
Abstract
There is increasing recognition that chronic pain is a problem affecting women survivors of intimate partner violence (IPV), and in Western literature evidence is emerging about significant factors mediating the relationship between IPV and chronic pain. However, little is known about the factors mediating IPV and chronic pain in Chinese women for whom prior research has shown that Chinese culture may influence their response to IPV. This study was conducted to assess the roles of posttraumatic stress disorder (PTSD) symptoms, depressive symptoms, and IPV-related injury on the relationship between IPV and chronic pain in Chinese women, using structural equation modelling (SEM). Data were collected from 308 Chinese women survivors of IPV recruited at community setting (n = 228) and at domestic violence shelters (n = 82). Results showed that only the relationship between psychological abuse severity and chronic pain severity was mediated by PTSD symptom severity (β = .30, 95% CI = 0.14-0.45, p < .001). Furthermore, although depressive symptom severity was strongly correlated with PTSD symptom severity (β = .69, 95% CI = 0.61-0.76, p < .001), it was not found to be mediating the relationship between any types of IPV and chronic pain. Similarly, IPV-related injury severity was not shown to have a significant mediating effect on the relationship between IPV and chronic pain. The findings affirm the importance of recognizing the complex interrelationships among IPV, mental health symptoms, and physical health problems as well as the need for considering PTSD symptoms when designing interventions for abused Chinese women with complaints of chronic pain.
Introduction
There is overwhelming evidence that intimate partner violence (IPV) is a major contributor to the ill-health of its women survivors. For example, an extensive review of the literature found that IPV posed a significant risk to women’s physical health, including increased mortality, injury, disability, chronic pain, substance abuse, reproductive disorders, and poorer pregnancy outcomes (Plichta, 2004). In this regard, the World Health Organization conducted a multicountry study on women’s health and domestic violence involving 15 sites in 10 countries and 24,000 women. Pooled analysis found significant associations between lifetime experiences of partner violence and self-reported poor health (Ellsberg, Jansen, Heise, Watts, & Garcia-Moreno, 2008). Among the health problems reported, chronic pain as a serious long-term health consequence of IPV is well documented in Western literature. For instance, in several large controlled studies, it was found that women who have experienced IPV have higher rates of chronic pain than nonabused women (Campbell et al., 2002; Coker, Smith, Bethea, King, & McKeown, 2000; Plichta, 2004). Similarly, chronic pain-related disabilities were more likely to be reported by abused women than nonabused women (Coker, Weston, Creson, Justice, & Blakene, 2005; Weinbaum et al., 2001). Also, women with a history of IPV and chronic pain have been found to have increased anxiety disorder rates (Scarinci, McDonald-Haile, Bradley, & Richter, 1994), depression (Koopman et al., 2007), and substance use (Green, Flowe-Valencia, Rosenblum, & Tait, 1999). As such, chronic pain is not only a problem that impacts negatively on the health and well-being of women survivors of IPV, it also adversely affects their ability to cope by limiting their capacity to care for themselves and their children, interfering with their ability to sustain employment, and hindering their efforts to strive for independence.
Despite recognition that chronic pain is a health problem affecting abused women, information about the significant mediators affecting the relationship between IPV and chronic pain is limited. Such information is important for identifying vulnerable individuals and initiating appropriate interventions in a timely manner. More recently, Wuest and colleagues (2009) have advanced the knowledge of chronic pain in women survivors of IPV through their use of structural equation modeling (SEM) to test a theoretical model of the relationships among key variables. Specifically, lifetime abuse-related injury and posttraumatic stress disorder (PTSD) symptom severity were found to be significant mediators of the effects of both assaultive IPV severity (i.e., physical and sexual battering) and past child abuse severity on chronic pain severity. Despite the link identified between assaultive IPV severity and PTSD severity, Wuest et al. did not find psychological IPV severity to have a significant direct effect on PTSD severity: They speculated that this could be due to the failure of including certain salient mediators in the model. Depression may be one of the missing salient factors in Wuest’s model as it is known to affect chronic pain (Demyttenaere et al., 2006).
The objective of the present study was to assess the relationship between IPV and chronic pain in Chinese women with a specific focus on the mediating roles of PTSD symptoms, depressive symptoms, and IPV-related injury. Despite the emerging evidence suggesting a complex interplay of IPV, mental health symptoms, and physical health problems in Western literature (Carlson, 2005; Green & Kimberling, 2004; Wuest et al., 2009), no study has explored the multivariate relationships among the factors mediating IPV and chronic pain in Chinese women. As previous studies have suggested that Chinese culture may influence women’s response to IPV (Tiwari et al., 2009), generalizability of the findings of Western studies to abused Chinese women cannot be assumed. IPV perpetration against Chinese women should also be viewed within a cultural context to provide a better understanding of and advance theories about how these women respond to their partner’s violence compared to those in Western societies. As shown in studies investigating dating violence, it is possible to provide valid cross-national comparisons by studying the results from different countries (Gover, Park, Tomsich, & Jennings, 2011; Straus, 2004, 2008, 2009). It is intended that this study would provide beginning evidence of women’s response to IPV within the Chinese cultural context. The present study therefore tested a model of the relationship between IPV and chronic pain in Chinese women and the extent to which PTSD symptoms, depressive symptoms, and IPV-related injury mediated the relationship.
