
Abstract
Acute non-traumatic urinary tract emergencies are a frequent cause of emergency department presentation and may result in significant morbidity if not promptly diagnosed. Imaging plays a pivotal role in identifying the underlying pathology, assessing disease severity, and guiding patient management. This review provides a comprehensive imaging-based overview of the most common acute non-traumatic urinary tract emergencies. Obstructive, infectious, vascular, and hemorrhagic conditions, as well as urinary leaks, are discussed with emphasis on their characteristic imaging findings. The roles of ultrasound, computed tomography, and magnetic resonance imaging are reviewed, highlighting appropriate modality selection in the emergency setting. In addition, the emerging role of photon-counting computed tomography (PCCT) is discussed. Owing to its improved spatial resolution, enhanced tissue contrast, and spectral imaging capabilities, PCCT may allow better detection of subtle parenchymal abnormalities, small calculi, vascular alterations, and urinary leaks, while potentially enabling dose optimization. Key diagnostic features, common pitfalls, and practical reporting considerations are presented to assist radiologists in achieving timely and accurate diagnoses. This review aims to support a systematic and clinically relevant imaging approach to acute non-traumatic urinary tract emergencies.
Introduction
Acute non-traumatic urinary tract emergencies are a frequent and clinically significant cause of emergency department presentation, often manifesting with nonspecific symptoms such as flank pain, hematuria, and fever.1-5 These conditions encompass a wide range of pathologies, including obstructive, infectious, vascular, hemorrhagic disorders, and urinary leaks, which frequently share overlapping clinical features and complicate prompt diagnosis.1-11 Delayed or missed diagnosis may lead to severe complications, including irreversible renal injury, sepsis, hemorrhagic shock, and increased mortality. Early identification is therefore critical for both immediate patient stabilization and long-term renal preservation.1-25 Given the nonspecific clinical presentation, imaging plays a central role in diagnosis and management. Ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI) provide complementary information. Ultrasound is commonly used as a first-line modality, particularly in vulnerable populations, whereas CT remains the cornerstone of acute evaluation due to its speed, high spatial resolution, and comprehensive assessment. MRI serves as a problem-solving tool in selected cases.26-31 Recent advances such as photon-counting CT (PCCT) may further enhance diagnostic performance by improving spatial resolution, contrast-to-noise ratio, and material differentiation, facilitating the detection of subtle abnormalities while potentially optimizing radiation dose.31-41 Although still limited in availability, early evidence suggests improved diagnostic confidence in acute urinary tract imaging.33,44-46 This review provides a structured, imaging-focused overview of acute non-traumatic urinary tract emergencies, emphasizing modality selection, key imaging findings, diagnostic pitfalls, and practical reporting strategies to support timely and accurate diagnosis.
Imaging Modalities in the Emergency Setting
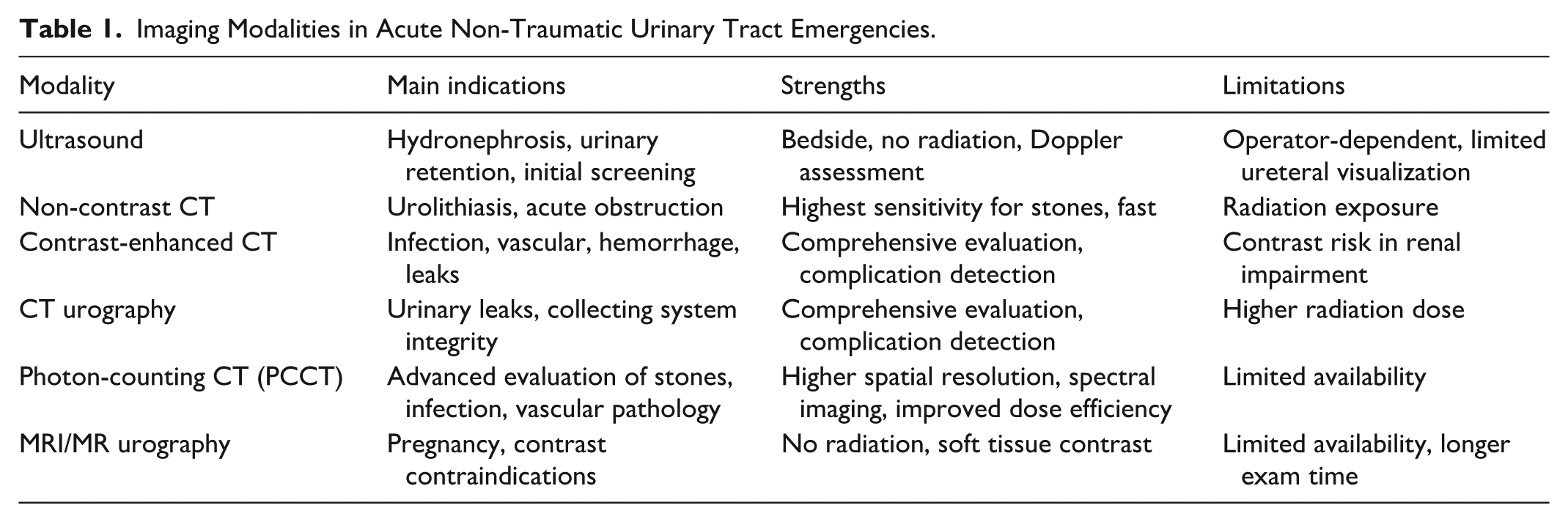
Accurate and timely imaging is essential in the assessment of acute non-traumatic urinary tract emergencies, both for diagnosis and for guiding management decisions. The choice of modality depends on the suspected pathology, patient characteristics, availability of equipment, and potential contraindications. Ultrasound (US), computed tomography (CT), and magnetic resonance imaging (MRI) serve complementary roles in this context, with recent technological advances such as photon-counting CT (PCCT) offering additional promise in improving image quality while reducing radiation dose (Table 1).26-41
Imaging Modalities in Acute Non-Traumatic Urinary Tract Emergencies.
