
Abstract
Focused Abbreviated Survey Technique (FAST) MRI protocols address the clinical challenges of prolonged scan times, sedation requirements, and ionizing radiation exposure in pediatric neuroimaging. These guidelines, developed by the Canadian Society of Pediatric Radiology (CanSPR), provide evidence-informed recommendations to assist practitioners in the selective application of abbreviated MRI protocols across diverse clinical scenarios. Based on comprehensive literature review and expert consensus, the working group established a framework for using FAST MRI as a targeted, CT-sparing strategy. The guideline outlines protocols and indications for the follow-up of hydrocephalus, arachnoid cysts, and syringomyelia. It also addresses its application in acute settings, including suspected stroke, first-time seizures, and accidental trauma, as well as its role in evaluating macrocrania following inconclusive ultrasound and headaches. While FAST MRI facilitates timely diagnosis and improves safety by minimizing anesthesia, it may have lower spatial resolution than conventional protocols. Consequently, these recommendations emphasize its use for targeted diagnostic questions rather than as a replacement for comprehensive MRI examinations.
Purpose
These guidelines, developed by the Canadian Society of Pediatric Radiology (CanSPR), provide evidence-informed recommendations for the use of FAST (Focused Abbreviated Survey Technique)
1
MRI protocols in pediatric neuroimaging. The goal is to assist radiologists and associated practitioners in making informed decisions about when and how abbreviated MRI protocols may be appropriately applied across different clinical scenarios. By promoting standardized approaches, these guidelines aim to support timely diagnosis while minimizing the need for sedation and exposure to ionizing radiation. Flexibility is built in to accommodate clinical variability and institutional resources while maintaining best practices. The document below is organized by clinical indication for imaging and is based on a comprehensive literature review (see
These guidelines are intended to support clinical practice in pediatric neuroimaging by outlining general principles for the use of FAST MRI techniques. They are not exhaustive and should not be interpreted as mandatory standards of care. The information provided does not replace the independent clinical judgment of the interpreting radiologist or the healthcare team. Because each patient presents unique clinical circumstances, diagnostic and management decisions remain the responsibility of the treating team and should be made in accordance with professional expertise, institutional policies, local protocol preferences, and available resources.
Introduction
Conventional, full-length MRI protocols comprise multiple sequences, are acquired in multiple anatomic planes, and can include imaging before and after contrast administration. These protocols aim for high spatial resolution and comprehensive anatomical coverage to fully characterize pathology and exclude differential diagnoses. Although diagnostically comprehensive, these protocols require prolonged scan times, which may necessitate sedation in pediatric patients and impact MRI availability in busy centers. In time-sensitive situations, CT may be used as an alternative, but at the expense of radiation exposure and reduced soft-tissue detail.
A “FAST” MRI protocol can be achieved in several ways2 -5:
Overview of FAST MRI Protocols
Rationale
The aim of FAST MRI is to provide a sedation-free, radiation-free, and time-efficient examination of the brain and/or spine that is explicitly tailored to answer a specific clinical question, rather than to achieve comprehensive anatomic characterization. In pediatric practice, it often serves as a CT-sparing strategy, enabling timely diagnosis while avoiding ionizing radiation. For example, in children presenting with acute focal deficits, detection of ischemia or hemorrhage can frequently be achieved with an abbreviated protocol. Similarly, in established hydrocephalus with prior imaging for comparison, shunt evaluation may not require full anatomic assessment.
Utility of Additional and Optional Sequences
In cooperative children, additional sequences may be selectively incorporated based on the clinical indication or on abnormalities identified on the initial fast sequences. These supplemental sequences can improve lesion characterization, confirm suspected findings, or address secondary diagnostic questions without substantially increasing overall scan time. When feasible, this flexible, stepwise approach allows targeted examination in real time, preserving the efficiency and sedation-free advantages of FAST MRI while enhancing diagnostic confidence.
Approaches for Pediatric MRI Without Anesthesia
Recent research strongly supports the use of non-pharmacologic techniques to perform pediatric MRI without anesthesia, significantly improving safety and efficiency. The feed-and-sleep method remains highly effective for infants, while melatonin has shown promise in gently inducing sleep in older children. 4 For older children, virtual reality (VR) preparation, 6 video goggles, and interactive MRI rooms with calming themes have been shown to reduce anxiety and improve scan success. Therapy dogs are also increasingly used to provide emotional comfort before procedures. A key advancement has been the integration of certified child life specialists (CCLS), who use tailored preparation, distraction techniques, and emotional support to help children remain calm and still during scans. 7 A large study at the Hospital for Special Surgery (HSS) involving nearly 2000 children achieved a 0% sedation rate using CCLS interventions. Similarly, the “Kids Can” program 8 at Children’s Health demonstrated that child life-led education and screening could predict and ensure successful non-sedated MRI in over 97% of cases. These findings underscore the importance of child life services as a standard component of pediatric MRI workflows, especially for children aged 4 to 12 years.9-11
Limitations of FAST MRI
Despite its advantages, implementation of FAST MRI presents several practical challenges. These include optimization of abbreviated sequences, protocol standardization across institutions, staff training, and ensuring timely access for emergent pediatric indications. Additionally, FAST MRI protocols may have lower spatial resolution than conventional examinations, which can limit detection of small parenchymal or vascular abnormalities. Importantly, FAST MRI should be implemented as a CT-sparing strategy for targeted clinical questions rather than as a replacement for comprehensive diagnostic MRI protocols. Careful protocol design and integration into clinical workflows are therefore essential to maximize diagnostic utility and ensure safe implementation.
