
Abstract
Eastern DRC has been the site of a protracted conflict in which sexual violence has been a defining feature. The method used was a retrospective registry-based study of sexual violence survivors presenting to Panzi Hospital between 2004 and 2008. This analysis aimed to describe the patterns of sexual violence described by survivors and to analyze perpetrator profiles. As regards results, a total of 4,311 records were analyzed. Perpetrators in this data set were identified as follows: (a) 6% were civilians; (b) 52% were armed combatants; and (c) 42% were simply identified as “assailant(s)” with no further identifying information. Those identified simply as “assailants” perpetrated patterns of sexual violence that were similar to those of armed combatants, suggesting that this group included a large number of armed combatants. Civilian assailants perpetrated a pattern of sexual violence that was distinct from armed combatants. Conclusions are as follows: These data suggest that a high proportion of sexual assaults in South Kivu are perpetrated by armed combatants. Protection of women in South Kivu will require new strategies that take into account the unique nature of sexual violence in DRC. Engaging with local communities, the UN and other aid organizations is necessary to create new context-appropriate protection programs.
Introduction
Accounts of rape in conflict date back almost as far as accounts of war itself (Gottschall, 2004). There is perhaps no clearer example of the brutality and widespread nature of rape in modern-day conflict than in the Democratic Republic of the Congo (DRC). International organizations have reported their observations from working with rape survivors in Eastern DRC (Amnesty International, 2004; Human Rights Watch, 2002, 2004, 2005, 2009; Medécins Sans Frontières, 2004, Steiner et al., 2009; Réseau des Femmes pour un Développement Associatif et al., 2005; Wakabi, 2008). In 2011, a nationally representative household survey estimated that 1.69 to 1.80 million Congolese women had been raped in their lifetime and 407,397 to 433,785 women reported having been raped over the preceding 12 months (Peterman, Palermo, & Bredenkamp, 2011). A 2010 cross-sectional, population-based cluster survey in Eastern DRC, estimated that 39.7% of women and 23.6% of men had lifetime experiences of sexual violence (Johnson et al., 2010). Thus, despite international recognition of the problem, levels of sexual and gender-based violence (SGBV) in Eastern DRC remain higher than ever.
In 2002, Human Rights Watch reported that sexual violence was being used as a weapon of war in Eastern DRC (Human Rights Watch, 2002) to destabilize, to dominate and to destroy entire communities as various armed actors struggle for political advantage and for control over the region’s economic resources. This finding supports the “strategic rape theory” that has been put forward by a number of academics. This theory proposes that SGBV is used as a deliberate tool within conflict to help armed groups achieve their objectives, which can include terrorizing civilians, curtailing movement and economic activity, stigmatizing women, undermining community and family cohesion, and in some cases, deliberately polluting the bloodlines of victimized populations (Allen 1996; Card, 1996; Eriksson, Wallensteen, & Sollenberg, 2003; Gingerich & Leaning, 2004; Olujic, 1998).
At the height of the “Second Congo War,” there were as many as 20 armed groups in Eastern DRC and it has previously been documented that “all warring parties” were known to rape civilian women (Medécins Sans Frontières, 2004; United Nations, 2008). Despite a series of international and national peace agreements in late 2002 and early 2003, the violence and insecurity are ongoing in Eastern DRC and armed actors continue to be implicated in the sexual violence. However, the insecurity and logistical challenges of working in Eastern DRC have made it difficult to collect rigorous data regarding sexual violence in the region and detailed information on the types of perpetrators and on their patterns of attack are lacking.
In Eastern DRC, militias operate with scant resources, low-tech weaponry and limited access to arms. In this setting, rape is an ideal weapon. Additionally, many armed combatants in Eastern DRC are unpaid and poorly supplied with food and clothing. As a result, they rely on pillaging of local villages to meet these material demands. This requisite pillaging is at least partially responsible for bringing the militias in direct contact with civilians. In Eastern DRC, military rape may also be tolerated because commanders and combatants are poorly trained and have little exposure to or knowledge of international humanitarian law. This observation is not to imply that an awareness of the law would guarantee compliance, since the militias in question are notoriously undisciplined and much effort at the level of the command structure would need to be exerted to bring these forces into line with accepted standards of military behavior in war.