Ultrasound (US)
Ultrasound is frequently the first-line imaging modality in patients with suspected urinary tract emergencies. Its widespread availability, rapid bedside applicability, and lack of ionizing radiation make it particularly suitable for vulnerable populations, including pregnant women, children, and patients with renal impairment. US is especially useful for the initial assessment of hydronephrosis, bladder distension, urinary retention, and renal size, as well as for the detection of large renal calculi and perinephric fluid collections.9,21,26,30,47 Gray-scale US provides evaluation of renal parenchymal echotexture, collecting system dilatation, cortical thickness, and perinephric fluid or hematoma. Color and power Doppler imaging add functional information, allowing assessment of renal perfusion, arterial and venous flow, and vascular patency. This is particularly valuable in suspected renal infarction or renal vein thrombosis, where absent or altered flow may serve as an early diagnostic clue.9,16,21,26,30,47-50 Despite its advantages, US is operator-dependent and can be limited by patient body habitus, overlying bowel gas, and difficulty visualizing the mid and distal ureters. Small calculi, early infectious changes, and subtle obstruction may be missed. Nevertheless, US is often used as a screening tool, guiding subsequent cross-sectional imaging with CT when findings are equivocal or complications are suspected.
Computed Tomography (CT)
CT remains the cornerstone imaging modality for adult patients with acute non-traumatic urinary tract emergencies due to its high spatial resolution, rapid acquisition, and ability to comprehensively evaluate the kidneys, ureters, bladder, and surrounding retroperitoneum.1-12,19-31,40,51 Non-contrast CT is the gold standard for detecting urinary calculi. It accurately determines stone size, composition (via attenuation), location, and secondary signs of obstruction, such as hydronephrosis, perinephric stranding, or ureteral wall thickening. Non-contrast CT is rapid, highly sensitive, and not limited by patient body habitus, making it the preferred first-line modality in adults presenting with acute flank pain. Contrast-enhanced CT, including “multiphasic protocols,” is essential for evaluating infectious, vascular, hemorrhagic, and neoplastic conditions. Typical phases include:
Non-contrast phase: for baseline attenuation and detection of calculi or hemorrhage
Corticomedullary phase: evaluates renal vascular supply and parenchymal perfusion
Nephrographic phase: highlights parenchymal lesions and infections
Excretory phase: allows assessment of the collecting system and urinary leaks (CT urography)
To optimize diagnostic yield while reducing radiation exposure, “split-bolus techniques” may be employed. In this approach, contrast material is administered in 2 sequential injections separated by a timed delay, allowing simultaneous visualization of the nephrographic and excretory phases in a single acquisition. Split-bolus CT is particularly useful in the emergency setting, as it provides combined evaluation of renal parenchyma and the urinary collecting system while minimizing scan time and cumulative radiation dose. This technique is well suited for suspected urinary tract obstruction, urothelial pathology, or urinary leaks when comprehensive assessment is required but full multiphasic imaging is undesirable. CT also identifies perinephric collections, renal infarctions, gas-forming infections such as emphysematous pyelonephritis, and spontaneous hemorrhage. Low-dose CT protocols are increasingly utilized to minimize radiation exposure, particularly in patients with recurrent stones or young adults. However, contrast administration must be carefully considered in patients with renal impairment or history of contrast allergy.1-12,19-31,40,51
Photon-Counting CT (PCCT)
PCCT represents a major advancement in CT technology, offering improved spatial and contrast resolution with the potential for radiation dose reduction. In genitourinary emergencies, PCCT may allow better differentiation of urinary stone composition, improved detection of subtle renal parenchymal abnormalities, and enhanced visualization of small urinary leaks or vascular abnormalities. Beyond improved spatial resolution, its added value lies in detector-based spectral imaging and quantitative analysis, which may support the assessment of infectious, inflammatory, vascular, and oncological conditions presenting as GU emergencies. Early clinical studies suggest that PCCT may increase diagnostic confidence while reducing radiation burden, a particularly relevant advantage in emergency imaging, where rapid and high-quality diagnosis is essential.31-45,51-54
Magnetic Resonance Imaging (MRI)
MRI plays a complementary but limited role in the acute emergency setting. Its principal advantages are excellent soft tissue contrast and absence of ionizing radiation, making it valuable when CT is contraindicated, such as in pregnancy or in patients with severe contrast allergy.16,28,44,55-59 Magnetic Resonance urography can delineate urinary obstruction, evaluate collecting system integrity, and detect urinary leaks. Diffusion-weighted imaging (DWI) provides functional information, highlighting areas of restricted diffusion in renal infections or infarctions. MRI is particularly useful for characterizing renal masses, vascular abnormalities, and complex infections without exposing patients to radiation.16,28,44,55-59 Limitations of MRI include longer acquisition times, susceptibility to motion artifacts, limited availability in emergency settings, and difficulties in unstable patients. Nevertheless, in select scenarios, MRI can prevent radiation exposure, clarify equivocal CT findings, or serve as a problem-solving tool for complicated renal and urinary tract conditions.
Acute Obstructive Conditions
Obstruction of the urinary tract represents a common and potentially serious cause of acute non-traumatic pain in Emergency Department patients. Timely recognition and characterization are critical because sustained obstruction can lead to acute kidney injury, infection, and permanent renal damage. Acute obstruction may be calculous or non-calculous, with varying imaging features and management considerations (Table 2).
Acute Obstructive Urinary Tract Emergencies.

Urolithiasis
Urolithiasis is the most prevalent cause of acute non-traumatic urinary tract obstruction, accounting for a substantial proportion of emergency presentations for flank pain. The lifetime incidence of urinary stone disease is approximately 10% to 15%, with a higher prevalence in men and a peak occurrence in the 30 to 50-year. 7 Predisposing factors include dehydration, metabolic disorders, dietary influences, obesity, urinary tract infections, and genetic susceptibility. Stones can form throughout the urinary tract, from the renal calyces and pelvis to the ureters and urinary bladder.