The Hypothesized Model
The hypothesized model for assessing how PTSD symptoms, depressive symptoms, and IPV-related injury mediated the relationship between IPV and chronic pain in this study is depicted in Figure 1. It is based on an integrated model of mechanisms linking trauma to health (Schnurr & Green, 2004). Specifically, exposure to trauma (including IPV) is theorized to result in a distress response that precipitates changes in health status, including chronic pain. Components of the model include trauma exposure (such as different types of IPV victimization, including physical assault, psychological abuse, and sexual coercion), psychological mechanisms (such as PTSD and depressive symptoms), and physical health outcomes (such as chronic pain).

The hypothesized model examined in the present study
As described above, higher rates of chronic pain (Campbell et al., 2002; Coker et al., 2000) and disability related to chronic pain (Coker et al., 2005; Weinbaum et al., 2001) have been documented in women survivors of IPV compared to nonabused women. Assaultive IPV severity was also shown to have a significant indirect effect on chronic pain severity, whereas psychological IPV severity had a significant direct effect (Wuest et al., 2009). Similarly, lifetime physical assault and/or sexual coercion have been associated with gastrointestinal and pelvic pain (Leserman & Drossman, 2007; Leserman, Zolnoun, Meltzer-Brody, Lamvu, & Steege, 2006).
Women who are physically assaulted by their intimate partners are also likely to suffer injuries (Tjaden & Thoennes, 2000). Persistent, inadequately treated acute pain from such injuries, even minor ones (Carr & Goudas, 1999), can lead to hyperresponsiveness and dysregulation of pain inhibitory mechanisms (Martelli, Zaster, Bender, & Nicholson, 2004), which can progress into chronic pain. In addition, chronic pain can occur in the absence of injury and is thought to be an outcome of a complex biopsychosocial stress response (Chapman, Tuckett, & Song, 2008) related to dysregulation of chemical mediators (MacEwan, 2007). Thus, it is probable that the stressors associated with IPV may overwhelm stress-regulation systems in the body and result in chronic pain.
PTSD, a distress reaction that develops as a result of exposure to IPV, has frequently been suggested to mediate the relationship between trauma exposure (such as IPV) and health outcomes (such as chronic pain; Green & Kimberling, 2004). Chronic pain that is associated with PTSD is also likely to be more intense, distressing, and debilitating than chronic pain that is not associated with PTSD (Woods et al., 2005). Furthermore, Wuest and colleagues (2009) found that the relationship between assaultive IPV severity and chronic pain severity was significantly mediated by PTSD symptom severity. It has also been suggested that PTSD substantially changes trauma survivors’ psychological and internal physiological functioning and that such changes are associated with physical health symptoms (including chronic pain) and psychological health symptoms (including depression; Schnurr & Green, 2004).
Despite the close link between PTSD and depressive symptoms, and that they are both frequent outcomes of IPV, only two studies have included both of these symptoms when examining the relationships between IPV and chronic pain. In the studies conducted by Wuest et al. (2008) and Humphreys et al. (Humphreys, Cooper, & Miaskowski, 2010), bivariate associations among IPV, chronic pain, PTSD, and depressive symptoms were found. However, the complex and multiple-determined phenomena cannot be adequately addressed by two-variable (bivariate) analyses. Multivariate analysis, as intended in the present study, has the capacity to deal with multiple relationships and allows simultaneous estimation of several interrelated dependence relationships (Polit & Beck, 2008).
On the basis of the literature described above, we constructed a hypothesized model (Figure 1) for multivariate analysis by linking IPV severity, IPV-related physical injury severity, PTSD symptom severity, depressive symptom severity, and chronic pain severity. Specifically, we hypothesized that the effect of IPV severity on chronic pain severity would be significantly mediated by PTSD symptom severity, depressive symptom severity, and IPV-related injury. In the present study, the hypothesized model was tested using SEM, a multivariate analysis technique, to determine how well the model can be explained by the empirical data.
Method
Design and Setting
This is a prospective, cross-sectional study. Convenience sampling was used to recruit participants from three domestic violence shelters located in different districts in Hong Kong, as well as at one community center serving three large urban areas. The three shelters represent 50% of the residential refuge for abused women in Hong Kong. Regardless of geographical location, each of the shelters admits abused women and their children from all over Hong Kong. Thus, for the present study the participants recruited from the shelters were drawn from different districts in Hong Kong. The participating community center, established in 1973, has about 30 outreach sites covering three large diverse districts serving a population of approximately 800,000. The center was chosen for this study not only because it provided a broad range of health, social, child care, educational and recreational services to users of all age groups, including abused and nonabused women in the community, it is also where the investigators have developed a long-term relationship and trust after many years of collaboration in research and service provision.
Ethical approval for conducting the study was obtained from the Institutional Review Board of the host university.
