
Abstract
Research has reported that not only characteristics of the perpetrator but also characteristics of the victim influence risk for intimate partner violence (IPV). This would suggest that prevention of repeat abuse could benefit from a focus on both perpetrator and victim characteristics. Knowledge on factors that are within victims’ sphere of influence is important because a focus on victim characteristics can help victims to take control of their situations and can thereby empower them. Dynamic victim-related factors are most relevant here as these are factors that can be changed or improved, in contrast to unchangeable static factors. Surprisingly, however, little is known about how victim-related factors affect risk for revictimization of IPV. The current study was conducted among a Dutch sample of 156 female, help-seeking IPV victims. The aim was to examine to what extent prior IPV and, in particular, dynamic victim-related factors influence risk for future IPV. In accordance with the models articulated by Foa, Cascardi, Zoellner and Feeny, we studied how the three key factors from their models—partner violence, victims’ psychological difficulties, and victims’ resilience—related to risk for IPV revictimization. Results provide support for several key factors (partner violence and victims’ psychological difficulties) and, moreover, show which victim-related factors contribute to revictimization risk above and beyond the influence of prior violence committed by a partner against the victim (i.e., victims’ prior IPV victimizations). Findings are discussed in terms of recommendations for practice and future research.
Keywords
Introduction
In the last decades, researchers, policy makers and practitioners have shown increased attention for the prevention of intimate partner violence (IPV), which is considered a persistent social problem worldwide. Incidents of partner violence are seldom isolated events; they often occur repeatedly, as part of a cycle of relationship violence. Therefore, identification of risk factors for repeat partner violence is an important step in solving the problem. Until now, most research and prevention strategies have focused on a variety of perpetrator characteristics that influence the risk for (repeat) partner violence, such as men’s extensive criminal histories, substance abuse, psychological problems, and unemployment (see, for example, Dutton, 1995; Hilton et al., 2004; Kropp, Hart, & Belfrage, 2005). However, several studies have reported that characteristics of both members of a couple increase risk for IPV (e.g., Capaldi & Kim, 2007; Moffitt, Robins, & Caspi, 2001; Sonis & Langer, 2008). This would suggest that prevention of repeat partner abuse could benefit from a focus on both perpetrator and victim characteristics. Knowledge on victim-related factors is relevant for practice as it enables practitioners to provide appropriate and efficient services to victims of IPV and might serve as a basis for optimizing these services. Moreover, a focus on factors within victims’ influence might, when properly embedded, provide a means to victim control and empowerment (Goodman, Dutton, Vankos, & Weinfurt, 2005; Perez & Johnson, 2008). Dynamic victim-related factors are most relevant here as these are factors that can be changed or improved, in contrast to static factors (such as victim age), which cannot be changed by any action or intervention. Surprisingly, however, little is known about how victim-related factors affect risk for revictimization of IPV (Bennett Cattaneo & Goodman, 2005). One of the few conceptual models that integrate victim-related variables associated with the cessation or continuation of partner violence (i.e., repeat IPV) is that of Foa, Cascardi, Zoellner, and Feeny (2000). Actually, they formulated two models; one centering on psychological factors and the other on environmental factors related to repeat IPV. However in both models, they hypothesize the same mechanisms in which three key factors—partner violence; psychological difficulties; and resilience—work together in influencing victims’ ability to prevent future IPV. Partner violence and psychological difficulties are suggested to interact in a vicious cycle whereby victimization by partner violence causes psychological difficulties that, in turn, put women at greater risk for revictimization by hindering the victim’s ability to curtail future violence. Foa et al. further argue that victims’ intrapersonal resources—resilience—temper the negative psychological impact of partner violence and, thereby, serve to reduce the risk of revictimization.
The aim of the current study is to examine to what extent prior IPV and, in particular, dynamic victim-related factors influence the risk for future IPV. In accordance with the models articulated by Foa et al. (2000), we will study how the three key factors partner violence, victims’ psychological difficulties, and victims’ resilience relate to risk for IPV revictimization. Data for the current article come from a comprehensive prospective study aimed at identifying victims at (high) risk of revictimization of partner violence. Therefore, the operationalization of key factors is at some points slightly different from the definitions provided by Foa and colleagues.
The first key factor partner violence is defined by Foa et al. (2000) to comprise the severity of prior violence committed by a partner against the victim. It is hypothesized to increase the risk for future IPV because it is supposed to be related to victims’ psychological difficulties. However, the perpetration of violent acts by their male (ex-)partner is not within victims’ direct control. Because we are specifically interested in factors within victims’ own sphere of influence here, we decided to focus not only on violence committed by a partner (in accordance with Foa et al.’s definition) but also on IPV committed by the victim herself. Victim-perpetrated partner violence has been reported to be related to (re)victimization of IPV; however, these relations were mainly found cross-sectionally (Anderson, 2002; Fergusson, Horwood, & Ridder, 2005; Stith, Smith, Penn, Ward, & Tritt, 2004). For the current study, we hypothesize that prior IPV committed by a partner (i.e., victims’ prior IPV victimizations) as well as prior IPV committed by the victim herself prospectively relate to future IPV revictimization. Foa et al.’s second key factor involves victims’ psychological difficulties. In our comprehensive prospective study we included measures of victims’ borderline traits, feelings of anger, anxiety, and posttraumatic stress disorder (PTSD) symptoms. The first three constructs were all trait measures; these measures assessed the general presence of borderline traits, feelings of anger, and anxiety in victims. PTSD was operationalized as a state measure; items of the PTSD measure specifically asked for current PTSD symptoms related to prior partner violence. In line with Foa et al., we expect victims’ psychological difficulties to be risk factors for IPV revictimization. The third key factor resilience can be defined as victims’ level of intrapersonal resources. According to Foa et al., it tempers the negative psychological impact of partner violence and, thereby, serves to reduce the risk of revictimization. The only resilience-related construct that we measured in our comprehensive prospective study was quality of life. As described in the measures section of this article, our quality of life measure involves several internal (such as physical and psychological health) and external personal resources (such as social relationships) available to the victim. Therefore, we consider quality of life as an aspect of resilience in the current study. We hypothesize victims’ resilience to be a protective factor against IPV revictimization.
