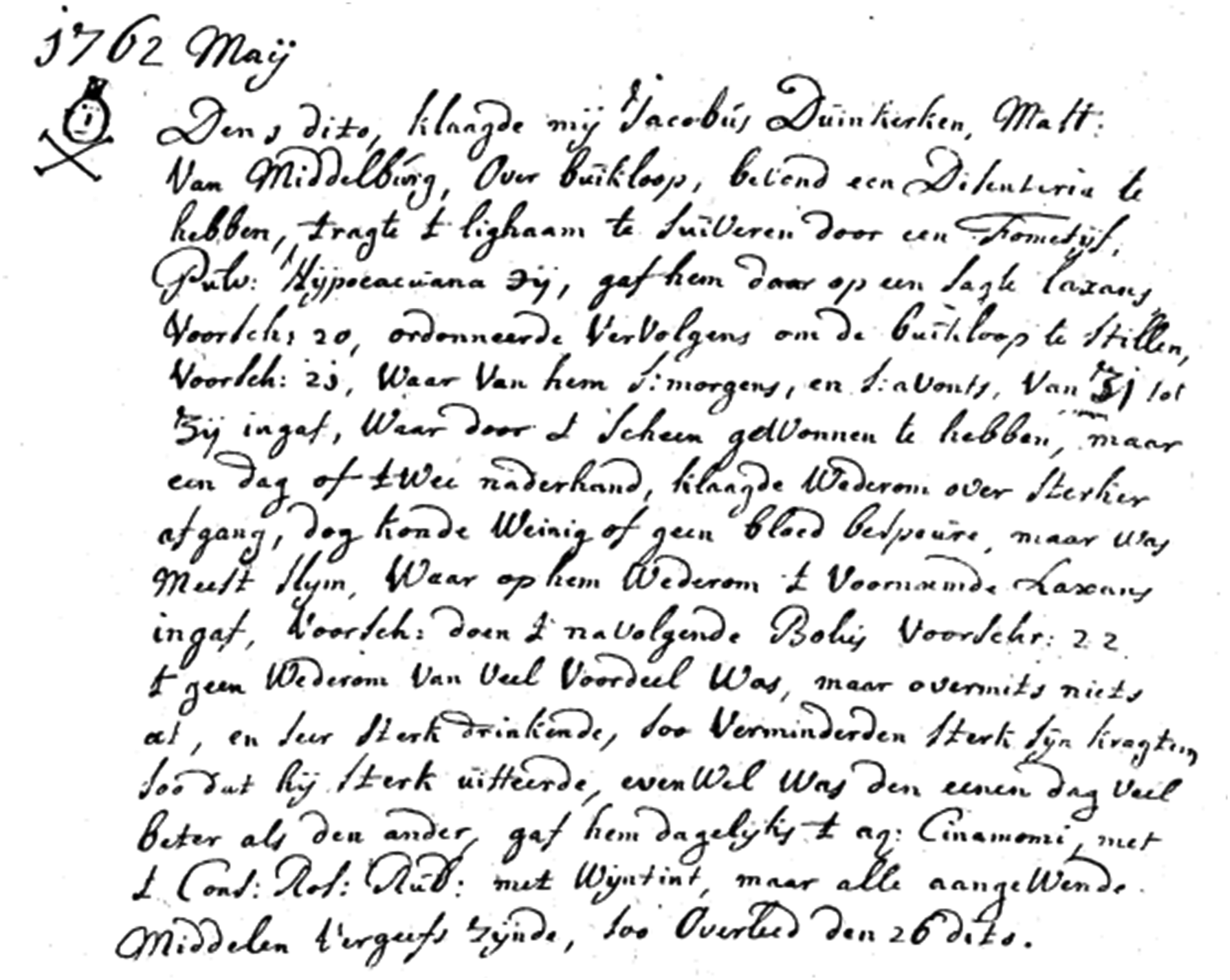
Excerpt from the journal of Petrus Henricus Couperus, dated May 1762. Drawn in the left margin is a skull with crossbones and an hourglass, indicating the death of the patient.