Hydrocephalus
FAST MRI has transformed the management of pediatric hydrocephalus by enabling rapid, radiation-free assessment of ventricular size and shunt patency without the routine need for sedation and lack of radiation exposure.12 -14 Over the past decade, multiple high-impact studies have validated the diagnostic accuracy and efficiency of this approach, which utilizes fast T2 and optional T1-weighted sequences to deliver critical information for children at risk of shunt malfunction and repeated exposure to ionizing radiation.12,13,15,16 Technological advances, such as ultrafast single-shot T2-weighted sequences, allow for rapid scanning in 2 to 3 minutes, offering a reliable alternative to CT for follow-up evaluation of hydrocephalus.14,16
For follow-up imaging of hydrocephalus, a FAST MRI protocol is
Recommended Protocol for Hydrocephalus
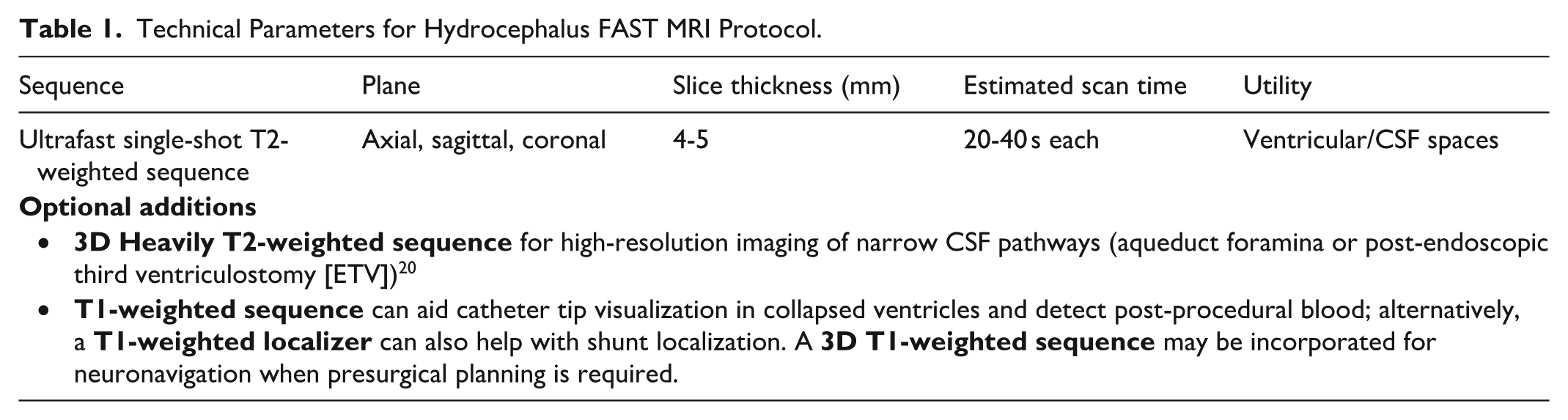
Table 1 details the technical parameters and recommended sequences for the FAST MRI protocol. Customization is common based on MRI scanner strength (1.5T vs 3T, 3T is preferred due to better resolution), coil type (16, 28, or 64 channels), patient cooperation and age, and clinical urgency.14,17 The abbreviated hydrocephalus protocol typically includes an ultrafast single-shot T2-weighted sequence acquired in axial, sagittal, and coronal planes to visualize the ventricles and extra-axial spaces, as well as to assess intracranial catheter position and visualized the extracranial part.12,14 A T1-weighted sequence is often added to enhance catheter visibility, especially in cases with slit-like ventricles, and to aid in detecting blood after shunt insertion.15,16,18,19
Technical Parameters for Hydrocephalus FAST MRI Protocol.
Limitations
Single-shot T2-based FAST MRI sequences generally have less anatomical detail than conventional MRI, revealing only gross pathology and potentially missing subtle parenchymal disease.16,21 Sequence susceptibility to valve-induced artifacts may compromise image quality, especially in single-shot sequences such as SSh (single-shot spin-echo)16,17 and can be improved with spin echo sequence. Unintentional changes in programmable shunt valve settings may occur during the MRI, requiring coordination with neurosurgery to reprogram the valve.
Headaches
Headaches are a common driver for pediatric imaging referrals in both outpatient and emergency settings. Nearly 60% of children and adolescents experience significant headaches, with Canadian data showing that 26.6% of adolescents aged 12 to 13 years and 31.2% of those aged 14 to 15 years report headaches at least one per week.22,23 According to the International Classification of Headache Disorders, 24 these are categorized as:
Current guidelines, including the CAR Referral Guidelines 25 and ACR Appropriateness Criteria 26 maintain that imaging is not routinely recommended for primary headaches. While incidental findings are reported in 3.5% to 10% of pediatric MRIs performed for headaches, these are frequently non-neoplastic and often unrelated to the headache itself (eg, incidental sinus mucosal thickening or middle ear fluid).27,28 Imaging plays an important role only when “red flags” are identified during the patient history or neurological examination. 29 While patient and family anxiety often influences the decision-making process, a normal scan should primarily be viewed as a tool for clinical reassurance in cases where imaging is already medically justified. In emergency settings, CT is often utilized for its speed; however, it is not preferred for children due to radiation exposure.
When imaging is clinically warranted for headache, a FAST MRI protocol is
Recommended Protocol for Headaches
The Working Group endorses the rapid MRI protocol described by Trofimova and Kadom as an effective approach for evaluating headaches in children. 3 The endorsed protocol includes sagittal T1-weighted, axial T2-weighted*or FLAIR*, axial DWI with ADC maps, and axial GRE sequences with a total table time of approximately 5 minutes. Implementation of this protocol demonstrated a 74% reduction in sedation use and maintained diagnostic accuracy across a broad range of pathologies. 3 While published data on long-term outcomes remain limited, this approach supports timely, safe, and effective imaging for children with primary headaches. Table 2 provides the recommended sequences for the FAST MRI protocol.
