
Abstract
The potential role of bovine leukemia virus (BLV), a zoonotic deltaretrovirus, in human breast carcinogenesis remains controversial, and evidence from seroepidemiological studies is limited. This study aimed to evaluate BLV IgG seroprevalence in women with malignant breast cancer and benign breast lesions and to explore the possible association between BLV exposure and breast cancer development. In this cross-sectional comparative study, a total of 124 women aged ≥18 years who presented to Ankara Etlik City Hospital between May and July 2024 were included. The malignant group comprised 82 women with histopathologically confirmed breast cancer, while the control group included 42 women with benign breast lesions. Serum samples were analyzed for BLV-specific IgG antibodies using a commercial enzyme-linked immunosorbent assay kit. Overall BLV IgG seroprevalence was 12.9% (16/124), with rates of 13.4% in the malignant group and 11.9% in the benign group, showing no statistically significant difference (p = 0.812). In the malignant group, BLV IgG seropositive patients were significantly older than seronegative patients, and seropositivity increased with age (p < 0.01). Although higher BLV IgG seropositivity were observed in invasive mucinous carcinoma cases, this association did not reach statistical significance in logistic regression analysis. Hematological parameters were evaluated to investigate potential systemic immune or inflammatory responses associated with BLV exposure; however, no significant associations were identified between BLV IgG seropositivity and these parameters. These findings suggest that BLV exposure, as reflected by humoral immune response, is not directly associated with breast cancer development but may represent cumulative or long-term exposure. Further large-scale, multicenter studies integrating molecular and serological approaches are warranted to clarify the potential role of BLV in human breast cancer etiology.
Keywords
Introduction
Breast cancer is the most frequently diagnosed cancer among women worldwide and represents a major global health concern. The reporting of approximately 2.3 million new cases and 670,000 deaths in 2022 clearly demonstrates the public health significance of the disease (Filho et al., 2025; Freihat et al., 2025). According to data from 2020, breast cancer is the most common cancer among women in Türkiye, accounting for 24,175 new cases and 7,161 deaths (Yekdeş et al., 2024). The incidence and clinical characteristics of breast cancer vary across geographical and demographic populations. Genetic predisposition, hormonal factors, environmental exposures, and lifestyle-related factors collectively contribute to disease development (Admoun et al., 2022). Nevertheless, in the vast majority of sporadic breast cancer cases, the specific etiological factors that initiate tumor formation have not yet been fully identified (Buehring et al., 2014).
Breast cancer may arise from certain benign breast diseases. The risk of malignant transformation in benign breast lesions varies depending on the degree of proliferation and the presence or absence of atypia. Proliferative lesions such as atypical ductal hyperplasia and atypical lobular hyperplasia have been reported to carry a higher risk of breast cancer compared with nonproliferative lesions (Beca et al., 2021). Therefore, elucidating both premalignant lesions and the etiological determinants of breast cancer is of critical importance for improving early diagnostic opportunities and developing preventive strategies (Olaya-Galan et al., 2021).
In addition to genetic and environmental factors, it has been suggested that viral infections may contribute to the development of malignancies in humans and may play an etiological or facilitating role in certain cancer types. It is estimated that approximately 15%–20% of human cancers are associated with viral infections. Viral sequences associated with human papillomavirus, Epstein–Barr virus, and mouse mammary tumor virus have been detected in breast tissue in some studies, which has increased research interest in the potential role of viral agents in breast cancer pathogenesis. However, the involvement of these viruses in breast carcinogenesis remains controversial. Among the viral agents investigated, bovine leukemia virus (BLV) has recently attracted attention due to its oncogenic potential in cattle and the possibility of zoonotic transmission, prompting investigations into its potential association with human breast cancer (Arias-Calvachi et al., 2022; Lawson et al., 2018; Lawson and Glenn, 2017; Ross, 2010).