In short, we will analyze how (prior) partner violence and the above victim characteristics and behaviors relate to both the occurrence of any future IPV revictimization as well as the severity of future IPV revictimization. Moreover, we are interested in the relative strength of the risk factors to identify those factors on which practitioners could intervene to decrease risk for future IPV most. However, in prior studies some difficulties related to the analysis of victim-related variables are described. As Bennett Cattaneo and Goodman (2005) formulated, “researchers may worry that identifying victim behaviors that are associated with being revictimized places the responsibility for stopping the violence too much at the victim’s door” (p. 168). This concern of “victim blaming” might explain the lack of (prospective) studies into victim-related risk factors for IPV. With the current study we do not want to suggest that we blame victims for what happened to them. We do, however, believe that research on victim-related risk factors for IPV revictimization is necessary to stimulate victim empowerment. Although we are particularly focused on victim-related risk factors in the current study, we will also examine how prior violence committed by a partner against the victim (i.e., victims’ prior IPV victimizations) relates to risk for IPV revictimization. Not only, has this variable been established as an important predictor by numerous studies (e.g., Bennett Cattaneo & Goodman, 2003; Bybee & Sullivan, 2005; Hirschel & Hutchison, 2003; Krause, Kaltman, Goodman, & Dutton, 2006; Perez & Johnson, 2008). Moreover, knowledge about victim-related factors that contribute to risk for IPV revictimization above and beyond prior violence committed by a partner offers suggestions for practice with regard to developing and optimizing victim services. This is important because interventions for male batterers have shown mixed results with regard to their efficacy until now (e.g., Babcock, Green, & Robie, 2004; Feder & Wilson, 2005). In that way, the type of research described in the current article may assist victims in stopping the violence they experience at the hands of their partners.
Method
Procedure and Participants
Participants were recruited from various victim support services in the Netherlands in four large and four medium-sized cities. The services included a victim support office, a mental health organization, a number of social work organizations, a shelter, victim service points of the Public Prosecution service, and various local domestic violence teams of a health authority. Participants were approached and included in our study if (a) they had been a victim of physical, sexual, or psychological violence by their current or ex-partner at least once in the past 2 years, and (b) if they sufficiently mastered the Dutch language to understand the Dutch questionnaires we used. Participants were recruited through the collaborating victim support organizations by having staff inform eligible clients about this study. Most victims were directly contacted by staff members; others were informed about the study through a letter. Staff of collaborating victim organizations were instructed to report the total number of victims they invited to participate, including those victims who declined. However, the number that was invited but declined was not reported systematically and hence, we do not know the exact number of victims invited for the study. We only know that eventually 134 victims registered for participation after they were contacted personally about the study by staff members. However, for the group of victims that was informed about the study through a letter, we do have exact information. In total, 175 victims received a letter about the study, which offered them the choice to participate. As 47 of them registered for participation, the response rate was 26.8%. Clients who indicated interest in participating received a registration form asking them to provide their contact details and to return it to the researchers. A researcher then telephoned registered participants to discuss any questions about the study they might have. For any questions during completion of the questionnaire, participants could phone or e-mail the researchers. Participants were asked to take part in the study at three different moments in time: after the initial assessment at baseline, assessments were repeated 2 and 6 months later. They were paid a 100 euro compensation for their time after completing the questionnaire at all three waves of data collection. In this article, we present data from all waves of data collection (data were collected between August 2008 and August 2010).
Measures
Predictors
Partner Violence
Victims’ recent IPV victimization and perpetration (at 2 months)
The occurrence of any recent IPV victimization and any recent IPV perpetration by the victim herself was assessed at first follow-up with the revised version of the Conflict Tactics Scale (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). Specifically, we were interested in four predictors: (a) any recent physical IPV victimization, (b) any recent psychological IPV victimization, (c) any recent physical IPV perpetrated by the victim herself, and (d) any recent psychological IPV perpetrated by the victim herself. We measure both physical as well as psychological partner violence because Foa et al. (2000) operationalize partner violence as including physical and emotional abuse. The CTS2 consists of 78 items listing violent behaviors for which respondents report the frequency of occurrence by either spouse. Thus it measures both violent behaviors that have been committed by a partner or ex-partner against the respondent (victimization measure) as well as the violent behaviors that have been perpetrated by the respondent itself (perpetration measure). For the current study we used both the victimization as well as the perpetration measure of the CTS2, as we were interested in victims’ recent IPV victimization and perpetration.
Items of the CTS2 are divided into five subscales: physical assault, psychological aggression, negotiation, injury, and sexual coercion. We assessed victims’ victimization by violence committed by their current or ex-partner and victims’ own perpetration of violence against their current or ex-partner during the previous 2 months (i.e., the period between baseline and first follow-up). To assess the occurrence of victims’ recent physical IPV victimization and perpetration, we used the 12-item CTS2 subscale physical assault; for victims’ recent psychological IPV victimization and perpetration, we used the 8-item CTS2 subscale psychological aggression. Sample items of the CTS2 physical assault subscale include “My (ex-)partner beat me up” and “My (ex-)partner kicked me” for the victimization measure, and “I beat up my (ex-)partner” and “I kicked my (ex-)partner” for the perpetration measure. Sample items of the CTS2 psychological aggression subscale include “My (ex-)partner insulted or swore at me” and “My (ex-)partner called me fat or ugly” for the victimization measure and “I insulted or swore at my (ex-)partner” and “I called my (ex-)partner fat or ugly” for the perpetration measure.
The CTS2 is usually scored using an 8-point ordinal scale indicating the frequency of occurrence of conflict tactics ranging from 1 (once in the past year) to 6 (more than 20 times in the past year), with 7 and 8 indicating not in the past year, but it happened before and this has never happened, respectively (Straus et al., 1996). According to Straus (2006), the CTS2 can be used not only as a frequency measure of conflict tactics but also as a prevalence measure of violent behaviors, by instructing respondents to indicate if the behaviors had occurred or not, instead of how frequent. Accordingly, participants in the current study were asked to indicate their victimization by and perpetration of each of the violent behaviors in the previous 2 months by giving a “yes” or “no” answer, thus using the CTS2 as a prevalence measure. If a victim gave one or more affirmative responses to any of the physical assault items on the CTS2 victimization measure, we considered it as any recent physical IPV victimization being present. Similarly, if a victim gave one or more affirmative responses to any of the psychological aggression items on the CTS2 victimization measure, we considered it as any recent psychological IPV victimization being present. The same goes for the CTS2 perpetration measure.
Good internal consistency has been demonstrated for all subscales of the CTS2 as well as adequate construct and discriminant validity (Straus et al., 1996). Reliabilities of the underlying variables of our physical IPV scales were good as Cronbach’s alpha was .95 for the victimization measure and .85 for the perpetration measure. To obtain a satisfying reliability for our psychological IPV measures, we had to delete one item on both scales (“My (ex-)partner threatened to hit or throw something at me” and “I threatened to hit or throw something at my (ex-)partner”) due to a high number of missing values on those items. Therefore, our final scales of psychological IPV each consisted of seven items (before dichotomization), for which a good reliability can be reported as well. Cronbach’s alpha was .84 for the victimization measure and .78 for the perpetration measure of psychological IPV.