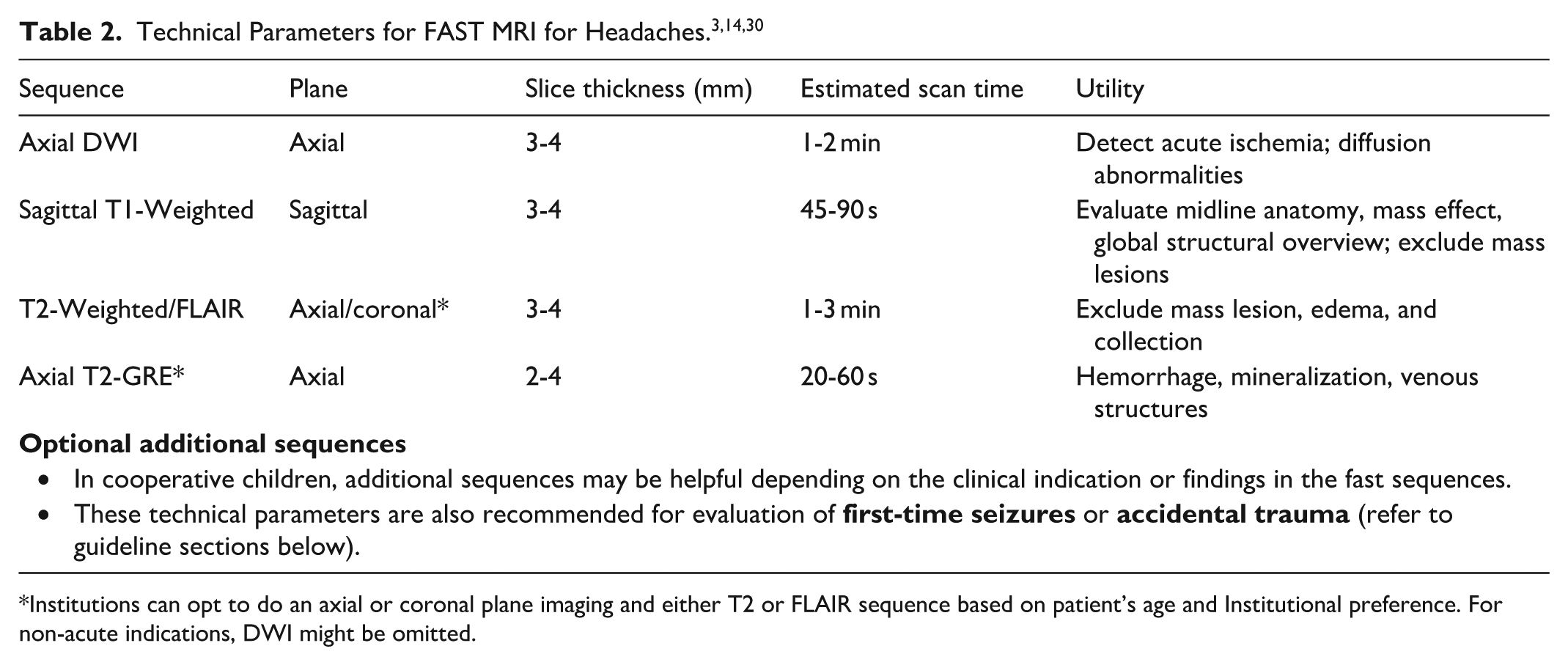
Institutions can opt to do an axial or coronal plane imaging and either T2 or FLAIR sequence based on patient’s age and Institutional preference. For non-acute indications, DWI might be omitted.
Limitations
Evidence regarding the diagnostic accuracy and long-term clinical impact of rapid MRI protocols for headaches remains limited. Further high-quality studies are needed to validate their effectiveness and support their integration into standardized imaging guidelines.
