
Abstract
This article investigates the relation between history of intrafamilial violence and self-regulatory capacity, cognitive processing, and mental health adjustment in incarcerated adolescents. Adolescents were incarcerated at the time of the study for various violent offenses, ranging from persistent delinquency to sexual assault (n = 115). A model is proposed that posits that self-regulation, cognitive ability, and cognitive processing are integral to the relation between intrafamilial violence and mental health function. The primary hypothesis of the study tests this mediation model. The relations between mental health, cognitive processing, self-regulation, and intrafamilial violence are also examined. The study was conducted during two sessions at a juvenile facility in the Midwest using survey measures, academic and intelligence testing, and cognitive tasks. Youth were between the ages of 13 and 20. Approximately 70% were previously diagnosed with a disability. Significant Pearson’s correlations were found between seven out of eight mental health subscales of the Youth Self-Report (YSR) and intrafamilial violence history. Structural equation modeling was used to examine the role of cognitive processing in the association between intrafamilial violence and mental health function. Nonverbal or performance deficits, a significant difference between verbal skills and nonverbal skills, were related to intrafamilial violence. Self-regulation partially mediated the relation between intrafamilial violence and mental health function. Self-regulation ability may be compromised by intrafamilial violence and be a precursor to both internalizing and externalizing mental health problem in incarcerated youth. Educational, clinical, and research implications are discussed.
Introduction
Intrafamilial violence is often a precursor to later mental health problems in children (Higgins, 2004), including both internalizing problems, like depression and anxiety, and externalizing problems, like aggression and delinquency. The mechanism that leads from intrafamilial violence to later internalizing and/or externalizing mental health problems remains unclear. Self-regulation and cognitive processing deficits are related to both intrafamilial violence and mental health problems and may mediate the relation between those two constructs (Buckner, Mezzacappa, & Beardslee, 2009; Jonson-Reid, Drake, Kim, Porterfield, & Han, 2004).
Cognitive processing is a broad term used to describe the ability to manage information using capacities including intelligence, planning, processing speed, memory, attention, and executive control, including self-regulation. Self-regulation is an essential underlying component to all cognitive processing, necessary for the down-regulation of emotion and up-regulation of cognitive skills necessary for the completion of academic or social goals (Efklides, 2008). Self-regulatory deficits are demonstrated in children exposed to violence (Dodge & Crick, 1990; Merwe & Dawes, 2000), which suggests that one possible contributing factor to the development of mental health problems after childhood exposure to violence is deficit in self-regulation.
Intrafamilial violence, Mental Health, and Achievement
Multiple studies have documented the negative influence of intrafamilial violence on subsequent internalizing, externalizing, and academic achievement. Although many studies examine internalizing and externalizing mental health separately, the overlap in these concepts leads us to take a more holistic approach to mental health function. Overall levels of intrafamilial violence (Hanson et al., 2008; Margolin, Vickerman, Oliver, & Gordis, 2010), exposure to domestic violence (Graham-Bermann, Gruber, Girz, & Howell, 2009), maltreatment (Haapasalo, & Virtanen, 1999; Hosser, Raddatz, & Windzio, 2007), sexual violence (Reed et al., 2009), and community violence (Ruchkin, Henrich, Jones, Vermeiren, & Schwab-Stone, 2007) are all related to deficits in mental health functioning. Exposure to family violence is also related to cognitive capacity, including lower achievement scores (Thompson & Wyatt, 1999) and verbal and full-scale intelligence (Graham-Bermann, Howell, Miller, Kwek, & Lilly, 2010).
Mechanisms of Cognitive and Self-Regulation Mediation
Criminal justice theory focuses on self-control as a factor in the development of criminal behavior (Gottfredson & Hirschi, 1990). Self-control theory posits that low self-control is a mediator between various ecological factors, including schooling and parenting, and later criminal behavior (Gottfredson & Hirschi, 1990). Low self-control is defined in the literature as a range of both psychological processes and behaviors and researchers postulate that self-control is fixed by the age of about 10 (Winfree, Taylor, He, & Esbensen, 2006). In contrast, Bandura’s social cognitive theory (1986) defines self-regulation as involving self-observation and behavioral monitoring, and as a component of cognitive control, which is neuroanatomically centered in the prefrontal cortex; self-regulation is known to develop well into the 20s (Casey, Jones, & Hare, 2008).
In schools, self-regulation is necessary for self-judgment of academic progress and reaction to performance outcomes (Bernier, Carlson, & Whipple, 2010; Buckner et al., 2009; Mischel et al., 2011). Self-regulation is a broad term used to encompass a variety of cognitive volitional activities in humans and is dependent on a complex neurocognitive network (Mischel et al., 2011). The development of self-regulation is dependent on early childhood experiences within the family (Bernier et al., 2010) and is influenced throughout the lifespan by experience, including schooling, and can be improved through training (Tang et al., 2007). The ability to self-regulate emotional response during times of high cognitive load is central to flexible responding during learning (Eccles & Wigfield, 2002). Self-regulated learners use active learning and possess a belief that they can perform efficaciously and set achievable academic goals (Eccles & Wigfield, 2002). In this sense, self-regulation is a mechanism that can be seen as an extension of self-control theory that links ecological factors with psychological processes.
Miller and Brickman (2004) suggest a component of past experience in the development of future oriented self-regulation. Past experience, success, or failure in learning situations leads to value for the task and knowledge of the possibility for success. Taken more broadly, past experience of abuse and other negative early life stress lead to a diminished capacity for self-regulation (Merwe & Dawes, 2000). According to social information processing theory, children with violence histories and experience with harsh parenting are biased toward threatening stimuli and interpret neutral social cues as negative or threatening (Dodge & Crick, 1990). This heightened threat appraisal is related to avoidant coping, hostility, depression, anxiety, and negative affect, suggesting that the inability to self-regulate negative associations and the subsequent use of avoidant coping may mediate the relation between intrafamilial violence and later mental health function. Self-regulation is a critical component of optimal mental health development and history of intrafamilial violence has a significant negative influence on the ability to develop self-regulatory skills.
