
Abstract
Background
Emotional exhaustion is a core component of burnout, linked to poor nurse well-being and negative patient outcomes. In Canada, where nurse burnout has risen sharply, there is limited evidence tracking changes across healthcare sectors over time. This study addresses that gap to inform workforce and policy interventions.
Purpose
To examine trends in emotional exhaustion and perceptions of quality and safety among nurses in British Columbia working in acute care, long-term care, and community care settings over three time points: 2015, 2019, and 2020.
Methods
We conducted a secondary analysis of three cross-sectional surveys of nurses in BC. The analytic sample included 8,412 nurses. Emotional exhaustion was measured using the Maslach Burnout Inventory, and quality and safety outcomes were assessed using validated RN4CAST indicators. Survey year was the key independent variable; six demographic and professional characteristics were included as controls. Linear regression was used for emotional exhaustion and ordered logistic regression for ordinal outcomes.
Results
Nurses' emotional exhaustion demonstrated a two-fold increase from 2015 to 2019 and a four-fold increase from 2015 to 2020. While nurses’ ratings of all quality and safety measures improved from 2015 to 2020, only their ratings of last shift and general quality of care improved between 2015 to 2019.
Conclusion
The observed increase in nurses’ emotional exhaustion over time likely reflects the cumulative impact of persistent system pressures and escalating workloads, particularly during the COVID-19 pandemic. Incorporating measures of burnout into Canada's health workforce dashboards would inform more targeted, data-driven strategies for sustainable health workforce planning.
Introduction
Nurses play a vital role in delivering high-quality healthcare and ensuring patient safety across the healthcare spectrum (e.g., acute care, long-term care, community care). Increasing workforce challenges include staffing shortages, high patient loads, and overall demanding work conditions. Research suggests that in response to these challenging circumstances, nurses experience increased emotional exhaustion, resulting in deterioration of care quality and safety (Q/S) (Aiken et al., 2012; Galanis et al., 2025; Maslach & Leiter, 2016; Woo et al., 2020). Emotional exhaustion is a key indicator of burnout and has been linked to negative outcomes for nurses (e.g., turnover) and patients (e.g., adverse events) (Aiken et al., 2012; Galanis et al., 2025; Maslach & Leiter, 2016). Despite widespread recognition of these risks, there is limited evidence documenting how nurses’ emotional exhaustion and perceptions of Q/S have evolved over time, particularly within the Canadian healthcare context.
This study examines trends in emotional exhaustion and Q/S perceptions among nurses in British Columbia (BC) over a five-year period using data from three timepoints—2015 (five years before the pandemic), 2019 (immediately before the pandemic), and 2020 (at the height of the pandemic). Given that BC faces nursing workforce challenges similar to other high-income health systems, these findings may offer valuable insights into global nursing trends and inform policies aimed at mitigating burnout-related risks to patient safety and quality of care (Adhikari & Smith, 2023; Baumann, 2006; Maier et al., 2017; World Health Organization, 2020).
Background & Purpose
Burnout in Nursing
Burnout is a psychological syndrome that arises in response to chronic workplace stress and is characterized by three dimensions: emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment (Maslach et al., 2018). Among these, emotional exhaustion is often the earliest and most prominent symptom of burnout, making it a key indicator of workforce well-being and an important target for intervention (Demerouti, 2024). Emotional exhaustion is characterized by overwhelming fatigue and depleted emotional resources due to prolonged exposure to workplace stressors (Demerouti, 2024). Among nurses, burnout, particularly emotional exhaustion, is associated with poor working conditions (e.g., excessive workloads, chronic understaffing, lack of organizational support, unhealthy workplaces), which contribute to high levels of stress and job dissatisfaction (Galanis et al., 2025; Maslach & Leiter, 2016; McHugh et al., 2011). The COVID-19 pandemic resulted in deterioration of nurses’ working conditions with evidence suggesting that burnout and emotional exhaustion rose sharply among healthcare workers during the pandemic (Sexton et al., 2022).
Globally, burnout and emotional exhaustion are widespread experiences among nurses, the largest group of healthcare workers. A 2020 systematic review analyzing 113 studies found that more than one-third of nurses worldwide reported severe burnout symptoms, with high emotional exhaustion being the most frequently reported symptom (Woo et al., 2020). Further work suggests that 43% of nurses suffer from high emotional exhaustion (Aiken et al., 2002), and each additional patient per nurse increased the odds of nurse emotional exhaustion by 23% (Aiken et al., 2002). Global prevalence rates vary substantially, with only 10% of nurses in the Netherlands reporting emotional exhaustion, compared to 78% in Greece (Aiken et al., 2014). In Canada, a national survey conducted in 2020 found that 63% of nurses reported at least some symptoms of burnout; by 2024, this figure had risen to 90% (Canadian Federation of Nurses Unions, 2020, 2024).
Nurses’ emotional exhaustion is notably affected by healthcare sector and individual demographic characteristics. Research has demonstrated that nurses working in acute care settings are nearly twice as likely to leave their jobs due to burnout compared to those in community care settings (Shah et al., 2021). In addition, younger nurses, those with fewer years of experience, and those in early-career roles report higher levels of emotional exhaustion, potentially due to their limited coping mechanisms and higher exposure to workplace stressors (Rudman & Gustavsson, 2011; Senek et al., 2020; World Health Organization, 2020).
