
Abstract
How and in what ways might we respond to the mounting “care deficit,” such that the dignity and well-being of both recipient and care provider are prioritized? This article takes up such a question by making use of feminist theories of care to recenter caring discourse away from neoliberal notions of autonomy and self-sufficiency and toward those of interdependence and social connectedness. In doing so, we interrogate the appropriateness—or not—of caring labor being delivered within the market by presenting a case study, detailing the promise of community-based, worker-owned cooperatives as a means through which to democratize caring labor.
Caregiving within the United States (and elsewhere) continues to transform at an ever-increasing pace. Traditionally delivered within domestic circles, most often by women without economic recompense, two demographic shifts have considerably transformed the caregiving landscape: the transition of women, either by desire or necessity, into the paid labor market and a rising aging population. The concomitant rise in demand for and decrease in supply of caring labor has created a so-called “care deficit” (Hochschild, 2003). Such a deficit raises questions regarding not only the adequacy of caring services in relation to access, cost, and quality but also the interrelated conditions under which this labor is conceived of and delivered increasingly within the market. That is, if those (women) who previously provided this care are entering the paid labor market to whom—or rather on whom—is this labor being transferred or displaced? And, on what terms?
A likely neoclassical economic response: Individuals (primarily women) will assume this labor and do so for low wages based on the minimal amount of skill required (i.e., theory of human capital investment; see Becker, 1971) and/or the associated intrinsic reward/nonpecuniary compensation in so doing (i.e., theory of compensating differentials; see Smith, 1979). The response from others, most notably critical feminist scholars: Women—most often those experiencing significant social and economic marginalization—are meagerly compensated and deprived adequate health and social benefits by virtue of this labor being fundamentally devalued by our society (e.g., England, 2005).
Central to the scholarship of the latter group is a critique of liberal individualism and its inability to respond to care needs in a socially equitable manner (e.g., Glenn, 2000; Held, 2002; Tronto, 1993; Young, 1997). It is argued that by emphasizing autonomous, independent individuals, liberal individualism devalues care by “obscuring the actual interdependence among people and the need for care that even ‘independent’ people have” (Glenn, 2000, p. 85). As an alternative, feminist scholars offer an ethics of care, stressing social connectedness, interdependence, and the universality of care needs (e.g., Tronto, 1993). By critically examining our conceptualizations and configurations of care and caring labor in this manner, the marginalization and exploitation of care workers—many of whom reside on the intersecting and socially volatile fault lines of gender, race, and class—is no longer relegated to the social and political periphery but instead (re)gains a central position within our individual and collective efforts toward greater social justice (e.g., Glenn, 2000; Held, 2002).
These efforts have involved a critical examination of the marketization of caring labor. Virgina Held (2002) and Nancy Folbre (2008), for example, suggest as an alternative to for-profit configurations that prioritize profit maximization, community-based, cooperative, socially responsible models might be better positioned to organizationally prioritize quality care and labor. And, worker-owned cooperatives have, in particular, emerged as a promising model in this regard (Coontz & Esper, 2003; Pestoff, 2008).
It is the aim of this article, then, to present (i) how and in what ways feminist theories of care call upon us to reimage the configuration and location of caring labor, with the well-being of both recipient and provider of primary concern; (ii) a case study exploring the social, emotional, and economic well-being of care providers prior to and following joining a community-based, worker-owned childcare cooperative; and (iii) a concluding section summarizing suggested next steps as we continue the work of recentering the discourse and practice of care, such that quality care and democratized labor emerge as viable alternatives to existing neoliberal, market-based models.
Feminist Ethics of Care
Historical Tracings
The point of departure for many care theorists is a critique of liberalism and its foundational tenets of equality, liberty, autonomy, rights, and the individual (Brown, 1995). Based on a sociopolitical frame such as this, questions arise as to how and in what ways we—individually and collectively—understand and thereby respond to care needs? That is, if members of a liberal polity are conceived of as self-sufficient and autonomous, where do children, the aging, and those temporarily or permanently in need of care—more generally—reside? Are they accorded a status somewhat (or possibly entirely) less than “citizen” and thus relegated to the social periphery? Or, is the issue of “need” fundamentally outside the domain of the liberal state and assigned, thereby, to domestic spaces in which women are most often situated—by choice, hire, or otherwise? Does the work of care then constitute—by innate virtue—the “work of women,” or is it an effect of unequal configurations of power inherent within a patriarchal liberal state?
