
Abstract
Women who experience recurrent intimate partner violence (IPV) may use alcohol or drugs because they expect that these substances will help them cope with the negative physical and psychological sequelae of IPV. However, expectancies for alcohol and drug use have not been explored among this population of women. We used the Relaxation and Tension-Reduction Scale, Arousal and Aggression Scale, and Social Assertion Scale of the Alcohol Expectancy Questionnaire and modified its items to assess both alcohol and drug expectancies of 212 community-based, IPV-exposed women. Results of bivariate correlations showed that greater alcohol and drug expectancies were significantly correlated with greater alcohol problems and greater posttraumatic stress total and symptom severity scores. Results of a multivariate regression model showed that after controlling for demographic characteristics and history of childhood trauma, Relaxation and Tension- Reduction expectancies were associated with number of days of alcohol use, alcohol problems, physical and sexual IPV severity scores, and posttraumatic stress total and reexperiencing symptom severity scores. Expectancies do not significantly moderate the relationships between IPV, posttraumatic stress, and problematic alcohol and drug use. Given the strong relationships of expectancies with IPV severity, posttraumatic stress, and alcohol problems, expectancies may serve as targets for interventions to reduce alcohol use and problems and improve health-related outcomes in IPV-exposed women.
Introduction
Women exposed to intimate partner violence (IPV) are at high risk for heavy and problematic alcohol and drug use (Centers for Disease Control and Prevention, 2008; Cunradi, 2007; Cunradi, Caetano, & Schafer 2002; El-Bassel et al., 2004; El-Bassel, Gilbert, Wu, Go, & Hill, 2005; McKinney, Caetano, Rodriguez, & Okoro, 2010; Salomon, Bassuk, & Huntington, 2002; cf., White & Chen, 2002). The nature of the relationship between IPV and alcohol and drug use is complex, such that experiences of victimization may contribute to the use of alcohol and drugs or vice versa (Martino, Collins, & Ellickson, 2005; Testa, Livingston, & Hoffman, 2007; Testa, Livingston, & Leonard, 2003; Testa, VanZile-Tamsen, & Livingston, 2007). If IPV-exposed women use alcohol and drugs as a coping strategy, they may do so because they expect that substance use will alleviate negative physical and psychological sequelae of IPV (Martino et al., 2005). This framework is in line with the self-medication hypothesis and tension reduction models of alcohol and drug use (Conger, 1956; Khantzian, 1997).
In addition to being at high risk for problematic alcohol and drug use, women exposed to IPV are at high risk for mental health problems, including posttraumatic stress; 31%-84% of IPV-exposed women report posttraumatic symptoms severe enough to be diagnosed with PTSD (Anderson, 2002; Burnam et al., 1988; Coker et al., 2002; Coker, Weston, Creson, Justice, & Blakeney, 2005; Golding, 1999). Furthermore, large epidemiological studies have documented the comorbidity of substance use disorders and PTSD to be between 27% and 52% (Chilcoat & Breslau, 1998a, 1998b; Cottler, Compton, Mager, Spitznagel, & Janca, 1992; Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). Because of its strong relationship with problematic alcohol and drug use (Breslau, Davis, Peterson, & Schultz, 1997; Breslau, Davis, & Schultz, 2003; Najavits, Weiss, & Shaw, 1997), posttraumatic stress has been examined as an important factor in the relationship between IPV and problematic alcohol and drug use. Indeed, recent research has suggested that posttraumatic stress may mediate the relationship between IPV and drug-related problems (Kaysen et al., 2007; Sullivan, Cavanaugh, Buckner, & Edmondson, 2009).