High levels of emotional exhaustion have significant consequences for patient care outcomes (Ball et al., 2018; Kirwan et al., 2013; Smith et al., 2018). For instance, hospitals with nurses reporting higher emotional exhaustion had significantly higher rates of healthcare-associated infections (Cimiotti et al., 2012). Additionally, evidence suggests that nurse burnout, particularly the experience of emotional exhaustion, is significantly associated with reduced healthcare Q/S, such as increased medication errors, patient falls, and missed care, as well as lower patient satisfaction (Li et al., 2013). These findings emphasize the critical importance of addressing burnout, and in particular, emotional exhaustion as a fundamental patient safety concern across the healthcare spectrum.
Quality and Safety in Nursing
Q/S in nursing refers to the provision of nursing care that is safe, effective, timely, efficient, equitable, and patient-centered while preventing harm and adverse outcomes (Healthcare Excellence Canada, 2019; Incident Analysis Collaborating Parties, 2012; Institute of Medicine, 2001). Nurses’ Q/S ratings are influenced by working conditions (Aiken et al., 2014; McGilton et al., 2013). Research with nurses across nine European countries showed those working in acute care hospitals with unhealthy working conditions, operationalized as lower scores on the Practice Environment Scale, had significantly worse Q/S ratings compared to their counterparts in a healthy work environment (Ball et al., 2018; Kirwan et al., 2013). Notably, among the various factors influencing these ratings, understaffing was consistently identified as a critical predictor (Ball et al., 2018).
Just as workplace conditions shape Q/S ratings, individual nurse characteristics, including experience and education level, also play a role in nurses’ ratings of Q/S. Research suggests that nurses with more experience and higher education often report frequent critical assessments of Q/S, potentially due to their heightened awareness of system inefficiencies and safety risks (Aiken et al., 2002; American Association of Colleges of Nursing, 2024; Nowrouzi-Kia et al., 2022). Nurses’ ratings of Q/S vary significantly across the globe, with only 4% of nurses in Switzerland providing a poor or failing safety grade, compared to nearly half (47%) of nurses in Greece (Aiken et al., 2014). In Canada, CFNU's national survey found that approximately one in three rated the Q/S in their workplace as “poor” or “fair”; over half reported a deterioration of the Q/S at their workplace over the last year, and experienced a near miss or patient safety incident (Canadian Federation of Nurses Unions, 2024).
Nurses’ Q/S ratings of their own care are highly correlated with actual patient outcomes, making them crucial indicators of health system performance (Aiken et al., 2012). To illustrate, a 10% increase in the proportion of nurses rating the Q/S in their hospital as excellent is associated with a 5% decrease in the odds of 30-day inpatient mortality (McHugh & Stimpfel, 2012). Poor nurse Q/S ratings have also been linked to higher rates of patient dissatisfaction, patient adverse events, job dissatisfaction, nurse moral distress, and nurse turnover (Kirwan et al., 2013; Li et al., 2024).
Knowledge Gap
While an extensive body of evidence has examined emotional exhaustion and Q/S of care among nurses, most research have been cross-sectional and disproportionately focused on acute care settings, with limited evidence from long-term care or community care contexts (MacLeod et al., 2017; Pijl-Zieber et al., 2008). The few existing longitudinal studies have either been conducted with the general healthcare workforce (as opposed to just nurses), completed outside of Canada, employed only two time points, or failed to examine effects across the healthcare spectrum, limiting understanding of how these phenomena change across different healthcare sectors (Incident Analysis Collaborating Parties, 2012; Institute of Medicine, 2001; Sexton et al., 2022). The current study addresses this gap by analyzing data from BC nurses from acute care, long-term care, and community care across three time points (2015, 2019, 2020), examining trends in both emotional exhaustion and nurse-reported Q/S perceptions.
Methods and Procedures
Study Design and Participants
This study is a secondary analysis of data from three provincial cross-sectional surveys of British Columbia (BC) nurses focused on their workplace and care delivery experiences long before, immediately before, and during the height of the COVID-19 pandemic. Administered in 2015 (July–September), 2019 (September–December) and 2020 (April–May), all three surveys were conducted electronically and supported through a partnership between nurse researchers at a Canadian University and the BC Nurses’ Union (BCNU). The 2015 survey targeted a stratified random sample of 20,000 nursing members of the BCNU, yielding a total of 2,366 nurse respondents across acute care, long-term care, and community care (response rate: 12%). The 2019 and 2020 surveys were sent out to all BCNU nurse members (∼47,000), yielding a total of 5,512 (response rate: 12%) and 3,676 (response rate: 8%) nurse participants across the three healthcare sectors respectively. Additional details on the broader study methods are available in the study final reports for each survey timepoint University of British Columbia.