Acute Stroke
Pediatric arterial ischemic stroke (AIS) is challenging to diagnose due to nonspecific, age-dependent symptoms, a high rate of stroke mimics, and the lack of standardized pediatric imaging protocols.31,32 Conventional MRI can be limited by motion, long scan times, and the need for sedation. 33 FAST MRI addresses these issues by providing high sensitivity for acute ischemia. DWI is superior to CT for detection of acute ischemia, including posterior fossa stroke, improves identification of stroke mimics, and reduce the need for sedation while facilitating rapid evaluation for acute reperfusion therapies. 34 Additionally, it aids in identifying stroke etiology, making FAST MRI the preferred first-line imaging in many pediatric AIS pathways.30,35
For imaging in children with suspected stroke after initial emergency clinical assessment, a FAST MRI protocol incorporating diffusion‑weighted imaging is
Recommended Protocol for Acute Stroke
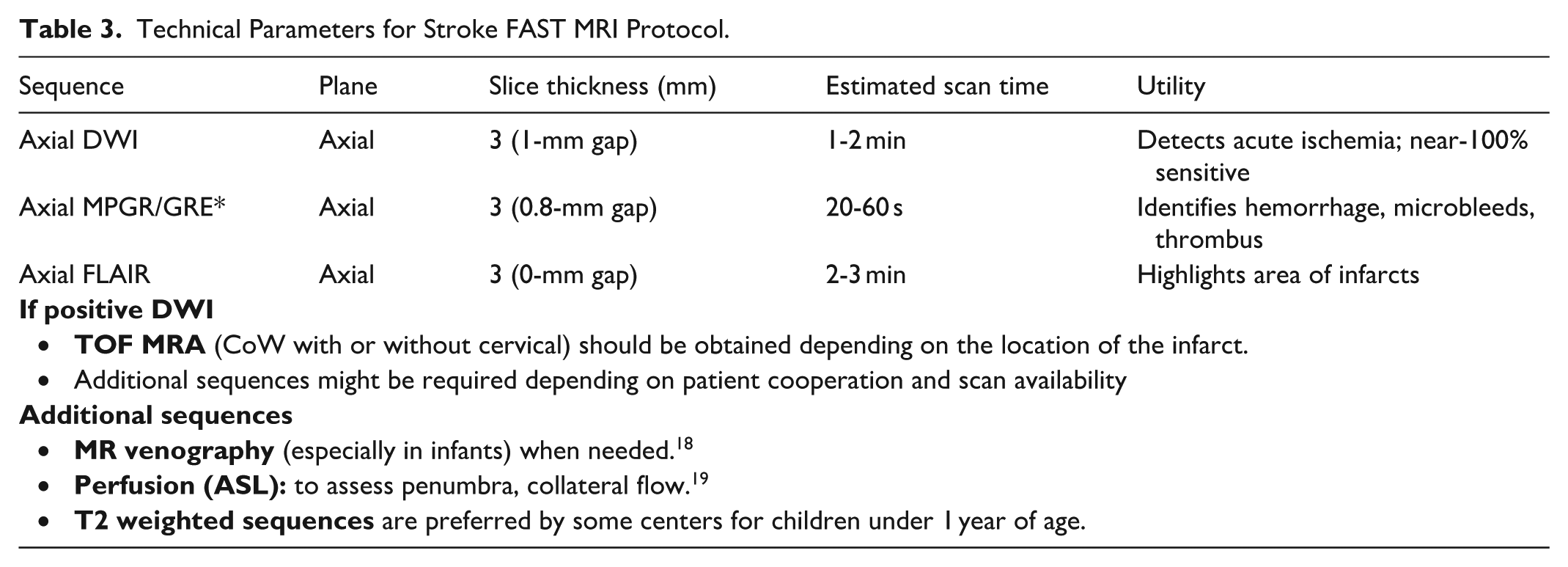
This protocol shortens scan time (~6 minutes) while maintaining accuracy for detecting ischemia and hemorrhages. Table 3 details the recommended sequences for the FAST MRI protocol. A practical approach is to begin with DWI to assess for acute ischemia, followed by susceptibility-weighted or gradient-echo sequences to evaluate for hemorrhage, and then FLAIR or T2-weighted imaging. If abnormalities are identified on these initial sequences, further vascular assessment with time-of-flight (TOF) MR angiography should be considered and additional sequences may be obtained as clinically indicated.
Technical Parameters for Stroke FAST MRI Protocol.
Limitations
TOF MR angiography can overestimate stenosis, and flow-related artifacts are common. Additionally, FAST MRI protocols have limited spatial resolution, particularly in very small vessels, which can affect diagnostic accuracy. 33
Arachnoid Cyst Follow-Up
Arachnoid cysts are benign, frequently encountered cysts in pediatric neuroimaging, often discovered incidentally. While most cysts remain stable and asymptomatic, follow-up imaging is recommended in the first few years after diagnosis to assess interval growth, the development of mass effect, or complications such as hemorrhage, particularly in settings of trauma. MRI protocols, although comprehensive, often require prolonged scan times and sedation—factors that can be particularly challenging in young children and unnecessary for stable cyst surveillance.
For follow-up imaging of arachnoid cysts, a FAST MRI protocol is
Recommended Protocol for Cyst Follow-Up
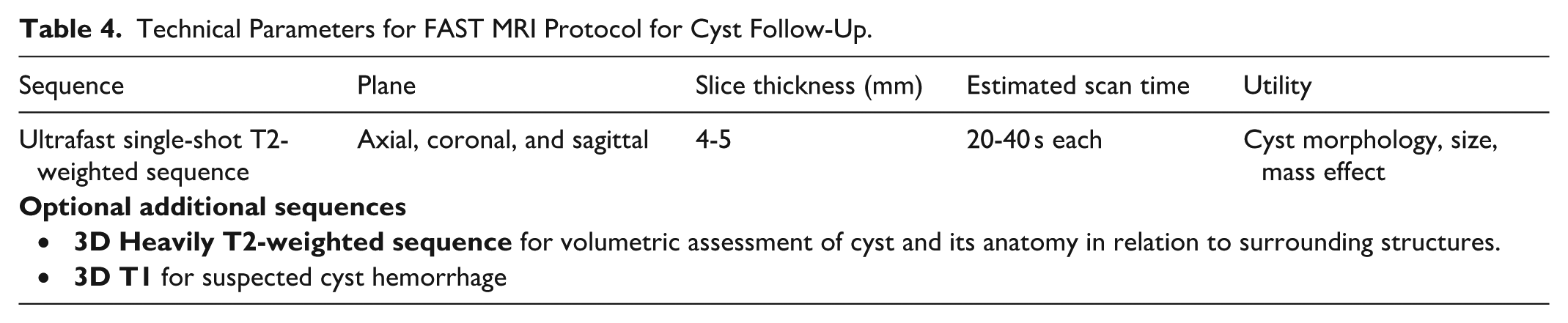
Initial MRI assessment of intracranial cysts should include conventional protocols to fully characterize lesion morphology and differentiate cyst types.16,36,37 Table 4 details the recommended sequences for the FAST MRI protocol for follow-up imaging. The essential components include 3 planes ultrafast single-shot T2-weighted sequence (slice thickness 4-5 mm; scan time 20-40 seconds per plane) are sufficient to assess cyst size, configuration, and interval change.