Imaging Evaluation
Non-contrast CT (NCCT) is the modality of choice, offering very high sensitivity and specificity for stone detection. Stones appear as hyperattenuating foci within the collecting system or ureter. CT also reveals secondary signs of obstruction, including: Hydronephrosis (pelvicalyceal dilatation) Perinephric fat stranding Ureteral wall thickening or edema Delayed or asymmetric contrast excretion on multiphase imaging
Stone size, density, and location inform management decisions. Stones smaller than 5 mm often pass spontaneously, whereas stones larger than 10 mm or those impacted at anatomical narrowing points frequently require intervention, including ureteroscopy, extracorporeal shockwave lithotripsy, or percutaneous extraction. Dual-Energy CT (DECT) provides additional functional and compositional information by acquiring datasets at 2 different X-ray energy levels. DECT enables reliable differentiation between uric acid and non–uric acid stones based on their material-specific attenuation properties, which has direct therapeutic implications, as uric acid calculi may be managed conservatively with urine alkalinization. DECT may also improve stone conspicuity in challenging locations and assist in predicting response to shockwave lithotripsy. With modern protocols, radiation dose is generally comparable to standard NCCT. Photon-Counting CT (PCCT) is an emerging CT technology that directly converts individual X-ray photons into electrical signals and sorts them by energy. Compared with conventional energy-integrating CT systems, PCCT offers higher spatial resolution, reduced image noise, and enhanced spectral separation. In urolithiasis, PCCT improves detection of very small calculi, better delineates stones adjacent to dense structures, and allows more accurate characterization of stone composition. Intrinsic spectral information may enable material differentiation similar to, or exceeding, that of dual-energy CT, potentially at equal or lower radiation dose.32-46,60-62 Ultrasound (US) is a radiation-free option, particularly in pregnant patients and children. Stones appear as echogenic foci with posterior acoustic shadowing, and the color Doppler “twinkling artifact” may help identify small stones. Hydronephrosis is an important indirect sign of obstruction. However, US is less sensitive for distal ureteral calculi, small stones (less than 3 mm), and is limited by patient body habitus and bowel gas.9,21,26,30,47,63,64 Magnetic Resonance Imaging (MRI) is rarely used for direct stone detection, as calculi are typically hypointense and may be overlooked. However, MR urography can reveal secondary signs of obstruction, including collecting system dilatation, renal edema, and impaired excretory function. MRI is mainly reserved for problem-solving in patients with contraindications to CT or in radiation-sensitive populations.16,28,44,55-59,65
Pitfalls
Small distal ureteral stones may be missed on ultrasound.
Radiolucent stones, particularly uric acid calculi, may appear subtle on conventional NCCT; dual-energy CT and photon-counting CT improve detection and compositional assessment.
Hydronephrosis may persist after spontaneous stone passage, potentially mimicking ongoing obstruction and requiring careful clinical correlation.
Acute Hydronephrosis
Acute hydronephrosis results from sudden obstruction of urinary outflow, causing retrograde dilatation of the renal pelvis and calyces. If unrecognized, prolonged obstruction can lead to acute kidney injury and permanent parenchymal damage. Causes include calculi, blood clots, strictures, tumors, and extrinsic compression from adjacent structures such as lymphadenopathy or retroperitoneal masses.
Imaging Features
Ultrasound is highly effective in detecting pelvicalyceal dilatation, renal cortical thinning, and perinephric fluid. Doppler assessment can reveal alterations in renal perfusion in cases of severe obstruction. CT provides superior anatomic detail, allowing precise localization of the obstruction, characterization of the underlying cause, and detection of associated complications such as infection or hemorrhage. Delayed contrast-enhanced images may demonstrate impaired or absent excretion in the affected kidney.1-12,19-31,40,51 MRI may be used in select cases to evaluate obstruction in radiation-sensitive populations, showing collecting system dilatation, parenchymal edema, and functional excretory impairment.16,28,44,55-57
Reporting Recommendations
Radiology reports should systematically describe:
Degree of hydronephrosis (mild, moderate, severe)
Laterality (unilateral or bilateral)
Cause of obstruction (stone, tumor, clot, stricture, external compression)
Associated complications (infection, parenchymal thinning, perinephric collection)
Recommendation for follow-up or intervention, if indicated
Non-Calculous Obstruction
Non-calculous obstruction can arise from malignancy, retroperitoneal fibrosis, or intraluminal blood clots. Though less common than calculous obstruction, prompt recognition is crucial, as these conditions may progress rapidly or be associated with significant morbidity.
Imaging Features
CT is the preferred modality, providing excellent evaluation of intrinsic and extrinsic causes of obstruction.1-12,19-31,40,51 It identifies: (1) Hyperattenuating filling defects (blood clots) within the collecting system. (2) Soft tissue masses causing intrinsic obstruction (tumors). (3) Extrinsic compression from retroperitoneal fibrosis, lymphadenopathy, or adjacent masses. Blood clots appear as hyperattenuating intraluminal material on NCCT and may be associated with hematuria or recent instrumentation. Differentiation from tumors is critical, as the management and prognosis differ significantly. In ambiguous cases, follow-up imaging, cystoscopy, or contrast-enhanced evaluation may be necessary.
Pitfalls
Intraluminal blood clots can mimic calculi or neoplasms. Retroperitoneal fibrosis may be subtle early, requiring careful review of perinephric and ureteral soft tissues. Bilateral obstruction from non-calculous causes may present subtly but has high risk of acute renal failure, necessitating urgent recognition.
Clinical Implications
Identification of the underlying etiology directs management—stones may require extraction, clots may resolve spontaneously or require intervention, and tumors or fibrosis necessitate oncologic or surgical referral. Radiologists must clearly communicate the level and suspected cause of obstruction, potential complications, and urgency for intervention.
Acute Infectious Emergencies
Acute Pyelonephritis
Acute pyelonephritis is a bacterial infection of the renal parenchyma and collecting system, commonly presenting with fever, flank pain, and urinary symptoms. Imaging is not routinely required in uncomplicated cases but is indicated in patients with severe illness, immunocompromised population, or patients with poor response to therapy. Contrast-enhanced CT typically demonstrates wedge-shaped areas of decreased enhancement, renal enlargement, and perinephric fat stranding.1-12,19-31,40,51 MRI with DWI may show restricted diffusion in affected areas.16,28,44,55-57 Photon-counting CT (PCCT) may improve the evaluation of acute pyelonephritis (Figure 1) by enabling earlier detection of renal parenchymal abnormalities and a more accurate delineation of the extent of infection. Owing to its higher spatial resolution and improved contrast-to-noise ratio, PCCT can better depict subtle inflammatory changes, such as wedge-shaped areas of decreased enhancement and striated nephrogram patterns. In addition, the enhanced image quality may facilitate earlier recognition of complications, including renal or perinephric abscesses and collecting system involvement. These features may ultimately increase diagnostic confidence, particularly in atypical or complicated presentations of acute pyelonephritis, and may contribute to a more precise assessment of disease severity and extent (Table 3). Complicated pyelonephritis includes abscess formation, gas production, or obstruction. Emphysematous pyelonephritis is a life-threatening condition characterized by gas within the renal parenchyma, collecting system, or perinephric space, most commonly in diabetic patients. CT is the modality of choice, allowing classification of disease extent and guiding management decisions, including percutaneous drainage or nephrectomy.