A higher rate of both intrafamilial and community violence exposure has been found in both adult and adolescent offenders. In one recent study of adults, using a self-reported measure, sexual abuse by a family member was experienced by 18% of inmates and physical abuse by 50% (Carlson & Shafer, 2010). In incarcerated adolescents, 14% to 19% have substantiated histories of maltreatment (Jonson-Reid & Way, 2001), which suggests that self-report rates would be higher. Intrafamilial violence is a risk factor for later criminal behavior. For adults, having been touched sexually prior to puberty results in a 7% to 10% increase in the probability of being incarcerated later in life (Curtis, Leung, Sullivan, Eschbach, & Stinson, 2001). Incarcerated populations also exhibit deficits in self-regulation (Ross & Fontao, 2007). Deficits in self-regulation and any of the broad areas of cognition often result in developmental problems collectively called disabilities.
Terms, like learning disability, encompass multiple facets of cognitive processing, such as intelligence, attention, and processing speed. Approximately 13.4% of the general school age population is served under the Individuals with Disabilities Education Act (IDEA; U.S. Department of Education, 2010). Among juvenile offenders, national rates of disabilities are between 33% and 45% (Krezmien, Mulcahy, & Leone, 2008; Quinn, Rutherford, Leone, Osher, & Poirier, 2005). Deficits in self-regulation may be related to the high prevalence of learning and behavioral disabilities in incarcerated populations (Quinn et al., 2005). Direct relations between violence and mental health problems (Hosser et al., 2007, Margolin et al., 2010), violence and cognitive processing (Graham-Bermann et al., 2010), and cognitive processing and mental health suggests that cognitive processing deficits may be an underlying mechanism in the relation between intrafamilial violence and mental health.
In the present study, we conceptualize self-regulatory capacity as a developmental construct and measure the current level of functioning within a framework of developmental psychopathology rather than as a fixed capacity. We believe that differences in current level of cognitive processing ability (including self-regulation) may mediate the relation between past history of intrafamilial violence and current level of mental health functioning in an incarcerated population. Community violence and the cumulative exposure to different forms of violence also have deleterious effects (Margolin et al., 2010). In the current study we focus on intrafamilial violence to isolate the effect of intrafamilial violence from the very high rates of community violence exposure in this population. The high rates of intrafamilial violence, cognitive processing deficits, and mental health problems in this subpopulation make this group especially appropriate for examining these complex interactions. The current study aims to further our understanding of the interdependence between these constructs in a population of violent and nonviolent youth offenders. Specifically we postulate that cognitive processing deficits, in general, and self-regulation, in particular, may mediate the relation between intrafamilial violence and mental health problems. It is first hypothesized that incarcerated adolescents will show a direct relation between intrafamilial violence and mental health functioning. In addition, it is hypothesized that this relation will be partially mediated by cognitive processing, learning, or self-regulatory problems.
Method
Design
The study was conducted at a youth incarceration facility in Michigan and included survey data, individual cognitive and neuropsychological assessment, and educational records review. Permission to conduct the study was obtained from the University of Michigan Institutional Review Board and the State of Michigan Office of Human Services. A Certificate of Confidentiality was obtained from the National Institutes of Health.
Consent was obtained for the study from parents or the court (for wards of the state) before asking the minors for assent to participate. Letters were sent to parents with consent documents attached. If there was no response to a second letter and the juveniles were covered under Delinquency Act 150, we asked that the State Department of Human Services give permission for the youth to participate in the study. Legal adults (those youth above 18 years) were asked to sign participant consent. After parent/guardian, court, or Human Services permission was granted, each youth was contacted individually to obtain assent. Researchers explained that the study was voluntary and that no consequence positive or negative would result from participation or refusal to participate. If necessary, assistance with reading the surveys was provided. Youth were not compensated directly for participation in the study. Instead, a donation was made to the facility for purchase of recreational equipment.
Participants
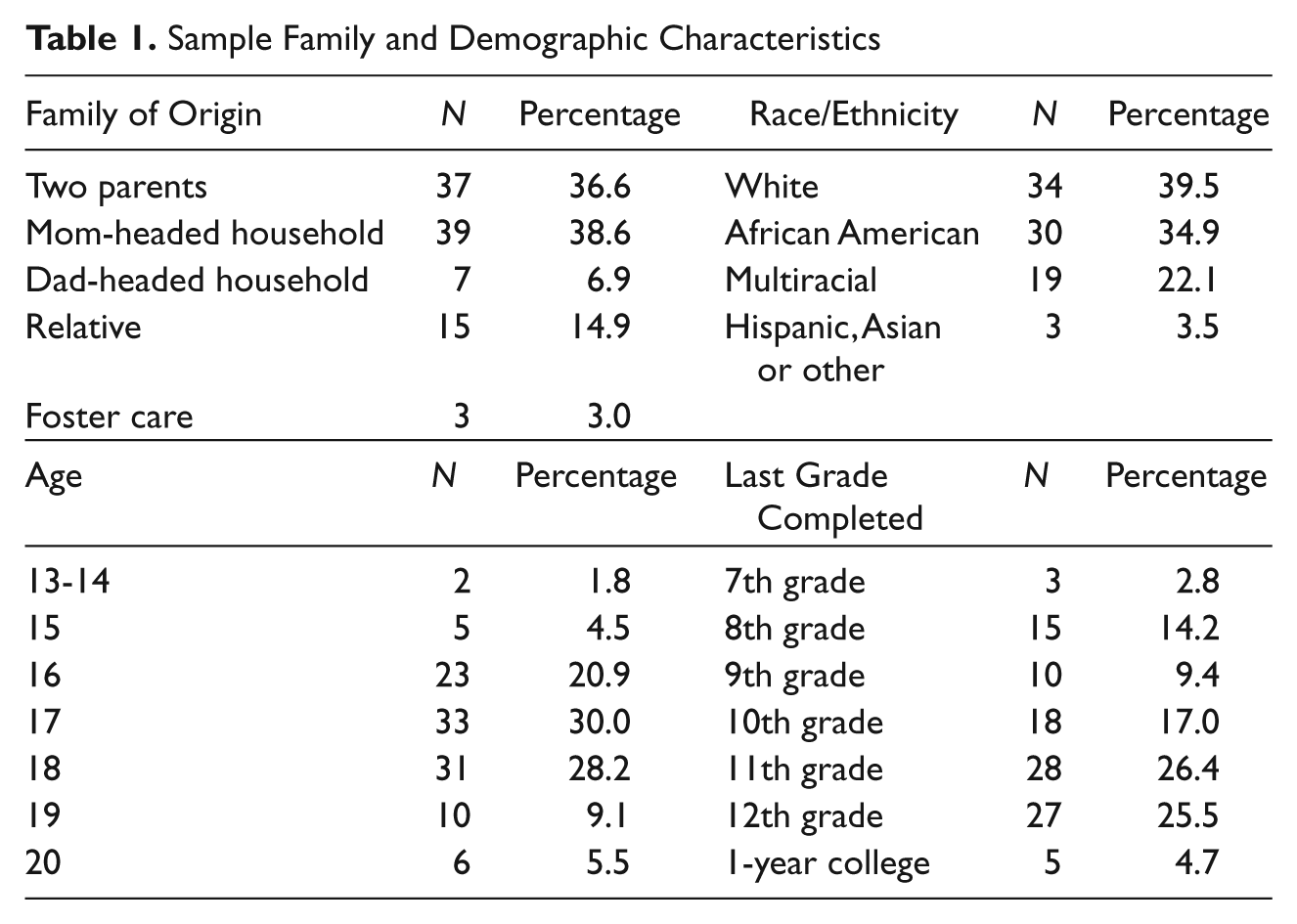
The sample consisted of 115 males that ranged in age from 13 to 20 with a mean age of 17 (SD = 1.304). Ethnicities were approximately one third African American, one third White, and one third self-defined as mixed ethnicity. Grade levels were between 7th and the 1st year of college (see Table 1) Crimes committed prior to the study ranged in seriousness and in type (see Table 2).