Participants
Chinese women, aged 18 or above, able to understand Cantonese or Putonghua (the two major dialects in Hong Kong), and who had been screened positive for physical, psychological, or sexual abuse by a current or former intimate partner based on the Chinese version of the Abuse Assessment Screen (C-AAS) were recruited. Those who were unable to communicate in Cantonese or Putonghua were excluded.
Sample size calculation was based on the objective of the study, which was to assess the hypothesized mediating roles of PTSD symptoms, depressive symptoms, and IPV-related injury in the relationship between IPV and chronic pain. This was accomplished by an SEM analysis for which a study sample exceeding 200 participants is generally considered as sufficient (Kline, 2005). In this study, we aimed to recruit 300 abused women, thus allowing for a small number of attrition due to incomplete questionnaires.
Procedures
The study was conducted between September 2009 and July 2010. Participants were recruited through public notices in the community center or weekly announcements during the shelters’ house meetings. Our research staff contacted those who expressed an interest to schedule face-to-face interviews.
In a private room and on her own without the presence of her partner or other family members, the potential participant was met by our research staff and given a detailed description of the study and the rights of research participants, including voluntary participation, confidentiality, and the potential benefits and risks. Those who agreed to participate were asked to provide written consent. Once consent had been given, the C-AAS was administered and those who screened negative for IPV were thanked for their interest and told that no further contact would be made. Those who screened positive for IPV were invited to continue and completed a questionnaire administered by the research staff. The questionnaire took about 30 min to complete.
Measures
Intimate partner violence
The 5-item C-AAS was used to screen potential participants for IPV. If a participant answered “yes” to having been emotionally, physically, or sexually abused in the past year, and if the perpetrator was her current or former intimate partner, she was screened positive for IPV. The C-AAS has been validated and demonstrated satisfactory measurement accuracy in detecting IPV in Chinese women (Tiwari et al., 2007).
Information relating to the types and frequency of IPV and abuse-related injury severity was collected using the Chinese version of the Revised Conflict Tactics Scales (C-CTS2; Chan, 2005). Specifically, 12 items from the Physical Assault subscale, 8 items from the Psychological Aggression subscale, 7 items from the Sexual Coercion subscale, and 6 items from the Injury subscale were used to measure intimate partner physical assault, psychological abuse, sexual coercion, and IPV-related injury, respectively. Participants were asked to report on the frequency of each of the abusive acts occurring in a partner conflict situation over the past year using a 7-point scale, with the following response options: 0 = never, 1 = once, 2 = twice, 3 = 3 to 5 times, 4 = 6 to 10 times, 5 = 11 to 20 times, and 6 = more than 20 times. The total scores for each subscale were calculated by adding up the midpoints of the response categories for each item (e.g., the midpoint for the 6 to 10 times response was 8). The Physical Assault subscale, Psychological Aggression subscale, Sexual Coercion subscale, and Injury subscale scores ranged from 0 to 300, 0 to 200, 0 to 175, and 0 to 150, respectively. The C-CTS2 was validated in a representative household survey of IPV in Hong Kong and demonstrated satisfactory validity and reliability (Chan, 2005). In this study, the Cronbach’s alpha coefficient was .87 for the Physical Assault subscale, .89 for the Psychological Aggression subscale, .73 for the Sexual Coercion subscale, and .74 for the Injury subscale.
PTSD symptom severity
The Chinese version of the Impact of Event Scale—Revised (C-IES-R; Wu & Chan, 2003) was used to evaluate the severity of PTSD symptoms. The C-IES-R is a 22-item self-report instrument that consists of 3 subscales: the Intrusion subscale (7 items), the Avoidance subscale (8 items), and the Hyperarousal subscale (7 items). Participants were asked to rate the degree of distress for each of the subscale items with respect to their abusive experience in the past 7 days on a 5-point scale ranging from 0 (not at all) to 4 (extremely). The total C-IES-R scores were calculated by adding up the responses for each of the items, resulting in a total score ranging from 0 to 88. The C-IES-R has been validated in Chinese adult samples and has yielded good sensitivity and specificity for the screening of PTSD symptoms (Wu & Chan, 2004). In this study, the Cronbach’s alpha coefficients were .97 for the Intrusion subscale, .96 for the Avoidance subscale, and .96 for the Hyperarousal subscale.
Depressive symptom severity
The severity of depressive symptoms was assessed using the Chinese version of the Patient Health Questionnaire Depression Module (PHQ9; Kroenke, Spitzer, & Williams, 2001). The Chinese PHQ9 is a self-report instrument focusing on nine core symptoms of a major depressive episode that correspond to the DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders, 4th ed., text rev., American Psychiatric Association, 2000) diagnostic criteria. Participants were asked to rate the frequency of the nine symptoms they had experienced in the previous 2 weeks on a 4-point scale from 0 (not at all) to 3 (nearly every day). The Chinese PHQ9 has been shown to have high internal consistency and good concurrent validity when previously tested in a sample of Hong Kong Chinese adolescents (Lee et al., 2008). The Cronbach’s alpha coefficient for the Chinese PHQ-9 in this study was .93.