Psychological Difficulties
Borderline traits (baseline)
The borderline subscale of the Personality Diagnostic Questionnaire–4+ (PDQ-4+; Akkerhuis, Kupka, Van Groenestijn, & Nolen, 1996; Hyler, 1994) was used to assess borderline traits in our victim sample at baseline. The full PDQ-4+ is a self-report questionnaire and it assesses the 10 DSM-IV personality disorders, and additional diagnoses of the passive-aggressive and depressive personality disorder included in an appendix of the DSM-IV (American Psychiatric Association, 1994). The borderline subscale that was used in this study consists of nine items that correspond with the nine criteria for a borderline personality disorder as described in the DSM-IV. Sample items include “I’ll go to extremes to prevent those who I love from ever leaving me” and “I have done things on impulse that can get me into trouble [such as] spending more money than I have or having sex with people I hardly know.” For each statement, participants were asked to indicate whether it applied to them by giving a “true” or “false” response. We computed a sum score by adding up the answers (true = 1, false = 0), thereby treating borderline traits as a continuous variable. Evidence for the validity and reliability of the PDQ-4+ can be derived from research on an earlier version of this instrument, the PDQ-R (Hyler & Rieder, 1987). The PDQ-R shows adequate criterion validity for most axis II disorders, including borderline personality disorder (Hyler, Skodol, Oldham, Kellman, & Doidge, 1992). Although instruments such as the PDQ-R are not substitutes for a structured diagnostic interview, it appears to be an efficient screening instrument in clinical (Hyler, Skodol, Kellman, Oldham, & Rosnick, 1990; Hyler et al., 1992) and nonclinical populations (Johnson & Bornstein, 1992). For reliability analysis of the borderline subscale of the PDQ-4+ used in the current study, an acceptable Cronbach’s alpha of .74 can be reported.
Anger (baseline)
Anger in the victim was assessed at baseline with the Dimensions of Anger Reactions scale (DAR; Forbes et al., 2004; Novaco, 1975). Besides being a measure of trait anger, the DAR reflects STAXI constructs (State Trait Anger Expression Inventory; Spielberger, 1988) of anger out, state anger, and anger control as well. Therefore, the DAR is best described as a measure of anger disposition directed toward others (Forbes et al., 2004). It consists of seven items that can be rated on a 5-point Likert-type scale ranging from 1 (not at all) to 5 (exactly so). The five response categories were adapted from the DAR5 (Hawthorne, Mouthaan, Forbes, & Novaco, 2006), as Hawthorne and colleagues (2006) report that “the [original] nine response categories of the DAR were problematically labeled, [. . .] and prevented equivalent measurement when translated” (p. 166). A sum score was computed by adding up the responses on the seven items, thereby treating anger in the victim as a continuous variable. Sample items of the DAR are “I often find myself getting angry at people or situations” and “When I get angry I stay angry.” The DAR has been reported to be a reliable and psychometrically strong measure (Forbes et al., 2004). Scale reliability for the current study was good as well, as Cronbach’s alpha was .82.
Anxiety (baseline)
The trait subscale of the Dutch version of the State-Trait Anxiety Inventory (STAI; Van der Ploeg, Defares, & Spielberger, 1980) was used to assess trait anxiety in our victim sample. This self-report scale measures to what extent respondents experience symptoms of anxiety in general. The scale consists of 20 statements that ask people to describe how they generally feel (e.g., “I feel nervous and restless,” and “I feel secure”), which can be rated on a 4-point Likert-type scale ranging from 1 (almost never) to 4 (almost always). We created a sum score by adding up the scores, which could range from 20 (low level of trait anxiety) to 80 (high level of trait anxiety). A good reliability and validity for the Dutch version of the STAI have been reported (Van der Ploeg, 2000; Van der Ploeg et al., 1980). For the current study, Cronbach’s alpha of the trait subscale was found to be .93, indicating a high reliability.
PTSD symptoms (at 2 months)
PTSD symptom severity was assessed after 2 months with the PTSD Symptom Scale-Self Report (PSS-SR; Foa, Riggs, Dancu, & Rothbaum, 1993). As we were interested in PTSD symptoms related to recent partner violence, we decided to measure the presence of PTSD symptoms at first follow-up. The PSS-SR consists of 17 items that represent the criteria for a PTSD listed in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV; American Psychiatric Association, 1994). Current PTSD symptom severity was measured by asking respondents to indicate to what extent they experienced each of the symptoms during the previous week. Answers could be rated on a 4-point Likert-type scale, ranging from 0 (never) to 3 (five times or more). Items were clustered into five reexperiencing (e.g., intrusive thoughts about the violent incident(s)), seven avoidance (e.g., avoiding thoughts and feelings about the violent incident(s)), and five arousal (e.g., sleep disturbance) symptoms. For each of these symptom clusters, sum scores were computed. The PSS-SR has been reported to have good psychometric properties (Foa et al., 1993). Cronbach’s alpha in the current study was .88 for the reexperiencing cluster, .88 for avoidance, and .83 for the arousal cluster, indicating a high reliability.
Resilience
Quality of life (baseline)
Victims’ quality of life was assessed at baseline with the Dutch version of the WHOQOL-BREF (WHOQOL Group, 1998). The WHOQOL-BREF is an abbreviated version of WHOQOL-100 quality of life assessment (Dutch version: De Vries & Van Heck, 1995), and consists of 26 items. Two items measure overall quality of life and general health and the remaining items are categorized into four domains: physical health, psychological health, social relationships, and environment. Items of the WHOQOL-BREF refer to the extent to which they were experienced or the satisfaction with them during the past 2 weeks and can be rated on a 5-point Likert-type scale, ranging from 1 (not at all/very dissatisfied) to 5 (completely/very satisfied). Examples include “To what extent do you feel that pain prevents you from doing what you need to do?” for the physical health domain, “How much do you enjoy life?” for the psychological health domain, “How satisfied are you with your personal relationships?” for the social relationships domain, and “How safe do you feel in your daily life?” for the environmental domain. The WHOQOL-BREF has been reported to be “a sound, cross-culturally valid assessment of quality of life” (Skevington, Lotfy, & O’Connell, 2004, p. 299), showing good to excellent reliability and validity. In the current study, the WHOQOL-BREF showed a good reliability as well; Cronbach’s alpha was .92.