Sample Family and Demographic Characteristics
Percent of Sample Offense Type and Class

Note: There were no Property Class 2 violations.
Measures
Intrafamilial violence was measured using an adapted version of the Conflict Tactics Scale (CTS; Straus & Gelles, 1990) to assess how conflicts in the family are handled on a 1 to 5 Likert-type Scale where 1 is equal to never and 5 equals every day. Internal consistency of the CTS was determined as part of the National Family Violence Survey (n = 2,143). This measure has been widely used in incarcerated populations (Haapasalo, & Virtanen, 1999; Hosser et al., 2007; Reed et al., 2009). The CTS was amended to include violence between siblings. Participants were asked to state how often they experienced each of 18 conflict tactics during two time frames; from 6 to 12 and from 13 to 18. The 18 items were repeated within four familial relationship types; parents to participant, parent to parent, sibling to participant, and participant to sibling. Participants were instructed to include any woman who raised them (e.g., grandmothers or foster mothers) as mothers, and any significant male (e.g., boyfriend or foster father) as father. If participants did not have experience with both figures, they were instructed to leave blank the corresponding section.
Although there is likely overlap between sibling to participant and participant we did not include participant to sibling in the present analysis as it most closely represents violence perpetration by the participant rather then experienced by the participant. There existed a high correlation between these subscales. The intrafamilial violence scale used in this study is a sum of total intrafamilial violence at both developmental stages and is defined as total violence from siblings, parents, and intimate partner violence (IPV). Cronbach’s alphas were between .923 and .945.
Mental Health was assessed with the 118-item Youth Self-Report (YSR; Achenbach, 1991) and with the Beck Depression Inventory (BDI). Three subscales were created from the BDI according to the factors derived by Shafer (2006). General Depression (GD), Performance Impairment (PI) and Somatic Complaints (SC). Reliability for the first two scales was moderate but was low for the third factor (GD: α = .79; PI: α = .73; SC: α = .18). Eight subscales of the YSR were derived according to the manual. In this study, reliability of the eight subscales, Withdrawn, Somatic Complaints, Anxious/Depressed, Mood Disorders, Thought Disorders, Attention Problems, Delinquency, and Aggression, range from α = .71 to .97.
A computerized battery included the Wisconsin Card Sort (WCST), a test of strategic planning and cognitive set shifting (Kongs, Thompson, Iverson, & Heaton, 2000) and five cognitive processing tasks: Go—No Go (G-NG), Task Switching (TS; Rogers & Monsell, 1995), Flanker Shape (FS), Shape Matching (SM) and Anti-Saccade Arrows (ASA; Friedman & Miyake, 2004). The response and reaction time (RT) were recorded. Average RTs and percent correct were calculated for each condition. G-NG and ASA are response inhibition tasks. ASA requires oculomotor inhibition. TS required the participant to switch mental sets between two different tasks. The FS and SM tasks require resistance to distracter interference.
Self-regulation was measured using the Behavior Rating Inventory of Executive Function (BRIEF; Guy, Isquith, & Gioia, 2004). In this study, reliability of the eight subscales, Withdrawn, Somatic Complaints, Anxious/Depressed, Mood Disorders, Thought Disorders, Attention Problems, Delinquency, and Aggression, range from α = .71 to .97.
Verbal and nonverbal (or performance) ability were assessed using the Kaufman Brief Intelligence Test Second Edition (K-Bit-2; Kaufman & Kaufman, 2004). Reading, spelling, and arithmetic achievement were assessed with the Wide Range Achievement Test (WRAT-3; Wilkinson, 1993).
Analyses
Missing Data
Thirty-eight participants had missing data on some of the measures. Participants with missing data were compared to participants with complete data across demographic and other key variables. Group differences were not significant. To avoid excessive missing data, means were imputed using an iterative procedure. Missing data were imputed using parameter estimates that were obtained by performing a linear regression of main variables with the variable of interest as the outcome measure. Data had to be present in two thirds of other variables to be imputed. These parameter estimates were then used to impute missing data. For each iteration, a new regression was run to obtain new parameter estimates using imputed data.
Structural Equation Modeling
Structural Equation Modeling (SEM) is similar to multiple regression but takes into account latent constructs measured by multiple indicators to model interaction, measurement error, correlation of error, and interactions. In the current study a model specification process was used to determine mediation (Kenny, 2006). To test the hypotheses above, a model was tested positing that cognitive and learning problems mediate or partially mediate the known relation between experience of family violence and subsequent mental health function. To assess the adequacy of power to detect differences in with or sample size and the number of variables in the SEM, we conducted a power analysis. With 230 df and a sample size of 115, to reject a model with an RMSEA of .10 at a significance level of .05, we have power of 0.9999912 (Preacher & Coffman, 2006).