The academic and humanitarian communities acknowledge that to understand rape in war, it is necessary to understand more about patterns of perpetration (Gottschall, 2004). In his 1-year follow up report on UN Security Council Resolution 1820, UN secretary general Ban Ki-Moon noted the importance of analyzing the trends of sexual violence in armed conflict, calling for more and better data to understand the profiles and manifestations of sexual violence in individual settings, including a better understanding of perpetrators of sexual violence (United Nations, 2008).
Data about patterns of perpetration can inform protection, prevention, and security strategies in DRC. The 2009 Comprehensive Strategy on Combating Sexual Violence in the DRC called for the collection and analysis of data on sexual violence with the goal of understanding the dynamics and offering insight into the most effective responses (United Nations, 2009). Furthermore, in 2010, the United Nations Organization Mission in the DRC (MONUC), the largest peacekeeping force in the world, extended its 1999 peacekeeping mandate in DRC (United Nations Security Council, 2010). The 2010 mandate, Security Resolution 1925, notes significant security challenges in the Kivu provinces due to the presence of armed groups and the need for effective State authority (United Nations Security Council, 2010). Understanding patterns of perpetration and attack could be used to inform important protection strategies in DRC.
This study uses patient charts from Panzi Hospital in Bukavu, South Kivu Province to analyze patterns of attack as reported by women presenting to Panzi Hospital. Panzi Hospital is a full service hospital offering obstetrics and gynecology, pediatrics, internal medicine, surgery, dentistry and nutrition services. Panzi Hospital has a long history of serving the needs of women affected by the war in Eastern DRC and in recent years, it has become recognized for its care of sexual violence survivors. The hospital’s Victims of Sexual Violence Program, which receives approximately 10 sexual assault survivors daily (D. Mukwege, personal communication, Panzi Hospi, November, 2007), provides free medical treatment and free psychosocial care to sexual violence survivors.
Method
Trained female health care providers privately interviewed women who presented to hospital requesting postsexual assault services between 2004 and 2008. Individuals were chosen for interview based on staff availability and perceived level of trauma. In this sample of sexual violence survivors, the mean age was 35 years. Most women were married (53%), self-identified with the Bashi tribe (65%), were illiterate (59%) and reported agriculture as their livelihood (74%). A semistructured questionnaire collected basic demographic information, asked several directed questions about the sexual assault (including the date, time of day, and location of the assault as well as the number of perpetrators) and then allowed the patient to describe her sexual assault in an open format. Study investigators later coded the type of sexual violence by reading the self-reported narratives and categorizing the assault as either gang rape, sexual slavery, single perpetrator rape or “other rape.” For our study purposes, “gang rape” represented any act of sexual violence committed by two or more assailants. “Sexual slavery” was defined as being held captive for the purpose of sexual violence for more than 24 hours. “Single perpetrator rape” was taken to be sexual violence committed by a single assailant and not involving sexual slavery. Other types of sexual violence were infrequently reported and these were therefore grouped together. This category, “Other rape,” includes forced rape between victims, rape in the presence of family members, being forced to undress, and sexual harassment as well as those assaults that were described only as “other.”
Sexual assault records were reviewed between November 2007 and April 2009. A single sexual violence experience was extracted from each of the 4,311 reviewed records and this was the most recent sexual assault prompting the woman to seek services at Panzi Hospital. The records described here represent all the data collected under the Victims of Sexual Violence Program at Panzi Hospital from 2004 to 2008. In the same 5-year period, another 4,709 women accessed postsexual violence services at Panzi Hospital. However, because of sporadically insufficient staffing, these sexual violence survivors did not undergo the in-depth interview and details of their sexual assaults were not captured.
Quality assurance checks were performed by having a second investigator review the data extraction and type of sexual violence coding. Discrepancies were resolved by joint discussion. The data were then translated from French to English and entered into an electronic spreadsheet (Microsoft Excel 2004; Version 11.5.5). Panzi Hospital staff members were available as needed to clarify any translation questions and to provide cultural context. Quantitative analysis was performed using STATA (Statistical Software: Release 10.0. College Station, TX: Stata Corporation). This study was approved by the Institutional Review Board at the Harvard School of Public Health and by the medical director at Panzi Hospital.