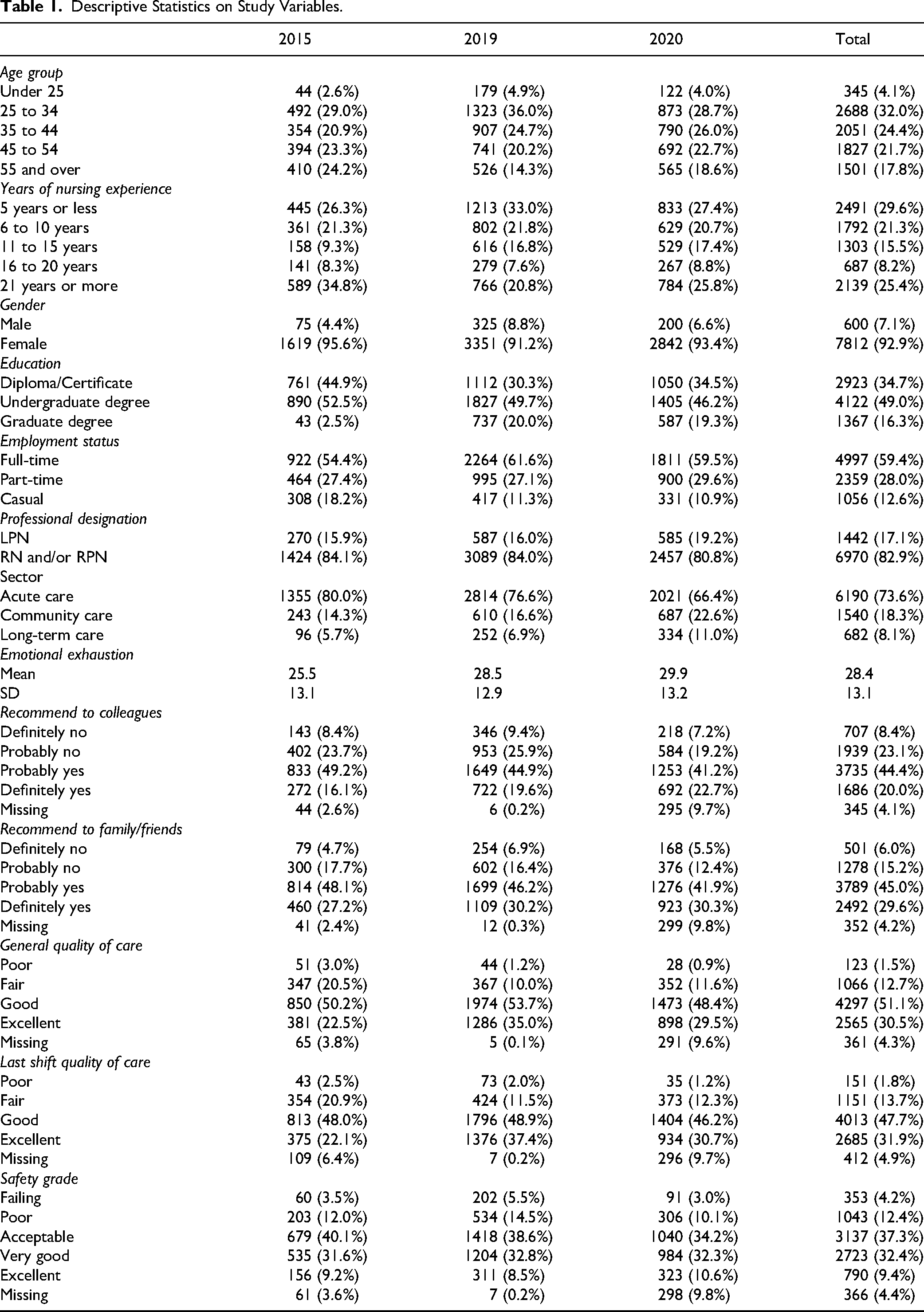
This secondary analysis was conducted with a subset of the data from each survey timepoint after a series of inclusion and exclusion criteria were applied. Eligible participants included actively working (not retired or on leave) registered nurses (RNs), registered psychiatric nurses (RPNs), and licensed practical nurses (LPNs) in direct care roles with a “diploma/certificate,” “undergraduate degree,” or “graduate degree” who identified their gender as male or female. Nurses who identified their gender as “prefer to not disclose” or “prefer to describe” represented only 0.6% of the data and therefore were excluded from the analysis. Likewise, nurses who identified their role as “leader,” “educator” or “other,” their professional designation as “other” or as “student nurse,” and their education as “other” were excluded from the analysis. Finally, all responses with missing values in any of the categorical independent variables were removed from this analysis. Overall, applying these inclusion/exclusion criteria resulted in a final sample size of 8,412 participants from the three nursing sectors, comprising 1,694 participants from the 2015 survey, 3,676 from the 2019 survey, and 3,042 from the 2020 survey (Table 1). This secondary analysis of data was approved by the University of British Columbia Behavioral Research Ethics Board (approval number: H24-02218).
Descriptive Statistics on Study Variables.
Patient and Public Involvement
Patients and the public were not involved in the production of this research.