The above-mentioned percentage of Postma connects with the database of https://www.slavevoyages.org in Table 2. The average percentage of slaves embarked who died, so the overall death rate, during voyages was 12.2%. 52
Transatlantic slave trade – database

"Imputed results are calculated by an algorithm"; https://www.slavevoyages.org, accessed 10 February 2022.
Couperus left behind a list of recipes to treat several diseases, not only dysentery, based on reports about the type of sickness of the crew and of slaves. His list included 27 recipes for the crew and 14 for slaves. Schoute's article includes some of these recipes, used in an unsuccessful attempt to save the live of the slave who had turned ill. He prescribed a vometyf (purging medication), the ipecacuanha plant. Next, he prescribed laxation medication, using recipe 20: a mix of rhubarb and nutmeg. These recipes did not stop the diarrhoea, and Couperus prescribed a conditium (a syrup), consisting of rosehip, fragastorius (an opiate), copaivae balm, deer antlers, snake blood, laudanum and peppermint oil. Initially, the treatment had an effect – the diarrhoea stopped. When the symptoms returned, Couperus prescribed a mix of poppy syrup, lobster eyes, snake blood and laudanum – to no avail, as the patient did not survive. To a modern physician, this comes as no surprise, as none of these remedies targeted the cause of the disease – the microbial infection of the intestines. In the eighteenth century, it was not known what caused the disease and surgeons simply tried to fight the symptoms, which severely diminished the probability of survival. 53
When the cause of a disease was known, however, the surgeons did move from a symptomatic to a curative treatment, indicating that they were not fixated on the symptoms alone. For example, as a lack of fruits such as limes and lemons was thought to be at least one cause of scurvy, these were used to prevent and cure the notorious nautical disease.
Besides well-known ‘nautical’ diseases such as diarrhoea and scurvy, the slaves also suffered from diseases indigenous to the African continent and therefore completely unknown to the European slavers. For these indigenous diseases, Gallandat recommended that surgeons turned to indigenous cures, stating that he recognised the merit of African medicine and that the Dutch owed it to the ‘illiterate and barbarian gentiles’ to apply the medical knowledge.
Two examples of these indigenous maladies will be discussed here: the Guinea worm, and a disease known as koortskoek. As the name implies, the Guinea worm is a parasite – Dranunculus medinesis, a roundworm that can grow up to 80 cm in length. 54 It posed a problem for the slavers both on board the slaving ships and in the colonies themselves. Larvae of the parasite could be found in fresh water taken from the western coast of Africa, from which the worm derives its name. After ingestion, the larvae of the Guinea worm make their way through the intestine wall and mature into adult worms. Male worms die in the host, while female worms migrate to subcutaneous tissue. At the end of their life cycle, Guinea worms cause a blister on the skin, and eventually emerge from the skin to get back to the water. Symptoms of an infection with these parasites include severe muscle pains and a blister on the skin of the lower extremities, followed by the eruption of the worm through the skin. The only treatment is removal of the worm, when found. 55
In the literature, several descriptions of the disease koortskoek exist, sometimes with different descriptions of the symptoms. Often it is described as periodic fever, jaundice, fatigue and a hardened and enlarged spleen. This is a combination of symptoms that is very reminiscent of the disease we now call malaria, which is indigenous to Africa. However, it has also been described by European colonists in the Western Colonies. In this case, the main symptoms were hardening of the liver and jaundice. It could very well be that these descriptions are actually descriptions of two different diseases, namely malaria and liver cirrhosis – as life in the colonies was not always the prime example of the allegedly sober Reformed lifestyle. 56 Similar to the treatment of dysentery, the treatment of koortskoek only focused on the fevers, not the underlying cause. Couperus treated a febrile slave with a laxantium and a so-called pulvis antefebrilis: a mixture of lobster eyes, corallum rubum, burned deer horn, antimonium, saltpetre, saffron and nutmeg oil. It is unknown whether this slave suffered from koortskoek or another disease, but the treatment did not work – the slave did not survive. 57
Overall, medical care for slaves on board was fairly acceptable when one considers the (lack of) knowledge about causes and cures of diseases, although Gallandat stated that part of this ignorance could be attributed to the unwillingness of surgeons to consult updated literature. As discussed above, several preventive measures were taken to prevent slaves from falling ill. In addition to these preventive measures, surgeons were instructed to visit the slaves every day to assess their health and administer treatment if necessary. If there was no surgeon on board, this responsibility fell to the captain.