Questioning the elements and social implications of liberal individualism in this manner has been the work of care theorists for several decades, beginning for most with that of Nancy Chodorow (1978) and Carol Gilligan (1982). Although since critiqued for obfuscating the social construction of gender and asymmetrical power relations between the sexes (e.g., Brown, 1995), engendering biological determinism (e.g., Moody-Adams, 1991), and reifying a particular conception of “femininity” (e.g., Deveaux, 1995), Gilligan’s work, in particular, outlined two perspectives to moral/ethical reasoning: one in which rationality is central to the attainment of justice and the other which elevates caring as a means through which needs are met. The latter’s emphasis on relationality and interdependence, particularly as they juxtapose the former’s liberal notions of independence and autonomy, was and continues to remain central to the scholarship of care theorists (e.g., Daly, 2002; Dalley, 1996; Graham, 1983; Held, 2002; Nakano Glenn, 1992, 2000; Robinson, 2006a, 2006b; Sevenhuijsen, Bozalek, Gouws, & Minnarr-McDonald, 2003; Thomas, 1993; Tronto, 1993; Ungerson, 1983; Williams, 2001, 2011).
Contemporary Foci
Expanding the geopolitical analysis further, several scholars argue that an insular focus on gender obfuscates the impact of other socially oppressive domains—race, class, and legal status, for example—and falsely universalizes the experience of women (e.g., Nakano Glenn, 1985, 1992). Explicit attention is brought to the ways in which women do not universally “share the same lot” (hooks, 1984), such that the liberation of some from the “oppressive ranks” of domesticity has led to the encumbrance of others (Brown, 1995; Ehrenreich & Hochschild, 2002; Harrington, 1999; Nakano Glenn, 1985, 1992; Robinson, 2006a, 2006b; Williams, 2001, 2011). As posed by Parker (1981), one must ask “who is left to perform the tasks of caring…and what implications [does that have] for the social and economic distribution—or re-distribution—of opportunities, status and freedoms” (p. 31)?
In questioning the displacement of caring labor in this way, several scholars critically interrogate the intersection of globalization and immigration in particular (Graham, 1991; Hankivsky, 2006; Harrington, 1999; Hochschild, 2002; Mahon & Robinson, 2011; Nakano Glenn, 1992; Parreñas, 2005; Raghuram, Madge, & Noxolo, 2009; Razavi, 2007; Robinson, 2006a, 2011; Sassen, 2002; Tronto, 2011; Williams, 2001). As suggested by Barbara Ehrenreich and Arlie Hochschild (2002), the extraction of resources from the South to the North has historically transformed to include not only material but also human resources, in which “…love and care [have] become the ‘new gold’” (p. 26). Immigration and citizen-related concerns regarding a “care drain,” and resulting “global care chains,” include the ways in which the children, families, and communities of migrating women are deprived care providers; the social conditions under which these women “consent” to labor within the Global North; the ways in which the readily available, “low-cost” (poorly compensated) care labor distorts the extent of care needs within Northern social policy; and the perpetuation of gendered divisions and devaluation of caring on a global scale (Harrington, 1999; Hochschild, 2002; Mahon & Robinson, 2011; Robinson, 2006a, 2011; Sassen, 2002; Williams, 2011).
Such concerns—and the social justice and human rights implications therein—have fostered continued exploration of the mechanisms through which care is devalued due to its social and cultural association with women and mothering more generally (Cancian & Oliker, 2000; England, Budig, & Folbre, 2002; England & Folbre, 1999; Folbre, 2001; Folbre & Nelson, 2000). Paula England, Budig, and Folbre (2002) have, for example, explored not only sex but also care-related wage penalties for nearly two decades, finding an average 5–6% pay penalty for those engaged in caring labor, even after controlling for education level, worker’s labor background/experience, and job characteristics. Similarly, based on a multivariant analysis of data obtained from 12 countries spanning the globe (e.g., Finland, France, Hungary, United States, Mexico, etc.), Michelle Budig and Joya Misra (2010) find a consistent care-related wage penalty, particularly in those nations experiencing greater inequality (e.g., United States), lower union density, and minimal public spending on care; therein, underscoring that political context does matter.
Joan Tronto (1993) situates such findings within the larger critique and sociopolitical context of liberalism. That is, she suggests that framing care as innately natural, feminine, private, and an emotionally based response to needs positions care as the conceptual opposite of those qualities valued within liberalism, namely, masculine, public, autonomous, and rational. And, it is precisely this—the reality that care framed as such “embodies [liberalisms] opposites” or as Wendy Brown might suggest—its constitutive others—that leads to its continued devaluation (1995, p. 117). Thus, attempting to advocate for more caring social/public policy or “developing an institutional context that facilitates the work of care” without reconceptualizing care, theoretically and in practice, “may seem an impossible if not outright contradictory project” (White, 2000, p. 1).