Measures
Outcome Variables
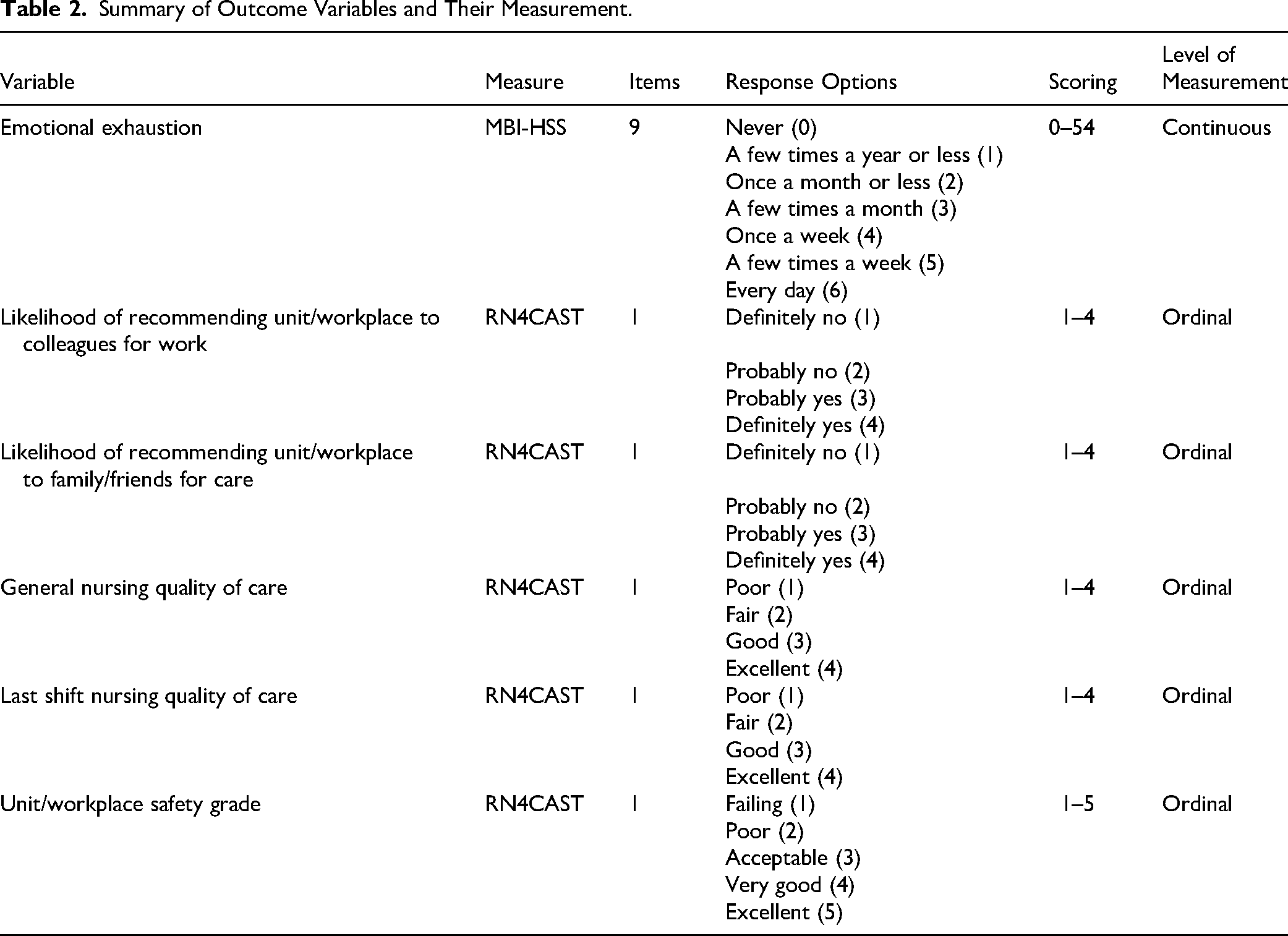
The outcome variables consisted of emotional exhaustion subscale of the Maslach Burnout Inventory-Human Services Survey (MBI-HSS) and five Q/S measures from the RN4CAST study. Table 2 summarizes these outcome variables and their measurement.
Summary of Outcome Variables and Their Measurement.
Independent Variable
As the focus of this secondary analysis was on the change over time in outcome variables, “Survey Year” is used as the key independent variable in this analysis. For simplicity, “Survey Year” is hereafter referred to as “Year.”
Control Variables
Nurses were asked about their demographic characteristics, including age (in ordinal categories of years), and years of nursing experience (in ordinal categories of years), gender (male, female), professional designation (LPN or RN/RPN), education (diploma/certificate, undergraduate degree, graduate degree), employment status (full-time, part-time, casual) and healthcare sector (acute care, community care, and long-term care).
Data Analysis
Since these three surveys were not repeated measures, we were unable to conduct latent growth curve modeling (LGCM). Instead, we obtained a regression model for each outcome variable with the time point (Year) as the key predictor while controlling for the impact of six control variables.
Age and years of nursing experience were highly correlated (r = .791), and subsequently age was removed from the regression models to address multicollinearity. A general regression model was applied to the continuous outcome variable (emotional exhaustion), while an ordered logistic regression was used for the remaining ordinal variables. The categorical variables (independent and control) were dummy coded through the dummy_cols function in the fastDummies (Kaplan, 2025) package in R. For example, the independent variable ‘Year’ was converted into two dummy variables—Year 2019 and Year 2020—using Year 2015 as the reference category. Year 2019 and Year 2020 were entered into the regression model after the control variables. The regression coefficient for the variable ‘Year’ was evaluated to explore the change in emotional exhaustion and Q/S outcomes over time (2019 and 2020) compared to the reference year of 2015.
The regression analysis also examined the potential moderating effect of healthcare sector on the relationships between Year and each outcome variable. Interaction terms between healthcare sector and Year were obtained and included in the regression model. However, all interaction terms were found to be non-significant across all models, and therefore removed from the final regression models.
All analyses were performed in RStudio (Posit Team, 2023). General linear models were fitted using the glm function from the stats (R Core Team, 2021) package in R, while ordered logistic regression models were fitted using the polr function from the MASS (Venables & Ripley, 2002) package in R.
Result
Table 1 provides descriptive statistics on key study variables across each survey time point and for the total sample. Overall, the majority of participants were female registered nurses under the age of 45, with 15 or fewer years of nursing experience, an undergraduate degree, and full-time employment in an acute care healthcare setting.
Regression Analysis: Year
Table 3 illustrates the results of the regression analysis. In 2020, the coefficient for Year was significant for each outcome variable assuming all control variables remained constant (which, in our case, means they were fixed at their reference levels due to the ordinal or categorical nature of the data). For instance, emotional exhaustion scores were 4.1 units higher in 2020 compared to 2015. For Recommending to Colleagues, the log-odds coefficient was 0.312, meaning that in 2020, the odds of a nurse recommending their unit or workplace to a colleague as a good place to work were approximately 1.4 times higher than in 2015 (odds e0.312 ≈ 1.4, p < .001). Other significant findings include: In 2020, the odds of a nurse recommending their unit or workplace to friends and family were 1.3 times higher than in 2015 (odds e0.259 ≈ 1.3, p < .001). The odds of general (odds e0.650 ≈ 1.9, p < .001) and last shift quality of nursing care (odds e0.615 ≈ 1.9, p < .001) were both 1.9 times higher than in 2015. The odds of unit or workplace safety grade were 1.2 times higher than in 2015 (odds e0.183 ≈ 1.2, p < .01).