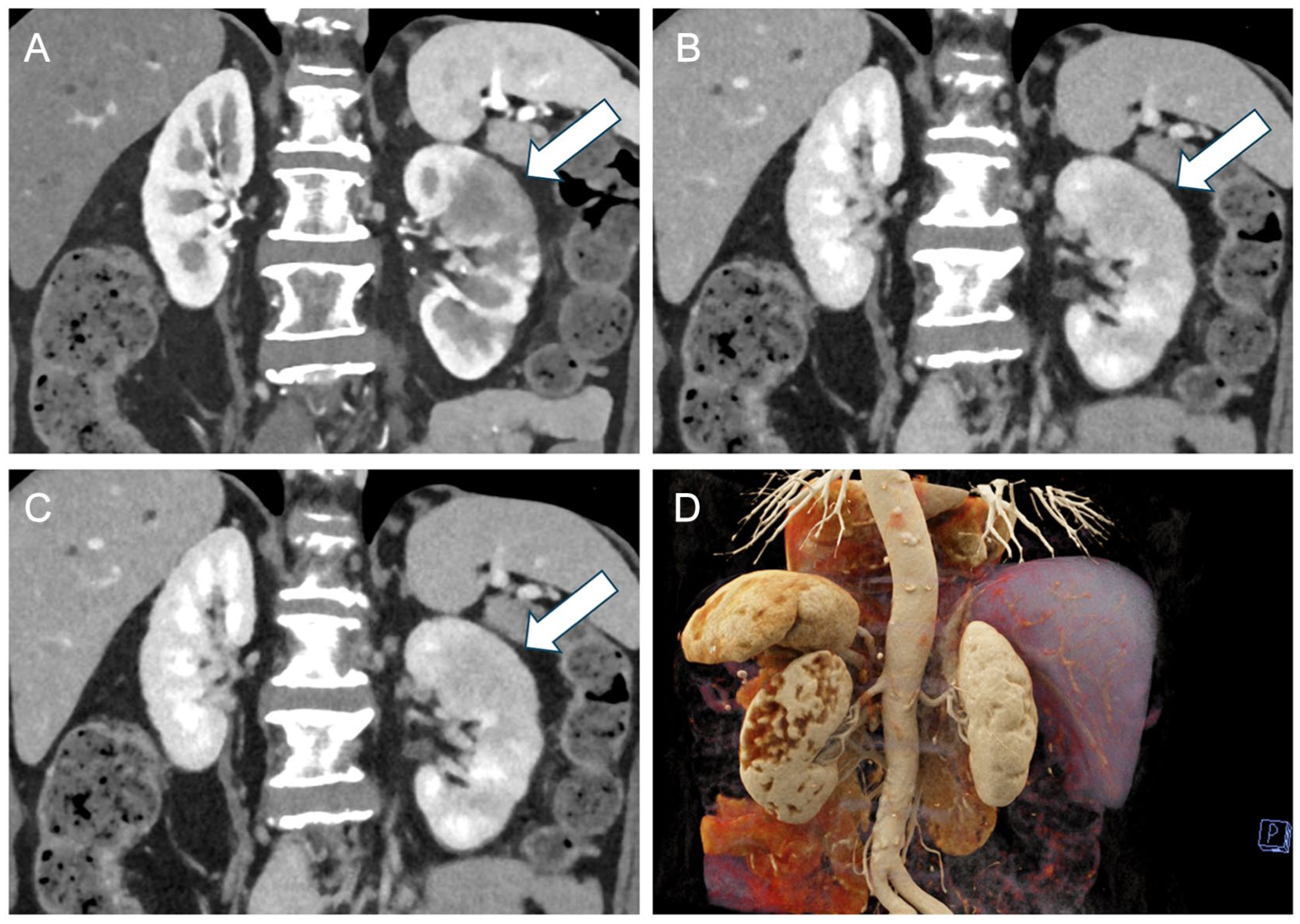
A 60-year-old woman presenting with fever, left flank pain, and dysuria. (A-C) Coronal MPR reconstructions from contrast-enhanced Photon-Counting CT obtained during the arterial, venous, and excretory phases demonstrate an enlarged left kidney with multiple wedge-shaped areas of reduced perfusion, most prominent in the upper-mid third (arrow), consistent with acute pyelonephritis. (D) Volume-rendered reconstruction (posterior view) from the portal venous phase shows surface irregularity of the left kidney corresponding to the previously described areas of decreased vascularity.
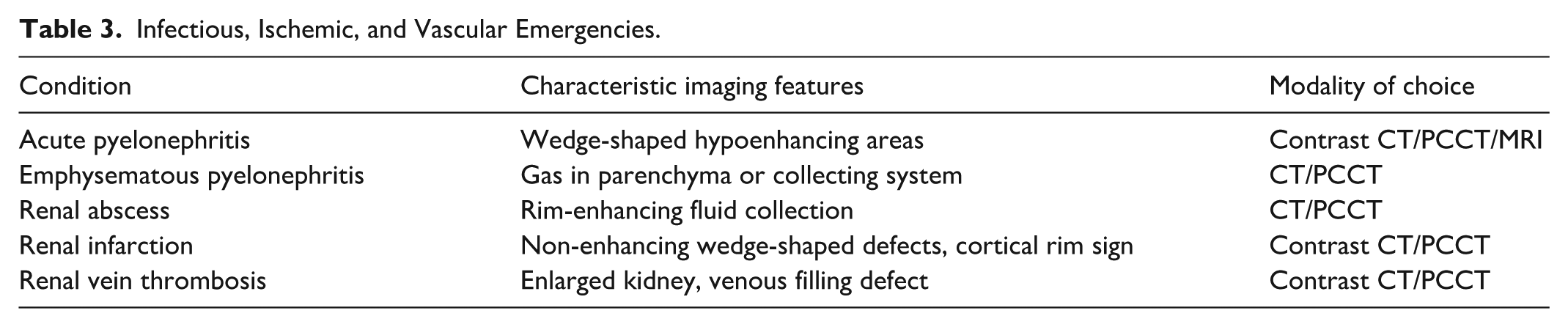
Infectious, Ischemic, and Vascular Emergencies.