From the journal of Couperus, we can infer that there were 27 different recipes available for the crew and 14 for the slaves, although Couperus used all recipes for the slaves. It is unknown whether other surgeons did this as well, but at least Couperus did what he could when treating slaves. He did not cure all of them, but often he was simply too ignorant of the diseases that he dealt with. As discussed above, this does not mean that he cared for the slaves or felt sympathy for them. It simply means that he was doing his job. The WIC needed the slaves healthy and alive when they set foot on the coast of Brazil, Suriname, Guyana or the Dutch Antilles, so that they could see a return on their initial investment.
Phase three: arrival in the New World
Numbers and destinations
The Dutch were not the first Europeans to be involved in the transatlantic slave trade. At the outset, the Dutch were against slave trade and thought of it as ‘morally wrong’. They strongly condemned the Portuguese and the Spanish for being engaged in this kind of trade, although one could argue that this was merely out of anti-Iberian sentiments rather than ideological and moral reasons (Table 3).
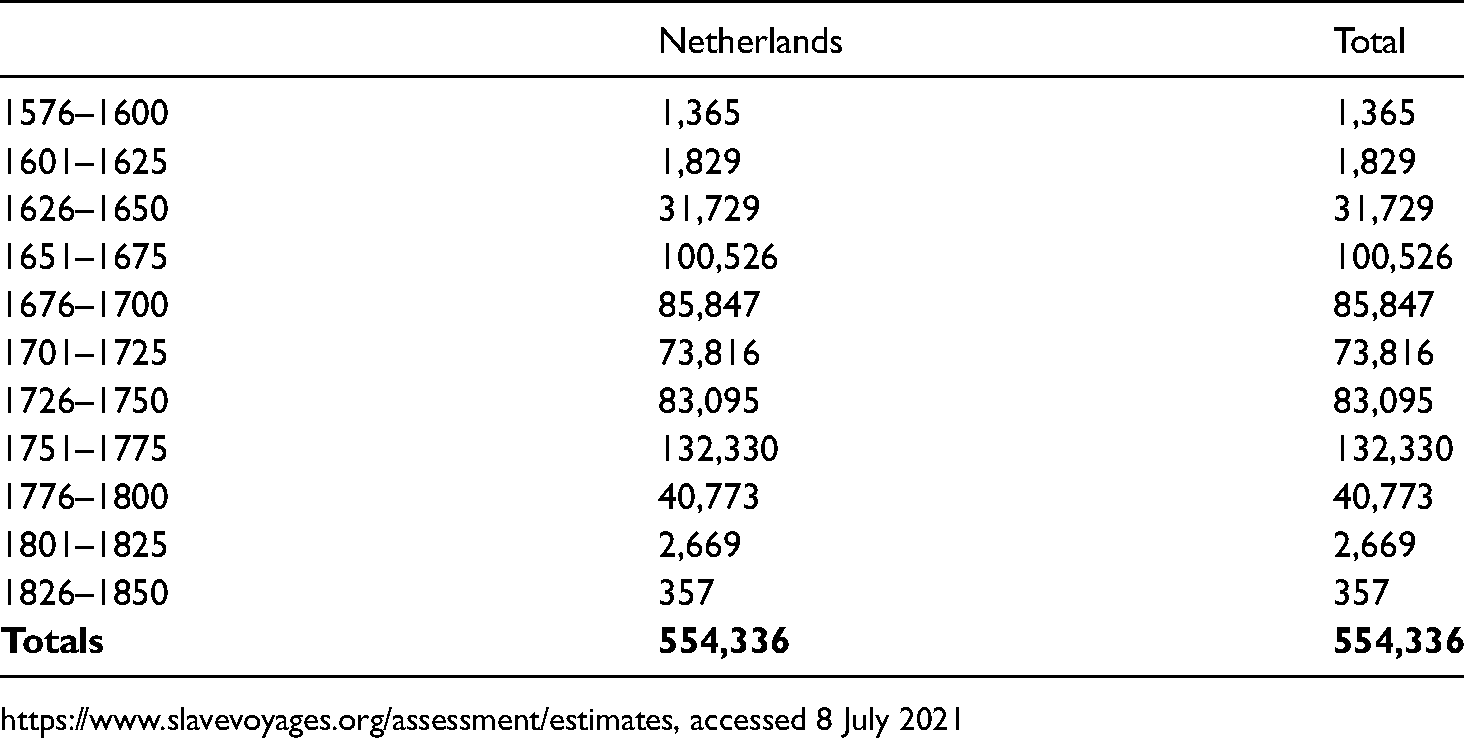
Transatlantic slave trade 1576–1850 – numbers embarked and disembarked under a Dutch flag – estimate

Source: https://www.slavevoyages.org/assessment/estimates, accessed 8 July 2021.