Regression Analysis of Quality and Safety Outcomes by Year, Controlling for Demographic Variables.
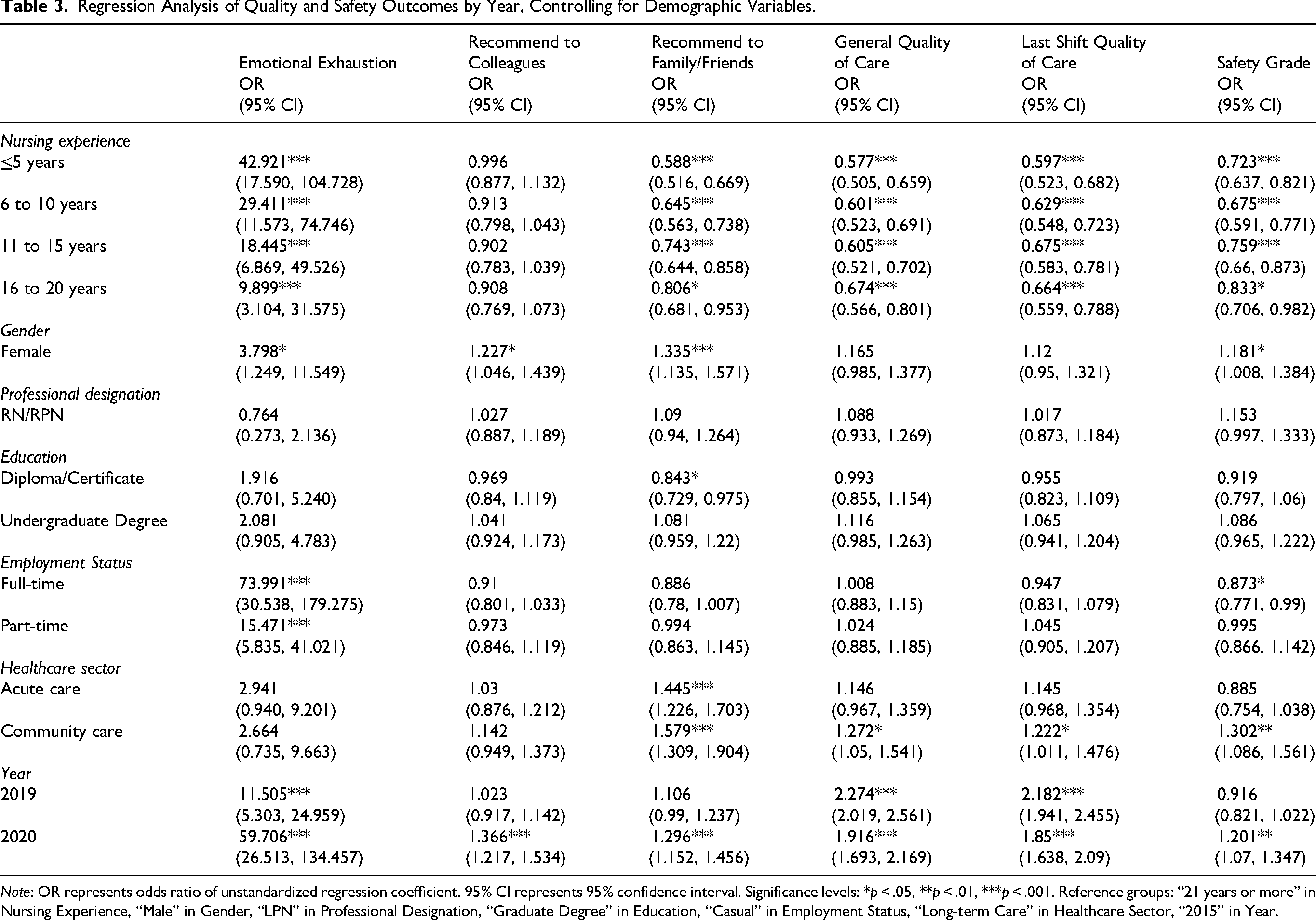
Note: OR represents odds ratio of unstandardized regression coefficient. 95% CI represents 95% confidence interval. Significance levels: *p < .05, **p < .01, ***p < .001. Reference groups: “21 years or more” in Nursing Experience, “Male” in Gender, “LPN” in Professional Designation, “Graduate Degree” in Education, “Casual” in Employment Status, “Long-term Care” in Healthcare Sector, “2015” in Year.
In 2019, nurses reported a higher level of emotional exhaustion compared to 2015 (2.4, p < .001), as well as higher general (odds e0.821 ≈ 2.3, p < .001) and last shift (odds e0.780 ≈ 2.2, p < .001) quality of nursing care. However, there were no significant trends over time in the likelihood of recommending their unit or workplace to colleagues for work and to friends and family for care, or overall patient safety grade. Figure 1 provides visual depiction of the odds for each year and their corresponding 95% confidence interval through an error-bar plot.