Chronic pain severity
Participants were screened for chronic pain using a question that was developed by Elliott and colleagues (Elliott, Smith, Penny, Smith, & Chambers, 1999) to detect chronic pain in a population-based study. Those who reported pain symptoms for more than 3 months were considered to have chronic pain. In addition, chronic pain severity was assessed using the Chronic Pain Grade Questionnaire (CPG; Von Korff, Ormel, Keefe, & Dworkin, 1992). The CPG is a seven-item instrument consisting of three components: pain intensity (three items), pain-related disability (three items), and disability days due to pain (one item). Specifically, pain intensity seeks to elicit information on (a) worst pain intensity, (b) average pain intensity, and (c) present pain intensity, based on a visual rating scale ranging from 0 (no pain) to 10 (pain as bad as it could be). For pain-related disability, participants were asked to rate (a) how the pain interfered with daily activities, ranging from 0 (no interference) to 10 (unable to carry out any activity); (b) how the pain changed their ability to take part in recreational and social activities, ranging from 0 (no change) to 10 (extreme change); and (3) how the pain changed their ability to work (including housework), ranging from 0 (no change) to 10 (extreme change). To assess the number of disability days due to pain, participants were asked to count the number of days in the past 6 months when they were kept from their usual activities because of pain. The CPG is a well-established instrument used to assess the severity of chronic pain among adults in both clinical and community samples in Western populations (Elliott et al., 1999; Wuest et al., 2008). In the present study, CPG items were translated into Chinese and then back-tranlsated into English by independent bilingual professional translators. Both versions were compared by a team of bilingual clinicians, and modifications were made as required to reconcile the meaning between the original English version and the Chinese translated version. The process of modification was repeated until consensus was reached among the research team. For the present study, the Cronbach’s alpha coefficients were .90 for the pain intensity component and .97 for the pain-related disability component.
Demographic characteristics
The following demographic characteristics were collected from the participants: age, marital status, number of children, place of birth, number of years living in Hong Kong, educational level, employment status, financial hardship experienced in the past year, monthly family income, and history of physical and/or mental health problems.
Statistical Analyses
Demographic characteristics and the hypothesized model variables were first summarized using descriptive statistics. The hypothesized model was then evaluated by using SEM. Based on the covariance matrix of the variables involved, the maximum likelihood estimator implemented in the Mplus program version 5 (Muthén & Muthén, 1998-2009) was used to estimate all the standardized parameter estimates (β). As recommended by MacKinnon et al. (MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002), all the hypothesized mediating effects were evaluated using the Sobel test (1982). The chi-square statistic (χ2) and its degrees of freedom were reported. Due to the high sensitivity of χ2 to large samples, three other fit indices, the comparative fit index (CFI; Bentler, 1990), the root mean square error of approximation (RMSEA; Steiger, 1990), and the standardized root mean square residual (SRMR; Jöreskog & Sörbom, 1993), were used, in tandem, to assess the model fit. As suggested by Hu and Bentler (1999), a model can be considered adequate if the CFI > 0.95, the RMSEA < 0.06, and the SRMR < 0.08. To avoid doubts about the adequacy of the model, the addition of covariance was made based on the largest modification index (Brown, 2006). All statistical tests were performed using a 5% level of significance, and a 95% confidence interval accompanied each estimate, where appropriate.
Results
Overall, 310 abused Chinese women were recruited to the present study, of which 228 were recruited from the community center and 82 from the domestic violence shelters. Two women did not complete the questionnaire. Thus, 308 women were included in the data analysis. The women’s demographic information and their health outcomes are shown in Table 1. A correlation matrix of the major study variables is displayed in Table 2.