Although expectancies for alcohol and drug use are associated with problematic alcohol and drug use among the general population and people seeking substance use treatment, expectancies have not been studied among the high-risk population of IPV-exposed women. Thus, it is unclear what role positive and negative expectancies for alcohol and drug use play in the relationships among IPV, posttraumatic stress, and alcohol and drug use. Stronger positive expectancies of alcohol use, which are thoughts that consuming alcohol will produce desirable outcomes, are associated with greater alcohol consumption and related problems (Brown, Goldman, Inn, & Anderson, 1980; Jones, Corbin, & Fromme, 2001). Similarly, stronger positive expectancies related to marijuana and cocaine use are associated with heavier drug consumption (Hayaki et al., 2010; Schafer & Brown, 1991; cf., Galen & Henderson, 1999). Positive expectancies for alcohol and drug use are distinct from negative expectancies, which are thoughts that alcohol and drug use will produce undesirable outcomes, in that negative expectancies tend to restrain alcohol and drug consumption (Jones et al., 2001). Although the relationships of expectancy measures to alcohol and drug use vary depending on how each is measured, positive alcohol expectancies are typically associated with quantity, rather than frequency, of alcohol use (Jones et al., 2001). Importantly, positive alcohol expectancies predict changes in drinking and the development of alcohol-related problems (Jones et al., 2001). Given the prevalence of alcohol and drug use among IPV-exposed women (i.e., 7%-44% report drug and alcohol problems severe enough to be diagnosed with substance abuse or dependence; Golding, 1999), we would expect that stronger positive expectancies for alcohol and drug use also would be associated with heavier alcohol and drug consumption and related problems in this population. Although alcohol expectancies are related to dating violence among college students (Williams & Smith, 1994) and to female perpetration of IPV (Rapoza & Baker, 2008), we are not aware of data describing alcohol and drug expectancies in the unique population of community-based victims of recurrent IPV. In other populations, both alcohol and drug expectancies are modifiable with intervention (Darkes & Goldman, 1993, 1998; Jones & McMahon, 1996); if expectancies are associated with alcohol and drug consumption and problems in IPV-exposed women, expectancies may serve as targets in future community- or clinic-based interventions aimed to reduce alcohol and drug use and associated problems.
As this is the first study to examine alcohol and drug expectancies in IPV-exposed women, we sought to understand how expectancies are associated with other prevalent and clinically meaningful characteristics of this high-risk group, including severity of physical, sexual, and psychological IPV; severity of mental health problems such as posttraumatic stress and depression; and strategies to cope with IPV after controlling for demographic characteristics and childhood trauma, the latter of which is a known correlate with both IPV and substance use (Anda et al., 2006; Whitfield, Anda, Dube, & Felitti, 2003). We also sought to explore whether positive expectancies moderate the relationships between IPV, posttraumatic stress, and alcohol and drug use. If expectancies moderate these relationships, then alcohol- and drug-related interventions can be targeted to those IPV-exposed women who report greater positive expectancies. Thus, we hypothesized that IPV-exposed women with greater positive expectancies would report stronger relationships between IPV and alcohol and drug use, and between posttraumatic stress and alcohol and drug use, than IPV-exposed women with weaker positive expectancies.
Method
Sample
We examined alcohol and drug use, problems, and expectancies in a cross-sectional study that was largely focused on risk and protective factors for IPV-related posttraumatic stress and substance use among community-based women who were currently experiencing IPV (see Sullivan et al., 2009 for further details about study methods). We recruited 240 women from an urban community in New England to participate “in a 2-hour interview about the relationship with your boyfriend or husband.” Flyers with tear-off sheets were posted in community establishments such as grocery stores and nail salons, agencies such as the Department of Adult Education, and two primary care clinics. Women completed a telephone screen to determine their eligibility to participate in the study. The primary inclusion criterion was that a woman experienced at least one act of physical victimization within the past 6 months by her current male partner, as measured by selected screening questions from the Conflict Tactics Scale-2 (CTS-2; Straus, Hamby, & Warren, 2003). The final sample was composed of 212 women.
A 2-hour, semistructured, computer-assisted interview was administered by trained master- or doctoral-level female research associates in private offices to protect participants’ safety and confidentiality. No participant reported safety concerns. After completion of the interview, participants were debriefed, remunerated US$50, and provided with a list of community resources for employment, food, and benefits assistance; mental health and substance use treatment; and domestic violence services. All procedures were approved by the internal review board of the Yale University School of Medicine.