Renal and Perinephric Abscess
Renal and perinephric abscesses may arise as complications of untreated pyelonephritis. CT findings include rim-enhancing fluid collections with surrounding inflammatory changes. Prompt diagnosis is critical, as management often requires drainage in addition to antibiotics.
Ischemic and Vascular Emergencies
Vascular and ischemic pathologies of the kidney, though relatively uncommon, constitute critical non-traumatic emergencies due to their potential to cause irreversible renal injury, systemic complications, and death if unrecognized. These conditions include renal infarction, renal vein thrombosis, and spontaneous renal hemorrhage. Early diagnosis relies heavily on imaging, particularly contrast-enhanced CT, with MRI and ultrasound serving complementary roles in select scenarios. PCCT can improve the evaluation of renal vascular emergencies such as renal infarction, renal artery thrombosis or embolism, vasculitis, and renal vein thrombosis. Thanks to its higher spatial resolution and improved contrast-to-noise ratio, PCCT enhances the detection of small wedge-shaped perfusion defects and subtle parenchymal hypoenhancement. In addition, the intrinsic spectral capabilities of PCCT allow the generation of iodine maps, which facilitate the identification of renal perfusion abnormalities and help distinguish true ischemia from inflammatory conditions such as acute pyelonephritis. PCCT also improves visualization of the renal arterial and venous systems, enabling better detection of segmental vascular occlusions and thrombi. Overall, these features may increase diagnostic confidence and allow earlier recognition of renal ischemic injury, which is essential for timely management (Figure 2; Table 3).
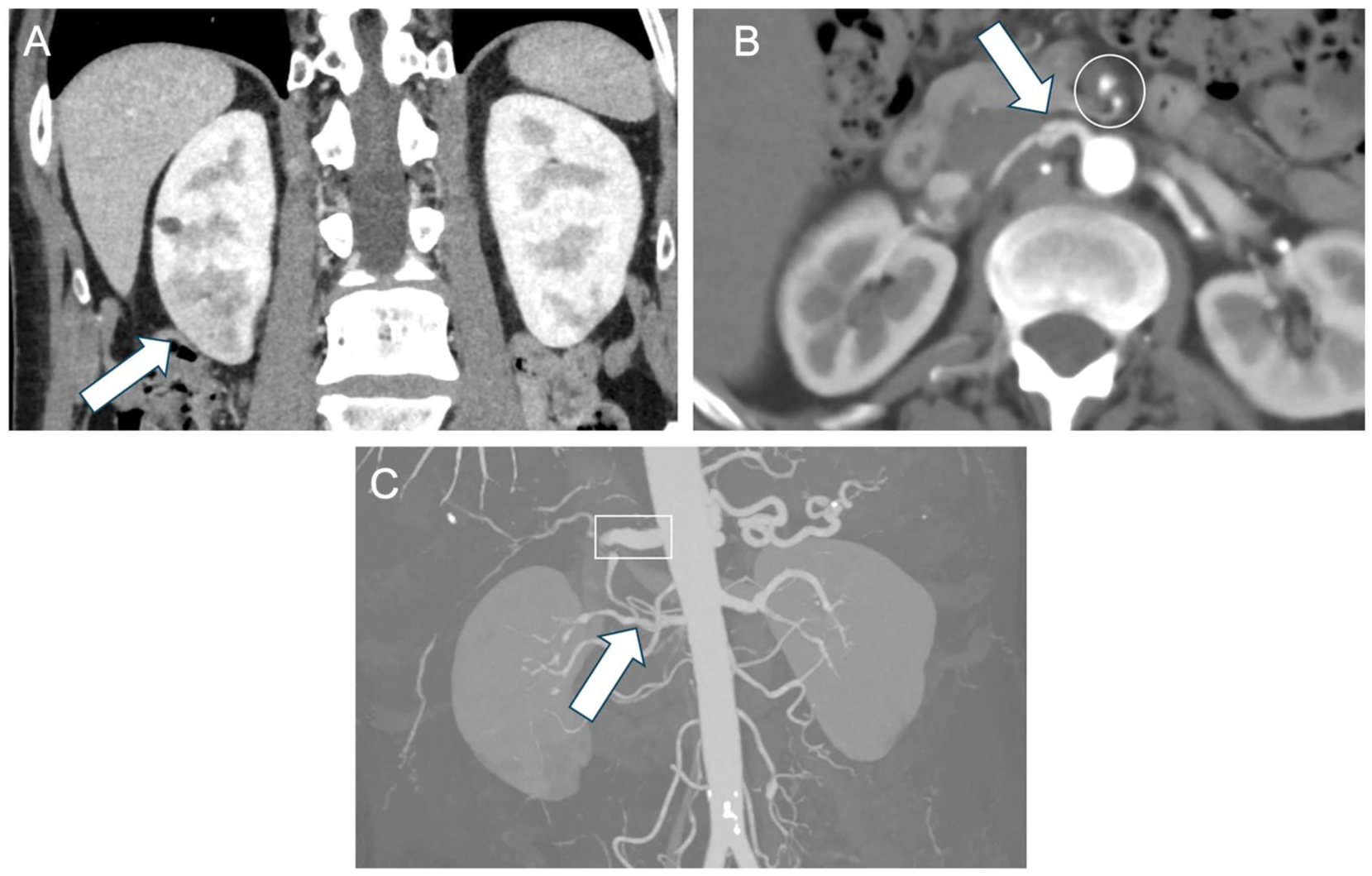
A 56-year-old man presenting with vague abdominal pain. (A) Coronal MPR images from venous-phase contrast-enhanced Photon-Counting CT shows wedge-shaped areas of decreased perfusion in the lower renal poles, more pronounced on the right (arrow), consistent with renal ischemia. (B, C) Axial and coronal thin- and thick-slab MIP reconstructions from contrast-enhanced photon-counting CT obtained during the arterial phase demonstrate multiple vascular abnormalities. These include circumferential wall thickening of the superior mesenteric artery (circle), irregular caliber of the common hepatic artery with upstream dilation preceding a marked pre-occlusive stenosis (rectangle), and a pseudoaneurysmal irregularity of the right renal artery (arrows). These findings are consistent with vasculitis, later confirmed.
Renal Infarction
Renal infarction occurs when renal arterial blood flow is acutely interrupted, leading to ischemia and necrosis of the renal parenchyma. The condition is uncommon but frequently misdiagnosed as urolithiasis or acute pyelonephritis due to overlapping clinical presentations.