Outcome Measures
IPV revictimization (at 6 months)
The four outcome measures of our study—the occurrence of any physical and psychological IPV revictimization, and the severity of physical and psychological IPV revictimization—were assessed at second follow-up (6 months after baseline). All outcomes were measured with the revised version of the Conflict Tactics Scale (CTS2; Straus et al., 1996), which has been described above. To assess any and severity of physical IPV revictimization we used the 12-item CTS2 subscale physical assault; for any and severity of psychological IPV revictimization we used the 8-item CTS2 subscale psychological aggression. Participants in the current study were asked to indicate the occurrence of victimization by each of the violent behaviors in the previous 4 months (i.e., the period between first and second follow-up) by giving a “yes” or “no” answer. If there were one or more affirmative responses to any of the physical assault items, we considered it as any physical IPV revictimization being present. Similarly, if there were one or more affirmative responses to any of the psychological aggression items, we considered it as any psychological IPV revictimization being present. In addition, for the victims who reported being revictimized, sum scores were computed for severity of physical and psychological IPV revictimization by adding up the affirmative responses to the violent behaviors of the corresponding scales. By doing so, we created two scales (a) a scale for the variety of different physically assaultive behaviors and (b) a scale for the variety of different psychologically assaultive behaviors by which one had been revictimized. Participants with a higher sum score were revictimized by a greater variability of physically or psychologically violent behaviors than participants with a lower sum score. According to Moffitt et al. (1997), violence severity is often measured by frequency scores; however, variety scores have proved to be a good alternative. In this study, we therefore interpret our variety score of violent behaviors as a severity measure of IPV. 1 Cronbach’s alpha for the CTS2 revictimization measure of physical IPV in this study was .95, indicating a high reliability. To obtain a satisfying reliability for our measure of psychological IPV revictimization, we had to delete one item on the scale (“My (ex)-partner threatened to hit or throw something at me”) due to a high number of missing values on that item. Therefore, our final scale for psychological IPV revictimization consisted of seven items, for which a good reliability can be reported (Cronbach’s α = .86).
Statistical Analyses
For any IPV revictimization, bivariate associations with our study variables were examined by performing separate binary logistic regression analyses. All bivariate significant variables were subsequently entered as independent variables in a multivariate backward logistic regression analysis (method: likelihood ratio) to identify the best subset of predictors of any IPV revictimization. To see what study variables might predict the severity of IPV revictimization, we only considered those respondents who reported to be revictimized. Here, bivariate associations between all study variables and severity of IPV revictimization were examined by computing Pearson’s correlation coefficients. Again, all bivariate significant variables were entered as independent variables, this time in a multivariate backward linear regression analysis to identify the best subset of predictors. The alpha level was set at .05 in all statistical tests. All statistical analyses were performed using the software package SPSS 17.0 for Windows (SPSS, Inc., Chicago, IL, USA).
Results
Sample Characteristics
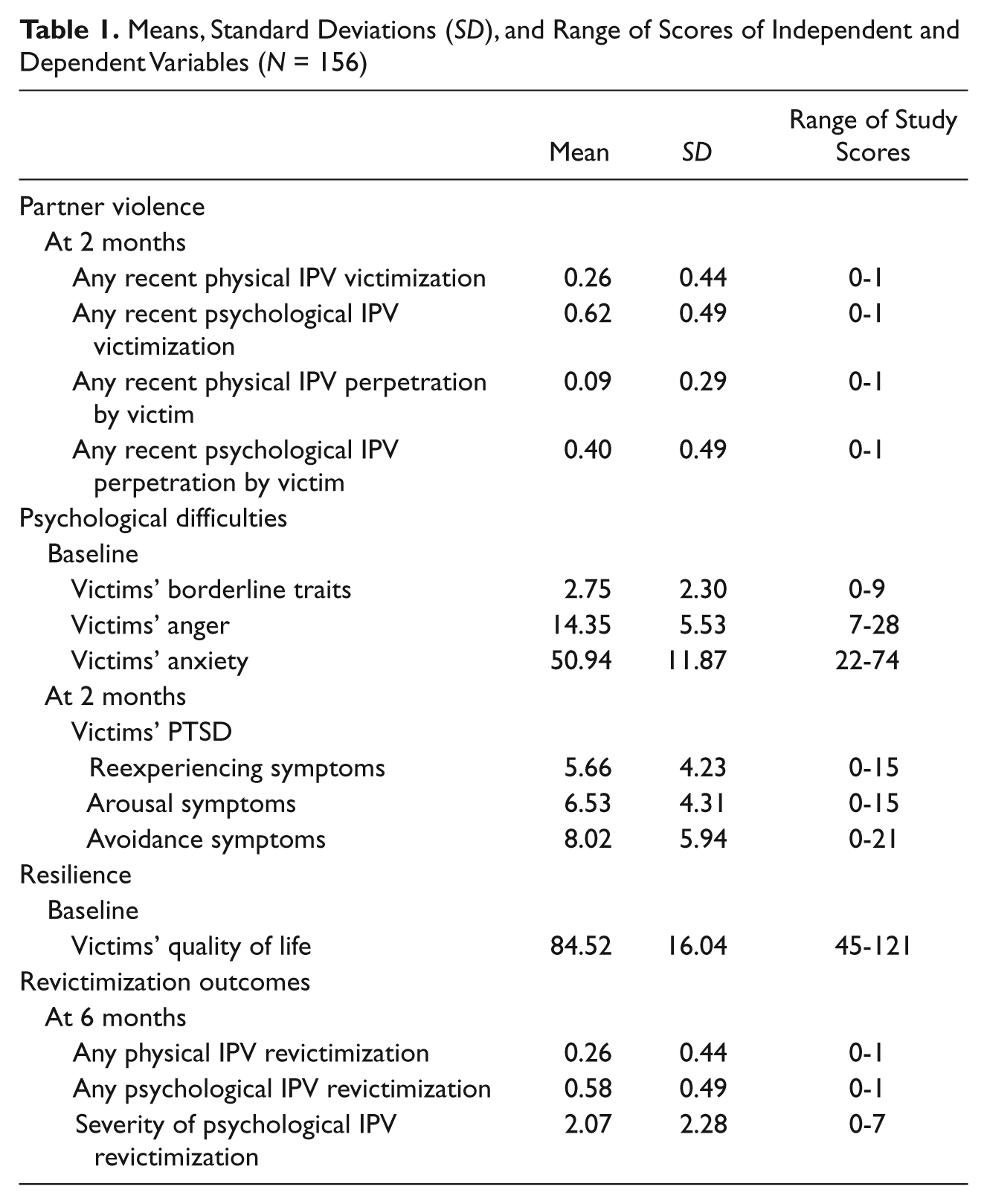
We were able to recruit 181 victims of partner violence, of whom 166 participated in the current study. 2 Of these 166 victims, 3 were excluded (2 because they were male and 1 because she was younger than 18 years), leaving 163 female help-seeking victims of IPV who were included at baseline. As 7 of them dropped out during the study, all subsequently reported analyses were conducted on the final sample of 156 victims. They ranged in age from 20 to 68, with a mean age of 37.74 years (SD = 10.42). The cultural background of participants was determined by their parents’ birthplace. Ninety-six participants (61.5%) had Dutch parents, 15 (9.6%) had a Western immigrant background, 43 (27.6%) had a non-Western background, and 2 (1.3%) participants’ background was unknown. Of all respondents, 75.6% were born in the Netherlands. A vast majority had one or more children (85.3%). Most participants completed intermediate vocational education (46.8%), a second group having completed lower vocational education (19.9%). Only 43.6% held a paid job, the other 56.4% did not. The annual income of participants was rather low. Of the respondents who answered this question (n = 142), 78.2% had an income of less than 20,000 euro. Thirty-six victims (23.1%) reported being in a romantic relationship with the perpetrator at baseline, 30 victims (19.2%) at 2 months, and 25 victims (16.0%) at 6 months. At baseline and at 2 months, 11.5% of victims reported living in a shelter, at 6 months this was even less; 7.1%. The mean number of days between baseline and second follow-up (at 6 months) was 186.93 (SD = 16.71, range 168-284). There was some variety in the number of days although only a few exceeded a period of 7 months; 92.9% filled out the follow-up questionnaire within 210 days. Of the 156 victims in our final sample, a quarter (25.6%) reported to be revictimized by any physical IPV and more than half (58.3%) by any psychological IPV at 6 months. Means, standard deviations, and range of scores of all our study variables are presented in Table 1.