Perpetrators were classified into three categories: (a) “Civilian” refers to perpetrators who were clearly identified by the survivor as noncombatants according to their dress (wearing civilian clothes), by their familiarity to the survivor (boy next door) or by their role within society (driver, vendor in the market); (b) “Armed combatants” refers to perpetrators who were described as soldiers or assailants in military uniform without specifying any particular military affiliation and also to those perpetrators who were identified as belonging to a specific military group; and (c) “Nonspecified” refers to those perpetrators simply identified as being assailants without providing any further identifying information. Each sexual assault had only one perpetrator code even though there may have been a group of perpetrators (example: a group of Mai Mai perpetrators would have had a single perpetrator code of Mai Mai). Additionally, there were no mixed perpetrators described in the registry (example: civilian perpetrator and FDLR perpetrator implicated in the same rape) thus each perpetrator code is exclusive. Reporting the identities of military groups responsible for mass rape when those groups are still active, may place the women of South Kivu at risk of retaliatory attacks. For this reason, we feel it most appropriate to report perpetrators as armed combatant, civilian, or not specified without identifying military affiliations
Results
A total of 4,311 records of female sexual violence survivors were reviewed and analyzed. Detailed demographics of the sexual violence survivors presenting to Panzi Hospital between 2004 and 2008 have been published elsewhere (Bartels, VanRooyen, Leaning, Scott, & Kelly, 2010).
Perpetrators