Etiologies include:
Cardioembolic events: atrial fibrillation, mural thrombus post-myocardial infarction.
Atheroembolic disease: cholesterol crystal emboli in elderly patients with vascular disease.
Hypercoagulable states: inherited thrombophilias, malignancy, or antiphospholipid syndrome.
Renal artery dissection or trauma (rare non-traumatic spontaneous dissections)
Clinical Presentation
Patients typically present with sudden, severe flank or abdominal pain, nausea, vomiting, and sometimes hematuria. Fever may occur, mimicking infection. Laboratory evaluation often shows elevated lactate dehydrogenase (LDH) due to tissue necrosis, leukocytosis, and mild elevation in serum creatinine.
Imaging Features
Contrast-enhanced CT (CECT) is the modality of choice. Typical findings include: Wedge-shaped, sharply demarcated areas of non-enhancement within the renal cortex Cortical rim sign: a thin peripheral rim of capsular enhancement representing preserved subcapsular perfusion from collateral vessels Possible renal enlargement or perinephric stranding in acute cases
CT angiography (CTA) can identify occluded segmental or main renal arteries, helping guide interventional thrombolysis or surgical management.66-68
MRI with contrast or diffusion-weighted imaging can also detect infarction, showing restricted diffusion in the affected parenchyma, and is useful in patients with renal dysfunction or contrast allergy.69-71
Pitfalls
Early infarction may be subtle on imaging and mistaken for pyelonephritis
Small segmental infarcts may be overlooked on US or non-contrast CT
Misinterpretation can delay anticoagulation or revascularization therapy
Management Implications
Prompt anticoagulation is indicated for embolic or hypercoagulable causes
Endovascular intervention may be considered in large or bilateral infarcts
Recognition is essential to preserve renal function and prevent systemic embolic complications
Renal Vein Thrombosis
Renal vein thrombosis (RVT) is a rare but potentially serious cause of acute renal impairment, particularly in adults with nephrotic syndrome, malignancy, or hypercoagulable disorders.
Clinical Presentation
Symptoms are often subtle or nonspecific, including flank pain, hematuria, proteinuria, and acute kidney injury. Bilateral involvement may present with rapid-onset renal failure.
Imaging Features
CT with contrast is preferred, showing:
Pitfalls
RVT may mimic pyelonephritis or obstruction, particularly when flank pain and hematuria are present
Subtle thrombosis may be missed without contrast imaging
Management Implications
Anticoagulation is the mainstay of therapy
Treatment of underlying nephrotic syndrome, malignancy, or hypercoagulable state is essential
Severe or bilateral thrombosis may require interventional thrombectomy or thrombolysis
Spontaneous Hemorrhage and Urinary Leaks
Spontaneous Renal Hemorrhage (Wunderlich Syndrome)
Spontaneous renal hemorrhage is defined as non-traumatic bleeding into the subcapsular or perinephric space (Figures 3 and 4). It is most often associated with:
Renal neoplasms (angiomyolipoma, renal cell carcinoma)
Vascular abnormalities (aneurysms, arteriovenous malformations)
Systemic causes (anticoagulation therapy, coagulopathy)
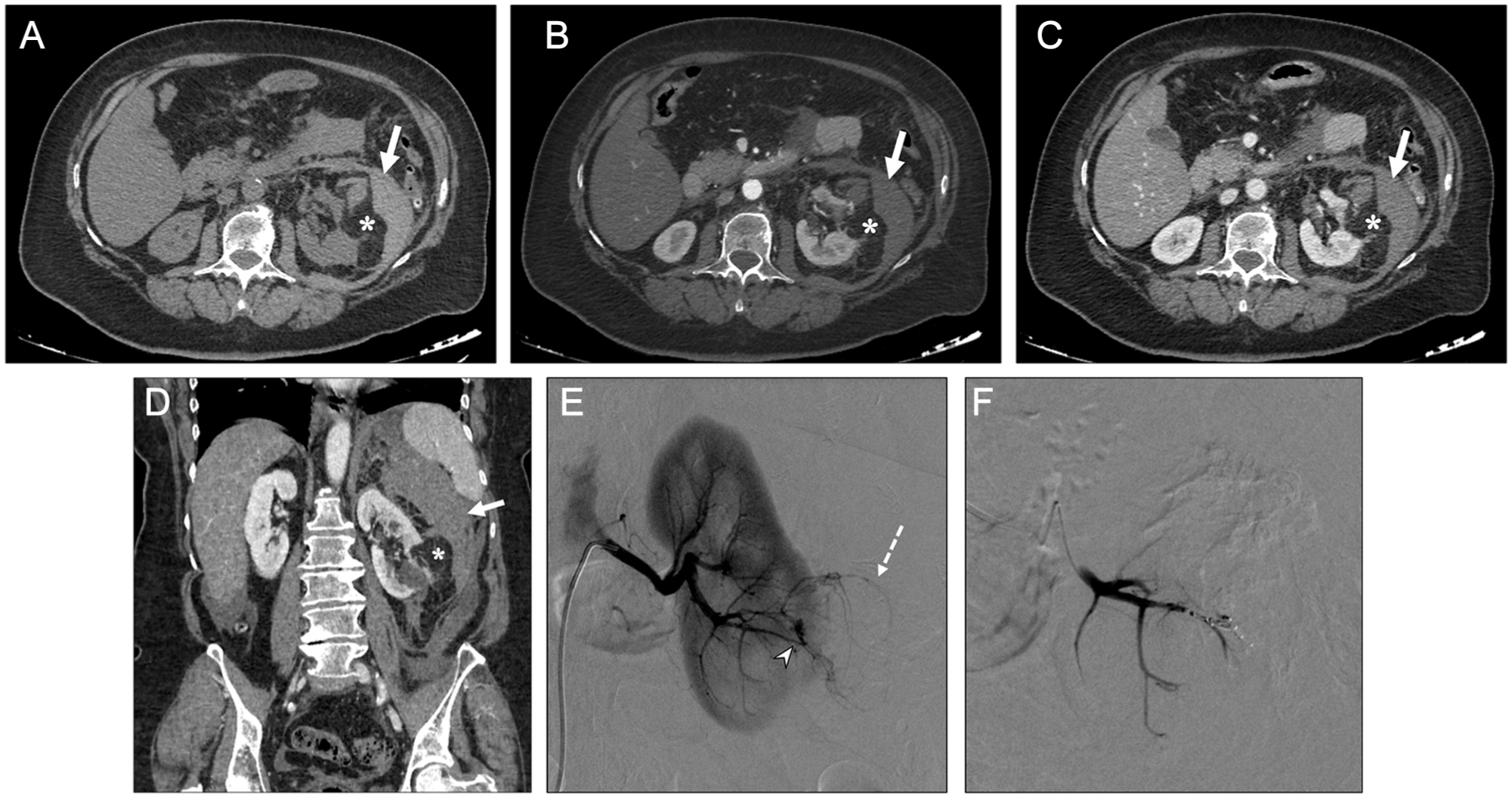
A 76-year-old woman. Axial unenhanced (A), contrast-enhanced arterial (B), and venous (C) phase CT images, together with a coronal venous-phase reconstruction (D), show a fat-containing mass arising from the inferior pole of the left kidney (asterisk in A-D), associated with extensive perirenal, anterior pararenal, and posterior pararenal hematoma (arrow in A-D), consistent with Wunderlich syndrome secondary to rupture of a renal angiomyolipoma. Digital subtraction angiography (DSA) (E) confirms a hypervascular lesion in the lower third of the left kidney corresponding to the angiomyolipoma (dotted arrow in E), with a pseudoaneurysm arising from a feeding vessel originating from an arcuate branch of the inferior segmental renal artery (arrowhead in E). Superselective coil embolization of the feeding arcuate artery was successfully performed (F).