Women’s Demographic Information and Health Outcomes
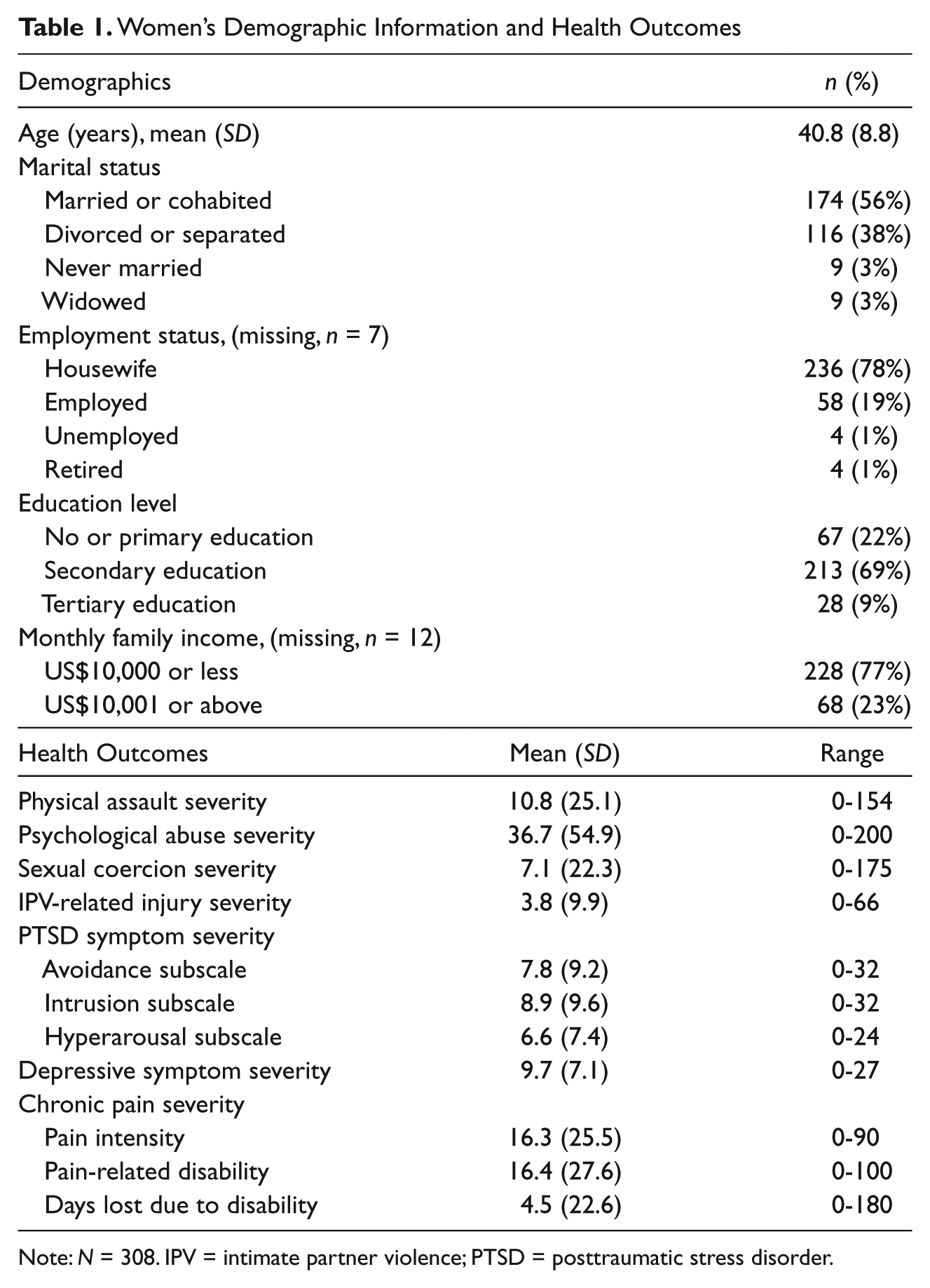
Note: N = 308. IPV = intimate partner violence; PTSD = posttraumatic stress disorder.
Correlation Matrix for the Major Study Variables
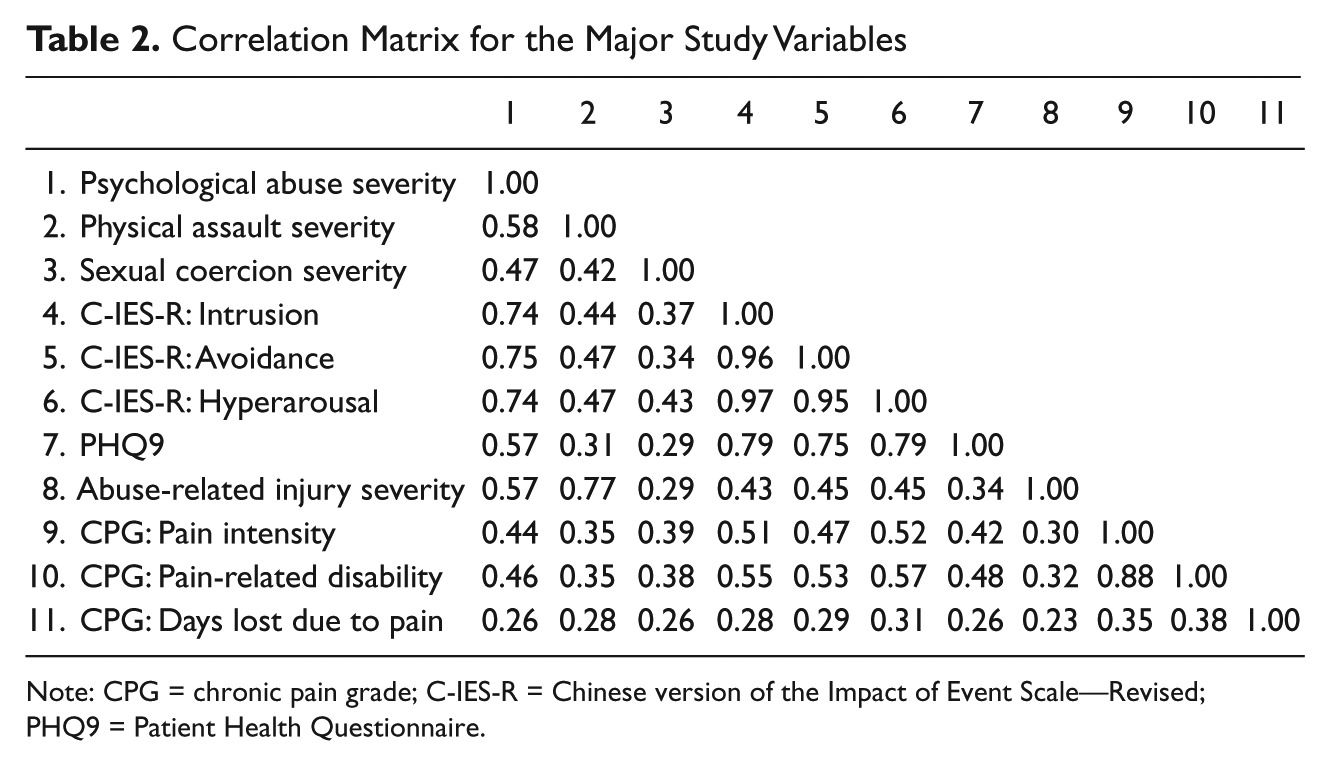
Note: CPG = chronic pain grade; C-IES-R = Chinese version of the Impact of Event Scale—Revised; PHQ9 = Patient Health Questionnaire.