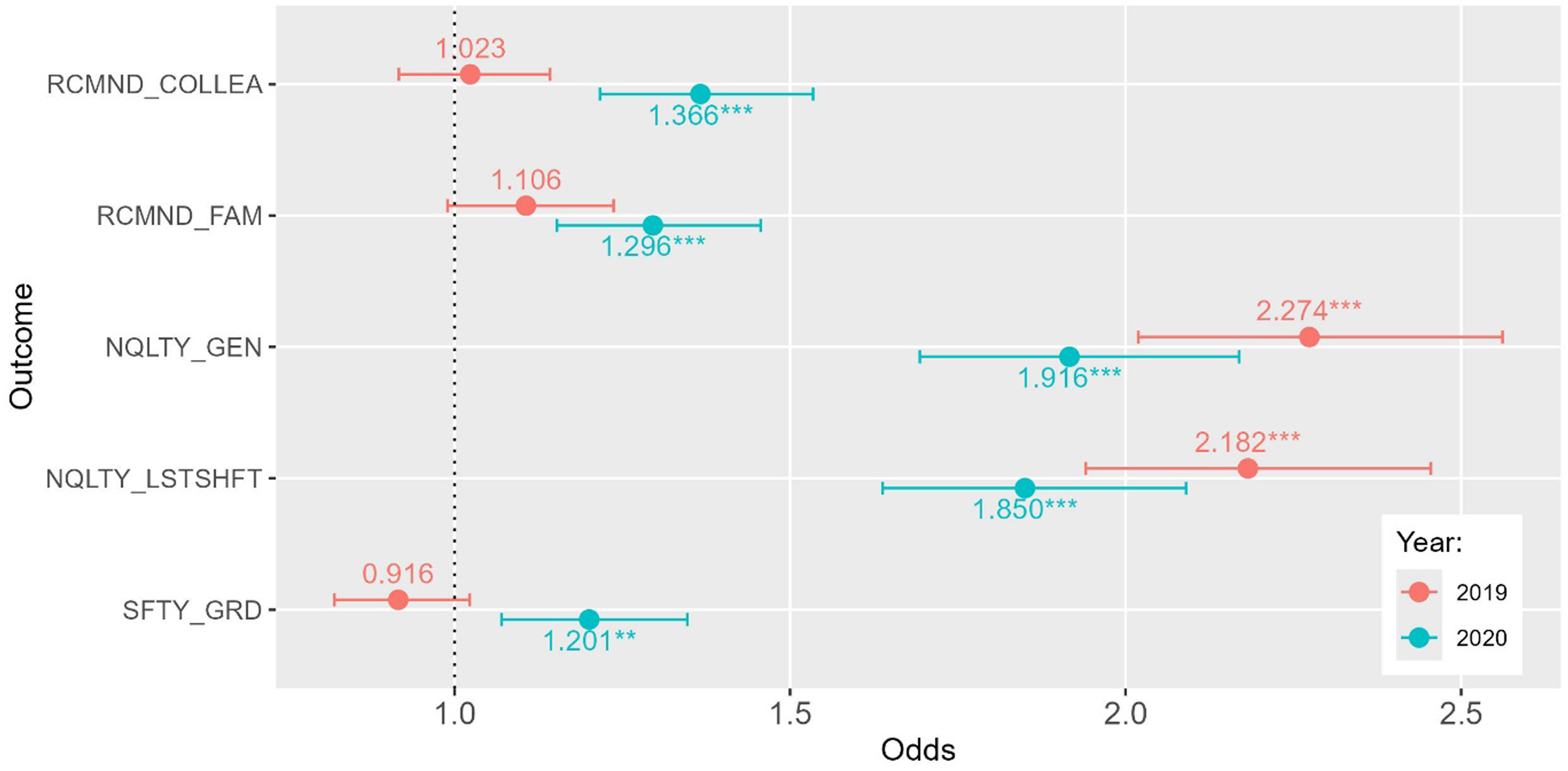
Odds (95% CI) of year 2019 and 2020 vs. 2015 (reference group). Note: Dots and crosses indicate the estimated odds, while horizontal bars depict the 95% confidence interval of these estimates. Significance levels: * represents p < .05, ** represents p < .01, *** represents p < .001. Regression of Emotional Exhaustion is not included because it is a general linear regression.
Regression Analysis: Control Variables
Nurses working in acute care and community care were more likely to recommend their unit or workplace for care compared to those in long-term care (odds e0.368 ≈ 1.4, p < .001 and odds e0.457 ≈ 1.6, p < .001, respectively). Community care nurses also rated general and last-shift nursing care quality (odds e0.241 ≈ 1.3, p < .05; odds e0.200 ≈ 1.2, p < .05) and overall safety grade (odds e0.264 ≈ 1.3, p < .01) higher than their long-term care counterparts.
Regarding nursing experience, nurses with all levels of experience reported higher emotional exhaustion than their most experienced peers with 21+ years of experience (odds e2.3 to odds e3.8 ≈ 9.9–42.9, p <.001 for all). Less-experienced nurses were also less likely to recommend their unit/workplace for care (odds e−0.532 to odds e−0.216 ≈ 0.6-.8, p < .001 to p < .05) and gave lower ratings for general and last-shift nursing care quality (odds e−0.550 to odds e−0.395 ≈ 0.6-.7, p < .001 to p < .05) and overall safety grade (odds e−0.324 to odds e−0.183 ≈ 0.7–0.8, p < .001 to p < .05), compared to the most experienced nurses.
Regarding gender, female nurses reported higher emotional exhaustion than male nurses (odds e1.335 ≈ 3.8, p < .05). However, they were more likely to recommend their workplace for employment (odds e0.205 ≈ 1.2, p < .05) and care (odds e0.289 ≈ 1.3, p < .001) and rated patient safety higher (odds e0.166 ≈ 1.2, p < .05).