In this dataset, 6% of perpetrators were classified as civilians. Another 42% were described as “assailant(s)” and no further identifying information could be gathered. Twenty-four percent of assailants were described as being either “soldiers” or “men in military uniform” without identifying any particular military affiliation. Twenty-eight percent of perpetrators were identified as belonging to a specific military group. Combining the 24% of assailants without a particular military affiliation with the 28% that had a specific military affiliation, 52% of the perpetrators were identified as being armed combatants. Within this dataset, named military affiliations included Interahamwe, Hutu soldiers, Forces Armées de la République Démocratique du Congo (FARDC), Mai Mai, Nkunda soldiers, Congolese soldiers, Tutsi soldiers, Soldats de 106, Rwandan soldiers, Forces pour la Défense de la Démocratie (FDD), Rassemblement Congolais pour la Démocratie (RCD), Mudundu 40, Mutebutsi, and Rasta.
After the initial analysis, we hypothesized that many of the perpetrators in the “nonspecified” category were indeed armed combatants and we therefore performed additional analyses to compare the patterns of sexual violence committed by “nonspecified” perpetrators with patterns committed by military and civilian perpetrators. As shown in Figure 1, there were remarkable similarities between armed combatants and nonspecified perpetrators in terms of type of violence committed. Armed combatants were still the most common perpetrators for all types of sexual violence and civilian assailants were the least common perpetrators regardless of the type of sexual violence. Figure 2 illustrates that nonspecified perpetrators were much more similar to armed combatants than they were to civilian perpetrators with regards to location of attack. Figure 2 also illustrates that armed combatants were much more likely to attack in the forest.