Results
Descriptive Statistics
Sample characteristics
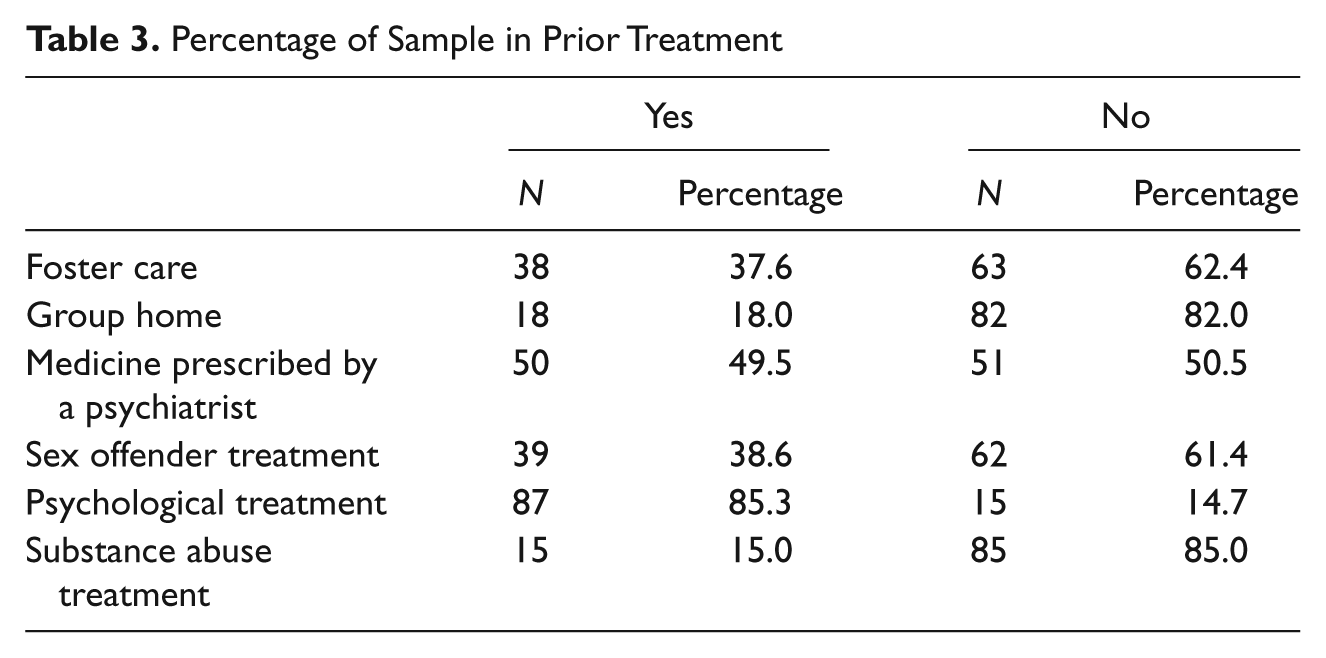
There was a high prevalence of both mental health problems and out-of-home placement in this sample (see Table 3). From the educational records, it was found that 70% had a current Individual Education Plan (IEP) with a lifetime incidence of special education diagnosis of 75.5%. Attention deficit disorder was the most common diagnosis affecting 47% of the population, followed by cognitive impairment and speech problems (approximately 12%).
Percentage of Sample in Prior Treatment
Intrafamilial violence
Mean levels of intrafamilial violence from the CTS ranged from 1.64 to 1.95 (.74-.81 SD) on the four subscales, which is equivalent to a mean level of less than once a year. Approximately 25% of the participants reported IPV of at least a couple of times a year. Thirty-four percent of the sample reported mean maltreatment by parents at least a couple of times a year or more and 46% reported this level of maltreatment by their sibling. Intrafamilial violence was negatively related to nonverbal (or performance) intelligence and positively related to three subscales of the BDI and the withdrawn subscale of the YSR (see Table 4).
Cognitive Processing and Mental Health Measure Means
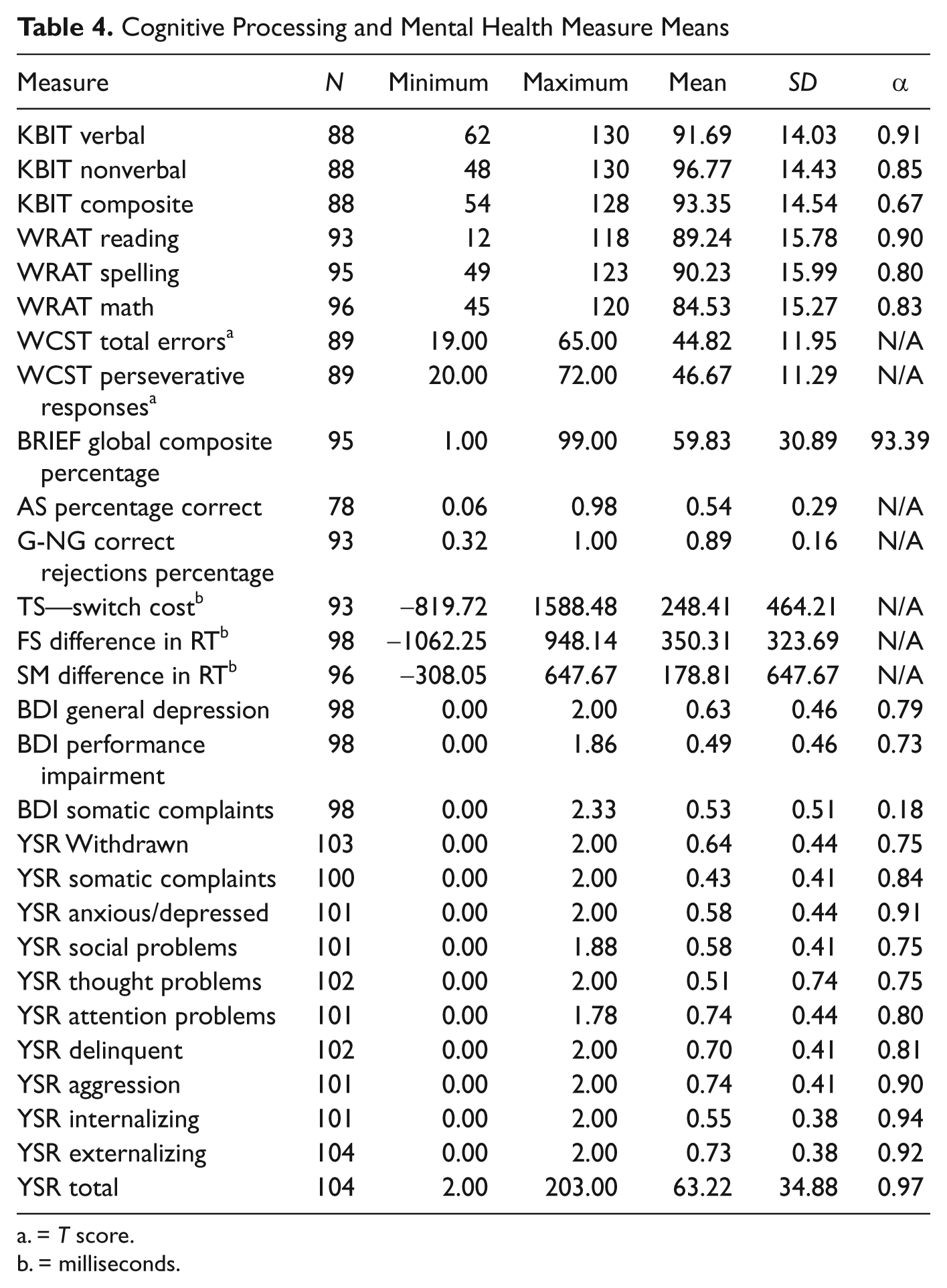
= T score.