Measures
The Alcohol Expectancy Questionnaire (AEQ; Brown, Christiansen, & Goldman, 1987) is a reliable and valid self-report instrument that assesses expected or anticipated outcomes related to alcohol consumption. To minimize response burden, we administered three of the six scales of the AEQ: (a) the 9-item Relaxation and Tension-Reduction Scale (e.g., “If I am tense or anxious, having a few drinks or using drugs makes me feel better”; α = .83), (b) the 5-item Arousal and Aggression Scale (e.g., “After a few drinks or using drugs, it is easier to pick a fight”; α = .54), and (c) the 11-item Social Assertion Scale (e.g., “If I have a couple of drinks or use drugs, it is easier to express my feelings”; α = .91). As we sought to understand expectancies related to consumption of alcohol and drugs, we modified items by asking participants to respond based on their “own personal thoughts, feelings and beliefs about alcohol and drugs”. Participants reported their expectancies using the AEQ dichotomous response format (agree = 1; disagree = 0). Sum scores were created for each scale. Higher scores indicate stronger expectancies that alcohol and drug consumption will reduce tension, increase arousal and aggression, and increase social assertion.
The number of days of alcohol, cocaine, marijuana, and nonheroin opioid use in the past 6 months was determined with the Addiction Severity Index (ASI; McLellan et al., 1992). Alcohol problems experienced over the previous 6 months were assessed with the 10-item Alcohol Use Disorders Identification Test (AUDIT; Babor, Higgins-Biddle, Saunders, & Monteiro, 2001). The sum of all items (e.g., “How often during the last year have you failed to do what was normally expected from you because of drinking?”) produced a total score; a higher total score reflects a greater likelihood of risks and problems related to alcohol use (α = .90). Drug problems over the previous 6 months were assessed with the 10-item version of the Drug Abuse Screening Test (DAST; Skinner, 1982). The DAST assessed problems associated with all drugs (excluding alcohol; e.g., “Did you ever experience withdrawal symptoms [felt sick] when you stopped taking drugs?”). The sum of affirmatively endorsed items (0 = no; 1 = yes) produced a total score (α = .87). We included the AUDIT and DAST after enrolling several participants; thus, 158 of the 212 participants provided data on alcohol problems, and 180 of the 212 participants provided data on drug problems.
A referent time period of 6 months was used to assess the partner’s commission of IPV behavior toward the woman. Physical IPV was measured by the 78-item CTS-2 (Straus et al., 2003). Response options that were a range were recoded according to Straus et al. (2003; e.g., “6-10 times” was recoded to the midpoint of 8). The physical IPV score was a sum of 12 items of physical aggression (e.g., pushing or shoving, slamming against a wall; α = .88). Frequencies of sexual and psychological IPV were measured by the Sexual Experiences Survey (SES; Koss, Gidycz, & Wisniewski, 1987) and the Psychological Maltreatment of Women Inventory (PMWI; Tolman, 1989), respectively, because these measures assess their respective domains more comprehensively than the CTS-2. The sexual IPV variable was a sum of the 10 SES items. Given that the SES has been used largely with college populations and requires a fairly high reading level, the measure was revised to improve comprehension among study participants (e.g., “Has your partner tried to make you have sex by using force like twisting your arm or holding you down, or by threatening to use force?”; α = .89). The 48 PMWI items (e.g., “My partner tried to keep me from seeing or talking to my family”) with response options from 1 (never) to 5 (very frequently) were summed to create a total score (α = .96).
IPV-related posttraumatic stress was measured with the 49-item Posttraumatic Stress Diagnostic Scale (PDS; Foa, 1995). To examine posttraumatic stress related to current IPV exposure, Diagnostic Criterion A was assessed in relation to IPV by the current partner for the duration of the relationship (i.e., we instructed participants to consider “all of the abusive events that have happened throughout your relationship with your partner, [such as] hitting, slapping, grabbing, or pushing”). Diagnostic Criteria B (reexperiencing symptoms), C (avoidance and numbing symptoms), D (arousal symptoms), E (duration of symptoms), and F (symptoms’ impact on functioning; American Psychiatric Association, 1994) were assessed over the previous 6 months. The occurrence of reexperiencing, avoidance and numbing, and arousal symptoms was rated on a 4-point scale from 0 (not at all) to 3 (almost always). Severity scores were summed for each symptom category separately, and total severity scores were summed for all 17 symptoms (range 0-51). Depressive symptoms within the past 6 months were assessed using the Center for Epidemiological Studies-Depression Scale (CES-D; Radloff, 1977). The response scale ranges from 0 (experienced symptoms 0 days in the last 6 months) to 3 (experienced symptoms 5-7 days in the last 6 months), and all 20 items (e.g., “I felt that everything I did was an effort”) were summed to create the total score (α = .91). Total scores range from 0 to 60, with higher scores indicating more symptoms of depression. Strategies for coping with conflict in the current relationship were assessed with the Coping Strategy Indicator (CSI; Amirkhan, 1990). The CSI is a 33-item measure that assesses problem-solving coping (e.g., brainstormed all possible solutions before deciding what to do, α = .84), social-support coping (e.g., confided fears and worries to a friend or a relative, α = .94), and avoidance coping (e.g., slept more than usual, α = .75). Participants were instructed to describe a conflict with their intimate partners in the past 6 months that was important to them and caused them to worry, and to rate the extent to which they used each of the 33 strategies with respect to that conflict: 1 (not at all), 2 (a little), and 3 (a lot). Each subscale is composed of 11 items that were summed to create a subscale score.