Means, Standard Deviations (SD), and Range of Scores of Independent and Dependent Variables (N = 156)
Bivariate and Multivariate Predictors of Any IPV Revictimization
Table 2 shows the variables included in our study and their bivariate associations with revictimization of any physical and psychological IPV. For the key factor partner violence, results showed that both (any) recent physical IPV victimization as well as (any) recent psychological IPV victimization (at 2 months) were significantly and positively related to revictimization of any physical and psychological IPV at 6 months. Furthermore, we found that the variables any recent physical IPV perpetration and any recent psychological IPV perpetration by the victim herself were significantly and positively associated with any physical IPV revictimization. For our outcome revictimization of any psychological IPV, only the occurrence of any recent psychological IPV perpetrated by the victim reached significance. Examining a variety of psychological difficulties, PTSD reexperiencing symptoms measured at 2 months were found to hold a significant positive relation with any physical as well as any psychological partner violence revictimization reported at 6 months. For the resilience-related factor quality of life, no significant association with reoccurrence of any physical or psychological IPV was found. Table 2 shows odds ratios for each variable: it explains how much the odds of any IPV revictimization increase or decrease for a one-unit change in the predictor variable. For instance, the odds ratio for any recent psychological IPV perpetrated by the victim herself is 3.72 for any psychological IPV revictimization at 6 months. This means that if the variable increases from 0 (psychological IPV by victim absent) to 1 (psychological IPV by victim present), the risk for revictimization of any psychological IPV at 6 months is 3.72 times higher. In other words, if the victim perpetrates any psychological IPV herself, she is more than 3.5 times as likely to be revictimized by any psychological IPV.
Bivariate Associations With Revictimization of Any Physical and Psychological IPV at 6 Months (N = 156)
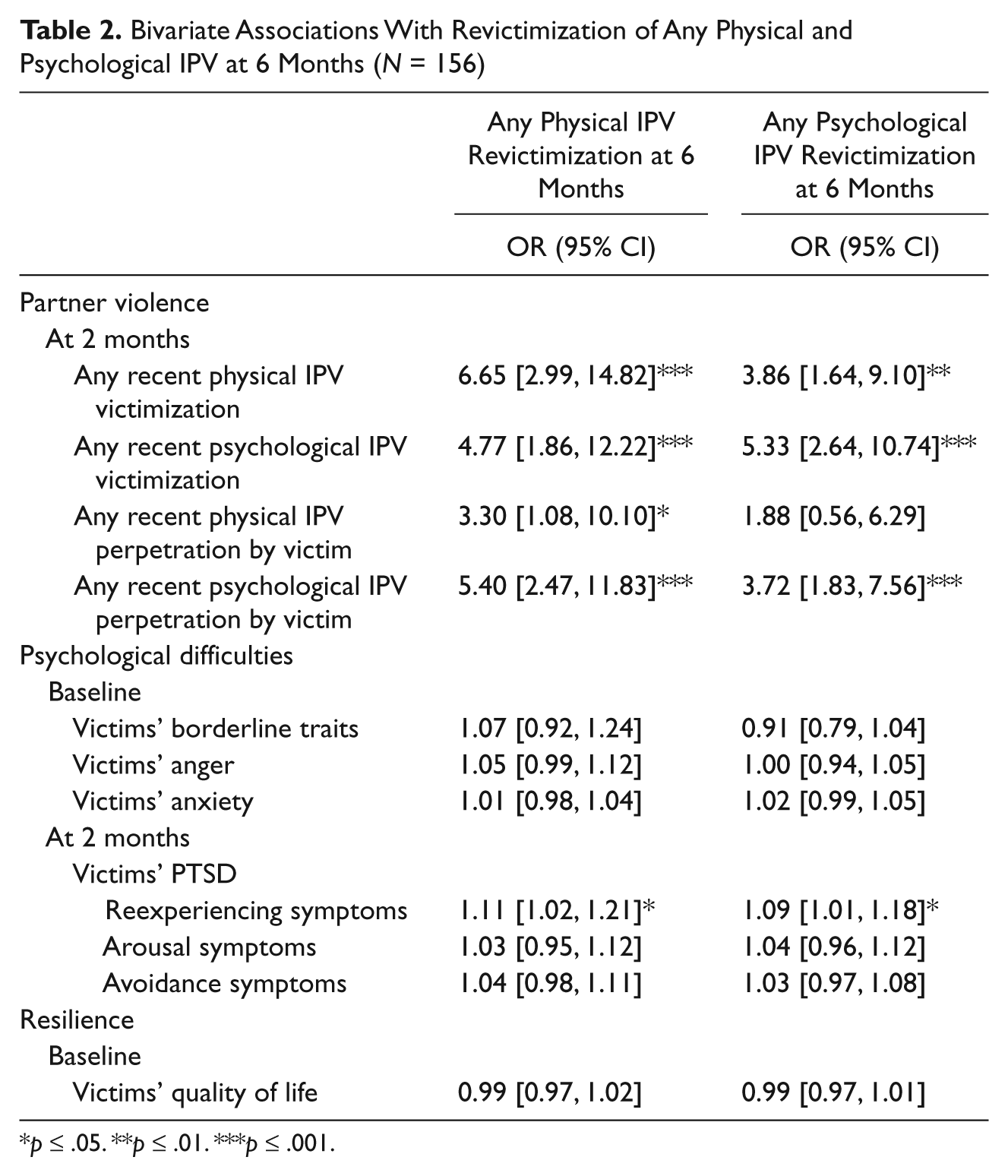
p ≤ .05. **p ≤ .01. ***p ≤ .001.