Toward that end, Virginia Held (2002) offers a response by advocating for alternative models within a larger critique of liberal individualism. In so doing, she suggests that a particular shortcoming of liberalism lies in its failure to respond to questions concerning the marketization—or not—of caring labor. One might assert, for example, that the market fails to ensure equal access to food, shelter, and health care, thus calling upon a “government concerned with justice” to intervene. Bearing witness to the increasing decentralization of many Western welfare states, one notes that such intervention increasingly involves ensuring individuals are able to reenter the market to purchase said necessities via, for example, supplemental nutrition assistance, housing and school vouchers, and subsidized health care. Virginia Held (2002) suggests, however, that: Liberal individualism does not seem to address such questions as whether the institutions providing the food, the housing, the medical care, and the education, should be private and profit-making, or cooperative and socially responsible, whether, in other words, they should be in or out of the market and governed or not governed by its values. (p. 28)
Cooperative Possibilities
In contrast, the “third sector of the economy,” comprised of nonprofit entities that “fit neither the standard capitalist nor standard public-enterprise models” present an alternative, hybrid approach that “…offers local governments resources to meet care needs but encourages subcontracting to small businesses that can be held accountable for high quality” (Folbre, 2008, p. 384). In discussing recent trends within the United Kingdom toward this end, Nancy Folbre (2008) suggests that “Worker-owned businesses and cooperatives offer a particularly promising model for care provision” (p. 384). Furthering this claim, Held (2002) suggests that local, community-based cooperatives—“would not be governed by market principles…and that [they] might value care in entirely appropriate ways” (p. 24). The value of care, that is, would (likely) take priority over economic gain (Pestoff, 1992).
Classical cooperative theory
Several social theorists and reformers have long supported the implementation of cooperatives to address deleterious labor conditions and facilitate social transformation premised on greater equality and justice. Proudhon ([1923]2007), for example, argued that the increasing divisions of labor rendered the actual producer—the laborer—as “subordinated, exploited” and resulting in a “permanent condition defined by obedience and poverty” (p. 216). As an alternative, he advocated for the development of “worker associations” or cooperatives in which the laborer “resume[s] [her/]his dignity as a [wo]man and citizen,…may aspire to comfort,…and forms a part of the producing organization of which [s/]he was before but the slave” (p. 216). Likewise, writing from a classical reformist position, Bernstein (1911) suggests that cooperatives are uniquely positioned—if sufficiently financed—to facilitate improvements in the social order, particularly within the “domain of public service” (p. 124).
Contemporary significance
Based on a recent online survey of 581 individuals and 14 semi-structure interviews among those (directly and indirectly) associated with cooperatives throughout the globe, cooperatives were reported to enhance negotiating power related to contractual labor agreements and foster greater transparency with payments for service—both of which enhanced women’s income (International Labour Organization [ILO], 2015, p. 9). Likewise, the democratized nature of cooperatives supported collective action to enhance labor conditions and provided greater flexibility to support work/life balance (i.e., greater time to be with/care for members’ own kin). And, most recently, based on a survey of 182 online respondents and 29 key informant interviews, the ILO (2016) finds that “Cooperatives foster interdependency in care by privileging equitable inclusion and democratic decision-making across the care chain,” such that care recipients and providers are active participants in determining the scope and nature of care provision (p. 4). Several benefits experienced by cooperative members were noted, to include provision of “paid sick leave (34%), paid maternity leave (31%), a guaranteed-hour work week (30%)”, and collective protection for members lacking legal status (p. 22). In addition, a small number of cooperatives noted provisions for paid paternity leave, asserting an organizational analysis of and commitment to addressing gendered divisions of care.
Exploring the values underlying care theory and the cooperative model more directly, the complementary nature of the two clearly emerges. Joan Tronto (1993) suggests that an ethic of care is premised on valuing notions of responsibility, competence, attentiveness, and responsiveness. Similarly, the International Cooperative Alliance (2012) outlines the following values as foundational in guiding the development and governance of cooperatives: caring for others, social responsibility, democracy, equality, and solidarity. With the alignment among theoretical and applied values, it appears that cooperatives involved in the provision of caring services might be well positioned to provide—as suggested by Held (2002)—a decentralized, community-based model that institutionally values care. To explore this more directly, a case example of a worker-owned, community-based childcare cooperative is offered.