However, it may come as no surprise that the people in the Dutch Republic rapidly changed their mind when the Dutch first set foot in the New World in 1609. Especially after expelling the Portuguese from northeastern Brazil in 1630, it became clear that it was impossible to cultivate the plantations in these overseas territories without a continuous influx of cheap labour. It was not long before the Dutch were also transporting slaves across the ocean. Table 4 presents the main colonies to which the Dutch transported slaves over the Atlantic Ocean during the seventeenth and eighteenth centuries. Between 1630 and 1654, Brazil was an important colony to which a fairly large number of slaves was transported. The Dutch were leading the transatlantic slave trade between 1655 and 1675. This was not the WIC, however, which was almost bankrupt. In that period the Dutch slave trade was mainly in the hands of private merchants from Amsterdam. 58 After 1654, the Dutch involvement in the slave trade to Brazil stopped completely, owing to the fact that the Portuguese recaptured this colony from the Dutch. 59
Transatlantic slave trade 1576–1850 under a Dutch Flag – estimate
https://www.slavevoyages.org/assessment/estimates, accessed 8 July 2021
Postma argues that between 1662 and 1689 the Republic was the major slave-trading nation. 60 In these years, the Spanish Crown granted the asiento de negros only indirectly and for a very short time to the Dutch merchant Balthasar Coymans in the 1680s. The Dutch delivered slaves to Curaçao to hand them over to agents of the asentistas. The Dutch were able to manoeuvre into this position as they could utilise their previously acquired knowledge and experience in the slave trade. Moreover, they had a very important asset that the Spanish did not have: their settlements in Africa that could provide them with slaves.
Another development to notice is the explosive increase in the number of slaves being transported to Suriname in the eighteenth century, primarily in the period 1745–1774. Inikori and Engerman consider the advent of stable governments and the subsequent growth of the Surinamese colony as an important reason for this increase. More plantations appeared, requiring substantial numbers of slaves. After they lost most of their contracts with the Spanish American colonies, Suriname became the most important market for Dutch slave traders.
At first glance one might conclude from the numbers presented above that the Atlantic region was of major importance to the Dutch colonial activities. Emmer and Klooster, however, point out that it played a relatively modest role. Already 50 years after their initial arrival, the influence of the Dutch maritime presence in the Atlantic was declining and the English, Spanish and Portuguese took over the leading position.
Keeping the purpose of this article in mind, some information can be found on the treatment of slaves in Suriname. As this colony has been the most important Atlantic overseas territory for the Netherlands for a long period, looking at the life of slaves in Suriname will provide important insights. Therefore, we try to create a broader context for the treatment of slaves on plantations in general, based on the case of this single country – of course knowing that policies could vary between different colonies.
Living and working conditions on the plantations in Suriname
Sickness and health cover a broad range of aspects. Working conditions had an important influence on the health situation of slaves, since they spent most of their time working – it was the sole reason their owner had bought them. There may be no doubt that these conditions were poor. Child labour was not uncommon, and slaves had to work at night, without being compensated for this. Moreover, until the eighteenth century, women had to continue working even if they were pregnant. Alex van Stipriaan points to quantitative data that suggests that conditions improved during the nineteenth century. 61 However, these improvements were not yet introduced in the period discussed in this paper and thus working conditions would have been severe in those years.