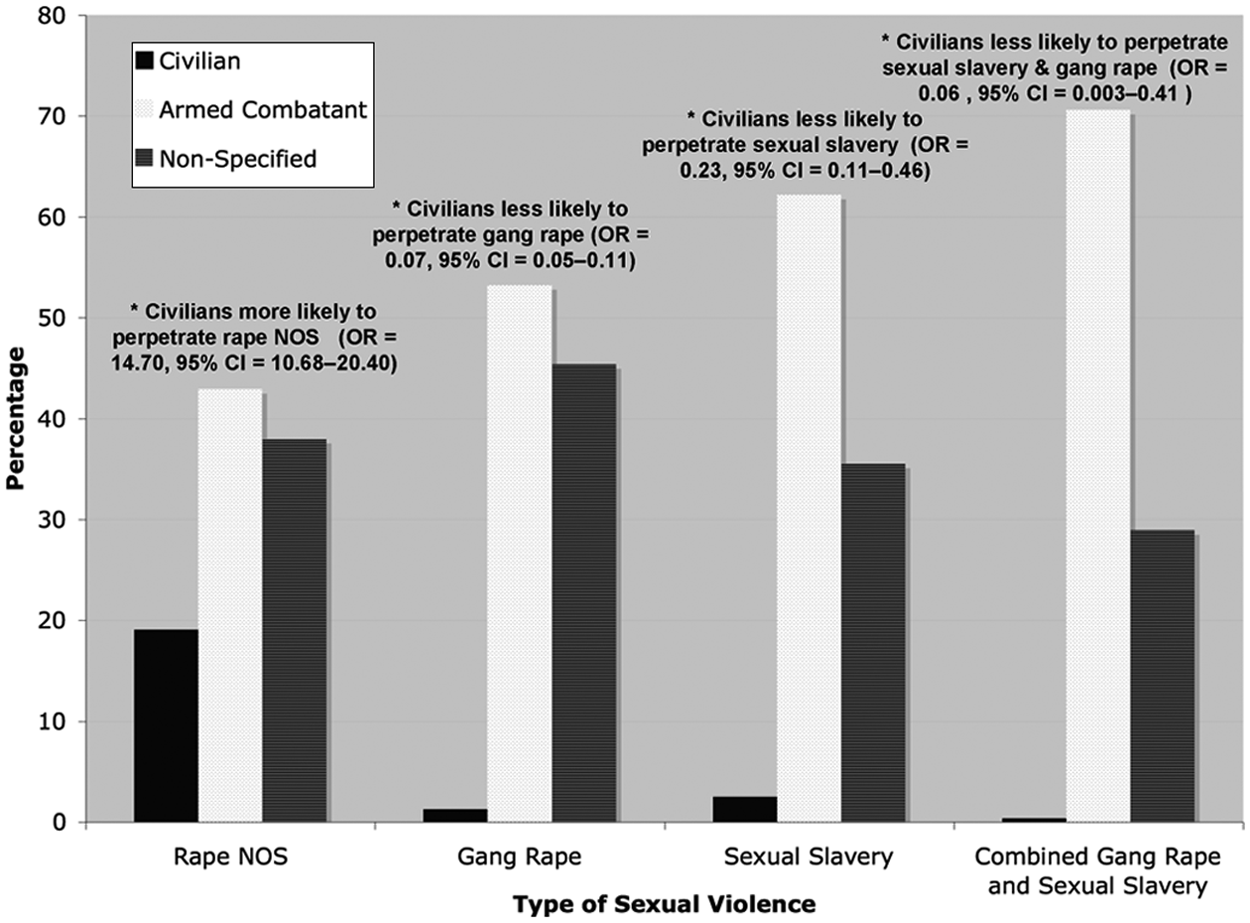
Type of sexual violence by perpetrator
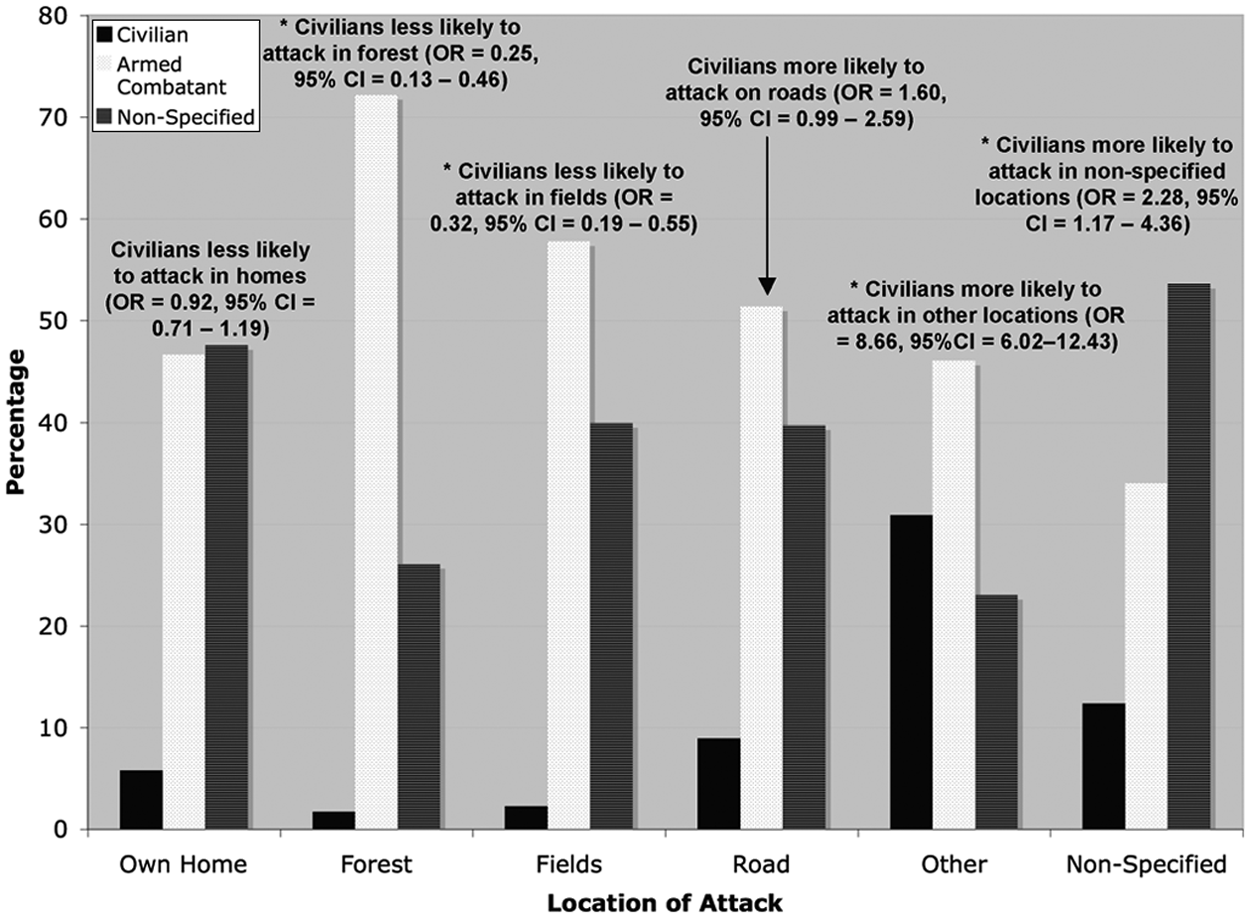
Locations of attacks by various perpetrators
Attack Characteristics
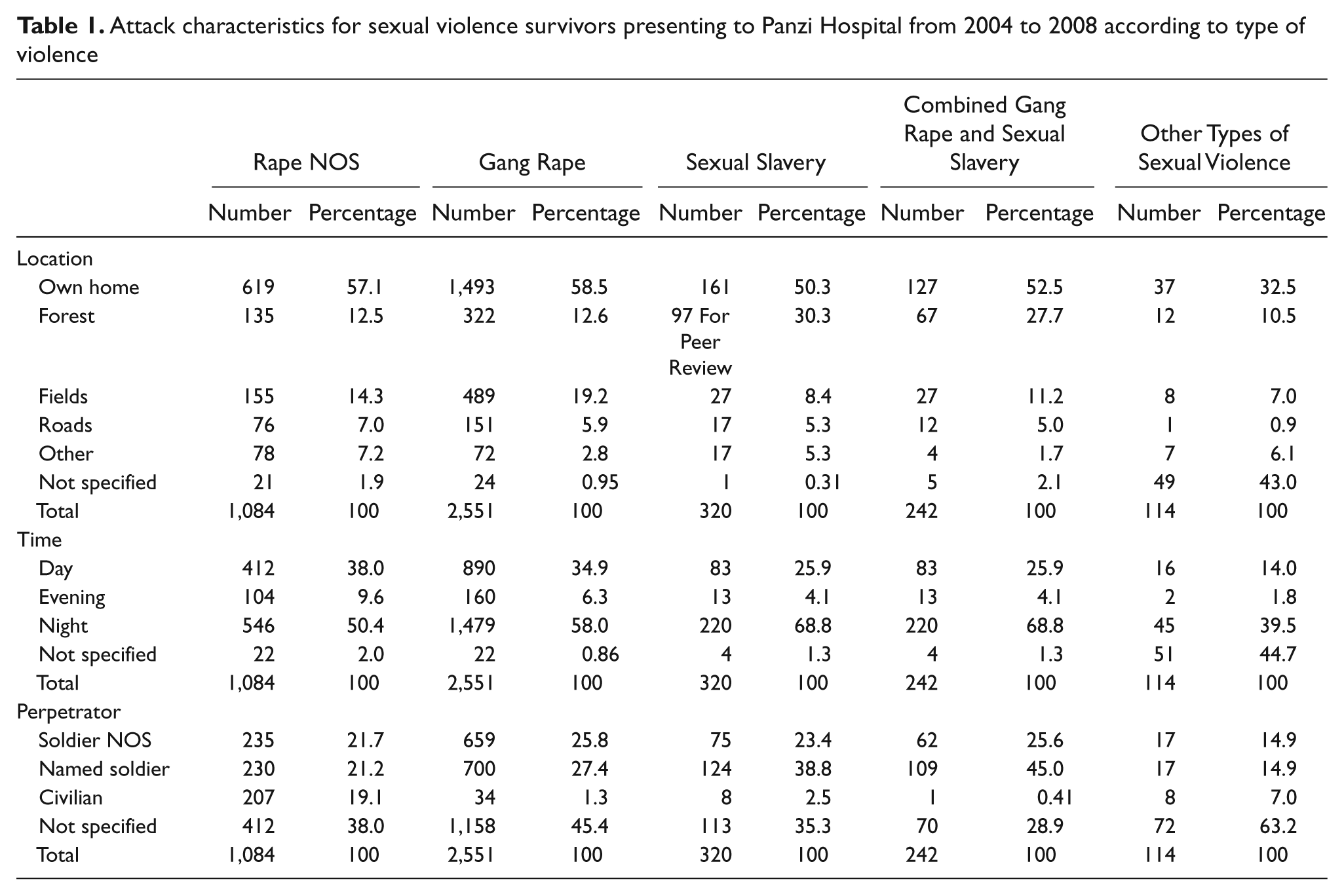
Details of attack characteristics disaggregated by type of sexual assault are provided in Table 1. Overall, gang rape comprised the majority of the sexual assaults (59.2%). The mean number of assailants per sexual assault was 2.5 with a median of 2 and a range of 1 to greater than 20 assailants. Within the collective category of “other” sexual assaults, there were 4 assaults that included forced rape between victims, 24 assaults that involved rape in the presence of family members, 8 assaults that included being forced to undress, 6 assaults that involved sexual harassment and 72 assaults that were described only as “other” by the interviewer. Most sexual assaults were initiated in the woman’s own home (56.5%), in the fields (16.4%) or in the forest (14.7%) and 57% of attacks occurred at night.
Attack characteristics for sexual violence survivors presenting to Panzi Hospital from 2004 to 2008 according to type of violence
The behaviors of civilian perpetrators were notably different from those of armed combatants and nonspecified perpetrators, giving rise to a distinct pattern of civilian perpetrated rape. As shown in Figure 1, civilian perpetrators were much more likely to commit single perpetrator rape than were other perpetrators (OR = 14.70, 95% CI = [10.68, 20.40]) and civilians were much less likely to commit sexual slavery (OR = 0.23, 95% CI = [0.11, 0.46]), gang rape (OR = 0.07, 95% CI = [0.05, 0.11]) or combined gang rape and sexual slavery (OR = 0.06, 95% CI = [0.003, 0.41]). The locations of attack by civilian perpetrators were also distinct