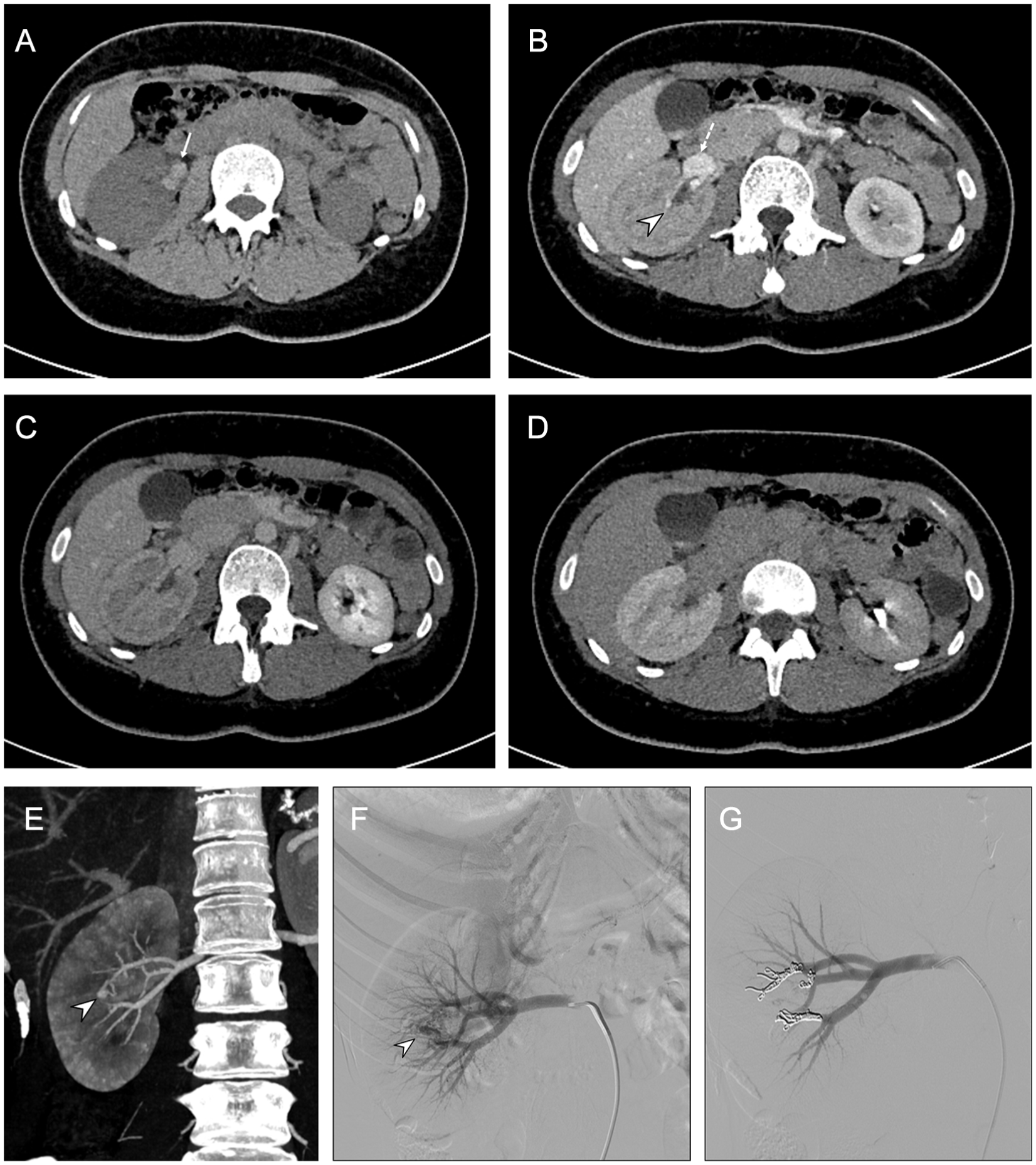
A 24-year-old woman presenting with acute flank pain and hematuria. Unenhanced CT (A) shows hyperdense material within the right renal pelvis (thin arrow in A). Contrast-enhanced CT in the corticomedullary phase (B) demonstrates an enhanced vascular tangle in the renal sinus (arrowhead in B) with early opacification of the right renal vein (dotted arrow in B), consistent with a renal arteriovenous malformation. A delayed nephrogram with absence of iodinated urine excretion up to 20 minutes is observed (C, D). Follow-up CT performed 6 hours later shows a striated nephrogram and intraparenchymal arteriovenous malformations (arrowhead in E) (E). Digital subtraction angiography (DSA) confirms a high-flow renal arteriovenous malformation (arrowhead in F) supplied by arcuate arteries arising from both anterior and posterior segmental branches (F). Selective coil embolization of the feeding interlobar arteries was performed (G).
Clinical Presentation
Patients present acutely with flank or abdominal pain, palpable mass, hematuria, and sometimes hypotension or hemorrhagic shock. The classic Lenk triad includes pain, mass, and hypotension.