Technical Parameters for FAST MRI Protocol for Cyst Follow-Up.
Limitations
Given susceptibility to artifacts near the skull base and CSF flow interfaces, FAST MRI follow-up should be limited to previously characterized, uncomplicated cysts and interpreted in direct comparison with prior imaging, with careful attention to consistent slice orientation and measurement to ensure reliable assessment of interval change. 16
Pineal cysts are frequently encountered as incidental findings in the pediatric population. Cysts measuring ≥1 cm are commonly followed with interval imaging.38,39 Although data specifically evaluating FAST MRI protocols for surveillance of isolated pineal cysts in children remain limited, abbreviated protocols may provide sufficient information for follow-up in clinically stable patients while reducing scan time and the need for sedation.
Macrocrania
Macrocrania is a relatively common indication for neuroimaging, defined as a head circumference (HC) greater than 2 standard deviations above the mean for age and sex. It may be associated with a range of underlying conditions, including benign familial macrocephaly, hydrocephalus, megalencephaly, metabolic disorders (such as Canavan disease), genetic syndromes (eg, Sotos syndrome, PTEN-related disorders), and intracranial masses or hemorrhage. Benign enlargement of the subarachnoid spaces (BESS) is the most common cause of macrocephaly in infants. It typically presents in otherwise healthy children with a rapidly increasing head circumference that exceeds the 95th percentile and crosses percentile lines on the growth chart. Neurodevelopment in these children is usually normal or near-normal. 40 Neuroimaging plays a key role in differentiating these causes and guiding further management.
The initial imaging evaluation of macrocrania in infants should be guided by a thorough clinical history and physical examination, including developmental assessment and serial head circumference measurements. Ultrasound is typically the first-line modality in infants with open fontanelles because it is accessible, avoids ionizing radiation, and effectively visualizes ventricular size and subarachnoid spaces.
For imaging in young children with macrocrania who are otherwise clinically well with an inconclusive ultrasound, or for whom ultrasound is not possible, a FAST MRI protocol is
When ultrasound findings are inconclusive or additional anatomical detail is needed, MRI is preferred for its superior soft tissue contrast and ability to assess brain parenchyma. FAST MRI sequences, such as single-shot T2-weighted imaging or abbreviated protocols, are increasingly used to reduce scan time and avoid sedation in young children with otherwise reassuring clinical examination. These sequences have shown high diagnostic accuracy. 41
Recommended Protocol for Evaluating Macrocrania
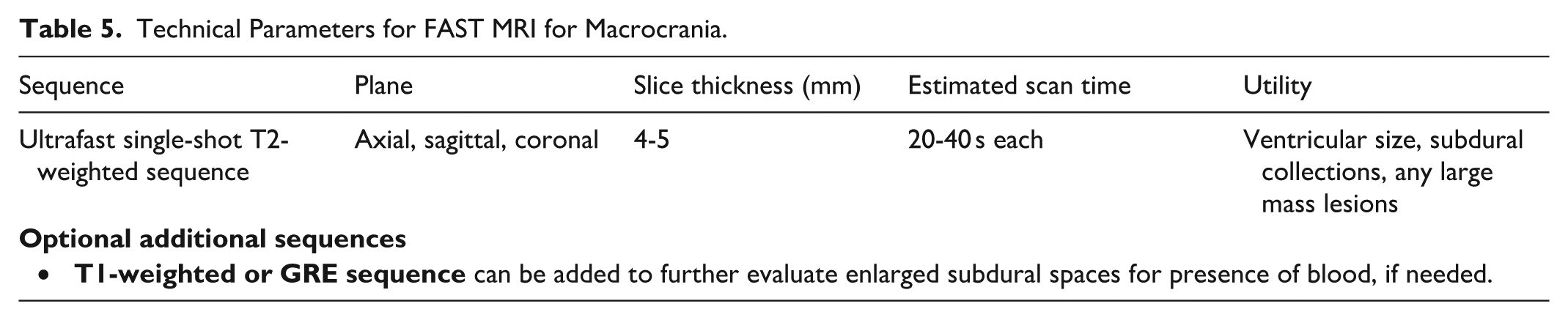
FAST MRI protocols are valuable for excluding major findings such as hydrocephalus, mass lesions, midline shift, or large extra-axial collections, and for follow-up imaging of CSF spaces. However, caution is warranted for baseline assessment, as subtle structural abnormalities may be missed. For example, in children with suspected genetic or overgrowth syndromes, FAST MRI may rule out hydrocephalus or mass lesions but fail to detect cortical malformations or dysmorphic features, which require high-resolution imaging.
In summary, FAST MRI may be considered in otherwise healthy infants presenting with macrocrania, particularly when cranial ultrasound is suboptimal or not applicable.
Table 5 details the recommended sequences for the FAST MRI protocol. If FAST MRI reveals intracranial abnormalities, a full protocol MRI should be tailored to the specific abnormality identified.
Technical Parameters for FAST MRI for Macrocrania.
Limitations
In cases of suspected head trauma presenting with macrocrania, FAST MRI protocols are insufficient for a comprehensive evaluation. These abbreviated scans can miss small subdural collections and parenchymal injuries.