= milliseconds.
Cognitive Processing
KBIT means for verbal, nonverbal, and composite IQ were all within the average range. WRAT mean scores for reading and arithmetic were in the low average range. Twelve percent of the population qualified for specific math disability, 7% for reading, and 5.2% for spelling disability. IQ and achievement scores were highly correlated (see Table 5).
Intercorrelations Between Violence, Cognitive Processing and Mental Health Subscales Controlling for Age and Psychiatric Treatment

Note: VE = Violence exposure; PS1 = Wisconsin Card Sort Task factor 1; PS2 = Wisconsin Card Sort Task factor 2; TSW = Task switching; FRT = Flanker RT; SMRT = Shape match RT; AS = Anti-Saccade; GNG = Go/No Go; BI = Behavioral Index; MRI = Metacogntive Regulation Index; GD = BDI General Depression; PI = BDI Performance Impairment; SB = BDI Somatic Complaints; WD = YSR Withdrawn; SY = YSR Somatic Complaints; AD = YSR Anxious/Depressed; SP = YSR Social problems; DEL = YSR Delinquency; AG = YSR Aggression.
< .050. ** < .010. *** = .000.
Self-regulation, as measured by the BRIEF, was highly variable in the population. Clinical T-scores (70 or more) were reported by 16.7% of the population for self-regulation. In terms of cognitive processing, WCST means were all within the normal range but clinically significant T-scores were common (35%—1 measure, 47%—2 or more measures). TS mean RTs were significantly higher during switching than during nonswitching tasks (t = 18.220, df = 98, p = .000). During interference, RT differed between the congruent and the incongruent trials (FS: t = 28.621, df = 97, p = .000; SM: t = 27.2348, df = 95, p = .000). Mean percent correct for AS was 89% and mean correct hits in Go/No-Go trials was 55%. Academic achievement and IQ correlated with measures of cognitive processing including problem solving (WCST), task switching, interference, and response inhibition (see Table 5).
Mental Health Results
Means for the three subscales from the BDI were less than 1, which represents between no problem and minor problems on the 0 to 3 Likert-type scale. Mean scores on the YSR subscales ranged from .43 to .74 on a 0 to 2 Likert-type scale. The majority of participants scored in the normative range on the YSR on all eight subscales. Clinical levels of T-scores on internalizing subscales of the YSR ranged from 9.6% to 16.3% of the population, and on externalizing problems subscales ranged from 16.3% to 27.9%. Almost half of the sample (47.3%) reported clinically significant scores on more than one measure across the WCST, BRIEF, or the YSR. Mental health measures were highly intercorrelated and also correlated with low self-regulation (see Table 5).
Results of Hypothesis Testing
To test Hypothesis 1, that incarcerated adolescents will show a relation between intrafamilial violence and level of mental health function, correlations were conducted. Intrafamilial violence was examined based on both the level of intrafamilial violence (psychological, mild, severe, and total) and the type of intrafamilial violence (sibling, parent, and interpersonal violence). Intercorrelations between the intrafamilial violence measures were high as were intercorrelations among the mental health variables.
Total mean violence was related to the YSR withdrawn subscale. Psychological violence was associated with BDI Somatic Complaints. Mild violence was associated with BDI General Depression, YSR Withdrawn, Social Problems, and Thought Problems. Severe violence was not significantly correlated with any mental health variable. Sibling psychological violence was significantly associated with all three BDI subscales and the Withdrawn scale from the YSR. Sibling mild violence was related to YSR Social Problems. All three types of sibling violence correlated with YSR attention. Parental psychological violence correlated with Somatic Complaints from the BDI and the YSR Withdrawn scale. Parent mild violence was related to three factors of the YSR Internalizing scale; Withdrawn, Anxious/depressed, and Social Problems. Mild IPV was associated with BDI General Depression.