Within this context, BLV (a zoonotic deltaretrovirus) has been proposed as a potential contributor to human breast carcinogenesis (Afzal et al., 2022). BLV shares genomic and biological similarities with human T-cell leukemia virus type 1, another oncogenic deltaretrovirus (Buehring et al., 2015). Possible zoonotic transmission of BLV through contaminated biological materials such as milk and dairy products has been discussed in the literature. In addition, BLV prevalence has been reported in several countries. However, data from Türkiye regarding whether BLV establishes persistent infection in humans and its potential clinical implications in breast cancer remain limited (Khalilian et al., 2019).
The Tax protein encoded by the pX region of the BLV genome is considered a major contributor to the virus’s oncogenic potential, although additional viral and host factors are also likely involved (Afzal et al., 2022; Buehring et al., 2014; Gao et al., 2020). Experimental studies examining Tax expression in cell culture models have reported the upregulation of proto-oncogenes such as CYR61, FOS, and JUN, along with dysregulation of the expression of more than 100 genes identified through transcriptomic analyses. These findings suggest that Tax may influence multiple cellular signaling pathways; however, such transcriptional changes alone do not establish a direct causal role in oncogenesis (Blanco et al., 2025).
The envelope proteins gp51 and gp30, encoded by the BLV env gene, play key roles in viral entry. Experimental studies have shown that gp51 mediates receptor binding and viral attachment, whereas gp30 facilitates membrane fusion and intracellular signaling. Polymorphisms in these proteins have been associated with alterations in viral entry efficiency and host cell signaling pathways, although their direct contribution to cellular transformation remains uncertain (Blanco et al., 2025; Pluta et al., 2018). In addition, the accessory G4 protein encoded in the pX region has been reported to enhance fibroblast transformation through interaction with Ha-ras in experimental models (Aida et al., 2013). In humans, proviral BLV DNA has been shown to be localized particularly in secretory mammary epithelial cells through in situ PCR studies (Buehring et al., 2015, 2014). Several studies have reported higher detection rates of BLV proviral DNA, gp51 and p24 proteins, as well as Tax expression in breast cancer tissues compared with controls (Blanco et al., 2025; Buehring et al., 2015; Gao et al., 2020). Meta-analyses also indicate that BLV exposure may be associated with an increased risk of breast cancer (Khatami et al., 2020; Saeedi-Moghaddam et al., 2024). In contrast, some studies have failed to demonstrate the presence of BLV in cancerous tissues, and these discrepancies have been attributed to differences in population characteristics, sample types, and methodologies used (Amato et al., 2023; Roheel et al., 2023).
A review of the existing literature reveals that studies investigating the association between BLV and breast cancer have largely focused on tissue-based molecular analyses, whereas serological studies remain limited (Gao et al., 2020; Saeedi-Moghaddam et al., 2024).
Serological approaches can provide complementary epidemiological information by reflecting individual exposure and humoral immune responses, even in cases where viral DNA cannot be detected in tissue. Moreover, studies comparing BLV-specific IgG responses between benign breast lesions and malignant cases are quite limited.
The primary hypothesis of this study is that BLV exposure may be associated with the development of breast cancer and that this association may differ between benign breast lesions and malignant cases. This study aims to evaluate the IgG seroprevalence against BLV in women diagnosed with breast cancer and in women with benign breast lesions, and to discuss the existing evidence regarding the possible role of BLV exposure in breast cancer development within a local patient population.
Materials and Methods
Study design and sample collection
This cross-sectional case-control study included women aged 18 years and older who presented to the General Surgery Outpatient Clinic of Ankara Etlik City Hospital between May 1, 2024, and July 30, 2024. The malignant breast cancer group consisted of patients with a histopathologically confirmed diagnosis of breast cancer established through biopsy or surgical specimen evaluation. Histological subtypes were classified according to the pathological diagnosis documented in the histopathology reports. The control group comprised patients with histopathologically confirmed benign breast lesions, including fibroadenoma, ductal hyperplasia, and cystic lesions.