First Time Seizures
Seizures represent approximately 1% of all pediatric emergency department visits, with the incidence of acute symptomatic seizures being highest during infancy.42,43 Neuroimaging is generally unnecessary when the clinical history and EEG findings indicate generalized epilepsy or simple febrile seizures. However, imaging is recommended in cases of convulsive or focal seizures, seizure clusters, changes in seizure pattern, or seizures with post-ictal focal neurological deficits.44,45
A recent pan‑Canadian survey of pediatric imaging practices highlights substantial variability in MRI protocols, sedation thresholds, and the use of abbreviated or FAST MRI techniques for new‑onset seizures, underscoring the need for clearer national guidance in this area. 46 It is essential to differentiate between MRI protocols designed to exclude structural causes of seizures (eg, mass lesions or tuberous sclerosis complex) and those tailored for epilepsy surgical planning. While both rely on high-resolution neuroimaging, surgical planning often requires more advanced protocols to detect subtle cortical malformations and common causes of drug-resistant epilepsy, such as focal cortical dysplasia.
There is a lack of literature validating the use of FAST MRI techniques for the brain for first time seizures in the pediatric age group. Despite ongoing efforts to optimize MRI protocols through adjustments in imaging sequences and parameters,47,48 the use of multidynamic multi-echo sequences (synthetic MRI, eg, MAGiC for GE), multicontrast EPI sequence (eg, EPIMix)49,50 as well as more recent advances such as deep learning-based reconstructions,51,52 there is still no conclusive evidence that FAST MRI protocols can fully replace standard, full-length brain MRI protocols for seizure evaluation or for detecting subtle cortical malformations and other pathologies.
In the evaluation of first-time seizures in the emergency settings, FAST MRI
Recommended Protocol for First-Time Seizures
Despite the lack of published evidence, FAST MRI brain examinations can detect major intracranial abnormalities, including ventriculomegaly, cysts, intracranial collections, ischemia, mass lesions, and significant parenchymal malformations associated with new-onset seizures. In acute or semi-urgent settings where MRI under sedation is not feasible, FAST MRI may be considered as an alternative to head CT for initial evaluation. Table 2 provides the recommended protocol.
Limitations
While often sufficient for most emergent indications as described above, resolution may not be sufficient if greater anatomic detail is required, such as a search for subtle cortical malformations or surgical planning. While MRI is widely used and many centers incorporate HARNESS-MRI elements, 53 few employ dedicated protocols. Sedation thresholds and non-pharmacologic strategies also differ, with limited use of FAST MRI. This heterogeneity reflects the absence of high-level evidence comparing protocol accuracy. National guidelines could help standardize practice, optimize sedation use, and improve diagnostic consistency. 46
Follow-Up of Syrinx
While the role of FAST MRI for brain pathologies is relatively well established, FAST spine MRI protocols are still evolving. Early studies show promising results with FAST spine MRI, achieving high diagnostic accuracy for conditions such as syringomyelia, spinal dysraphism, and conus medullaris anomalies—often without the need for sedation.54,55 These protocols have also shown potential as a first‑line option when spinal infection is suspected, though their utility in this context remains limited by the reliance of many infectious evaluations on contrast‑enhanced sequences. Although FAST MRI can identify major pathologies, its reduced sensitivity compared to full protocols may result in missed findings, particularly in cases of metastatic disease or when scans appear normal, creating a risk of false reassurance.
Across several pediatric centers, FAST spine MRI has shown promising diagnostic performance. In one cohort of infants and toddlers, abbreviated scans were consistently interpretable and comparable to standard sedated MRI examinations, with acquisition times reduced to just a few minutes. 56 However, small structures such as the filum terminale were occasionally less conspicuous, reflecting the trade‑off between speed and fine anatomical detail. 56 Similar results have been observed in older children, where non‑sedated FAST spine studies demonstrated moderate to very good image quality and high inter-observer agreement for detecting syringomyelia, conus medullaris anomalies, and filum terminale abnormalities. 57 More recently, a Canadian validation study of an abbreviated protocol in children under 4 years of age showed high concordance—over 95%—with full conventional MRI for clinically important findings such as cerebellar ectopia, syrinx, and spinal dysraphism, while reducing scan time by approximately 20 minutes. 58
In follow-up of syrinx with no focal neurological deficits, a FAST MRI protocol of the spine is
Recommended Protocol for Spine/Screening Syrinx
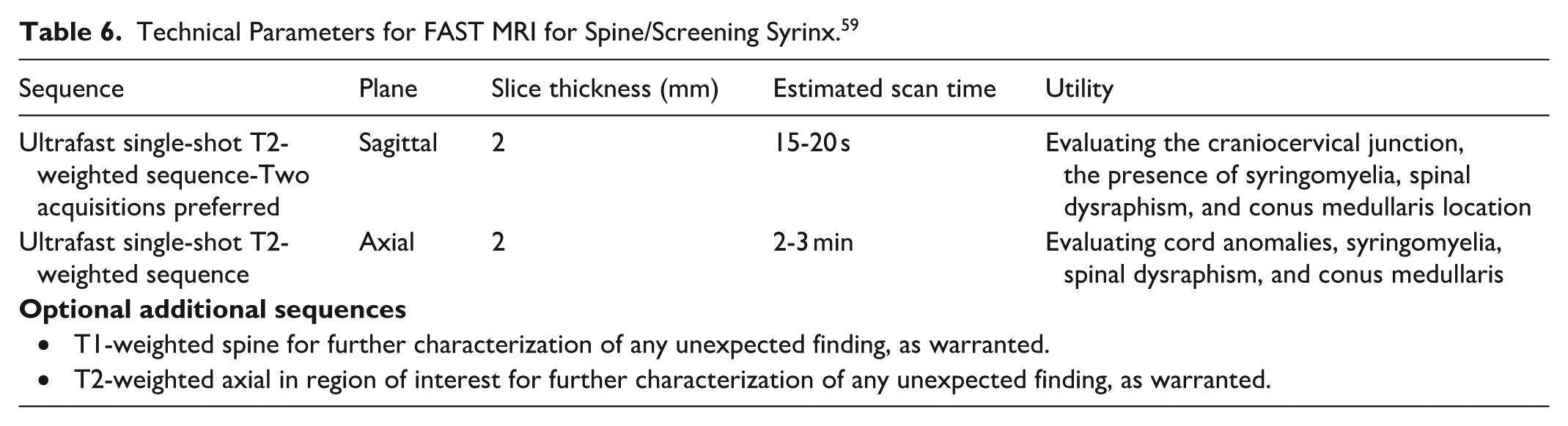
Fast spine MRI protocols typically use abbreviated sequences such as sagittal ultrafast single-shot T2-weighted sequence, significantly reducing scan times while maintaining diagnostic quality (Table 6). These protocols provide targeted evaluations with total imaging times under 10 minutes for young children and approximately 15 to 17 minutes for older children, including calibration, scout, and localizer acquisitions. Total room time generally remains under 20 minutes, making these protocols highly suitable for pediatric imaging workflows.