Reports in Surinaams Contrast by Alex van Stipriaan shed light on the differences in working conditions between three plantation sectors (coffee, cotton and sugar). 62 These indicate that slaves were treated best on cotton plantations and worst in the sugar sector. This was caused by a range of factors, including the fact that cotton cultivation did not require much night work, and the work was physically also relatively light. The difference between sectors can also be identified by the quality of nutrition, a second key element for the health of slaves. Cotton plantations were often situated near the sea, and slaves were therefore provided with seafood. This type of food contains high levels of protein, which made for a healthy diet compared with those in other sectors where slaves were deployed. 63
Nevertheless, in general, nutrition was often ignored. A study by X.G.J. Mulder, professor of chemistry, in 1846 found that slaves in these years only received around 40% of what was considered to be the minimum nutritional value that a soldier should get. 64 In general, slaves received food from their owners. However, it was also common for them to have small pieces of arable land where they could cultivate some crops themselves. Not only did this enable them to (partially) take care of their own food supply, but it could also prove beneficial for their self-esteem, as they had some private property and something to be responsible for.
The supply of food was organised, although it was not available in great quantities. This relative scarcity also applied to safe water. In addition, the infrastructure for water was also badly taken care of. In the seventeenth and eighteenth centuries, only a few plantations had water reservoirs installed, resulting in a limited and often unhealthy water supply for the rest of the colony. The Societeit van Suriname, a private Dutch company, was aware of the problems that could arise as a result of food and water scarcity – in the worst case a revolt could break out – and therefore urged plantation owners to provide slaves with sufficient food and water.
In addition to food and water, slaves were often also provided with some additional items. However, expectations should be low; according to Blom, who wrote about this topic in 1787, slaves only received a few items and they completely depended on the plantation owners for the supply. 65 In general, the basic goods that were given included a few pieces of fabric, which slaves had to use for a whole year as clothing and sheets. Plantation slaves only wore clothes that covered small parts of their body and small children walked around naked. It was only after the end of the eighteenth century that the supply of goods to slaves somewhat improved.
It was not until the nineteenth century that the quality of housing also positively changed. Before this shift took place, slaves often lived in a small ‘village’ on the plantation, which consisted of simple huts that were built and maintained by the slaves themselves. Primarily because of the wet ground, sleeping in these huts could certainly be considered unhealthy and the transition to houses of better quality was perceived as a positive development. Just like the small pieces of arable land mentioned before, the primitive housing was also valued for the relative degree of freedom and space that it provided. Judging from a sickness and health point of view, living conditions were undoubtedly worse before these housing improvements were carried out.
In addition to the quality of housing, the spatial location of a plantation could also have contributed to the better health of slaves. In this respect, it may have been favourable to be situated near the sea, since the relatively dry climate is generally healthier and makes it difficult for many diseases to thrive. As mentioned before, cotton plantations in Surinam were often situated near the coast, which might have contributed to the relatively low mortality rates in this sector.
The previous paragraphs all describe situations in which preventive care was used to influence sickness and health amongst the slaves. However, people did get sick, and thus required medical treatment. This so-called curative care was available in the colonies, but it was often of bad quality. In the eighteenth century, many plantations did not have their own clinic and professional treatment could not be given. Furthermore, even if a clinic was present, these were likely to be unhygienic – and according to some reports even bad for one's health. 66
When a slave got sick, they were first handed to another slave who was responsible for medical issues. Only if their sickness lasted for a few days were they were redirected to a ‘professional’ doctor – whose abilities were often also questionable. However, since the plantation owner needed all slaves to work on the plantations, he would not always acknowledge a slave to be sick. As a result, not all slaves received the medical care that they required, worsening the situation for some.
Owing to the differences in working conditions in different sectors (e.g. sugar, coffee, cotton), mortality rates could vary across plantations. When all resulting values are combined, one finds that the average annual mortality in the period 1780–1862 ranges between 35 and 50 deaths per 1,000 slaves.