Only patients with definitive pathological diagnoses recorded in the hospital information system were included in the study. The benign breast lesion group were evaluated as the control group for comparison with the malignant breast cancer group. Pathological subtypes of benign lesions were recorded.
The control group consisted of patients with histopathologically confirmed benign breast lesions evaluated in the same clinical setting during the study period. These benign lesions included fibroadenoma, ductal hyperplasia, and cystic lesions, as documented in the histopathology reports.
Exclusion criteria: Participants were excluded if they had received systemic steroid or immunosuppressive therapy within the previous 6 months, had an active acute infection, or had immunosuppressive conditions such as HIV/AIDS. Patients with a prior history of chemotherapy or radiotherapy were also excluded to avoid potential effects on immune response and serological measurements.
Sample size: Sample size calculations was performed using G*Power software with an alpha level of 0.05 and a statistical power of 80% (β = 0.20). Based on the expected difference in BLV seroprevalence between malignant and benign breast lesion groups reported in previous studies, the minimum required sample size was calculated as 120 participants in total.
In the present study, 124 participants were included (82 in the malignant group and 42 in the benign group), which exceeded the minimum required sample size. Since the study design was cross-sectional and data were obtained at a single time point, no additional adjustment for dropouts was applied.
Data collection: During clinical examination, sociodemographic and clinical data such as age, marital status, family history of breast cancer, and place of residence (rural/urban) were collected using a standardized case report form. Efforts were made to ensure that age and sociodemographic characteristics were comparable between the malignant and benign groups. Clinical data including pathological diagnosis, steroid use, history of chemotherapy, and metastasis status were obtained by reviewing hospital information management system records and patient files. In addition, hematological parameters (including white blood cell count [WBC], hemoglobin, platelet count, and differential leukocyte counts) were recorded to explore whether BLV seropositivity might be associated with systemic immune or inflammatory responses. Since BLV infection is known to affect hematopoietic cells in animal hosts and may lead to hematological alterations such as persistent lymphocytosis, these parameters were evaluated as potential indirect indicators of immune response.
Written informed consent was obtained from all participants or their legal representatives prior to enrollment. The study received ethical approval from the Etlik City Hospital Scientific Research Evaluation and Ethics Committee with the decision dated May 22, 2024 and numbered AEŞH-BADEK-2024-489.
Serological analysis
From all patients included in the study, 5 mL of venous blood samples were collected into gel-containing vacuum tubes. After collection, blood samples were centrifuged at 4,000 × g for 5 min to obtain serum. The obtained serum samples were transferred into 1 mL Eppendorf tubes and stored at −20°C until the day of analysis.
The presence of BLV-specific IgG antibodies were determined using a commercially available enzyme-linked immunosorbent assay (ELISA)-based BLV IgG ELISA kit (Sunlong Biotech, China, Lot No: SL0313Bo). Test results were interpreted based on the evaluation criteria specified by the manufacturer. The optical density (OD) values of the samples were compared with the cut-off value calculated by adding 0.15 to the mean OD of the negative control. Samples with OD values below the cut-off were considered negative (nonreactive), whereas samples with OD values equal to or above the cut-off were considered positive (reactive).
The assays were performed according to the manufacturer’s instructions using the reagents provided in the kit. Positive and negative controls included in the kit were used in each run to ensure assay validity. The ELISA kit used in this study was intended for research use only, and detailed information regarding the specific antigen targeted by the assay was not provided by the manufacturer. Samples that were initially reactive were retested to confirm the results.
Statistical analysis
Statistical analysis of the data was performed using IBM SPSS Statistics version 27 (IBM Corp., Armonk, NY, USA) software. Within the scope of descriptive statistics, categorical variables were presented as frequencies and percentages. Continuous variables were expressed as mean ± standard deviation for descriptive purposes, while the normality of data distribution was assessed using the Kolmogorov–Smirnov test.