For professional designation, no significant differences were found between LPNs and RNs/RPNs across all outcomes. Similarly, education level did not significantly impact most outcomes, except that nurses with a diploma or certificate were less likely to recommend their workplace for care compared to those with a graduate degree (odds e−0.170 ≈ 0.8, p < .05). Regarding employment status, full-time and part-time nurses reported higher emotional exhaustion than casual nurses (odds e4.304 ≈ 74.0 and odds e2.739 ≈ 15.5, p < .001 for both). Additionally, full-time nurses assigned lower overall patient safety grades compared to casual nurses (odds e−0.135 ≈ 0.9, p < .05).
Discussion
A key finding from this study was the rise in nurse emotional exhaustion from 2015 to 2020, with levels peaking during the COVID-19 pandemic. Paradoxically, despite this increase in emotional exhaustion, nurses reported higher ratings of Q/S in 2020 compared to 2015. Further, female nurses reported greater emotional exhaustion than male counterparts, although they gave more favorable ratings with respect to care Q/S.
Nurses’ increased emotional exhaustion over time may reflect cumulative stress from ongoing systems pressures and intensified workloads, particularly during COVID-19. Previous studies have shown how nurses working during epidemics and pandemics suffered increased stress due to secondary traumatic stress from working with infected, critically ill patients (Carmassi et al., 2020). Secondary traumatic stress is significantly associated with emotional exhaustion (Alshammari et al., 2024; Jeong & Shin, 2023). In addition to the findings from this study, other longitudinal studies reported mental health deterioration during the COVID pandemic, such as increases in secondary traumatic stress and psychological distress (Sasaki et al., 2021; Zhou et al., 2021).
Despite increased emotional exhaustion during the study's time period, participants reported improved Q/S ratings between 2015 and 2020. In 2019, nurses reported higher general and last shift quality of nursing care, but there were no significant differences in overall reported patient safety between 2015 and 2019. Increases in nurses’ quality of care reports across time points may be due to healthcare organizations’ enhanced efforts to educate staff about ongoing, evidence-based Q/S protocols. Beginning in 2014, the World Health Organization (WHO) announced a global patient Q/S initiative to enhance healthcare organizations’ uptake of standard operating protocols (SOPs) (Leotsakos et al., 2014). Since then, healthcare organizations’ accreditation standards have included enhanced efforts to educate staff and to implement SOPs intended to decrease patient safety challenges (Leotsakos et al., 2014). It may be that nurses’ reports of higher Q/S over time were reflections of their own practice and applications of new knowledge and skills; as where patient safety ratings may have been more influenced by their capacity to meet new patient safety mandates outside their professional control (e.g., use of ceiling lifts and additional staff to turn and maneuver patients).
In 2020, during the height of the COVID pandemic, many Q/S studies reported how Q/S indicators decreased due to insufficient resources to maintain aggressive infection control practices for patients and staff. For example, Fleisher et al. (2022) in a U.S. context, discussed stresses on health system safety during the pandemic. Similarly, Boone et al. (2023), in a U.S.-led integrative review of nurses’ well-being and safety during the pandemic found that insufficient Q/S planning and response increased nurses’ reports of anxiety, depression and moral distress. Our findings, therefore, are counter to what has been reported in the literature. Our explanation is that in BC, the public health officer was a highly visible leader making daily updates of public health provincial and regional initiatives (Shaban & Brunet-Jailly, 2022; Spoel et al., 2023). Communications networks and command/control sites ensured rapid deployment of resources with evidence-based rationale for Q/S policies and procedures. Most BC nurses had access early on to many COVID-specific Q/S practices and policies such as visitation restrictions, N95 masks, plexi-glass screens, and front entry visitor management (Spoel et al., 2023).
With respect to our study's gender difference findings, female nurses’ higher rates of emotional exhaustion may reflect greater pressure on them to fulfill public expectations and their own caregiving role expectations, both at work and at home. To illustrate, it was recently reported that more than half of Canadian women provide some form of paid or unpaid care for others (Statistics Canada, 2022). In an integrative review of nursing stereotypes (Teresa-Morales et al., 2022), a pervasive public stereotype is that nursing is an appropriate profession for women, given assumptions about women's innate capacity to care for others (a stereotype that is a common belief among nurses themselves) (Teresa-Morales et al., 2022). Given female nurses’ strong identification with the profession and duty to care, they may feel a greater obligation to ensure patients receive Q/S care. Our study showed that female nurses gave higher Q/S ratings to their work environments versus male nurses, and these higher ratings may reflect a greater sense of accountability for their caregiving roles. A recent cross-sectional study reported significant positive relationships between nursing self-image and quality of care with no differences for men or women (Grinberg & Sela, 2022). In contrast, our findings may indicate that in our study population, female nurses had a stronger sense of nursing self-image linked to their caregiving roles.
Our analysis also provided evidence in alignment with expected outcomes. For example, among the different workplace sectors, community care nurses consistently rated Q/S higher than LTC nurses. An integrative review of nursing work in the LTC sector found that nurses typically provide indirect care tasks, such as care coordination, and they carry out many non-nursing activities that are unrelated to their clinical knowledge and skills. Nurses in LTC have high levels of job dissatisfaction that may be associated with their LTC roles that encompass more indirect than direct care responsibilities (Aloisio et al., 2019). In contrast, in community care settings, nurses have considerable professional autonomy (Pursio et al., 2021). Professional autonomy includes nurses’ application of their knowledge and skills to make shared care decisions with their clients. For community care nurses, autonomy in making clinical decisions based on their own professional competence and judgment is closely aligned with increased quality of work (Pursio et al., 2021).