Childcare Case Example
Current Configurations of Labor
The labor conditions of childcare workers have come to be defined by chronically low—at times poverty level—wages, poor (if any) benefits, and lack of advancement opportunities (e.g., Cleveland, Forer, Hyatt, Japel, & Krashinsky, 2007; U.S. Department of Labor, 2014; Whitebook & Sakai, 2004). Based on a survey of occupational earnings, the U.S. Department of Labor (2014) estimates the median hourly wage of nearly 600,000 U.S. childcare workers to be US$9.48, with a corresponding annual median wage of US$19,730. Occupations exhibiting comparable median wages include locker room, coatroom, and dressing room attendants (US$9.59); dishwashers (US$9.03); fast food cooks (US$9.15); short order cooks (US$9.71); and baggage porters and bellhops (US$10.06; U.S. Department of Labor, 2014).
Based on a sample of 659 childcare workers within the San Francisco Bay Area, Whitebook and Sakai (2004) report that despite the fact that 37% of the lead childcare teachers (n = 435) held a bachelor’s degree in addition to an average of 11 years working within the childcare field, their salaries constituted two thirds of the local self-sufficiency wage, defined as the minimal income needed to acquire basic needs without public or private assistance (Pearce & Brooks, 2002). Labor condition as such is thought to directly contribute to a median job tenure of only 2.7 years and an annual turnover rate of approximately 30%—a rate nearly twice that of most occupations, including other child-related jobs such as elementary school teacher (Deery-Schmitt & Todd, 1995; Doherty-Derkowski, 1995; Organisation for Economic Co-Operation and Development [OECD], 2006; Whitebook & Sakai, 2004).
Worker-Owned Cooperative Alternatives
Seeking alternative configurations of labor that structurally prioritize both quality care and labor, worker-owned cooperatives have emerged as innovative, yet time-tested organizational form (Curl, 2009), particularly in sectors with low-profit margins (e.g., direct care home health aides, childcare; see Inserra, Conway, & Rodat, 2002; Stone, 2004) and among care/service workers and communities of color (Flanders, 2014; Nembhard, 2014; Savitch-Lew, 2015). Defined as a “business that is owned and controlled by the people who work in it,” a worker-owned cooperative is governed according to two primary principles: (i) worker ownership and profit sharing and (ii) democratic decision-making (e.g., one worker = one vote; U.S. Federation of Worker Owned Cooperatives, 2015). And, although a comprehensive survey of worker-owned cooperatives within the United States has yet to be conducted, recent estimates suggest a steady rise in this organizational form over the past 20 years resulting in greater than 300 “democratized” workplaces providing employment to more than 3,500 people and garnering yearly revenues in excess of US$400 million (U.S. Federation of Worker Owned Cooperatives, 2015). With respect to childcare in particular, one organization, the Beyond Care Childcare Cooperative (BCCC), is a particularly illustrative example.
BCCC is a worker-owned cooperative providing childcare services in the Sunset Park neighborhood of Brooklyn, NY. In late 2006, the Center for Family Life (hereafter referred to as the Center), a nonprofit, community-based organization providing various services (e.g., family counseling, foster care services, school-based programs, youth and adult employment programs) to the Sunset Park Community since 1978, recognized that their community—of which approximately 90% are immigrants—was facing significant employment barriers. As the Center’s cooperative development director at the time, Bransburg, LMSW, suggested that many of the women were engaged in domestic services and/or babysitting, often on a part-time basis further impacting their already low-earning potential (V. Bransburg, personal communication, October 6, 2013).
In response, the Center sought the guidance of Women’s Action to Gain Economic Security (renamed Prospera: http://prosperacoops.org/), an Oakland, CA-based nonprofit cooperative developer committed to building worker-owned, eco-friendly cleaning cooperatives among immigrant Latinas for more than 20 years, to explore the possibility of supporting the launch of a local worker-owned cooperative. The Center began to explore the possibility in their English as a Second Language (ESL) classes and family-counseling program, with overwhelming positive feedback. As the Center’s coop development director suggested, “Many of these women come from countries with a strong history of worker cooperatives, so the idea was not new to them…and they were really interested” (V. Bransburg, personal communication, October 6, 2013). In 2006, the Center helped incubate the first women’s worker-owned coop—Si Se Puede— which provides household cleaning services, the success from which quickly spawned interest in cooperative, home-based childcare services.