Relationships between categorical variables were examined using the Pearson chi-square test or, when appropriate, the Fisher–Freeman–Halton exact test. Comparisons of numerical variables between two independent groups were conducted using the Mann–Whitney U test for non-normally distributed data. In odds ratio analyses, adjusted odds ratios (adjusted odds ratio, aOR) and their corresponding 95% confidence intervals were calculated using logistic regression analysis, taking into account the potential confounding effect of age. Age was included in the logistic regression model as a continuous variable. No correction for multiple comparisons were applied because the analyses conducted in this study were exploratory in nature. P < 0.05 was considered statistically significant
Results
Demographic characteristics of the study population
A total of 124 women were included in the study. The mean age of the participants was 52.8 ± 12.8 years, with an age range of 28–82 years. The mean age of patients with benign breast lesions were 47.43 ± 13.8 years, whereas the mean age of patients diagnosed with malignant breast cancer were 55.52 ± 11.3 years. The mean age of patients in the malignant group were statistically significantly higher compared with the benign group (p < 0.001).
When age distribution was evaluated, 14.5% of participants were aged 20–39 years (n = 18), 51.6% were aged 40–59 years (n = 64), and 33.9% were aged 60 years and older (n = 42) (Table 1).
Demographic and Clinical Characteristics of the Study Population
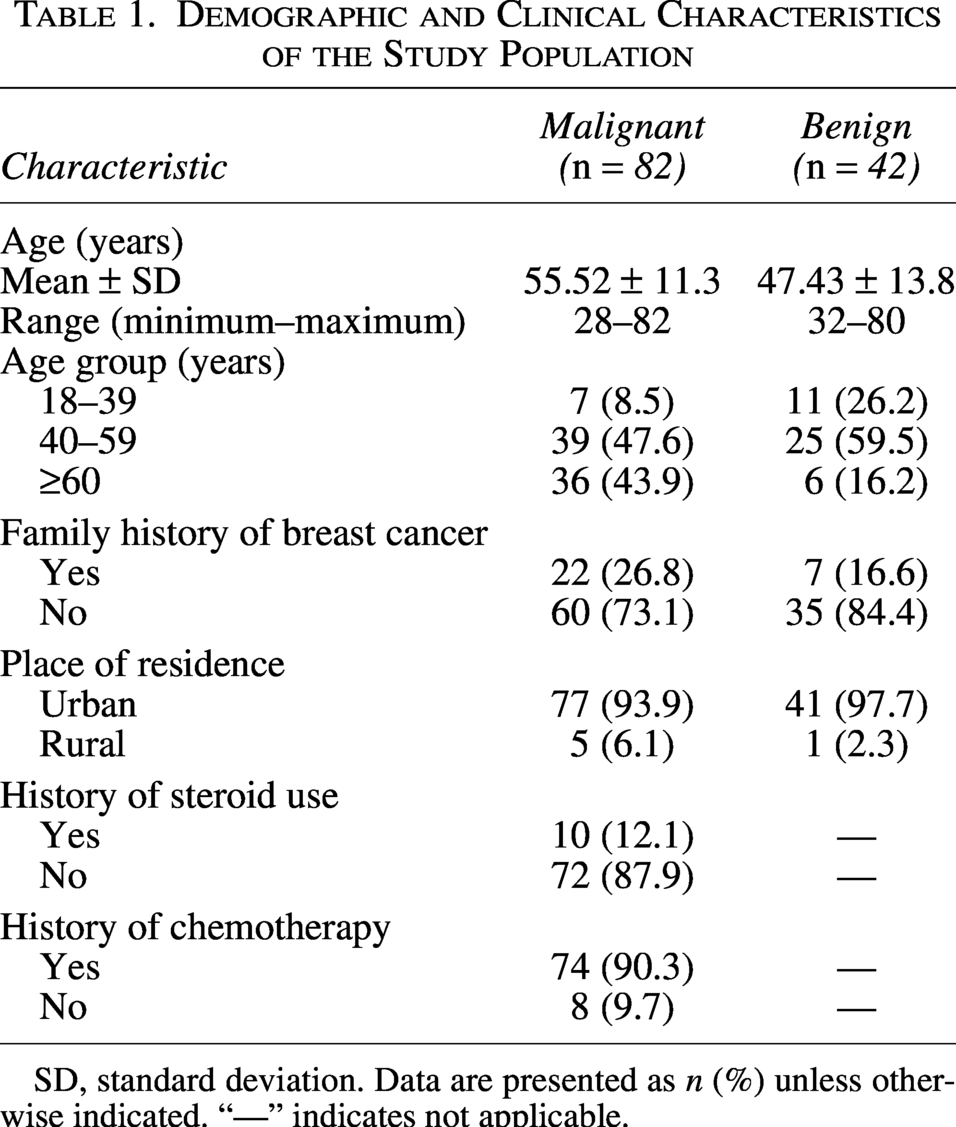
SD, standard deviation. Data are presented as n (%) unless otherwise indicated. “—” indicates not applicable.