Model Testing
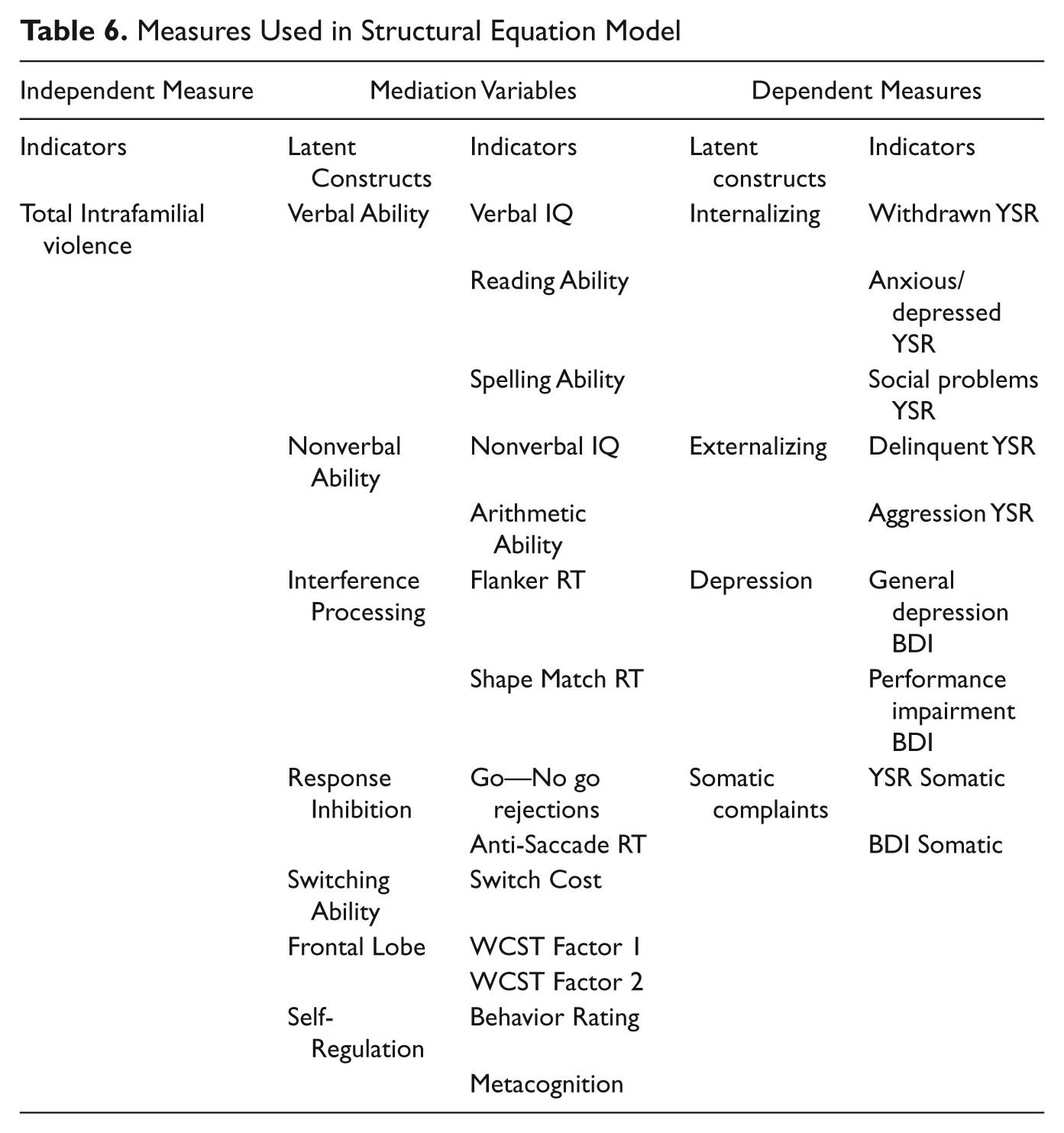
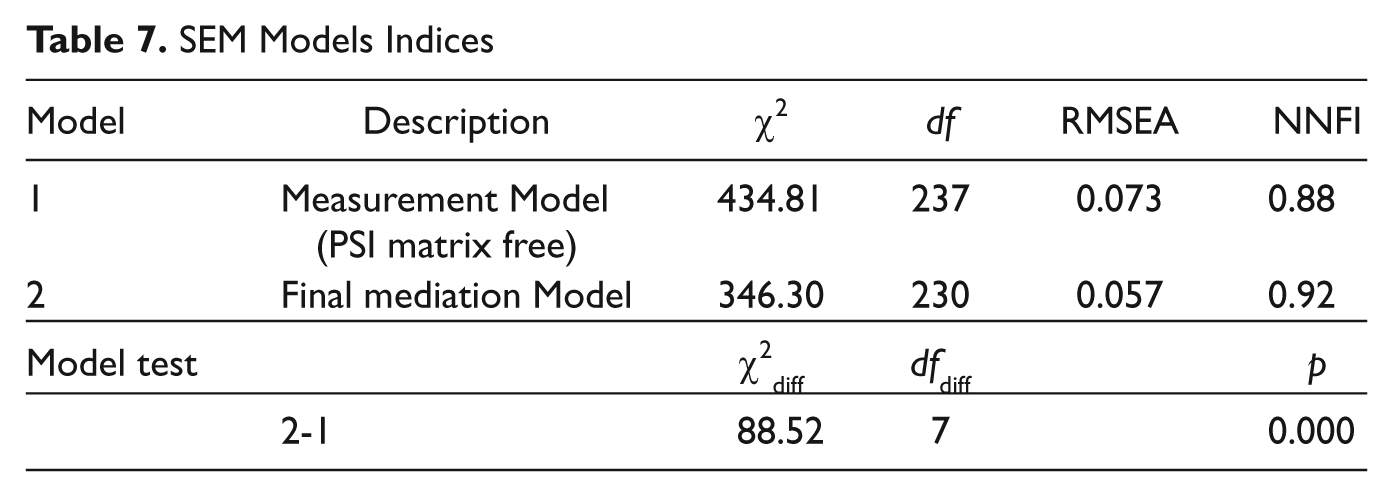
Hypothesis 2, that the above relation will be partially mediated by cognitive processing, learning, or executive functioning problems, was tested using SEM with LISREL 8.52. The model (Table 6) had one latent independent variable (IV), seven mediating variables (MV), and four dependent variables (DV). In the measurement model, all 24 indicators were indicators for exactly one construct; within each construct indicator residuals were allowed to correlate when significant (see Tables 5 and 6). Although the χ2difference test was significant (Kline, 2005; see Table 7), the RMSEA and NNFI suggest a reasonably good fit of the model. NNFI suggests a good fit when the index is close to 1. A more liberal cutoff for a small sample is .80. An RMR of close to 0 suggests a good fit of the model. The RMR of this model was adequate. We therefore adopt the mediation model as the more parsimonious model with reasonable fit.
Measures Used in Structural Equation Model
SEM Models Indices
In the final model (Figure 1 1 ), intrafamilial violence was negatively associated with nonverbal (performance) ability and self-regulation. Nonverbal ability was positively associated with response inhibition but did not have any relation with mental health adjustment. Self-regulation was associated with mental health function, including Internalizing, Externalizing, Depression, and Somatic Complaints such that higher self-regulation predicted better mental health adjustment. Mediation was shown where self-regulation mediated the relation between intrafamilial violence and mental health adjustment. The SEM analysis used pairwise deletion to remove missing variables from the covariance matrix for those participants with too much missing data to be imputed.