And, in June of 2008, the BCCC was launched as a “nonprofit cooperative corporation.” The nonprofit structure was chosen as it was the most cost-effective (i.e., would not require a formal office with central bookkeeping, payroll, etc.) and time-effective model that enabled members to continue to provide services in much the same way as their previous work as independent nannies. As a result, contracts are drawn between clients and individual members and not the cooperative. The revenue that is generated from individual clients goes directly to the member providing service, minus the current US$100/month membership fee (which collectively covers the costs of a full-time office manager’s salary and benefits, utilities, administration, cooperative developer consultation, marketing, childcare during meetings, trainings, etc.). The full-time office manager provides support to new members by updating resumes/references and practice interviewing and negotiation as well as scheduling and assigning new jobs based on member’s established criteria emphasizing equity.
The initial 19 founding members of BCCC—Las Fundadoras—participated in a no-cost, 10-week orientation offered by the Center in 2008, which presented topics covering Cardiopulmonary resuscitation (CPR) certification, child development, cooperative values and principles, brand development, and the establishment of organizational/operating rules and norms. Following graduation, each of the members committed a substantial amount of time—“sweat equity”—to prepare for the launch of the cooperative in lieu of an initial “share cost.” This process involved developing their business structure, cooperative bylaws, governing principles, and the development of several committees (e.g., leadership, publicity, and training). During this process, the women elected to use consensus decision-making for the majority of their decision, while utilizing majority vote for the largest decisions.
Since its inception, BCCC has provided services to approximately 1,200 individuals/families and currently provides ongoing services to approximately 345 families. Given the success and increasing demand for services (based on a referral model), BCCC has opened its membership 5 times to new members, which has more than doubled its membership with 36 (as of February 2016) current member owners. Upon joining, new members are expected to participate in a five-session training program covering topics such as child development, CPR, child health, and workers’ rights, with a current cost of US$145. Currently, approximately 14 (39%) members work full time (40–50 hr/week), earning an average of US$600–US$750/week (depending on the number of children in care). The remaining 22 members (61%) work a mix of part time (3–39 hr/week) and “rapid care” (clients calling with 24 hr or less notice), earning US$16–US$22/hr, depending on the number of children in care. Several members have also joined a member-run advocacy organization—Domestic Workers United—to advocate for improved working conditions of all domestic workers (www.domesticworkersunited.org).