Childhood trauma was assessed with the 28-item brief version of the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 2003) that assesses experiences of physical, sexual, and emotional abuse, and physical and emotional neglect in childhood and adolescence (e.g., “When I was growing up, I got hit or beaten so badly that it was noticed by someone like a teacher, neighbor, or doctor”). The 25 clinical items are rated on a 5-point, Likert-type scale with response options ranging from 1 (never true) to 5 (very often true) and were summed to create a total score (α = .93).
Data analysis
Bivariate correlations and a multivariate regression model investigated the relationships between the three expectancy scale scores and the following characteristics:
number of days of alcohol, cocaine, marijuana, and nonheroin opioid use;
alcohol and drug problems;
physical, sexual, and psychological IPV scores;
posttraumatic stress total and symptom severity scores;
depression total scores; and
coping strategy scale scores.
Only characteristics that were significant bivariate correlates with any of the three expectancy scale scores (p < .05) were included as dependent variables in the multivariate regression model. Expectancy scores were included as independent variables. The model included the CTQ total score as a covariate because childhood trauma is a known correlate of adult IPV victimization and substance use (Anda et al., 2006; Whitfield et al., 2003). The model also included age, race, and employment status as covariates because each of these demographic characteristics was significantly correlated with at least one of the dependent variables.
To test moderation effects of expectancy scale scores, separate multiple regression models tested expectancy scores as moderators of the relationship between (a) physical, sexual, and psychological IPV and alcohol and drug use; (b) physical, sexual, and psychological IPV and alcohol- and drug-related problems; (c) posttraumatic stress and alcohol and drug use; and (d) posttraumatic stress and alcohol- and drug-related problems. In these tests of moderation, CTQ total score, age, race, and employment status were included as covariates; IPV/posttraumatic stress were independent variables on the first regression step; and the interaction of IPV/posttraumatic stress and the expectancy scale scores were independent variables on the second regression step. Evidence of the moderating effects of expectancies would be seen if the interaction of IPV/posttraumatic stress and expectancies accounted for significantly more variance than the main effect of either IPV/posttraumatic stress or the expectancy score.
Results
Sample Description
The average age of the 212 participants was 36.6 years (SD = 10.5). The majority of women were unemployed (65%), with a mean level of education of 12.1 years (SD = 1.6). The mean years in the relationship at the time of the interview was 6.5 (SD = 6.4), with more than half of the sample married or cohabitating (59%). One hundred forty-two women were African American (67%), 43 (20%) were White, 17 (8%) were Latina, and 10 (5%) were identified as multiracial. The high percentage of African American women may be due to the nature of the urban community where participants were recruited (37% African American) or to the fact that IPV tends to be higher in African Americans than in Whites or Hispanics (Caetano, Field, Ramisetty-Mikler, & McGrath, 2005).
For a full description of characteristics related to IPV and alcohol and drug use, see Sullivan et al. (2009). Briefly, 71% experienced severe physical victimization, 39% experienced rape by their current partners, and 34% met full criteria for PTSD. Twenty-nine percent of participants had not used alcohol or any drugs in the prior 6 months. Among the 126 participants who used any alcohol in the past 6 months, they used alcohol on a mean of 33.0 days (SD = 43.0) in the past 6 months and their mean AUDIT score was 7.6 (SD = 7.6), reflecting problematic alcohol use. Among the 99 who reported using any drug in the past 6 months, cocaine was used on a mean of 30.9 (SD = 35.4) days in the past 6 months, nonheroin opioids were used on a mean of 21.4 (SD = 51.2) days, and cannabis on a mean of 18.1 (SD = 42.7) days. Their mean DAST score was 3.6 (SD = 2.7), reflecting problematic drug use.