from all other perpetrators. As illustrated in Figure 2, civilian perpetrators were much more likely to attack in “other locations” (OR = 8.56, 95% CI = [6.02, 12.43) such as private residences other than the victim’s (often the assailant’s residence), the market area and public buildings including hospitals, shops and offices. Civilian perpetrators were also much less likely to attack in the forest (OR = 0.25, 95% CI = [0.13, 0.46) or in the fields (OR = 0.32, 95% CI = [0.19, 0.55]. Civilians were also more likely to attack in nonspecified locations (OR = 2.28, 95% CI = [1.17, 4.36]). Collectively, these differences give rise to a distinct pattern of civilian perpetrated rape.
Discussion
We reviewed patient records from 4,311 sexual violence survivors presenting to Panzi Hospital between 2004 and 2008, to analyze the patterns of sexual assault in South Kivu Province. This analysis revealed that the majority of sexual assaults are perpetrated by armed combatants and that armed combatants and civilians perpetrate distinctly different types of assaults.
Military Perpetrators
Collectively, our data suggest that in South Kivu, armed combatants have been responsible for the majority of sexual assaults. To try to specify responsibility more precisely, however, is very difficult. There are, and have been, many armed groups operating within the region during the time frame covered by this study. Indeed, in the current study, women named a multitude of military groups as perpetrators. Reporting the identities of military groups responsible for mass rape when those groups are still active, may place the women of South Kivu at risk of retaliatory attacks. For this reason, we feel it most appropriate to report perpetrators as armed combatant, civilian, or not specified without identifying military affiliations.