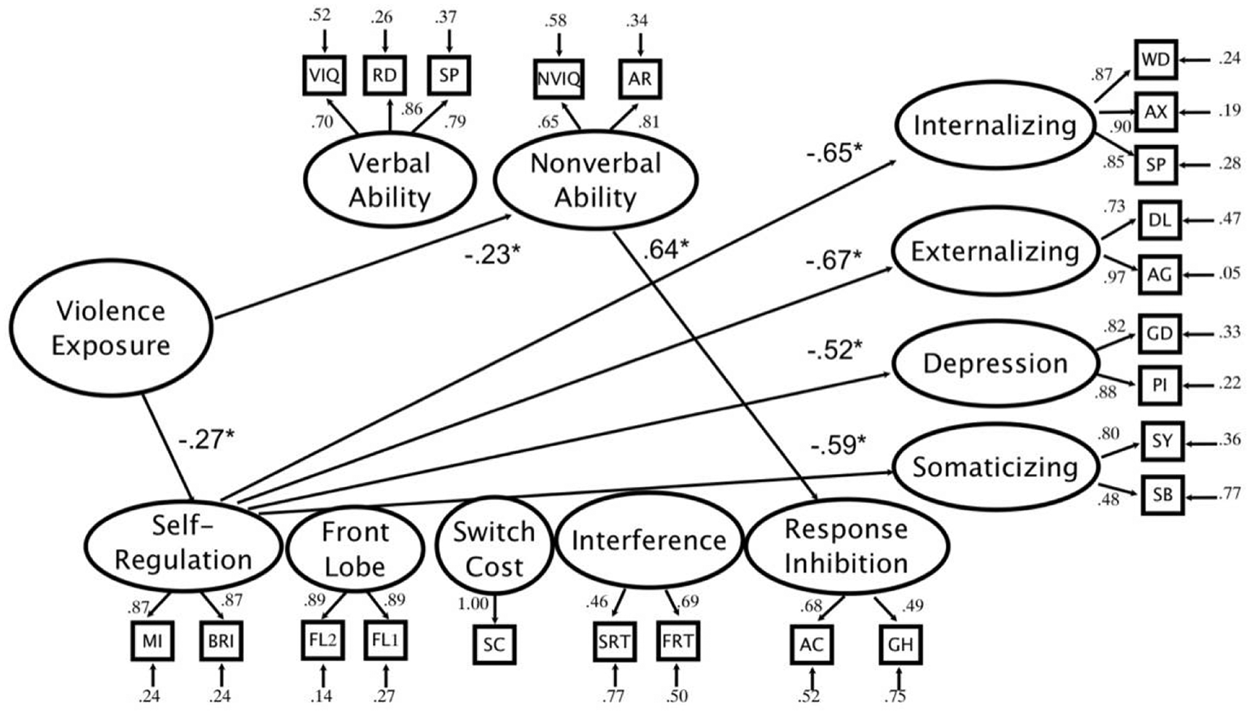
Full mediation model—Current self-regulation mediates relation between past violence exposure and current mental health functioning.
Discussion
This study represents a significant contribution to the understanding of the role of intrafamilial violence in the development of mental health problems in incarcerated youth. There are very few studies that have attempted to study youth during incarceration and have overcome the significant barriers to receiving permission from research institutional review boards, states, corrective institutions, youth, and parents to conduct research (Mulcahy, Krezmien, Leone, Houchins, & Baltodano, 2008). In addition, the present study incorporates measurement of past violence history, mental health, and cognitive processing including direct measurement of academic functioning and intelligence, self-regulatory capacity, response inhibition, and interference from distracters. This combined approach of psychological experimental research, records review, and survey research allows for a comprehensive examination of the complexities of mental health functioning in incarcerated youth.
Mediation of Cognitive Processing
Childhood intrafamilial violence is a major public health problem that has devastating effects. An often-overlooked outcome of exposure to violence is in the realm of cognitive and academic competence, where intrafamilial violence during development can lead to debilitating problems (Jonson-Reid et al., 2004). The hypothesis that cognitive processing and related self-regulatory skills partially mediate the relation between intrafamilial violence and mental health function is partially supported in this population of incarcerated adolescent boys. Self-regulation measured at the time of incarceration, mediates the relation between past history of exposure to violence and present mental health functioning but other cognitive processing measures do not mediate this relation. The current study supports the findings of other researchers that intrafamilial violence has a negative influence on the development of self-regulation (Merwe & Dawes, 2000).
Our results suggest that self-regulatory capacity may be integral to explaining high rates of metal health problems in incarcerated populations. Dodge and Crick (1990) have suggested that the mechanism for this negative relation is through the oversalience of threat in the environment. Our finding that self-regulation capacity is a mediator suggests a failure to process social cues appropriately in children exposed to violence. Other research suggests that this may be due to a neuroanatomical failure of top-down control over emotionally salient stimuli, interpreted as threat. This provides a mechanism by which history of exposure to violence causes self-regulatory deficits, necessary for school competence and achievement (Eccles & Wigfield, 2002). We fail to find mediation of other cognitive processing measures, which suggests that self-regulation may separately mediate the relation between intrafamilial violence and cognitive processing or mental health.
This study does find evidence that intrafamilial violence is related to cognitive processing through nonverbal skills. Deficits in nonverbal skills are in turn related to a decreased ability to inhibit a prepotent response. This supports the more general idea that intrafamilial violence has detrimental effects on cognitive and academic skills. A relation between cognitive processing, academic skills, and mental health function was found. As Nigg (2000) has suggested, executive function may be central to this relation and has a particularly strong negative association in the present study as has been seen in previous studies of at-risk populations (Campbell, Sameroff, Lewis, & Miller, 2000). Finally, there is high correlation between the different types of family violence, which suggests that violence in the home is interrelated, a finding that is supported by past research (Straus & Gelles, 1990).