Based on the coop’s success, the Center sponsored a survey in April 2010 among Las Fundadoras to assess more systematically how participation in the Coop had impacted employment, economic, and emotional well-being. Results indicate (see Table 1) that prior to joining the coop, 53% of the women were employed primarily in the service (childcare, cleaning) and/or textile sectors working, on average, 30.7 hr/week and earning US$8.73/hr (US$268/week). With respect to their social and emotion well-being at this time, results indicated high rates of stress/anxiety, loneliness/isolation, depressive thoughts, and a lack of adequate time to spend with their families. In contrast, following their joining of BCCC as worker-owners, the women reported a 58% increase in hourly wages, positive improvements in their emotional and psychological well-being, increased self-esteem, greater confidence in advocating for their needs, greater time with their own families, and increased confidence as mothers.
Labor Conditions and Indicators of Well-Being Prior to and Following Joining BCCC.
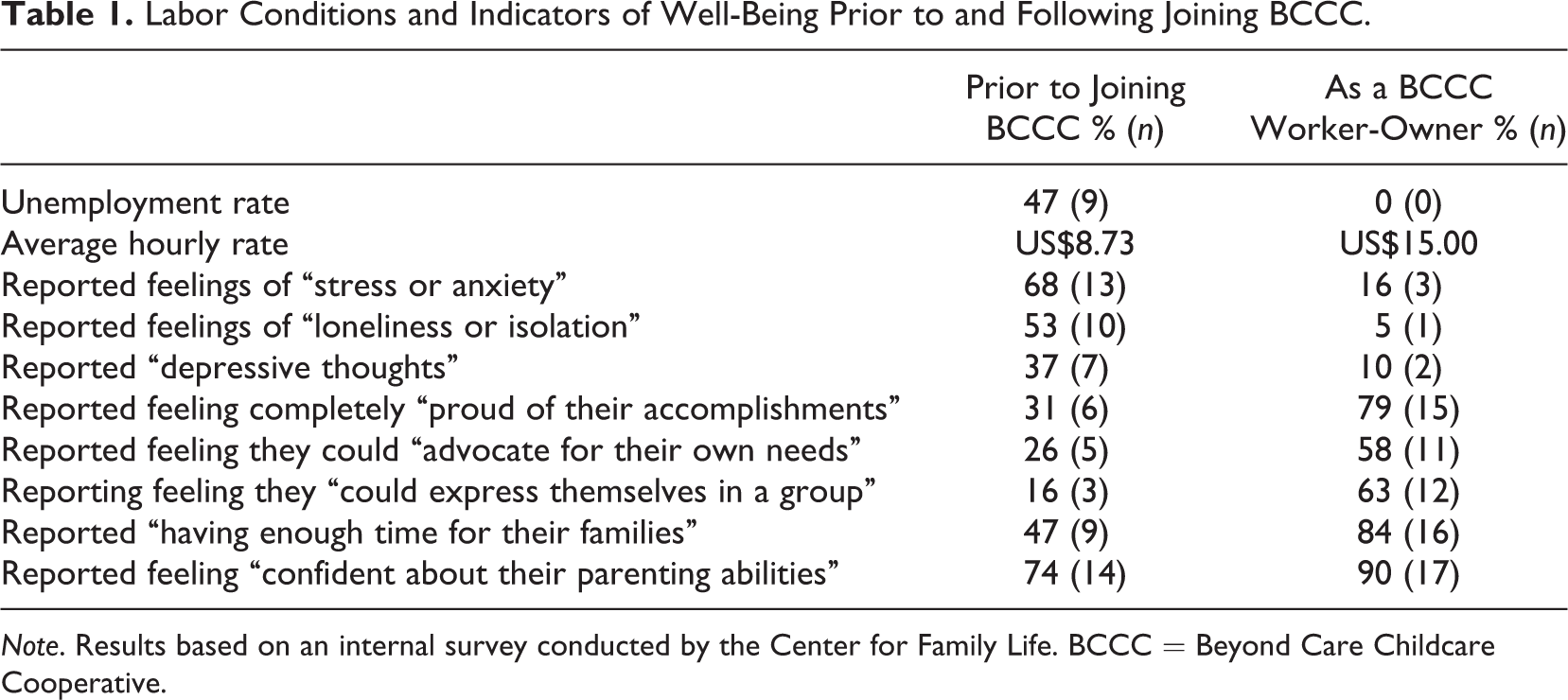
Note. Results based on an internal survey conducted by the Center for Family Life. BCCC = Beyond Care Childcare Cooperative.
These results highlight the ways in which BCCC has been able to achieve and, in many ways, surpass it stated goal of “creating living wage jobs that will be done in a safe and healthy environment, as well as to provide social supports and educational opportunities for [its] members” (http://www.beyondcare.coop). It has, for example, increased the hourly wages of members previously earning an average of US$8.73/hr to approximately US$15/hr (for full time, with US$16–US$22 for part time depending on the number of children in care), considerably higher than the industry median of US$9.48/hr and New York’s hourly average of US$12.37 (U.S. Department of Labor, 2014). Given such a significant wage increase, many (61%) of the current worker-owners have, moreover, elected to work part time (15–25 hr/week) to support increased time with their own children (V. Bransburg, personal communication, November, 15, 2015). Finally, BCCC notes a significant improvement in the employment stability of its growing membership (of whom 50% were previously unemployed or partially employed), noting an average yearly rate of 6.8% turnover (ranging from 0%–26.5% between 2008 and 2015; see Table 2), significantly lower than the industry average of 30% per year (OECD, 2006; Whitebook & Sakai, 2004). And, of those who are no longer owner-members of BCCC, the average length of employment was 18 months, with the following noted as reasons for leaving: return to school (e.g., graduate school; accounting degree), termination, pursuit of cooperative development work, and personal reasons.
Annual BCC Membership and Turnover.