When the hypothesized model was examined using SEM, fit indices showed that the model had an adequate fit to the empirical data (χ2 = 49.9, degrees of freedom = 31, p = .02, CFI = 0.99, RMSEA = 0.04, SRMR = 0.04). The parameter estimates of the model are shown in Figure 2 and Table 3.
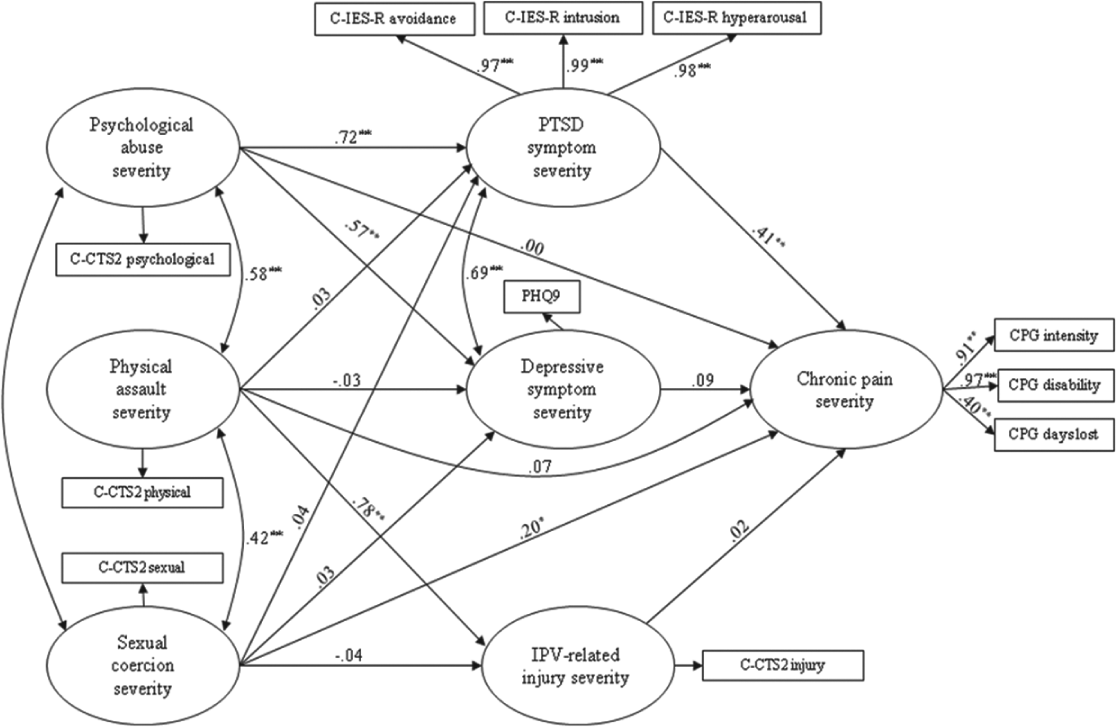
A path model illustrating the relationships among the study variables
Standardized Coefficients of the Path Model
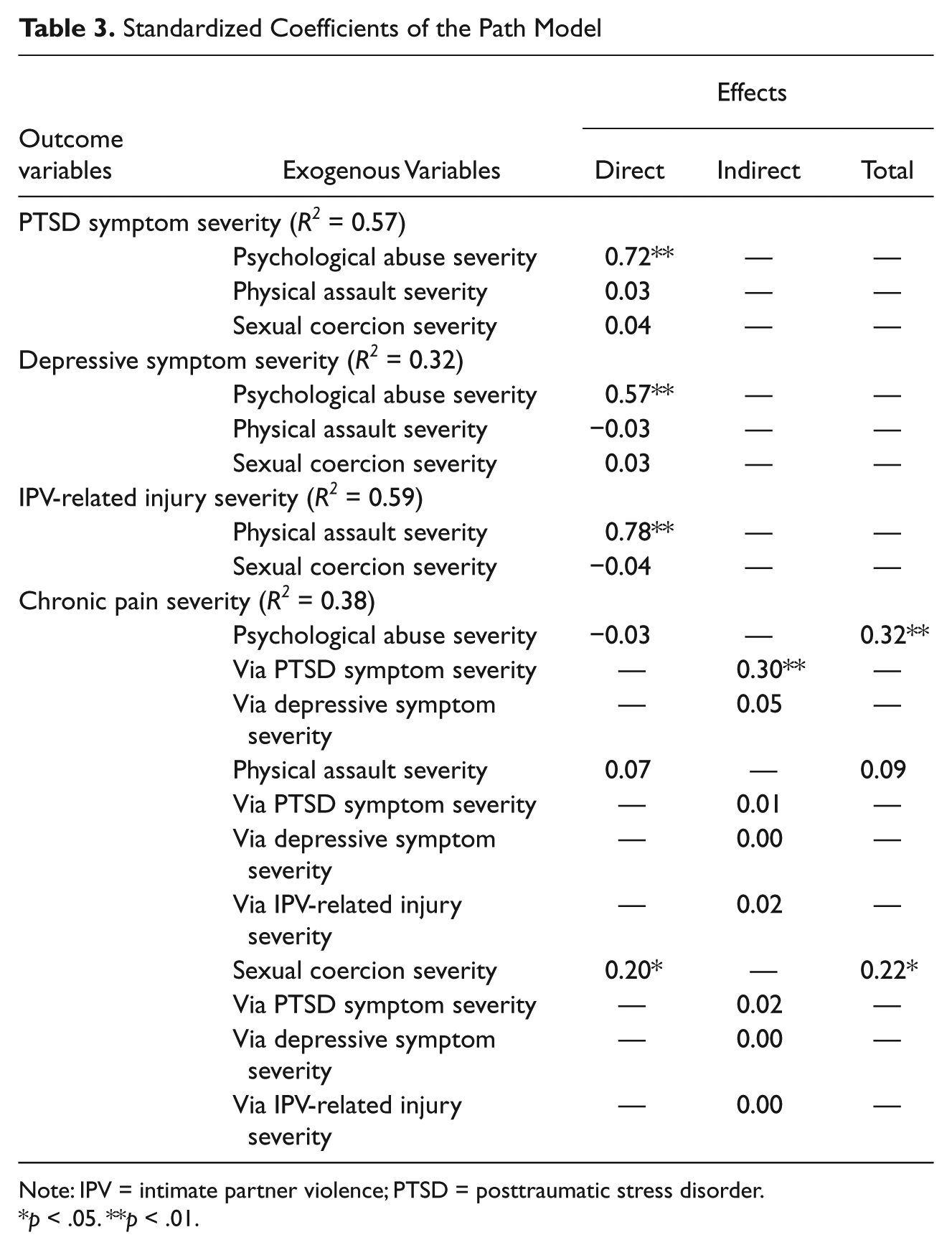
Note: IPV = intimate partner violence; PTSD = posttraumatic stress disorder.
p < .05. **p < .01.
Overall, this model accounted for 38% of the variance in chronic pain severity. As shown in Table 3, psychological abuse severity had an effect over and above sexual coercion severity and physical assault severity on chronic pain severity. Also, the effect of psychological abuse severity on chronic pain severity was significantly mediated by PTSD symptom severity (β = .30, 95% CI = 0.14-0.45, p < .001) but not by depressive symptom severity or IPV-related injury severity. Although the effect of physical assault severity on chronic pain severity was not significant, it had a significant direct effect on abuse-related injury severity (β = .78, 95% CI = 0.67-0.89, p < .001). Interestingly, IPV-related injury severity did not have a significant effect on chronic pain severity. Sexual abuse severity was found to have a significant direct effect on chronic pain severity (β = .20, 95% CI = 0.03-0.37, p < .05), but it had no significant effect on depressive symptom severity or PTSD symptom severity. Notably, psychological abuse severity had a significant direct effect on PTSD symptom severity (β = .72, 95% CI = 0.63-0.81, p < .001) and depressive symptom severity (β = .57, 95% CI = 0.45-0.69, p < .001), and depressive symptom severity was strongly correlated with PTSD symptom severity (β = .69, 95% CI = 0.61-0.76, p < .001).
Discussion
The present study found that PTSD symptom severity mediated the impact of psychological abuse severity on chronic pain severity. This is consistent with the general assertion that PTSD mediates the relationship between trauma and physical health outcome (Green & Kimberling, 2004). Furthermore, this study has shown that the trauma was in the form of psychological abuse. On the other hand, our hypothesis that the effect of IPV on chronic pain would be significantly mediated by depressive symptom severity was not supported. Despite this, since depressive symptom severity was found to be strongly correlated with PTSD symptom severity, it is probable that an increase in depressive symptoms could aggravate PTSD symptoms, which in turn could lead to worsening of chronic pain. It is, therefore, important not to overlook depressive symptoms in abused Chinese women with PTSD symptoms and/or chronic pain.