Disability
We exhibit further evidence that learning disabilities and behavioral problems are very common in incarcerated populations. Estimated national rates of mental health disorders in children using the Achenbach System of Empirically Based Assessment are between 3% and 11% (Achenbach, Dumenci, & Rescorla, 2003). For individual mental health we find clinical rates from between 11% and 28%, well above national norms but below those found in other studies of incarcerated youth (Colins, Vermeiren, Shuyten, & Broekaert, 2009; Quinn et al., 2005). This difference may be due to underreporting when using self-report measures.
Rates of cognitive processing problems and learning disabilities are similarly high. Seventy percent of the sample has current IEPs. This is at the higher end of prevalence rates reported in youth incarceration nationally (Krezmien et al., 2008; Quinn et al., 2005) and may reflect differences in state special education classification systems or differences in rates of youth incarceration versus service in residential placement. Mean IQ and achievement scores are 10 points below national norms at about 90, in line with the findings of other studies of incarcerated youth (Krezmien et al., 2008).
Comorbidity is also common. More than 70% of participants have at least one measure of mental health or cognitive function on which they perform above the clinical cutoff. Of youth who meet the study criteria for clinical level mental health or academic problems, two thirds of the sample present with more than one clinical level of academic and mental health functioning. Other studies have failed to adequately quantify comorbidity in the diagnosis of cognitive and learning disabilities and mental health problems in incarcerated populations. A more nuanced understanding of the subpopulations within incarcerated groups is necessary to further treatment and prevention programs (Perkins, Smith-Darden, & Graham-Bermann, 2011). Mental health and academic problems tend to co-occur and the compound effect is often more devastating. Approximately one third of the sample has reached the age of maturity (18) suggesting that adults with IEPs are being treated in juvenile facilities rather than in adult facilities. High rates of cognitive and learning disabilities in prison populations argue for increased attention to the special needs of incarcerated youth (Mulcahy et al., 2008).
Limitations
The study has several limitations that include generalizability, diagnosis of cognitive and learning disabilities, missing data, and data collection. The sample represents a particular population that is more constricted in certain ways that might have influenced the findings. Close to 40% of the population had some experience with prior foster home placement, which suggests that many of the youth come from homes with a complex set of problems in the family of origin and our measures are limited in disentangling all of those complexities. This may also suggest that we have underestimated the rates of violence exposure. We asked about how conflicts were handled in the families. We intentionally left that open-ended because we were aware that many of the youth might have had multiple home placements. Several boys specifically asked if they grew up with a relative or in a foster home how they should answer. We asked them to answer for the time period independent of the type of family but this may have led to an underestimation.
The population has particularly high levels of mental health problems and low incidence behaviors (such as crime and delinquency). This might have created a ceiling effect on some measures. Every attempt was made to use measures that had strong reliability and validity but none of the norming samples included incarcerated adolescents. It is difficult for a large-scale study to accurately capture the complexity of diagnosis of disabilities. The inherent difficulties of collecting data in locked facilities made it extremely difficult to collect complete records on all participants. Participants were often released without notice, which meant that many participants had incomplete data files. A total of 38 participants were released with partial data collected. Missing data were replaced using an iterative process that maximized each participant’s empirical data. The conditions for collecting both survey and computerized data were not an ideal, for example, group of adolescents were given the survey at the same time. The conditions may have compromised the integrity of the data that were collected, particularly in regard to reaction times on cognitive tasks.
Implications
There are approximately 100,000 juveniles in residential placement nationwide. In this study 70% of the sample had current IEPs. Juvenile detention facilities clearly service large populations of children with disabilities and academic challenges. The model tested emphasizes the development of cognitive and learning skills as central to the known relation between intrafamilial violence and mental health function. Targeted interventions directed at cognitive processing and remediation of academic problems would seem to be essential in children with significant exposure to violence regardless of whether or not their functioning on any of those dimensions rises to the level of a diagnosable disability.
The finding that intrafamilial violence and self-regulation are significantly related to mental health functioning in general suggests the need to assess self-regulatory skills, anxiety, depression and withdrawal and their relation to learning disability in this population. Prevention and intervention programs often focus on externalizing behavior problems of aggression and delinquency. This is likely due to the societal cost of these behaviors but the current study finds clinical levels of anxiety, depression, or withdrawn behavior in our population. This suggests that underlying or preceding these behaviors may be deficits in self-regulatory behavior and that mental health must be approached holistically for at-risk youth.
Social control theory would benefit from incorporating our findings on the mediation of self-regulation in the prediction of criminal behavior. Currently, researchers in this vein have seen self-control as fixed at the age of 10 (Winfree et al., 2006). Recently researchers have attempted to incorporate the development of cognitive processing into social control theory (Beaver, Wright, & Delisi, 2007). Further expansion of social control theory to incorporate self-regulation as a developmental construct, would add a mechanism by which violence may be connected to later criminal behavior.
One future direction for research might focus on evaluating the efficacy of intervention and rehabilitation programs that can target self-regulation skills and cognitive deficits. It may be that struggling with language and information processing contributes to youth who have difficulty with maintaining behavior that conforms to societal norms. Dodge and others described deficits in social information processing as central to misinterpreting social cues as threatening or aggressive. It may also be that cognitive processing deficits, which are often seen as separate from behavior, contributes to youth misunderstanding of interpersonal interactions. Thus, the ability to self-regulate appears to be central in understanding how family violence effects youth behavior and should be a target of both future research study and intervention.
Footnotes
Acknowledgements
The authors would like to thank David Burton, Priti Shah, Addison Stone, and Michael Woolley for advice during the development of this proposal. Dr. Shah’s lab provided the computerized cognitive measures and was extremely helpful in providing guidance in the administration and scoring of the tasks. They are grateful to the University of Michigan Institutional Review board for advice in obtaining permission for the study. They received guidance and permission from the State of Michigan Department of Human Services, in particular, Diane Owens. They could not have completed the study without the dedicate support of their undergraduate research assistants; Rebecca Ametrano, Ashley Asbury, Daniel Davidson, Erica Friedman, Ho Lam, Katie Maki, and Linda Skaliski. They also could not have completed this study without the support and assistance from the staff and boys at the facility. They are indebted to them for their participation.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded in part from grant from Rackham Graduate School, the University of Michigan Department of Psychology, the University of Michigan Spencer grant program, and the NIH Interdisciplinary Training on Violence and Mental Health (Award No.: 5 T32 MH020041).