Bivariate Associations With Expectancy Scores
The 212 participants reported mean expectancy scores of 5.2 (SD = 2.8), 3.0 (SD = 1.3), and 7.3 (SD = 3.8) on the Relaxation and Tension Reduction, Arousal and Aggression, and Social Assertion scales, respectively. All three expectancy scores were significantly and positively correlated with alcohol problem scores, posttraumatic stress total and symptom severity scores, and depression symptom scores (all ps < .05; Table 1). In addition, Relaxation and Tension-Reduction expectancy scores were significantly and positively correlated with number of days of alcohol use, number of days of cocaine use, and severity of physical and sexual IPV (all ps < .05). None of the three expectancies scores were correlated with any demographic characteristic.
Bivariate Correlations With Alcohol and Drug Expectancy Scale Scores.
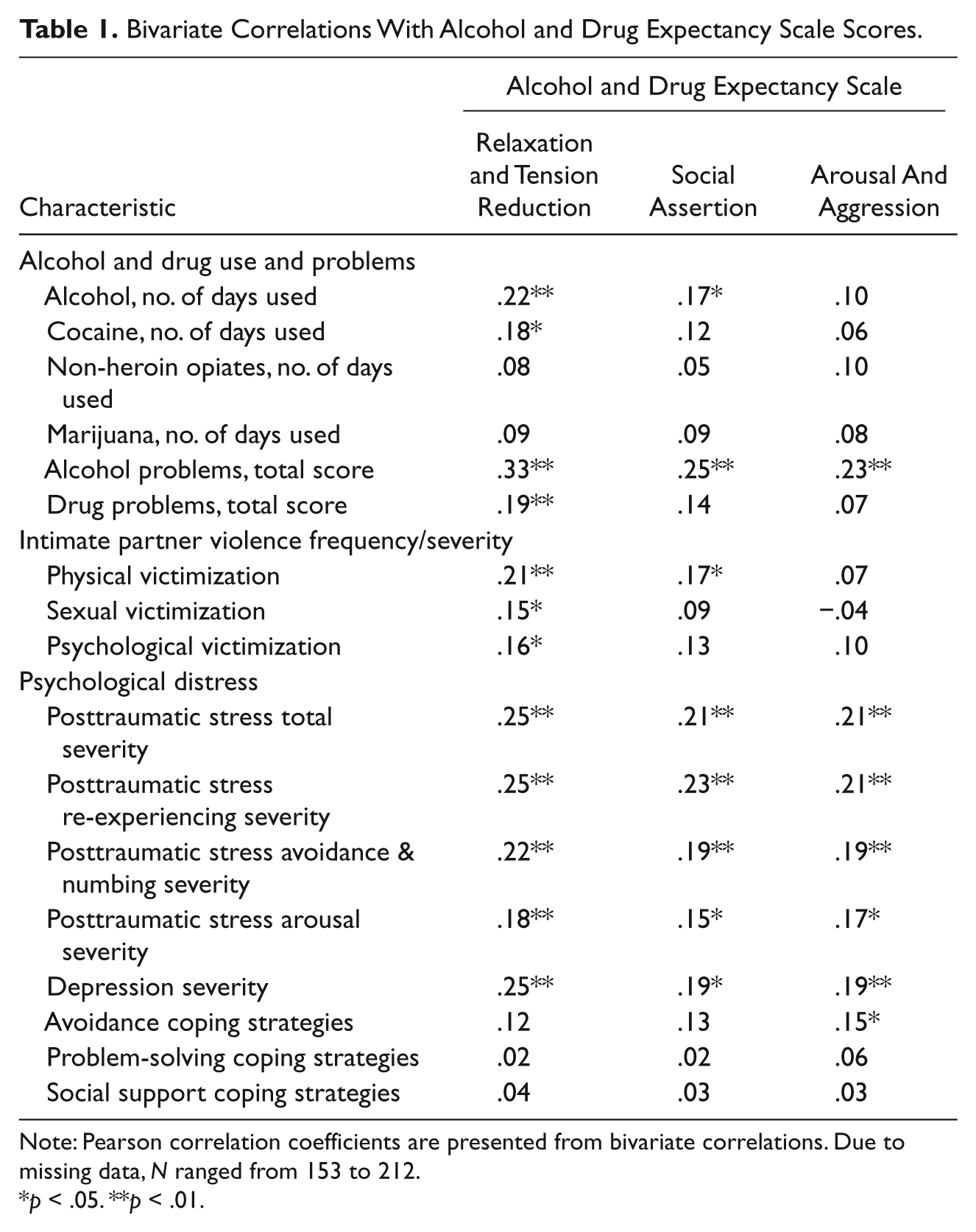
Note: Pearson correlation coefficients are presented from bivariate correlations. Due to missing data, N ranged from 153 to 212.