BLV IgG seroprevalence and distribution according to clinical groups
The overall BLV IgG seropositivity rate in the study population was 12.9% (16/124; 95% CI: 8.1–19.9). BLV IgG positivity was 13.4% (11/82; 95% CI: 7.7–22.4) in the malignant group and 11.9% (5/42; 95% CI: 5.2–25.0) in the benign group. The difference in BLV IgG seropositivity between the malignant and benign groups were not statistically significant (Pearson chi-square test, p = 0.812).
Relationship between BLV IgG seropositivity and age
In the malignant group, the mean age of BLV IgG seropositive cases were significantly higher than that of seronegative cases (65.4 ± 5.4 years vs. 54.0 ± 11.2 years; p < 0.01).
When BLV IgG seropositivity was evaluated according to age groups in the malignant group, an increasing trend in positivity with advancing age was observed. BLV IgG positivity rates were 0% (0/7) in the 18–39 age group, 2.6% (1/39) in the 40–59 age group, and 27.8% (10/36) in the ≥ 60 age group. This distribution was statistically significant (p = 0.003).
In contrast, in the benign group, BLV IgG seropositivity showed a decreasing trend with age. Positivity rates in the 18–39, 40–59, and ≥60 age groups were 18.2% (2/11), 12.0% (3/25), and 0% (0/6), respectively; however, this difference was not statistically significant (p = 0.705).
BLV IgG seropositivity according to tumor and lesion subtypes
According to malignant tumor subtypes, BLV IgG seropositivity rates were 12.3% (8/65) in invasive ductal carcinoma cases, 0% (0/11) in invasive lobular carcinoma cases, and 50.0% (3/6) in invasive mucinous carcinoma cases. A statistically significant difference in BLV IgG seropositivity was observed among tumor subtypes (Fisher–Freeman–Halton exact test, p = 0.026). The number of cases in some tumor subgroups, particularly invasive mucinous carcinoma, was limited.
In the benign breast lesion group, BLV IgG seropositivity was most frequently detected in fibroadenoma cases (36.4%; 4/11) and less frequently in cystic lesion cases (7.1%; 1/14). No statistically significant association was found between benign lesion subtypes and BLV IgG seropositivity (p = 0.114).
BLV IgG seropositivity and clinical and hematological parameters
In the malignant group, no statistically significant associations were found between BLV IgG seropositivity and history of chemotherapy, steroid use, presence of metastasis, or place of residence (all p values > 0.05; Table 2).
Clinical and Demographic Characteristics of Malignant Patients according to BLV IgG Status

BLV, bovine leukemia virus; IgG, immunoglobulin G; SD, standard deviation; WBC, white blood cell count. Data are presented as mean ± SD or n (%).