To identify the best subset of predictors of any IPV revictimization, two multivariate backward logistic regression analyses were conducted; one for our outcome any physical IPV revictimization and one for any psychological IPV revictimization. Only variables with bivariate significant associations were entered as predictors. Table 3 shows that for our outcome any physical IPV revictimization (at 6 months), two multivariate predictors can be identified: any recent physical IPV victimization and any recent psychological IPV perpetration by the victim herself (at 2 months). If the victim was recently victimized by any physical IPV, the risk that she would be victimized again by any physical IPV at 6 months is 3.63 times as high. Similarly, if the victim perpetrated any psychological IPV herself, her risk for revictimization of physical IPV is 2.73 times as high. These two predictors together explain between 16% (Cox & Snell) and 23% (Nagelkerke) of variance in scores on revictimization of any physical IPV. For any psychological IPV revictimization, one multivariate predictor emerged: any recent psychological IPV victimization. A victim who recently received psychological violence from her (ex-)partner is 5.33 times more likely to become revictimized by some form of psychological IPV than a victim who does not. This predictor explains between 14% (Cox & Snell) and 19% (Nagelkerke) of variance in scores on revictimization of any psychological IPV. In short, our results suggest that in a multivariate model, revictimization of any physical IPV is best predicted by the occurrence of any recent physical IPV victimization and by any recent psychological IPV perpetrated by the victim herself. Revictimization of any psychological IPV is best predicted by the occurrence of any recent psychological IPV victimization.
Multivariate Predictors of Revictimization of (1) Any Physical and (2) Any Psychological IPV at 6 Months (N = 156)
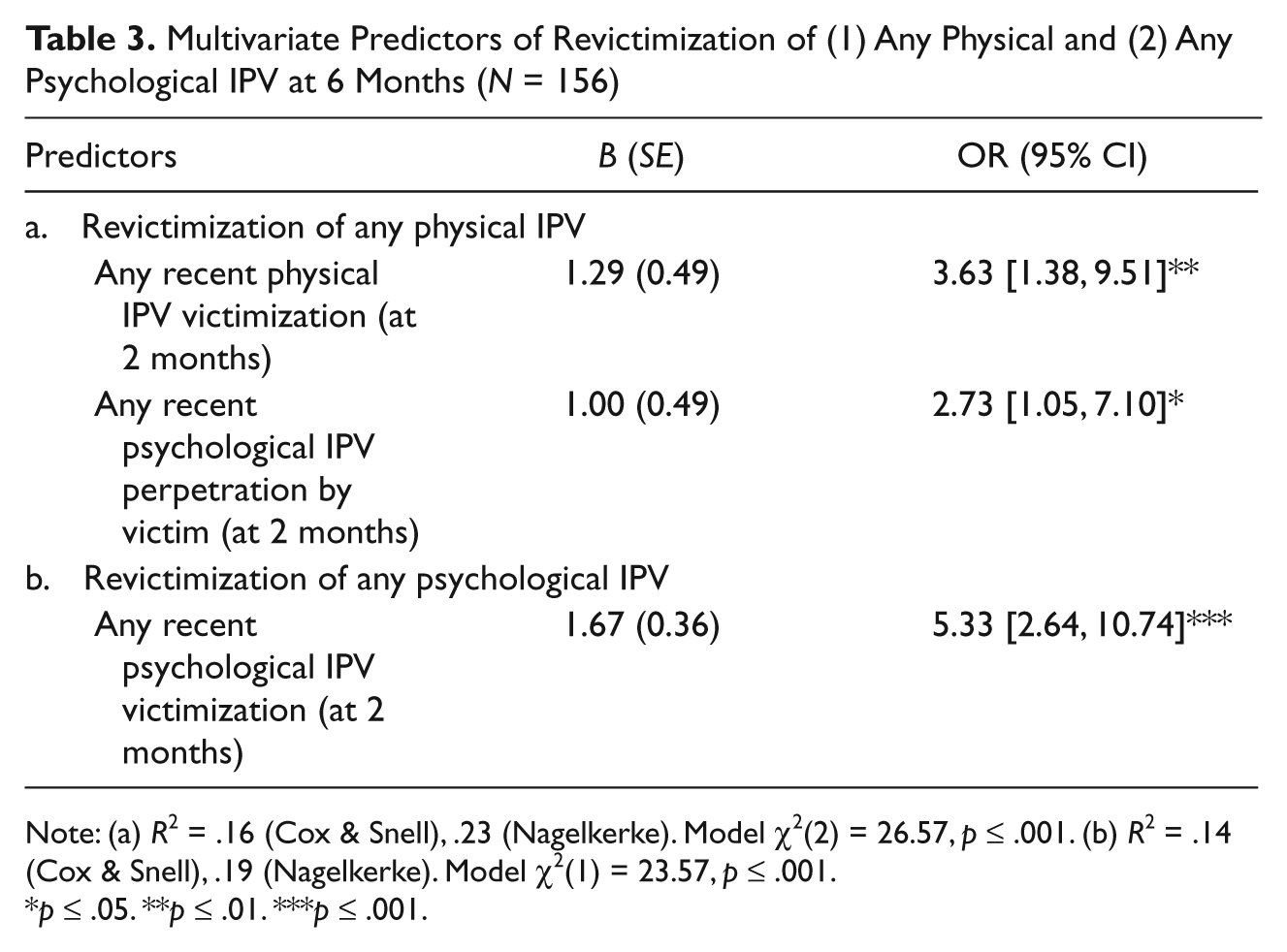
Note: (a) R2 = .16 (Cox & Snell), .23 (Nagelkerke). Model χ2(2) = 26.57, p ≤ .001. (b) R2 = .14 (Cox & Snell), .19 (Nagelkerke). Model χ2(1) = 23.57, p ≤ .001.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Bivariate and Multivariate Predictors of Severity of IPV Revictimization
As too few respondents reported physical revictimization (n = 40), no analyses were conducted to predict the severity of physical IPV revictimization at 6 months. However, we did conduct analyses on the 91 victims who reported to be revictimized by some form of psychological IPV at 6 months. Table 4 shows the variables included in our study and their bivariate associations with the severity of psychological IPV revictimization. For the key factor partner violence, results showed that the variable any recent physical IPV victimization was significantly and positively related to the severity of psychological IPV revictimization and in addition, any recent psychological IPV victimization showed a trend. Furthermore, we found perpetration of any recent psychological IPV by the victim herself to positively predict the severity of psychological abuse as well. In addition, the various psychological difficulties listed in Table 3 were all associated with the severity of repeat psychological violence. At baseline, victims’ borderline traits, feelings of anger, and anxiety were significantly related to severity of psychological IPV. Victims’ PTSD reexperiencing, arousal, and avoidance symptoms measured at 2 months also held a significant relation with psychological IPV severity. Quality of life, our only resilience-related factor, showed a negative trend; a good quality of life as experienced by the victim herself seems to serve as a protective factor against the severity of revictimization.