Even prominent Dutch representatives in Suriname recognised that the poor treatment of slaves negatively influenced mortality rates amongst them. Although commissioner-general of the Dutch East Indies Johannes van den Bosch (1780–1844) stated that the slaves’ way of living was a major cause of the many deaths, he also acknowledged that demanding working conditions and malnutrition were detrimental to the growth of the total slave population, and in his Nederlandsche bezittingen (1818) he urged the drawing up of policy on this subject. 67
It has often been recognised that the treatment of slaves, at least to some extent, caused high mortality rates. However, no continuous, synchronous decline in mortality rates could be observed once living conditions improved. Therefore, other factors could have influenced mortality rates too; Van Stipriaan identifies two of these elements – creolisation and epidemics. 68
Firstly, the process of creolisation could have decreased mortality rates. Creolisation can be described as the mixing of different cultures, which in Suriname created a mixture of people from African and European descent. Evidence suggests that this process, combined with the end of the influx of African slaves in 1827, resulted in a significantly lower proportion of Africans in the total Surinamese population. Since Africans were most susceptible to diseases and performed most heavy tasks, creolisation may have had an effect on the decreasing mortality rates.
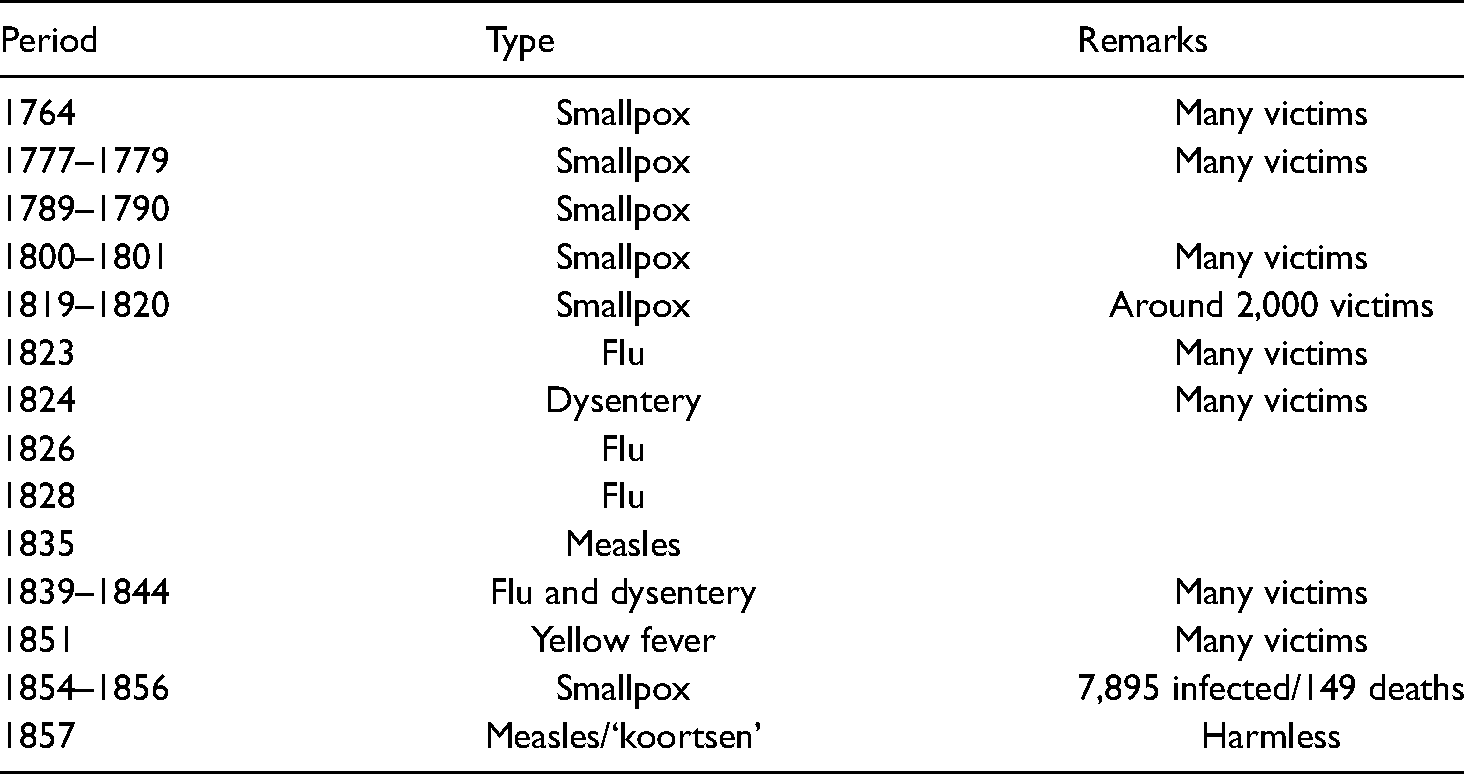
Secondly, and probably more influential, epidemics have caused periods of high mortality. The inhabitants of Suriname regularly faced these epidemics, of which pokken (smallpox) has been reported most often. Table 5 provides an overview of outbreaks of different diseases in Suriname between 1764 and 1857, often resulting in many deaths. In the nineteenth century however, doctors began experimenting with ‘variolation’, a treatment of pokken that could be considered the predecessor of what is currently known as vaccination. Although the adoption of variolation was slow since people were initially reluctant to adhere to this unknown method, the efforts eventually paid off.
An overview of outbreaks of different diseases in Suriname, 1764–1857 69
In general, it can be concluded that slaves’ living conditions improved over time, reaching their highest levels towards the end of slavery. In the last period (1840–1863) before the abolition, the percentage of slaves dying a natural death was 43% (which was already a 9% increase in comparison with the period between 1815 and 1839). 70 The fact that other death causes were predominant earlier suggests that living conditions were poor enough for sickness to thrive.
Conclusion