Regarding hematological parameters, the mean WBC count was 9.00 ± 3.43 in BLV IgG seropositive cases and 6.99 ± 2.30 in seronegative cases; however, this difference was not statistically significant (p = 0.085). No significant differences were observed between BLV IgG positive and negative groups in terms of mean hemoglobin, platelet, neutrophil, lymphocyte, monocyte, eosinophil, and basophil values (all p values >0.05; Table 2).
Association of age and tumor types with BLV IgG seropositivity
In the logistic regression analysis conducted by considering age groups and tumor types, an increased likelihood of BLV IgG seropositivity was observed in patients aged 60 years and older; however, this association was not statistically significant (OR = 5.95; 95% CI: 0.32–113.62; p = 0.254).
When evaluated in terms of tumor type, a trend toward an increased risk of BLV IgG seropositivity was observed in cases of invasive mucinous carcinoma; however, this finding did not reach statistical significance (OR = 23.0; 95% CI: 0.94–561.82; p = 0.054; Table 3).
Logistic Regression Analysis of BLV IgG Seropositivity according to Age Group and Tumor Type

BLV, bovine leukemia virus; CI, confidence interval; ILC, invasive lobular carcinoma; IDC, invasive ductal carcinoma; IgG, immunoglobulin G; OR, odds ratio; IMC, invasive mucinous carcinoma. Reference category is indicated as “Reference.”
Discussion
The potential association between BLV exposure and human breast cancer remains controversial. While several studies have investigated the presence of BLV genetic material in breast tissue using molecular methods, seroepidemiological evidence remains limited. The characteristics and reported BLV detection rates of previously published studies, together with the findings of the present study, are summarized in Table 4. In the present study, the findings suggest that BLV exposure, as reflected by the humoral immune response, may represent cumulative or past exposure rather than a direct indicator of breast cancer development. Although serological studies evaluating the presence of antibodies against BLV in both patient groups are limited in the literature, numerous studies have investigated the presence of BLV in breast tissues using molecular methods. Buehring et al. reported BLV DNA positivity rates of 59% in malignant breast tissues and 29% in benign tissues (Buehring et al., 2015). In the study by Baltzell et al., BLV DNA positivity were found to be 19.6% in benign breast lesions and 57.3% in malignant tissues, and positivity were reported to be associated with disease progression (Baltzell et al., 2018). Baltzell et al. emphasized that despite the low viral load, BLV may be present in breast tissue at an early and clinically silent stage, which may lead to a weak systemic humoral response. These observations suggest that BLV exposure may occur years before the development of breast cancer and that the serological response may not be prominent during advanced stages of the disease. In contrast, Schwingel et al. reported BLV DNA positivity rates of 30.5% in malignant tissues and 13.9% in healthy tissues; however, they found that ELISA-based antibody positivity against BLV was quite low and that there were no correlation between serological response and PCR positivity (Schwingel et al., 2019). This finding suggests that BLV infection in humans may remain localized and at a low level, and therefore, a systemic humoral response may not always be evident. Lawson et al. also proposed that oncoviruses such as BLV may play a role in early carcinogenesis through a “hit-and-run” mechanism, with viral markers present at low levels or becoming undetectable in later stages. This supports the hypothesis that BLV may act as an initiating or facilitating factor in carcinogenesis, while evidence of active infection may diminish over time (Lawson et al., 2018). Accordingly, the lower seropositivity observed in our study compared with rates reported by molecular methods may be interpreted as reflecting the limited ability of serological responses to accurately represent the presence of viral DNA within tissues.