Finally, our study indicated that less experienced nurses reported significantly higher emotional exhaustion and poorer Q/S perceptions than their colleagues with more nursing experience. This finding may be explained by limited transition support and collegial relations and mentorship support available to less experienced nurses (Regan et al., 2017). Further, we did not find any significant differences in emotional exhaustion or Q/S ratings based on nurse designation (RN/RPN versus LPN). Both of these findings are consistent with previously reported literature, though it should be noted that the evidence is mixed (Li et al., 2013; Ramírez-Elvira et al., 2021; Whitehead et al., 2019).
Limitations
Despite addressing an important knowledge gap, this study has several key limitations. First, due to the absence of participant identifiers, respondents could not be linked across the three time points. Consequently, longitudinal analyses and multilevel modeling could not be conducted and the cross-sectional design at each time point limits our ability to examine within-individual changes over time and precludes causal inferences (Sedgwick, 2014). Second, although the overall sample size was relatively large, the low response rates in the broader surveys may restrict the generalizability of the findings beyond the study sample (Sataloff & Vontela, 2021). Third, the reliance on self-reported measures—particularly regarding perceptions of Q/S—introduces the potential for social desirability and recall bias (Bispo Júnior, 2022). Fourth, although gender identity was measured using inclusive response options, the very small number of participants selecting non-binary or non-disclosed categories precluded their inclusion in multivariable analyses due to concerns about unstable parameter estimates and model validity. This analytic decision was driven by statistical constraints rather than conceptual assumptions about gender and reflects broader methodological challenges in quantitatively analyzing gender-diverse populations when sample sizes are limited. Future studies with larger and more diverse samples are needed to support more robust and inclusive analyses of gender diversity in nursing workforce research. Finally, utilizing mixed methods and linking administrative data on Q/S with nurses’ self-reported assessments could help mitigate biases commonly associated with self-reported data (Canadian Institute for Health Information, 2024).
Implications
Despite these limitations, our key findings carry several important implications. Most notably, in light of the growing prevalence of nurse emotional exhaustion and its detrimental impact on workforce wellbeing and patient safety (Dall'Ora et al., 2020; Leiter et al., 2014; Maslach & Leiter, 2016; McHugh et al., 2011), we recommend that burnout and its three domains (e.g., emotional exhaustion) be adopted as a leading indicator of workforce health and workplace safety. This indicator should be routinely collected and integrated into standardized workforce data to inform health system planning and policy development at organizational and jurisdictional levels. In 2022, the Canadian Institute for Health Information refreshed its health workforce Minimum Data Standards (MDS), originally developed in 2012. Concurrently, the Canadian Health Workforce Network (CHWN) is leading a Canadian Institutes of Health Research (CIHR) funded initiative to co-develop an MDS specifically for planning purposes that is more inclusive and integrative of data elements, including indicators of workforce wellness such as burnout and self-reported mental health. As argued in nursing-specific workforce reports, including regular assessment and public reporting of burnout within the MDS would offer a more comprehensive understanding of workforce challenges and support targeted interventions for sustainable healthcare staffing (Ben-Ahmed & Bourgeault, 2022). Committed to a cyclical review process of their MDS, CIHI is working with the CHWN to explore opportunities to include these and other data elements in their 2025 update.
Our findings indicate that certain groups of nurses—particularly women, those with less experience, and those employed in LTC homes—are more susceptible to emotional exhaustion. This underscores the need for systems-level interventions that are responsive to the unique challenges these groups face. While evidence supports the effectiveness of certain targeted interventions (such as face-to-face group mindfulness sessions), they do not address the underlying and multifaceted causes of burnout (Dall'Ora et al., 2020). To meaningfully reduce the risk of burnout, interventions must focus on improving various aspects of the work environment (i.e., staffing inadequacies, mandatory overtime, poor working relationships, workplace violence).
Conclusion
The observed increase in nurses’ emotional exhaustion between 2015 and 2020 likely reflects the cumulative impact of persistent system pressures, escalating workloads, and the added demands of the COVID-19 pandemic. Notably, despite worsening emotional exhaustion, nurses’ ratings of the quality and safety of care improved over time, highlighting their continued commitment to maintaining care standards even under challenging conditions. However, this paradox should not be misinterpreted as resilience without consequences. Sustained emotional exhaustion poses significant risks to workforce stability, patient outcomes, and the overall performance of the healthcare system.
To support more sustainable workforce planning, it is critical that emotional exhaustion and other indicators of burnout be systematically measured, routinely monitored, and publicly reported as part of Canada's health workforce data infrastructure. Incorporating burnout metrics into national dashboards would enable more targeted, data-driven strategies to strengthen workforce well-being and healthcare system resilience.
Footnotes
Acknowledgements
The study authors would like to thank BC nurses for their participation in the three study surveys.
ORCID iDs
Ethical Considerations
This secondary analysis of data was approved by the University of British Columbia Behavioral Research Ethics Board (approval number: H24-02218).
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Authors FH contributed to the conceptualization and design of the study. Authors FH, CS, DZ, and MM prepared the first draft of the manuscript. Author DZ, FH, and AW conducted the data analysis and provided interpretations of the findings. All authors made significant revisions to the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This secondary data analysis was not supported by any funding. However, the original studies received financial support as follows: The 2015 survey was funded by the BC Nurses’ Union and the Collaborative Alliance for Nurse Outcomes. The 2019 survey was funded by the Social Sciences and Humanities Research Council of Canada, with in-kind support from the BC Nurses’ Union. The 2020 survey was funded by the BC Nurses’ Union.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Provenance and Peer Review
Not commissioned, externally peer reviewed.
Data Availability Statement
No data are available.