Imaging Features
CT with contrast is essential for diagnosis:
Pitfalls
Hematomas may obscure underlying tumors
Early hemorrhage may appear isodense on NCCT, requiring contrast or follow-up imaging
Misdiagnosis may delay urgent intervention
Management Implications
Hemodynamically unstable patients require resuscitation and possible surgical intervention
Embolization may control bleeding from vascular lesions
Identification of underlying neoplasm is critical for oncologic management
Spontaneous hemorrhage and urinary leaks represent urgent non-traumatic conditions of the urinary tract that can lead to rapid deterioration of renal function, infection, or hemodynamic instability. Timely recognition through imaging is crucial, as clinical presentation is often nonspecific and may mimic other abdominal or genitourinary pathologies (Table 4).77-80
Hemorrhage and Urinary Leaks.

Urinary Tract Rupture and Urinoma Formation
Urinary tract rupture occurs when there is a breach in the integrity of the renal collecting system, ureter, or bladder. This leads to extravasation of urine into the perinephric, retroperitoneal, or even intraperitoneal space, forming a urinoma.
Etiology
Acute obstruction: Ureteral calculi are the most common cause, leading to increased intraluminal pressure and eventual rupture
Iatrogenic injury: Post-instrumentation (eg, ureteroscopy, catheterization) or surgical trauma
Spontaneous rupture: Rarely occurs in the context of infection, malignancy, or weakened urinary tract walls
Other causes: Pelvic radiation, retroperitoneal fibrosis, or chronic obstruction
Pathophysiology
Obstruction increases intraluminal pressure, which initially dilates the collecting system. If pressure exceeds the tensile strength of the urothelium, urine leaks into surrounding spaces, causing local inflammation, fibrosis, and potentially infection. Persistent urinomas can compress adjacent structures and impair renal function.
Clinical Presentation
Symptoms are variable and nonspecific, often including:
Flank or abdominal pain
Nausea and vomiting
Low-grade fever if secondary infection develops
Occasionally, hematuria or urinary retention
Because symptoms overlap with renal colic, pyelonephritis, or gastrointestinal conditions, imaging plays a critical role in accurate diagnosis.
Imaging Evaluation
CT urography (CTU) is the gold standard for detecting urinary leaks and urinomas. Key imaging findings include1-12,19-31,40,51:
Delayed contrast extravasation from the collecting system, ureter, or bladder
Urinoma formation, appearing as well-defined fluid collections with attenuation similar to urine (5-20 HU)
Perinephric fat stranding and inflammatory changes surrounding the collection
Hydronephrosis or upstream obstruction indicating the underlying cause
Protocol Considerations
Multiphasic CT is recommended, including non-contrast, corticomedullary, nephrographic, and delayed excretory phases
Delayed imaging (5-15 minutes post-contrast) is crucial to detect active urine extravasation.40,51
Ultrasound may identify perinephric fluid collections, but small leaks or retroperitoneal urinomas may be missed. Ultrasound can be used for follow-up or drainage guidance.
MRI with MR urography can demonstrate urine leaks in patients where CT is contraindicated, particularly in children or those with impaired renal function. T2-weighted sequences and heavily weighted MR urography highlight fluid collections and continuity with the collecting system.
Pitfalls and Mimics
Perinephric hematoma or abscess can mimic a urinoma; attenuation on CT and delayed imaging help differentiate
Small, intermittent leaks may be missed on initial imaging, requiring repeat or delayed studies
Iatrogenic extravasation post-catheterization or surgery should be distinguished from spontaneous rupture
Management Considerations
Prompt recognition is essential to prevent complications such as infection, sepsis, or loss of renal function. Management depends on the size of the leak, hemodynamic stability, and underlying cause:
Conservative management: Small urinomas without infection may resolve spontaneously; ureteral stenting or nephrostomy may facilitate drainage and relieve obstruction
Percutaneous drainage: Indicated for large, symptomatic, or infected collections
Surgical repair: Reserved for severe trauma, persistent leaks, or complex ureteral injuries
Antibiotics: Required if infection is present or suspected
Diagnostic Pitfalls and Mimics
Several conditions may mimic acute urinary tract emergencies, including musculoskeletal pain, gastrointestinal pathology, and gynecologic disease. Early or mild disease may demonstrate subtle imaging findings, leading to false-negative interpretations. Common pitfalls include mistaking renal infarction for pyelonephritis, overlooking non-calculous obstruction, misinterpreting hemorrhage as neoplasm and multiple renal abscesses that can mimic renal lymphoma. Correlation with clinical presentation and laboratory findings is essential.
Management Implications and Reporting Tips
Radiology reports should be clear, structured, and clinically actionable. Key elements include:
Identification of the primary diagnosis
Assessment of severity and complications
Description of laterality and extent
Recommendations for further imaging or urgent intervention when appropriate
Effective communication with the clinical team is essential, particularly in life-threatening conditions.
Conclusion
Acute non-traumatic urinary tract emergencies represent a clinically significant and heterogeneous group of conditions that frequently present with nonspecific symptoms, such as flank pain, hematuria, and fever, making diagnosis challenging in the emergency setting. These include obstructive, infectious, vascular, hemorrhagic conditions, and urinary leaks, often requiring imaging for accurate and timely diagnosis. Imaging plays a central role in evaluation and management. Ultrasound is commonly used as a first-line modality, particularly in vulnerable populations, while computed tomography (CT) remains the cornerstone of acute assessment due to its speed, high spatial resolution, and comprehensive evaluation. Non-contrast CT is the gold standard for stone detection, whereas contrast-enhanced CT enables accurate assessment of infection, vascular complications, hemorrhage, and urinary leaks. Magnetic resonance imaging (MRI) provides a complementary role in selected cases. Recent advances such as photon-counting CT (PCCT) may further improve diagnostic performance through enhanced spatial resolution, superior contrast-to-noise ratio, and spectral imaging capabilities, facilitating the detection of subtle abnormalities while potentially optimizing radiation dose. A structured imaging approach, combined with awareness of characteristic findings and potential diagnostic pitfalls, is essential for accurate diagnosis. Clear and clinically oriented reporting, along with effective communication with the multidisciplinary team, is critical for appropriate management. Overall, the integration of imaging findings with clinical context enables timely diagnosis and plays a key role in improving patient outcomes in acute non-traumatic urinary tract emergencies.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.