Both national and foreign-armed groups were described as perpetrators in the narratives. The pattern of military perpetration illustrated in the hospital records supports the UN assessment that one of the primary security challenges in the Kivu provinces is the continued presence of armed groups (United Nations, 2010). UN Security Resolution 1925 highlights the urgency of comprehensive security sector reform to include the disarmament, demobilization and reintegration (DDR) of Congolese armed groups and the disarmament, demobilization, repatriation, resettlement, and reintegration (DDRRR) of foreign armed groups (United Nations, 2010). The Comprehensive Strategy also calls for security sector reform to include military justice, demobilization and disengagement of armed groups, and reform of the Congolese Armed Forces, the FARDCU (United Nations, 2009). Knowledge of perpetrators and patterns is critical for the development and implementation of protection and security strategies.
Patterns of Military Rape
One striking feature of rape in South Kivu is the high prevalence of gang rape, which was reported by almost 60% of all sexual violence survivors presenting to Panzi Hospital. Armed combatants were responsible for most of the gang rape with only 1% of such rapes reportedly committed by civilians. A theme of gang rape also resonates from the narratives where descriptions of women being encircled by a group of men and then attacked are common. Some narratives provide detail about women being restrained by a group of men who each take turns assaulting the victim. More often, however, narratives simply state, “. . . then they took turns raping me.” This high prevalence of gang rape is significant since the odds of contracting sexually transmitted infections (STIs) or HIV naturally increase as the number of assailants increases, as does the chance of becoming pregnant. Similarly, we believe that the risk of serious physical injury likely increases with multiple assailants and that women are probably at higher risk for genital trauma, fistulas and bodily injury as a result. Such a high proportion of gang rape speaks to the widespread acceptability of sexual violence among armed combatants in South Kivu.
The majority of attacks described in this dataset occurred in the woman’s own home, often at night and usually perpetrated by armed combatants. This information is critical for the development and implementation of successful protection programs. Protection of women and girls during conflict has become a priority within the international community, particularly since the United Nations (UN) Security Council passed Resolution 1820 in June 2008, which recognized that sexual violence is often deployed as a military tactic and called for a more nuanced strategy for prevention and response (United Nations Security Council, 2008). Knowing that the majority of attacks are on individual homes at night, aid organizations need to collaborate with local communities and devise new protection interventions specific for South Kivu. For instance, firewood patrols, which have been used to protect women from rape in other conflict settings (Patrick, 2007), may have limited utility in decreasing rates of sexual violence in South Kivu, where most attacks occur on individual houses. By engaging with local community members, the UN and other aid organizations need to identify new and innovative protection programs based on the patterns of attack that are most prevalent in the region.
The narrative accounts of sexual violence survivors also highlight the extreme brutality of assaults committed by armed combatants in South Kivu. Women describe genital mutilation, instrumentation with sticks and weapons, forced rape between victims while held at gunpoint, and family members being forced to witness rape. In addition to the rape of young girls and elderly women, the atrocities perpetrated by armed combatants also include rape of women in the advanced stages of pregnancy, rape of disabled women and rape of hospitalized patients recovering from recent surgery. But the brutality extends beyond the sexual violence itself. Women also describe forced cannibalism, being forced to drink bodily fluids such as urine, the slaughter of infants and young children in front of their mothers and the burning alive of family members. Armed combatants perpetrated an overwhelming majority of these extremely violent and cruel assaults. A trend of looting and rape was also clearly noted throughout the narratives with many sexual assault descriptions beginning or incorporating phrases such as “. . . they came to pillage . . .” These ruthless attacks indicate that this is not rape for the sake of rape; instead these acts are meant to terrorize and intimidate an entire population. The shame and humiliation inflicted by these crimes is intended to prohibit recovery and reintegration into society, and to thereby destroy the victims’ families and communities (Gingerich and Leaning, 2004; Réseau des Femmes pour un Développement Associatif et al., 2005; Swiss & Giller, 1993).
Our data demonstrate that the majority of sexual assaults reported to Panzi Hospital between 2004 and 2008 were perpetrated by armed combatants. To this end, protection strategies must focus on armed combatants and might include military training on human rights and international humanitarian law, the reinstatement of military command and control, ensuring that military personnel are paid regularly and provided with sufficient food and lodging, and finally holding accountable, both soldiers who commit as well as commanders who condone, acts of sexual violence (Mosely, Cetinoglu, & Glad, 2010).