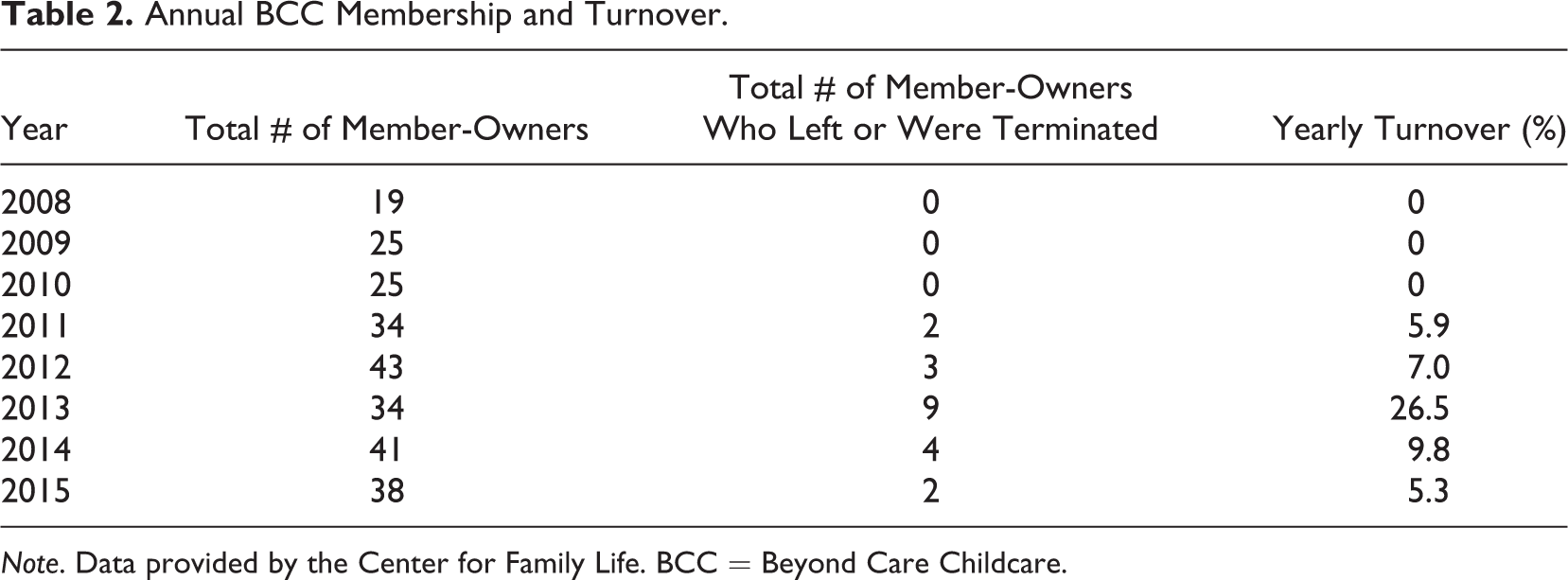
Note. Data provided by the Center for Family Life. BCC = Beyond Care Childcare.
Conclusion
By calling upon feminist scholarship, particularly that which interrogates the conditions under which caring labor is or might be rendered, the fallibility of liberal individualism to adequately define and thereby respond to care needs is emphasized. In particular, Brown’s analysis (1995) draws attention to the implicit, dualistic assumptions of liberalism and, in doing so, attempts to decenter the discourse of rights and autonomy and elicit questions such as equity, freedom, and autonomy for whom, on what terms, and at what or whose expense? In summoning a response to such questions, a discourse of universal need, social connectivity, and interdependence thus emerges as a viable and alternative discourse through which to reconceptualize and, thereby, respond more justly to growing care needs.
Said care needs are, moreover, rising exponentially given unprecedented demographic shifts in the aging population. The United Nations (2013) projects a near doubling of the global aging population (60 years and over), increasing from “841 million people in 2013 to more than 2 billion in 2050” (p. xii). Within the United States alone, the population of those 65 and over is projected to increase from 43 million (13.7%) in 2012 to nearly 73 million (∼20%) in 2030 (Ortman, Velkoff, & Hogan, 2014). Such a staggering rise in care demands has heightened concerns regarding not only access, cost, and quality of care but also the conditions under which this labor is being delivered—increasingly so within market-based settings (e.g., Kochera, Straight, & Guterbock, 2005; Poo & Conrad, 2015; Raghuram et al., 2009; Razavi, 2007; Wielink, Huijsman, & McDonnell, 1997).
Recent estimates suggest that more than three million direct care workers—certified nursing assistant/aides, home health aides, and personal and home care aides—are providing “70 to 80 percent of the hands-on, long-term care and personal assistance” to aging or disabled Americans (Paraprofessional Health Institute [PHI], 2011, p. 1). Such demands have led to personal-care aides and home health aides, in particular, becoming the “fastest growing occupations” in the country, with the overall demand for workers topping 5 million by 2020 (2011, p. 2). However, alarming to many are the ways in which the demographic composition of these carers parallels those found within the childcare sector, namely, middle-aged (average of 41 years) women (89%) of color (53%), who earn a median annual salary of US$17,000 (or US$14,000 among personal and home care aides) resulting in a significant number (49%, or nearly one in two) relying on public benefits such as Medicaid or Supplementary Nutrition Assistance Program to support themselves and their families (PHI, 2011, p. 1).