Bivariate Associations With Severity of Psychological IPV Revictimization at 6 Months (n = 91)

p ≤ .10. *p ≤ .05. **p ≤ .01. ***p ≤ .001.
Table 5 shows the results of a backward linear regression analysis with the bivariate significant and trend variables entered as predictors and severity of psychological IPV revictimization as dependent variable. Two multivariate predictors can be identified: any recent psychological IPV victimization and victims’ borderline traits. From the significance levels, we can conclude that borderline traits in the victim predict the severity of psychological IPV revictimization most strongly after controlling for all other variables in the model, followed by the presence of any recent psychological IPV victimization. The two predictors together explain 27% of variance in scores on severity of psychological IPV revictimization. In short, results show that in a multivariate model, the severity of revictimization by psychological IPV is best predicted by victims’ psychological difficulties, specifically borderline traits. Furthermore, the occurrence of any recent psychological IPV victimization predicts the severity of revictimization by psychological IPV as well, although to a lesser extent.
Multivariate Predictors of Severity of Psychological IPV Revictimization at 6 Months (n = 91)

Note: R2 = .27.
p ≤ .05. ***p ≤ .001.
Discussion
In the current study, bivariate and multivariate analyses were performed to examine how prior IPV and, in particular, dynamic victim-related variables relate to any IPV revictimization and severity of IPV revictimization. As proposed in Foa et al.’s (2000) models, we studied how the three key factors from these models —partner violence, victims’ psychological difficulties, and victims’ resilience—influenced the risk of revictimization. We found strong support for the effect of partner violence as aspects of this factor showed to predict each of our three revictimization outcomes: any physical IPV, any psychological IPV, and severity of psychological IPV. More specifically, physical partner violence that was recently committed against the victim was found to predict revictimization of physical IPV in a multivariate model. Similarly, psychological partner violence that was recently committed against the victim was found to predict the occurrence of revictimization of psychological IPV. In addition, recent psychological partner violence also predicted the severity of revictimization by psychological IPV. Moreover, our findings indicated that recent psychological IPV perpetrated by the victim significantly increased the risk for physical IPV revictimization, independently adding to the effect of prior physical violence by a partner. We furthermore found support for the relevance of victims’ psychological difficulties in predicting the risk of revictimization. Victims’ borderline traits showed to predict the severity of psychological IPV revictimization, independently adding to the effect of prior psychological violence by a partner. Contrary to our expectations, however, we did not find multivariate significant results supporting the hypothesized effect of victims’ resilience in predicting revictimization.
Findings of the current study show that victim-related variables significantly contributed to the prediction of any physical IPV revictimization and the severity of psychological IPV revictimization and, moreover, that they did so in addition to the influence of any prior violence committed by a partner against the victim (i.e., any prior IPV victimization). Yet victim-related variables did not significantly contribute to the prediction of any psychological IPV revictimization in a multivariate model. We would like to stress that we do not mean to imply that victims share any responsibility for the repeated victimization, but we do feel that the diverging results on our physical and psychological revictimization outcomes merit some further discussion. Unfortunately, we were unable to collect data among victims’ partners and as a consequence we cannot conclude anything about possible patterns of interaction between victims and their perpetrators, but we would like to discuss some very tentative explanations.
Both psychological violence by the victim and victims’ borderline personality traits, (which showed to contribute to the prediction of any physical IPV revictimization and severity of psychological IPV revictimization, respectively) can be regarded to reflect emotionally negative communication on the part of the victim. That victims’ use of psychological violence can be considered an aspect of an emotionally negative communication style seems rather clear. However, the way in which victims’ borderline traits may lead to such communication styles may need some further explanation. Borderline personality disorder is defined in the DSM-IV as a pervasive pattern of instability of interpersonal relationships, self-image and affects, and marked impulsivity (American Psychiatric Association, 1994). Victims with borderline traits might typically have unstable interpersonal relationships and poorer relationship skills through which they might have more frequent relationship conflicts. Furthermore, they may have difficulties with controlling their anger, which is another typical borderline trait. The expression of uncontrolled anger and the more frequent relationship conflicts of victims with borderline traits might lead to more severe partner violence committed against them. As such, our findings suggest that the partner violence that some victims experience may be influenced by negative communication patterns on the part of the victim. Victims who, for whatever reason, lash out verbally or psychologically against their partner are at a higher risk of experiencing either physical IPV or more severe forms of psychological IPV (e.g., being called fat or ugly, destroyment of victims’ personal belongings by partner). Apparently, victims’ negative communication styles mainly influence the risk of more serious forms of revictimization, as they seem to relate to the occurrence of any physical IPV revictimization and the severity of psychological IPV revictimization, but not to the occurrence of any psychological IPV revictimization, which may be considered a less serious form of partner violence. However, for a more complete understanding of the negative communication patterns that may be found to play a role in IPV, it is important to keep in mind the ongoing controversies in the field of gender and partner violence. The debate on gender and partner violence has “raised questions about the extent to which, and under what conditions, men and women’s violence toward each other should be understood as similar or different” (Langhinrichsen-Rohling, 2010, p. 179). Importantly, this debate should take the motivations for the use of violence into account (see Langhinrichsen-Rohling, 2010). Research has shown that women report various reasons for their use of partner violence including, but not restricted to self-defense (e.g., Bair-Merritt et al., 2010). However, the extent to which self-defense may be a primary motive for female perpetration but not for male perpetration of partner violence is still a topic of ongoing discussion (see Langhinrichsen-Rohling, 2010). For instance, in their review of research on women’s use of partner violence, Swan and colleagues (Swan, Gambone, Caldwell, Sullivan, & Snow, 2008) report on several studies that show women’s violence to be more likely than men’s violence to be motivated by self-defense (e.g., Barnett, Lee, & Thelen, 1997; Hamberger, 2005; Makepeace, 1986). Yet, other studies suggest different primary motives for women’s violence, such as poor communication, revenge, retaliation, and anger (Hettrich & Daniel O’Leary, 2007; Kernsmith, 2005). In the current study, we did not assess the motives for the partner violence that was reported. Therefore, we have no information about victims’ reasons for their use of violence or the context in which the victim perpetrated violence against her partner.