Technical Parameters for FAST MRI for Spine/Screening Syrinx. 59
Limitations
Fast MRI techniques have inherent limits in spatial resolution. Although adequate for selected indications, such as follow-up of syringohydromyelia or spinal dysraphism, they may be insufficient when detailed anatomic evaluation is required, including in suspected infection or neoplastic processes.
Trauma
Accidental Trauma
FAST MRI has an important but carefully defined role in the evaluation of accidental trauma. It can be used to confirm the absence of significant intracranial injury in children who present after minor falls or sports collisions, or to follow the progression or resolution of known hemorrhage without repeated radiation exposure. 60 Historically, CT has been the default modality in emergency settings because of its speed, widespread availability, and high sensitivity for acute hemorrhage and fractures. 61 However, concerns regarding cumulative radiation exposure in young patients, many of whom may require repeat imaging during their recovery, have created a strong interest in MRI as an alternative or adjunct modality. 62
FAST MRI offers meaningful advantages in these scenarios: it can typically be performed in a few minutes using rapid T2‑weighted single‑shot sequences or updated FAST protocols, avoiding sedation in many children and reducing radiation exposure. 21 It is especially useful in situations where repeated imaging is anticipated, such as follow‑up of subdural collections or postoperative assessments. For example, in a stable 5‑year‑old who presents after a minor fall with headache and brief vomiting but is neurologically intact, a FAST MRI using rapid DWI, T2, and GRE sequences may be sufficient to exclude large hemorrhage or mass effect, avoiding the need for CT. 63
In clinically stable children requiring follow‑up imaging after accidental head trauma, a FAST MRI protocol is
Recommended Protocol for Accidental Trauma
Please see Table 2 for the recommended protocol for accidental trauma.
Limitations
FAST MRI has reduced sensitivity for subtle parenchymal, vascular, and extra-axial findings compared with full protocols. 64 Small subdural hematomas, cortical contusions, venous sinus thrombosis, and diffuse axonal injuries may not be visible. Furthermore, MRI is inherently inferior to CT in evaluating bony structures, meaning skull fractures and subtle cranial abnormalities may not be identified. For this reason, FAST MRI is best understood as a complementary tool in accidental trauma rather than a replacement for CT or full MRI protocol, and should be reserved for children who are stable, when the clinical question is narrow and clearly defined. 65
Non-Accidental Trauma and Abuse
The evaluation of suspected non‑accidental trauma (NAT) is fundamentally different from accidental trauma, and FAST MRI is
The subtle, multilayered subdural collections that typify abusive head trauma require higher resolution, multi-sequence MRI for accurate detection. Sequences such as SWI or GRE are essential for visualizing small hemorrhagic foci and venous injury, while DWI is critical for identifying early ischemic or axonal injury. 63 High-resolution T2 sequences allow for the detection of cortical contusions or parenchymal abnormalities that may be overlooked on FAST protocols. FAST MRI protocols that rely primarily on single‑shot T2 imaging are insufficiently sensitive and carry a significant risk of false reassurance. 68 Likewise, CT often remains necessary for evaluating skull fractures, given its superior assessment of osseous structures.
For these reasons, guidelines must clearly distinguish between accidental and non‑accidental trauma pathways. FAST MRI may be appropriate for stable children with clearly accidental mechanisms and narrow clinical questions but should not be used as the primary imaging modality when abuse is suspected. In NAT evaluations, a full multi‑sequence MRI, often in combination with CT, remains essential.
For imaging non-accidental trauma, a FAST MRI protocol
Clinical and Workflow Implications
Successful implementation of FAST MRI requires thoughtful integration into existing clinical workflows. Because abbreviated protocols are short, they may be interleaved between longer examinations, potentially improving scanner utilization and patient throughput. However, scheduling these studies within already busy MRI services can be challenging and may require coordination among technologists, radiologists, and referring clinicians. Institutions have adopted different strategies to facilitate implementation, including dedicated time slots, prioritization of emergency indications, or scheduling exams during nighttime hours, when children are more likely to sleep naturally. Clear communication with referring clinicians is also essential, as reports should explicitly state the abbreviated nature of the protocol to avoid overinterpretation of negative findings.