This article deals with the treatment of slaves during the time of the Dutch West India Company's existence. This treatment was approached in a twofold manner – with a focus on both moral and medical grounds. Moreover, it provides an analysis of the medical treatment of slaves before, during and after their transport from Africa to the New World and the Caribbean on board Dutch West India Company ships in the seventeenth and eighteenth centuries. There seems to have been significant changes in attitude amongst the slavers regarding their interest in the slaves’ health whilst still residing in Africa as opposed to crossing the Atlantic.
We have discussed the abominable living conditions the slaves were subjected to prior to their departure. Although it seems fair to state that these conditions did not improve while sailing westward, preventive and curative medical measures were taken by ships' surgeons – and to a lesser extent by ziekentroosters (comforters of the sick) in attempts to ensure that the major part of the armazoen (the cargo) would make it alive to the plantations in America and the Caribbean. Assessing the results of the surgeons’ attempts we need to keep in mind that it has been acknowledged by contemporary doctors that those responsible for the slaves’ physical (and to a certain extent also mental) health more often than not were facing diseases unknown to them. In times of high demand, ziekentroosters were assigned but not particularly well-educated by the Dutch Reformed Church before entering the service of the Dutch West India Company. Surgeons moved between moral dogmata and state of the art research and publications by renowned doctors like David Henri Gallandat. Gallandat, although arriving on the scene at a rather late stage (1769), is quite remarkable in that he published some sort of medical guide for surgeons who faced the challenges of coping with diseases amongst the slaves unbeknown to the western medical profession. He seemed to have cared for black lives, albeit operating within the parameters of what – at least according to the standards used in early modern times – was morally and medically acceptable. As such, he stands out as one of few champions for those many hundreds of thousands who were forced to traverse the Atlantic Ocean among others under the flags of the Dutch West India Company.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Notes
Author biographies
Joost Schokkenbroek is professor emeritus at Vrije Universiteit Amsterdam and Director of the Hong Kong Maritime Museum.
Leon van den Broeke is Associate Professor Religion, Law and Society/Church Polity, and Chair of the Centre for Religion and Law at the Vrije Universiteit Amsterdam and Extraordinary Professor Church Polity at the Theological University Kampen, the Netherlands.