To protect women from civilian perpetrated rape in Eastern DRC, the environment of impunity must also end. At the national level, sexual violence laws need to be fully enforced and the process for seeking justice needs to be simplified and accessible for survivors. It will also be important to create the capacity to investigate and prosecute crimes against women within Eastern DRC, including the incorporation of trained female officers into investigation teams. The patterns of attack described in these hospital reports could be used to inform the prevention and protection components described in the Comprehensive Strategy, which include reducing vulnerability and exposure to sexual violence and creating a protective environment (United Nations, 2009).
Limitations
This study has a number of limitations. First, because the data are retrospective we could not clarify data inconsistencies or complete missing information. The original data and the manner in which it was collected also cannot be verified or validated. Additionally, it is impossible to make causal claims due to the retrospective nature of the data. Second, this study was limited by its sampling methodology. Our data represent only those sexual violence survivors presenting to Panzi Hospital for postsexual violence care, thereby creating an inherent selection bias. It is possible that women with more severe trauma and women who were raped by armed combatants were more likely to present to medical care. As a result, the proportion of military perpetrators may be overestimated from this hospital-based registry. The sampling within Panzi Hospital was also a limitation. The Victims of Sexual Violence Program was sporadically understaffed, so at times there were an insufficient number of trained staff to interview all presenting survivors. During these times of understaffing, the interviewers chose to interview those women whom they believed to have experienced the most traumatic violence based on their interactions during the triage process. These staffing gaps appeared to have arisen sporadically. It is possible that the sexual violence survivors in this dataset do represent those who have experienced the most severe violence. However, we believe that it would be difficult to determine during the brief triage period which women had suffered the most severe trauma. A third limitation of this study was the open, self-reporting format. Without asking more direct questions on the types of perpetrators, types of sexual violence and other assault characteristics, there were inevitable gaps in the dataset. And finally, the French to English translations that were required prior to analysis, have the potential to introduce errors.
Conclusions
With a modern day shift from nation-state conflicts to intrastate civil wars has come a fundamental change in sexual violence as a weapon of war. In Eastern DRC for instance, as in other contemporary conflicts, sexual violence is employed as a weapon of war because it is inexpensive and readily available, but still extremely effective. Features of the conflict in Eastern DRC have also contributed to the widespread use of sexual violence. With the exception of the Mai Mai group, which was ostensibly formed as a local defense militia, armed military groups in Eastern DRC have been largely unopposed; community members have not taken up arms to defend themselves and efforts of the Congolese national army have been weak and scattered. Indeed, forces that have been formed to protect the local population, like the Mai Mai and the national army, have been implicated as some of the worst perpetrators of sexual violence and other human rights abuses. In battles between the various armed groups, civilians have been the undisputed victims, regardless of the intended military target. In many ways, the current war in Eastern DRC has been a proxy war with the armed militias directing their violence on civilian populations rather than on other military groups.
Collectively, our data lead us to conclude that an extraordinarily high proportion of sexual assaults in South Kivu are perpetrated by armed military and supports the theory that rape in Eastern DRC is driven by the conflict. Many women were attacked in their own homes (56%) and at night (57%), which has important implications for protection. Protection of women in South Kivu will require new strategies and innovations since many of the protection interventions used in other environments will be less effective in this setting. By engaging with local community members, the UN and other aid organizations need to identify new protection programs based on the patterns of attack that are most prevalent in the region.
Footnotes
Acknowledgements
The authors would like to thank the staff of Panzi hospital, who provide frontline care to survivors of sexual violence. Without their hard work and dedication, the Victims of Sexual Violence Program and the assistance it provides to sexual violence survivors would not be possible. They are indebted to Oxfam America who generously supported this research. Thank you to their local data entry personnel and to PMU InterLife (The Swedish Pentecostal Mission Relief and Development Cooperation Agency). PMU InterLife funds the Victims of Sexual Violence Program at Panzi Hospital.
Acronyms
DDR = Disarmament, Demobilization and Reintegration
DDRRR = Disarmament, Demobilization, Repatriation, Resettlement, and Reintegration
DRC = Democratic Republic of Congo
FARDC = Forces Armées de la République Démocratique du Congo
FDD = Forces pour la Défense de la Démocratie
NOS = Not Otherwise Specified
OR = Odds Ratio
RCD = Rassemblement Congolais pour la Démocratie
SGBV = Sexual and Gender-Based Violence
STI = Sexually Transmitted Infection
UN = United Nations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Oxfam America.
Bios