p < .05. **p < .01.
Multivariate Associations With Expectancy Scores
In a multiple regression model holding age, race, employment status, and history of childhood trauma constant, only Relaxation and Tension-Reduction expectancy scores were significantly associated with the combination of dependent variables, F(9,139) = 2.29, p = .02. Post hoc tests showed that Relaxation and Tension-Reduction expectancy scores were significantly associated with number of days of alcohol use, alcohol problems, physical and sexual IPV severity scores, and posttraumatic stress total and reexperiencing symptom severity scores (all ps < .05; Table 2). 1
Multivariate Associations With Relaxation and Tension-Reduction Expectancy Scores
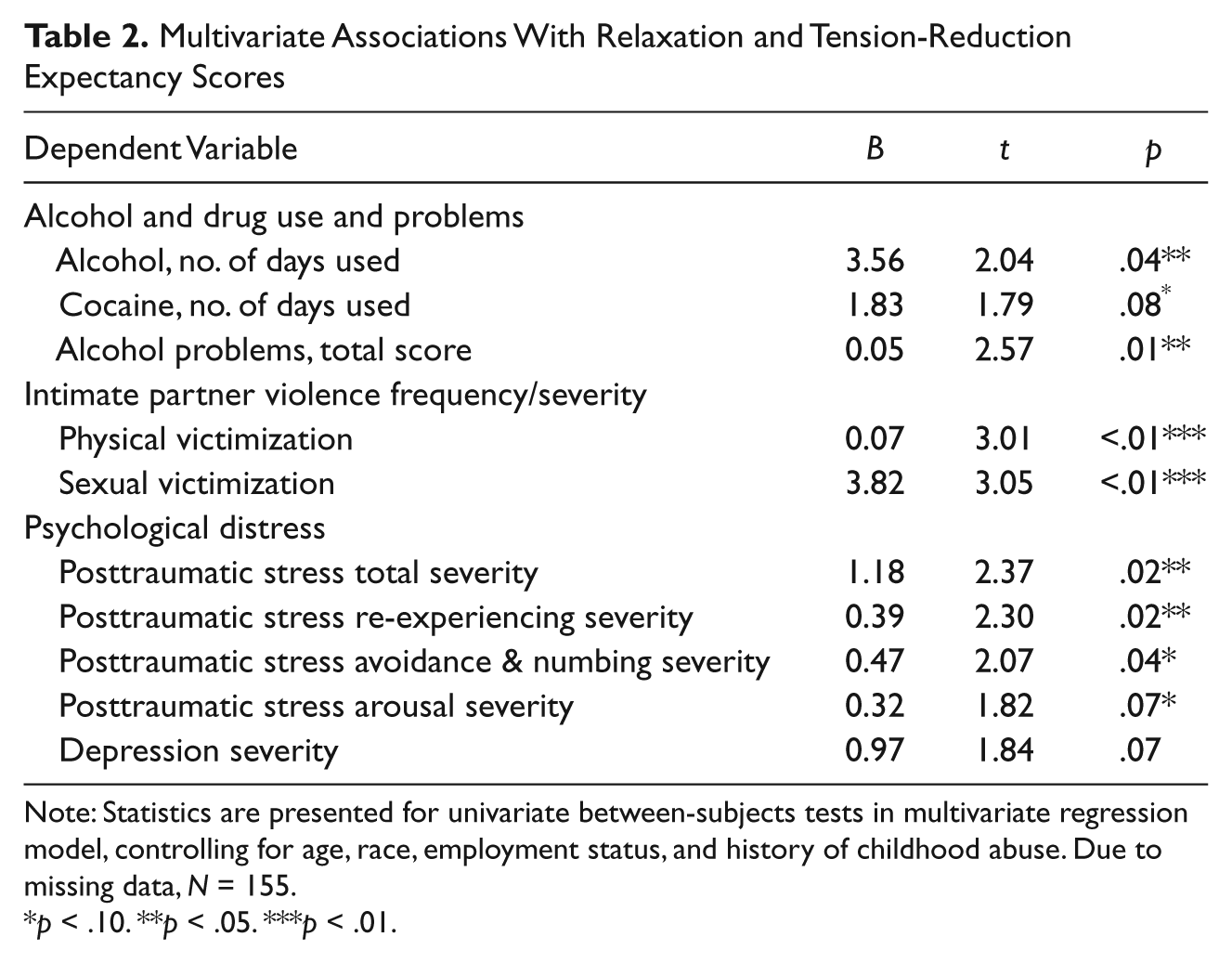
Note: Statistics are presented for univariate between-subjects tests in multivariate regression model, controlling for age, race, employment status, and history of childhood abuse. Due to missing data, N = 155.
p < .10. **p < .05. ***p < .01.
Moderators of Association Between IPV, Posttraumatic Stress, and Alcohol Use
As Relaxation and Tension-Reduction expectancies, but not Social Assertion nor Arousal and Aggression expectancies, were strongly associated with IPV, posttraumatic stress, alcohol use, and alcohol-related problems, subsequent analyses examined only Relaxation and Tension-Reduction expectancy scores as a possible moderator of these relationships. In addition, moderation analyses only included number of days of alcohol use and alcohol problems as dependent variables because they were more strongly correlated with Relaxation and Tension-Reduction expectancy scores than were drug use and drug problems. After covarying for age, race, employment status, and history of childhood trauma, Relaxation and Tension-Reduction expectancy scores did not significantly interact with physical, sexual, or psychological IPV, or with posttraumatic stress total symptom severity, to predict number of days of alcohol use or alcohol problems.