Summary of Selected Studies Investigating the Association between Bovine Leukemia Virus and Human Breast Cancer
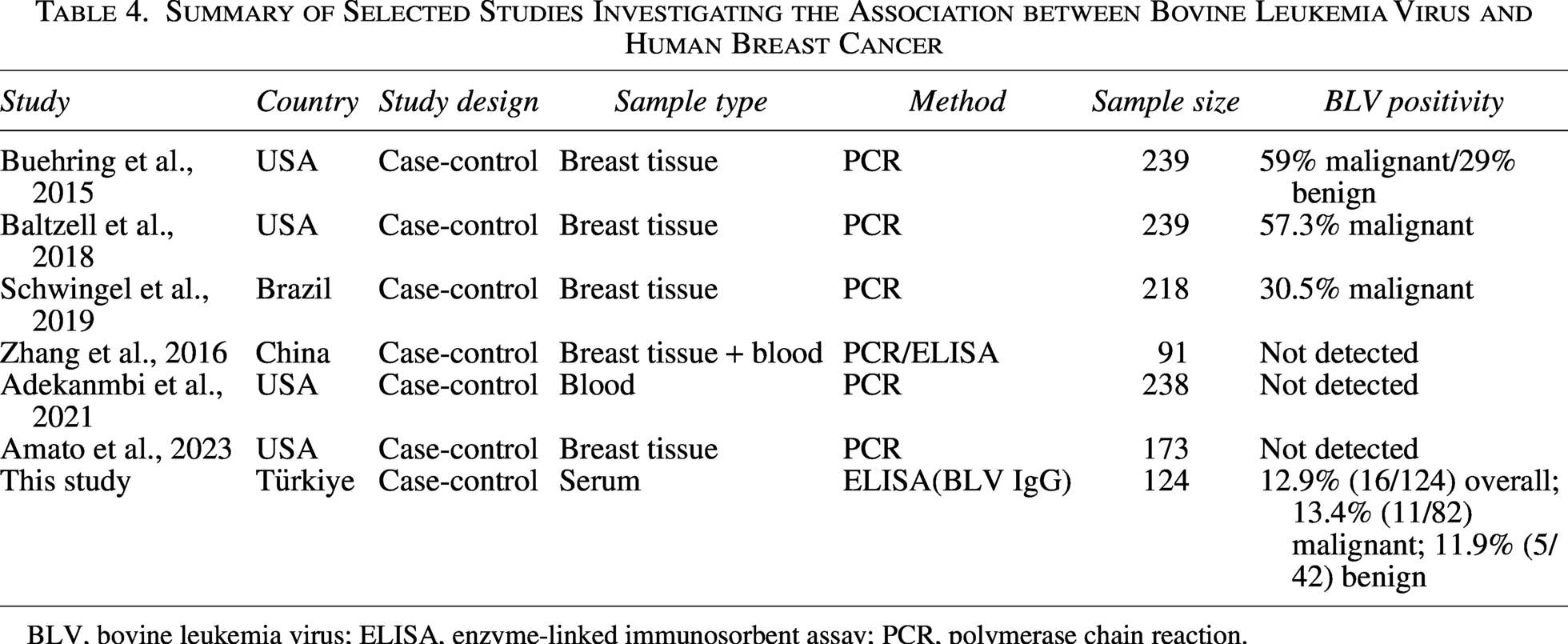
BLV, bovine leukemia virus; ELISA, enzyme-linked immunosorbent assay; PCR, polymerase chain reaction.
In the study conducted by Zhang et al., no serological or molecular evidence of BLV were detected in human breast tissue or blood samples obtained from breast cancer patients and healthy individuals using PCR and ELISA assays (Zhang et al., 2016). In contrast, BLV IgG seropositivity was detected in 47.3% of bovine samples used as positive controls, and viral presence was confirmed by PCR. The authors suggested that the negative findings in human samples may reflect differences in BLV exposure between populations as well as the limited sensitivity of ELISA assays originally developed for cattle in detecting low-level antibody responses in humans (Zhang et al., 2016). This may also be related to substantially lower antibody titers against BLV in humans compared with cattle and the limited sensitivity of serological tests for human immunoglobulins. Similarly, Adekanmbi et al. (n = 238 blood samples; BLV DNA positivity 0%) and Amato et al. (n = 173 breast tumor samples; BLV DNA positivity 0%) did not detect BLV DNA in breast cancer patients using PCR-based molecular assays (Adekanmbi et al., 2021; Amato et al., 2023). These findings highlight the considerable variability across studies, which may be related to differences in geographical regions, sample types (tissue vs. blood), and detection methodologies, including variations in PCR targets and serological assays (Saeedi-Moghaddam et al., 2024). These conflicting results indicate that the relationship between BLV and breast cancer remains controversial and that findings may be influenced by geographical, environmental, and methodological factors. Taken together, the available evidence indicates that the detection of BLV in human breast tissue and serological responses to BLV vary considerably across studies, likely reflecting differences in study design, sample type, detection methods, and population characteristics.