Previously, studies have shown that psychological abuse experienced by Chinese women was associated with negative mental health outcomes, including depressive symptoms (Tang, 1997), postnatal depressive symptoms (Leung, Kung, Lam, Leung, & Ho, 2002), and poor mental health-related quality of life (Tiwari et al., 2008). This study shows that psychological abuse in Chinese women was not only associated with mental health problems (depressive and PTSD symptoms) but also physical health problems (chronic pain). The findings of this study differ from that of an earlier study conducted in Canada, which showed that both lifetime abuse-related injury and PTSD symptom severity were significant mediators of the effects of physical and/or sexual IPV severity (but not psychological IPV severity) and past child abuse severity on chronic pain severity (Wuest et al., 2009). The discrepancy in findings between Wuest et al.’s and the present study may, in part, be due to cultural differences. It is possible that, in a shame-oriented culture such as the Chinese, women may be more susceptible to shameful emotions induced by psychological abuse (Tiwari et al., 2008) and the latter can therefore have a devastating effect on the victim (Bedford, 2004) with associated psychopathological problems (Tangney, Wagner, & Gramzow, 1992).
The finding in this study that PTSD symptoms mediate the effect of psychological abuse on chronic pain highlights the need for health professionals to assess for IPV and PTSD symptoms when caring for Chinese women with chronic pain. Since traditional Chinese health beliefs do not distinguish between physical and mental disorders and excessive expression of emotions is thought to be harmful to health (Lin, 1982), abused Chinese women may present with physiological symptoms rather than the emotional state associated with the mental health condition (Tang, 2007). Thus, when complaints of chronic pain are presented by abused Chinese women, assessment for PTSD symptoms should also be made. For the same reason, interventions designed to reduce chronic pain in these women should also consider PTSD symptoms. Indeed, because of the complex interrelationships among IPV, mental health problems, and physical health problems (Woods et al., 2005), interventions for survivors of IPV must adopt a holistic approach. As such, treatment of pain symptoms should go hand in hand with counseling services, safety planning, and community support for abused women.
In this study, IPV-related injury was not shown to be mediating the relationship between IPV and chronic pain. It is inconceivable that an injury does not cause pain, but the pain may not have lasted for more than 3 months for it to be identified as chronic pain. Also, as the severity of IPV-related injury reported by women in this study was relatively low (a mean score of 3.8 within a possible range of 0 to 150) and given the cross-sectional design of the study, the effect of the injury may not yet have been felt. In light of the suggestion that repeated inadequately treated injuries, even minor ones, may result in peripheral sensitization of pain pathways, which may lead to hyperresponsiveness and dysregulation of pain inhibitory mechanisms and, in turn, chronic pain (Martelli et al., 2004). IPV-related injury in abused women must be given proper attention. Specifically, health care protocols for abused women should include screening for and treatment and follow-up of IPV-related injuries to reduce the risk of chronic pain.
Notwithstanding some of the discrepancies between the findings of the present study and those conducted in Western societies as highlighted above, it is important to recognize the relationship between IPV and chronic pain that is mediated by identifiable factors. And such a relationship has been shown in studies involving Chinese women (as in the present study) and non-Chinese women (e.g., studies by Wuest et al., 2009). Previously, studies on dating violence perpetration and victimization have established that valid conclusions may be drawn from studies conducted in different nations based on the concept of national context effects (Straus, 2009). It is suggested that cross-national studies be conducted to advance the theoretical and practical bases of women’s response to IPV through multination comparative research.
Finally, the results of this study should be interpreted in light of the following limitations. The use of a convenience sample and recruitment through advertisements in the shelters and community center limit the generalizability of the findings to women outside of this population. Future studies should consider using representative samples to examine the problem of chronic pain in female survivors of IPV. In addition, the cross-sectional design does not permit an evaluation of the causal relationship among the study variables. Longitudinal studies, although notoriously difficult to conduct, are essential for verifying the causal link between IPV and chronic pain. Qualitative studies may also be conducted to explore the context within which IPV takes place so that a more comprehensive picture of the women’s experiences can be elicited and the impact of IPV on their mental and physical health better understood. As well, even though the measures used in this study yielded good reliability estimates and the utilization of individual face-to-face interviews allowed clarifications during data collection, the use of self-report measures may still be subject to bias and/or limited recall with the participants underreporting the extent of their IPV experience and/or health symptoms. Future studies might consider the use of multiple data collection methods, including the adoption of biological measures where appropriate.
Conclusion
Literature has suggested that IPV has a profound adverse impact on women’s health, and chronic pain has been identified as a sequelae. This study demonstrated the significant mediating effect of PTSD symptoms on the relationship between psychological abuse and chronic pain, thus affirming the importance of recognizing the complex interrelationships among IPV, mental health symptoms, and physical health problems as well as the need for considering PTSD symptoms when designing interventions for abused Chinese women with complaints of chronic pain.
Footnotes
Acknowledgements
The authors are indebted to the women whose valuable contributions to this study have enlightened our understanding of the complexity of IPV in general and psychological abuse in Chinese women in particular.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the University of Hong Kong, Small Project Funding (#10400657).