Discussion
Among community-based women who experience IPV, expectancies for alcohol and drug use, especially expectancies related to Relaxation and Tension Reduction, were associated with frequency of alcohol use and severity of alcohol problems, IPV, and PTSD. This study replicates findings on the association between expectancies and alcohol use and extends them to a high-risk population of women who are victims of IPV.
Consistent with findings in the general population and in substance abusers (Jones et al., 2001), stronger positive alcohol and drug expectancies in IPV-exposed women were correlated with worse alcohol-related problems. As IPV-exposed women are at high risk for heavy and problematic substance use (Anderson, 2002; Burnam et al., 1988; El-Bassel et al., 2004, 2005; Kantor & Straus, 1989; Martino et al., 2005; Quigley & Leonard, 2000; Salomon et al., 2002; Stalans & Ritchie, 2008; Testa & Leonard, 2001; Testa et al., 2003; cf., White & Chen, 2002), interventions addressing substance use are needed in this population. Our findings of a significant association between expectancies and problematic alcohol use suggest that expectancies may represent targets for these interventions. In other populations, interventions to modify expectancies have provided information that contradicts expectancies and have delivered motivational enhancement strategies that address anticipated negative outcomes of substance use; these modifications in expectancies have led to reductions in substance use (Darkes & Goldman, 1993, 1998; Jones & McMahon, 1996). Future research might examine, first, whether expectancies predict treatment outcome in IPV-exposed women and, second, whether interventions to modify expectancies have beneficial effects on substance use in this high-risk population.