Attempting to respond to rising care demands with a keen understanding of the ways in which “quality jobs = quality care” (http://phinational.org/), the development of worker-owned direct care cooperatives in the United States has sharply increased to include Golden Steps Cooperative Worker Owned Coop in Brooklyn, NY; Cooperative Care of Wautoma, WI; Circle of Life Caregiver Cooperatives in Bellingham, WA; and the Cooperative Home Care Associates (CHCA) of the South Bronx, NY (Egerstrom, 2013; Johnson, n.d.). Founded in 1985, CHCA stands as the largest worker-owned cooperative in the United States currently employing more than “2,000 home care workers in the South Bronx and generating revenue upward of US$40 million” (ILO, n.d., p. 18). As noted by Inserra, Conway, and Rodat (2002), “the worker-ownership structure was emphasized as a way to maximize wages and benefits in businesses with low profit margins, and to ensure that workers’ interests would receive priority in the business strategy of the firm.” (pp. 18, 19). Toward that end, they have and continue to offer their member-owners no-cost initial and ongoing training, health insurance, career advancement opportunities, paid vacation and leave time, a retirement plan option, and yearly dividends averaging between US$200–US$400 (Inserra et al., 2002, p. 60).
As evidenced in the BCCC case example, cooperative owner-membership positively impacts—individually and collectively—the social, economic, and emotional well-being of women who, prior to, occupied exceptionally vulnerable positions within the labor market precisely because of their gender, racial, and cultural identity and immigration status. Given, for example, the near doubling of their wages, more than half of BCCC worker-owners have chosen to reduce their work week to 15–25 hr/week to facilitate a work/life balance that allows for greater time with their own children and families, a significant “policy” shift called for by many feminist scholars (e.g., Nakano Glenn, 1985; Williams, 2001). These findings are also reflected in national and global research indicating positive associations between cooperative involvement and enhanced wages and benefits (to include sick, maternity, and occasionally paternity leave), by virtue of, for example, enhanced negotiating power, payment transparency, guaranteed-hour work weeks, flexibility to support work/life balance, and collective protection for members lacking legal status (DeFilippis, 2004; ILO, 2015, 2016; Inserra et al., 2002; PHI, 2011; Stone, 2004).
These findings, although preliminary, emphasize the critical importance of continued research on the worker-owned cooperative model and its impact on labor conditions as well as the social and emotional well-being of those (women) proving caring and service-oriented labor. Toward that end, mixed-methods comparisons of differences with respect to these outcomes as they relate to various organizational forms (i.e., for-profit, nonprofit, and worker-owned cooperatives) as well as in-depth analyses concerning the reflections, insights, and quality assessments of those consuming said services (directly or indirectly) are needed. Therein, specific attention should be brought to bear on the mechanism through which cooperatives do or might serve to counterbalance the devastating effects of global care chairs (Hochschild, 2002; Mahon & Robinson, 2011; Robinson, 2006a, 2011; Sassen, 2002) by organizationally prioritizing the labor conditions, well-being, and ability of members to maintain kin relationships (Nakano Glenn, 1985).
Final Thoughts
Given the current constellation of care demands and the sociopolitical and economic context in which care is being rendered, the challenge to seek out alternative configurations of caring labor that prioritize the dignity and well-being of both care recipient and provider has never been more urgent. In so doing, the decentralized, community-based, worker-owned cooperative model emerges as a promising organizational form through which to accomplish said aims by structurally prioritizing the values and practice of democracy, equity, and solidarity (Flanders, 2014; Nembhard, 2014; Poo & Conrad, 2015; Savitch-Lew, 2015; Stone, 2004). Further exploration of this model and its positive impact in the lives of care providers today is seen as complementary to a larger constellation of longer term local, national, and global policy reforms attempting to underscore human interdependence, universality of care needs, and thereby, redress gendered divisions of caring (e.g., Finch, 1983; Mahon & Robinson, 2011; Tronto, 1993, 2011; Williams, 2011). Toward that end, ongoing evaluation of, for example, the development and impact of a “caregiver’s allowances or citizen wage; taxation allowances; different types of paid and unpaid leave from employment; social security credits and social services” (Razavi, 2007, p. iv) is critically important to fostering responsive, equitable, and dignified caring policy in the future.
Footnotes
Acknowledgments
The authors greatly acknowledge the worker-owners of the Beyond Care Cooperative (BCCC) who—individually and collectively—exemplify the ways in which democratized labor is shifting the caregiving landscape with equity and justice as its guideposts. We would also like to extend our gratitude to the Center for Family Life for their willingness to provide pertinent information regarding BCCC and their ongoing support and development of worker-owned cooperatives in the Sunset Park neighborhood of Brooklyn, New York.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.