In the evaluation based on histopathological subtypes, the highest BLV IgG seropositivity in our study was observed in cases of invasive mucinous carcinoma. However, this finding should be interpreted with caution due to the limited number of cases in this subgroup. The small sample size may have reduced the statistical power of subgroup analyses and may also have contributed to the wide confidence intervals observed in the logistic regression model. Studies investigating BLV presence according to histological subtypes are limited in the literature, and reported differences appear to depend largely on the molecular targets, testing methods, and populations studied (Delarmelina et al., 2020; Giovanna et al., 2013; Olaya-Galan et al., 2021). This suggests that BLV may not be specific to a particular histopathological subtype, but rather a broadly detectable agent in breast tissue that may exert diverse biological effects.
In our study, BLV IgG seropositivity in the malignant group was found to increase with age, and the mean age of seropositive cases were higher. Similarly, Buehring et al. reported that the mean age of BLV-positive cases were higher and that an association between BLV and breast cancer persisted after adjustment for age (Buehring et al., 2017). In contrast, in our study, the increased risk trend observed for individuals aged over 60 years did not reach statistical significance. Considering that serological responses may reflect long-term or repeated exposure and may cumulatively increase with age, this finding can be regarded as biologically plausible.
Limitations of the study
This study has several limitations. First, the control group consisted of patients with benign breast lesions rather than completely healthy individuals. Although this design allows comparison within the spectrum of breast pathology, individuals with benign breast lesions may share certain biological or environmental risk factors with breast cancer patients, which may influence the interpretation of seroprevalence findings. Therefore, although this control group allowed comparison within the same clinical setting, it may not fully represent a completely healthy population.
Additionally, the serology-based design of the study does not allow for direct assessment of BLV localization within breast tissue or evaluation of viral load. Serological tests primarily reflect humoral immune responses indicative of past or cumulative exposure rather than active or localized infection. Therefore, serological results are not expected to directly correspond with tissue-based molecular findings.
Another limitation is that the ELISA assays used were not validated for human samples, which may have limited its sensitivity in detecting low-level BLV-specific antibodies. This may have led to an underestimation of the true seropositivity rates.
In addition, the absence of molecular confirmation methods (such as PCR or tissue-based analyses) restricts direct evaluation of the relationship between serological findings and viral presence in breast tissue.
Finally, the single-center design and the limited number of cases in certain histopathological subgroups constrain the generalizability of the results.
Conclusion
This study is one of the limited number of seroepidemiological investigations comparing BLV IgG seroprevalence in malignant and benign breast lesions. Our findings indicate that the humoral immune response against BLV does not show a direct or strong association with breast cancer development, while suggesting that BLV exposure in humans cannot be entirely excluded. The serological data imply that the potential role of BLV should be considered in terms of long-term or low-level exposure rather than active infection. To clearly elucidate the possible role of BLV in the etiology of human breast cancer, future prospective, large-scale, and multicenter studies integrating molecular and serological approaches and employing serological assays validated for human samples are warranted.
Authors’ Contributions
M.F.K. and A.B.: Conceptualization, methodology, formal analysis, data curation, writing (original draft and review and editing), supervision, and project administration. D.Ş. and G.E.Ş.: Investigation and sample collection.
Footnotes
Author Disclosure Statement
All authors declared no conflict of interest.
Funding Information
No funding was received for this article.