Consistent with findings in college women who are victims of sexual assault (Corbin, Bernat, Calhoun, McNair, & Seals, 2001; Marx, Nichols-Anderson, Messman-Moore, Miranda, & Porter, 2000; Messman-Moore, Coates, Gaffey, & Johnson, 2008), community-based victims of recurrent IPV report correlations between alcohol and drug expectancies and the severity of physical and sexual IPV. Thus, results from the present study support prior findings on the important relationship between expectancies and victimization and extend them to a unique group of community-based victims. Results from this study also point to an association between alcohol and drug expectancies and psychological distress (i.e., posttraumatic stress) secondary to IPV. Due to the prevalence and severity of PTSD in this population (Golding, 1999), there would seem to be a need to address posttraumatic stress and alcohol and drug expectancies in substance-related interventions. Evidence-based treatments for PTSD among women who have substance use problems exist (Hien, Cohen, Miele, Litt, & Capstick, 2004; Najavits, 2002); however, none are for women who continue to be in unsafe intimate relationships. Although we detected strong correlations between alcohol and drug expectancies and symptoms of posttraumatic stress, we did not observe evidence supporting a relationship between expectancies and coping styles (cf., Cooper, Russell, & George, 1988). Participants in this study rated their coping strategies with respect to conflicts with their partners, and it is possible that if instead they rated their use of coping strategies with respect to less-specific situations or to non-IPV-related situations, their reports would differ.
Results from multivariate analyses in this community-based sample of women currently exposed to IPV confirmed the significant association between alcohol and drug expectancies and alcohol problems that has been found in the general population and in treatment-seekers (Jones et al., 2001). Results also provide new information on how expectancies for relaxation and tension reduction are related to severity of IPV and PTSD symptomatology. The association between Relaxation and Tension-Reduction expectancies and severity of IPV points to the possibility that IPV-exposed women use alcohol or drugs specifically to manage the negative effects of recurrent victimization, e.g., they may consume more alcohol to attenuate tension resulting from being victimized. Moreover, the association between Relaxation and Tension-Reduction expectancies and PTSD severity has clinical implications insofar that IPV-exposed women may expect that alcohol and drug use will alleviate their psychological distress, particularly regarding re-experiencing symptoms such as nightmares or intrusive thoughts. If our findings are replicated, then future substance-related interventions for this special population of IPV-exposed women might address the overlap between expectancies for relaxation and tension reduction, IPV severity, and posttraumatic stress.
As an initial step in understanding the complex relationships between expectancies, severity of IPV, posttraumatic stress, and problematic alcohol and drug use, we sought to investigate whether expectancies moderated the relationships between these other clinically-important characteristics of IPV-exposed women. However, we did not find evidence in support of expectancies for alcohol and drug use moderating the relationships between IPV, posttraumatic stress, and alcohol and drug use. The lack of moderating effects suggests that future substance-related treatments for IPV-exposed women may not need to differentially target women with greater expectancies for alcohol and drug use. With larger sample sizes, future studies may further elucidate the role expectancies for alcohol and drug use play with respect to IPV, posttraumatic stress, and problematic alcohol and drug use.
Findings from this study are limited by inclusion of only three of the six scales of the AEQ and by modifying the wording of AEQ items to include expectancies for alcohol and other drugs. Although we had hypothesized that modification of the AEQ items would not be of significant concern because of overlapping effects of some drugs (Julien, 1987), expectancies might differ for different substances. To more fully understand alcohol and drug expectancies of IPV-exposed women, future studies might include the recently-developed Posttraumatic Stress Disorder—AEQ (Norman, Inaba, Smith, & Brown, 2008) because it specifically assesses beliefs about how substance use will affect PTSD symptoms and thus may be appropriate in IPV-exposed women. An intensive longitudinal study could examine within-day associations of alcohol and drug expectancies with alcohol and drug use and problems and PTSD symptoms, and a larger sample could address racial and ethnic differences in expectancies for alcohol and drug use. If findings are replicated, future substance-related interventions for IPV-exposed women might incorporate motivational enhancement strategies to reduce expectancies for alcohol and drug use or provide effective strategies for reducing tension associated with IPV and increasing relaxation.
Conclusion
Among a special population of IPV-exposed women, we observed that expectancies for alcohol and drugs to reduce tension are associated with more frequent alcohol use and more severe alcohol problems, greater severity of IPV, and more severe symptoms of PTSD, specifically reexperiencing symptoms. Results have clinical implications for targeting those IPV-exposed women who would be most likely to report strong expectancies for alcohol and drug use (i.e., those with more severe IPV and symptoms of PTSD) and would, thus, benefit most from interventions to reduce their problematic substance use and improve their health-related outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research described here was supported, in part, by grants from the National Institute on Drug Abuse (R03 DA17668; K23 DA019561; R25 DA020515).