Suggested Report Language
Technique: FAST (abbreviated) brain MRI performed without intravenous contrast, as clinically indicated. Typical sequences include (DWI/ADC, axial T2 or FLAIR, and GRE or 3 planes single shot T2). This is a
Disclaimer: This is a
Conclusion
FAST MRI protocols are increasingly incorporated into pediatric neuroimaging practice as efficient, radiation-free approaches for targeted clinical questions. For a summary of recommendations and suggested protocols, please see Table 7. When appropriately applied, they can provide timely diagnostic information while reducing the need for sedation. However, FAST MRI should be viewed as a focused problem-solving tool rather than a substitute for comprehensive diagnostic MRI when detailed evaluation is required. Continued efforts toward protocol refinement, clinician education, and clear communication of protocol limitations are essential to support safe and effective use of FAST MRI in pediatric imaging.
Summary of Recommendations and Suggested Protocols.
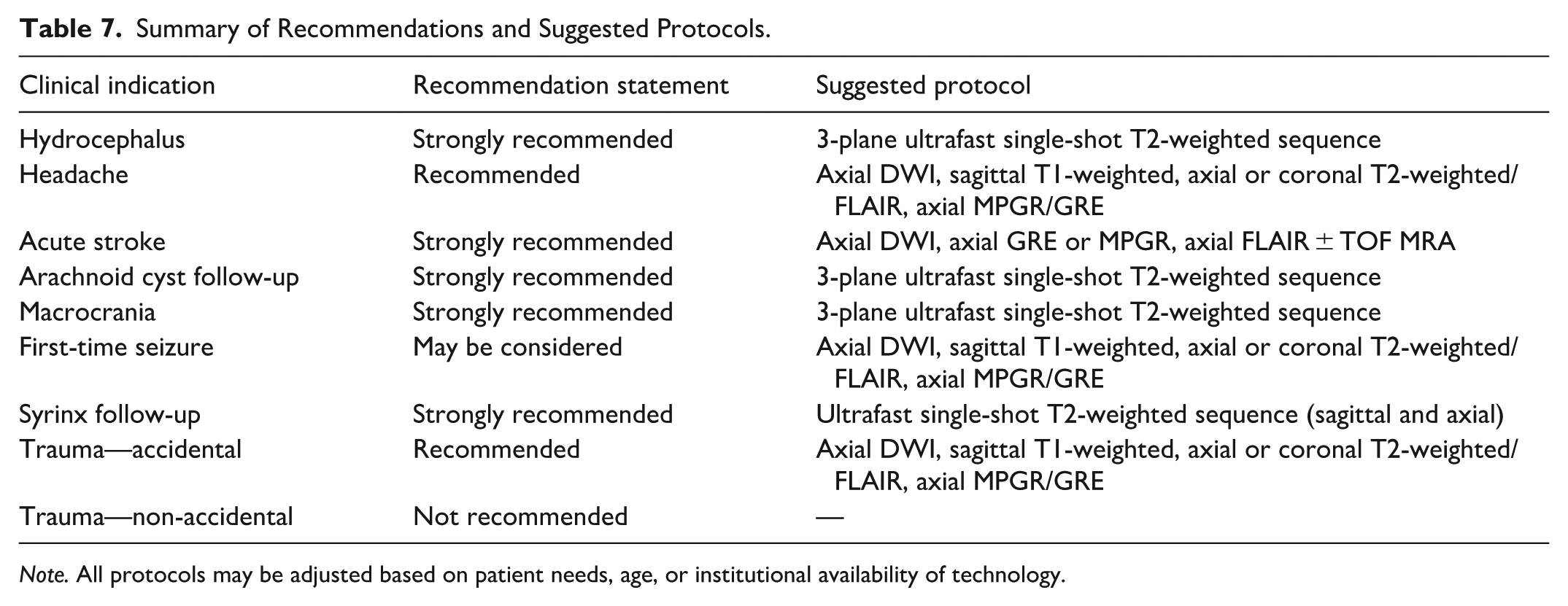
Note. All protocols may be adjusted based on patient needs, age, or institutional availability of technology.
Methodological Note
Literature Review
We conducted a review of the literature published since 2005 on FAST MRI sequences, protocols, and techniques relevant to pediatric neuroimaging. Published evidence on this topic remains limited; initial searches identified fewer than 150 references, of which 93 were deemed sufficiently relevant for detailed review and consideration for inclusion in this manuscript. As a result, the final recommendations in this guideline are informed by both the available literature and the expert consensus of the working group.
Consensus Recommendations
A modified Delphi process was used to establish expert consensus on the appropriateness of FAST MRI protocols for common pediatric neuroimaging indications. A purposive panel of pediatric neuroradiology experts completed an anonymous, web‑based survey.
In Round 1, panelists rated 9 clinical indications using a 4‑point Likert scale (strongly recommended, recommended, may be considered, not recommended). Consensus was defined a priori as ≥70% agreement within 2 adjacent Likert categories (eg, strongly recommended + recommended), reflecting directional agreement while allowing variation in strength of endorsement. For items meeting this criterion, the modal category (highest-frequency response) was reported as the consensus recommendation. Free‑text comments were collected to identify areas of disagreement or ambiguity.
Items with polarized responses or unclear wording were revised using panelist feedback and re‑circulated in Round 2, which applied the same rating scale and consensus criteria. The revised statements focused on macrocrania, spine/syrinx screening, accidental trauma follow‑up, and post‑assessment stroke imaging. Round 2 response distributions were reviewed to confirm whether revisions improved clarity and agreement.
The panel convened after survey completion to review results and finalize the recommendation statements.
Footnotes
Acknowledgements
The authors would like to thank the members of the Canadian Society of Pediatric Radiology and the Canadian Association of Radiologists who took the time to provide their feedback and peer review during the drafting of these guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.