Based on our study results, several recommendations for practice and research can be formulated. First, practitioners are encouraged to assess not only the recent violence committed against the victim but also the recent violence that has been perpetrated by the victim, as these both seem to be relevant factors in the continuation of partner violence. Victims who use partner violence themselves, especially acts of psychological violence, appear to be at higher risk of revictimization by physical violence. Decreasing victims’ psychological abuse could be facilitated by teaching victims how to manage and control their emotions such as anger or anxiety, and by handing them strategies that help them to cope effectively with conflict situations. Next, we found that victims’ psychological difficulties increase risk for more severe revictimization by psychological IPV. Particularly victims’ borderline traits seem to play an important role here. Practice could screen for presence of borderline traits in victims and start treatment aimed at effectively coping with these traits. Screening for borderline traits is important not only in terms of future IPV revictimizations but also in preventing the development of PTSD (see Kuijpers, Van der Knaap, Winkel, Pemberton, & Baldry, 2011), which in itself is a risk factor for partner violence as well (Perez & Johnson, 2008; Winkel, 2007). Regarding future research, further exploration of various resilience factors in the victim and their relation to revictimization of IPV is necessary. In the current study, victims’ resilience was operationalized as victims’ self-assessed quality of life. However, Foa et al. (2000) defined resilience as involving optimism, self-esteem, flexibility, and physical health. Although we found that victims’ quality of life is not related to risk for IPV revictimization in a multivariate model, it might be possible that other aspects of victims’ resilience actually are significant protective factors. A broader, more varied way of measuring victims’ resilience might lead to a more in-depth understanding of how this dynamic victim-related factor may be associated with risk for IPV revictimization. Furthermore, we argue for conducting this type of research into dynamic victim-related risk and protective factors in a more general population. Our current sample consists of a specific subsample of female help-seeking IPV victims who are registered as such at victim organizations, which limits the generalizability of our findings. Studying a more general sample might also provide us with knowledge about risk and protective factors among victims who do not seek help after experiencing episodes of partner violence.
When interpreting the results of our study, several limitations must be considered though. First, we did not differentiate between repeat partner violence from the same (ex-)partner versus partner violence from a new/different (ex-)partner. In other words, victims’ reports of received aggression could be based not only on the same male (ex-)partner but also on different (ex-)partners. Yet, for the current study we chose a victim approach by specifically examining characteristics and behaviors that are within victims’ control and that could help them to curtail future partner violence. Therefore, we were more interested in the question whether a specific victim was revictimized by some form of IPV than by who she was revictimized. Victims’ reports of revictimization by a specific person may lead to exclusion of IPV acts (because they were perpetrated by other (ex-)partners) and, in that way, predictors may only be applicable to the continuation or cessation of IPV by that specific male partner. Also, we only used victims’ self-reports to obtain information about partner violence that occurred and the (psychological) complaints they might have developed. Consideration of additional perpetrator self-reports would have provided us with the opportunity to see to what extent the victim and perpetrator agree on, for instance, the amount of partner violence they experienced. Furthermore, for our outcome measures regarding the severity of IPV revictimization, we were only able to perform analyses for the severity of revictimization by psychological IPV, due to insufficient statistical power for the outcome concerning severity of physical IPV. A larger sample size with more victims who reported to be revictimized by physical IPV would have increased statistical power, thereby preventing this limitation. Yet, it is a reassuring sign that the large majority of victims in our sample manages to keep themselves safe and is not revictimized by any physical partner violence.
Despite these limitations, the current study makes a relevant contribution to the relatively scarce prospective findings regarding victim-related risk and protective factors for IPV revictimization so far (see Kuijpers, Van der Knaap, & Lodewijks, 2011, for a review of prior prospective research in this area). Our results are in line with a wide array of research that shows (frequency and/or severity of) prior IPV victimization(s) to predict IPV revictimization (e.g., Bennett Cattaneo & Goodman, 2003; Hirschel & Hutchison, 2003; Krause et al., 2006; Perez & Johnson, 2008). Regarding victim-related variables in specific, our finding that partner violence perpetrated by the victim is related to future IPV victimization has been supported by prior, mainly cross-sectional studies as well (e.g., Anderson, 2002; Fergusson et al., 2005; Stith et al., 2004). Also, various psychological difficulties in victims have been reported to relate to risk for (repeat) partner violence (Foa et al., 2000; Krause et al., 2006; Perez & Johnson, 2008; Stith et al., 2004). Regarding borderline traits in particular, positive correlations have been reported between the severity of borderline personality disorder and the severity and extent of IPV victimization in cross-sectional studies (Sansone, Chu, & Wiederman, 2006; Shields, Resick, & Hanneke, 1990). As such, our results are not new but since our study was longitudinal in nature, the contribution to the literature lies within the prospective evidence we present. Moreover, this is one of the most comprehensive studies into dynamic victim-related risk factors, as it examines a wide variety of factors within victims’ sphere of influence in relation to IPV revictimization.
Concluding, our results provide support for several aspects of Foa et al.’s (2000) models on women’s influence on IPV (i.e., the key factor partner violence and victims’ psychological difficulties) and, moreover, show which victim-related factors contribute to revictimization risk above and beyond the influence of prior violence committed by a partner against the victim (i.e., victims’ prior IPV victimizations). As indicated earlier, a focus on victim-related factors is important because these are factors within victims’ own sphere of influence (Bennett Cattaneo & Goodman, 2005). It can help victims to take control over their lives and may serve as a way to empower victims of partner violence (Goodman et al., 2005; Perez & Johnson, 2008). Especially dynamic victim-related factors seem to be key elements in preventing future IPV, as these are changeable and intervenable factors. Knowledge on these factors might support victims of IPV to be active change agents (Foa et al., 2000) and help them to end the abuse they experience at the hands of their partners.
Footnotes
Acknowledgements
The authors would like to thank the Achmea Foundation Victim and Society that financially supported this study. Data collection was done in collaboration with Stichting Valkenhorst Breda, Bureau Slachtofferhulp Breda, Instituut voor Maatschappelijk Welzijn Breda, Veiligheidshuis Breda, Veiligheidshuis Bergen op Zoom, Traverse, GGZ Westelijk Noord-Brabant, LEV-groep Helmond, Slachtofferloketten Openbaar Ministerie Breda, Middelburg, Utrecht, Den Haag and Rotterdam, and the “local domestic violence teams” with all their cooperating partners and organizations of GGD Rotterdam.
At the time this study was conducted, Karlijn F. Kuijpers was employed at the International Victimology Institute Tilburg (INTERVICT) at Tilburg University, the Netherlands. Currently she is working at the Institute for Criminal Law and Criminology at Leiden University, the Netherlands.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank the Achmea Foundation Victim and Society that financially supported this study.