
Abstract
The present study investigated the impact of motivational interviewing (MI) and stage of change on a self-report measure of global functioning (Outcome Questionnaire [OQ 45.2]). Participants were men mandated to attend the Responsible Choices for Men (RCM) group therapy program following an incident of domestic violence. The study design utilized a quasi-experimental between-groups comparison utilizing data collected at three time points (pregroup, first group session, and final group session). One group of mandated program attendees received two sessions of MI (n = 106), whereas the comparison group did not (n = 106). Stage of change was assessed using the URICA-G and the URICA-DV (University of Rhode Island Change Assessment—Domestic Violence). Multilevel growth modeling indicated that stage of change has a significant relationship to global functioning. Discussion focuses on the potential benefits of MI as a pregroup treatment and the importance of accounting for individual readiness to change.
Introduction
The past 20 years has witnessed an expansion of research into the effectiveness of therapeutic programs for men who are violent in their intimate relationships. In part, this research reflects increased pressure from third-party payers and funders to examine measurable forms of improvement in therapeutic accountability and success (Duncan, Miller, Wampold, & Hubble, 2010). This involves using evidence from real-time therapy interventions to evaluate effectiveness. The results from these studies are mixed, suggesting a mitigating factor that may differentiate men who benefit from therapy and whose violence is reduced. The present investigation explored differences in self-reports of global functioning in the context of the implementation of motivational interviewing (MI) and appreciating the stage of change at which each participant was assessed prior to the implementation of therapy.
Literature Review
Nature of treatment
Group therapy is the format of choice in 90% of male domestic violence interventions (Austin & Dankwort, 1999; Gondolf, 2002), and among the most widely used models of male domestic violence group treatment is the Duluth Feminist Model (DFM; Pence & Paymar, 1993). The DFM requires men to be confronted early in the therapeutic process regarding the issues that relate to their responsibility for the violence along with an acknowledgment of a patriarchal power and control ideology (Eckhardt, Holtzworth-Munroe, Norlander, Sibley, & Cahill, 2008). Such feminist-based groups utilize narrative techniques and report encouraging rates of success (Jenkins, 1990; McGregor, Tutty, Babins-Wagner, & Gill, 2002; Tutty, Babins-Wagner, & Rothery, 2009).
Mandated treatment
Domestic violence is a criminal offence, and it is commonplace within the judicial system to impose mandatory domestic violence therapy such as DFM as a component of an individual’s probation (Canadian Centre for Justice Statistics, 2004; Hoffart & Clarke, 2004). In 2002, a probation order occurred in 72% of spousal violence charges (Canadian Centre for Justice Statistics, 2004). There has been significant interest and research on the effectiveness of mandated treatment. Whereas early studies questioned the effectiveness of mandated treatment (Chen et al., 1989; Dutton, 1986), more recently studies are noting that court-mandated men show greater gains from treatment (Bowen & Gilchrist, 2004; Hamberger & Hastings, 1986; McMurran, 2002; Scott & Wolfe, 2003).
Motivation to change
The controversy regarding mandated versus self-referred participation in domestic violence programs speaks to the level of motivation and engagement in the treatment process. Motivation is often accompanied by ambivalence (Miller & Rollnick, 1991), and with respect to therapeutic motivation, an important distinction is made between internal and external motivational factors. Whereas court mandates may be an important external motivator for clients to enter treatment, once in treatment, internal motivation can be enhanced as part of the explicit goals of the treatment program (Jaffe, Wolfe, Telford, & Austin, 1986; McMurran, 2002). Offenders who are at the highest risk for serious recidivism are viewed as the least motivated to change (McMurran, 2002). Small effect sizes seen in the male domestic abuse intervention literature may in part be attributable to the perpetrator’s lack of investment in the therapeutic process and subsequent high attrition rates from the program (Babcock et al., 2004).
The transtheoretical model (TTM) and the stages of change
TTM suggests that individuals move through a sequence of stages before they successfully establish and maintain changes in their behavior. Proschaska and Levesque (2002) and Scott (2004) summarize that individuals move through a series of stages from precontemplation, contemplation, preparation, action, and maintenance within the change process. In practice, individuals do not progress through such stages in a linear fashion but rather move forward and backward between stages through the course of their treatment. Proschaska and DiClemante’s (1982) original research with smoking cessation hypothesized the stages of change to act as a wheel or revolving door, with most individuals proceeding in a circular fashion several times before exiting from treatment. The lack of progress seen in many male domestic violence groups may be attributable to their being at an early stage of change, unwilling to “give up” their investment in the use of violence within their intimate relationships.
Initial research on TTM focused on smoking cessation and other addictive behaviors, finding promising results (Velicer, Prochaska, Fava, Laforge, & Rossi, 1999. In 2005, the Journal of Addictions Nursing dedicated a special issue to the topic of TTM with several papers outlining the success and potential within this field (DiClemante, 2005; Finnell, 2005; Nochajski & Stasiewics, 2005; Velasquez et al., 2005).
Several studies have applied TTM to male domestic violence counseling, reporting that treatment was more beneficial in reducing anger when treatment readiness was initially high (Scott & Wolfe, 2003; Williamson et al., 2003). Men in an early stage of change consistently reported fewer problems with anger and tended to downplay their abusive behavior. This is consistent with denial and minimization of the situation, rather than an accurate description and acceptance for responsibility of their behavior (Alexander & Morris, 2008). Levesque, Gelles, and Velicer (2000) found that in a sample of 292 men involved in a domestic violence counseling group, 24% were in the precontemplative stage, 63% were in the contemplation/preparation stage, and only 13% were in the action stage. Thus, the lack of progress seen in many men in domestic violence groups may be attributable to their being in an earlier stage of change. Levesque, Driskell, Prochaska, and Prochaska (2008) reported findings from a pilot study on a stage-matched system intervention for domestic violence offenders. Such a program utilizes a computer program geared at identifying what stage of change an individual is at, as well as identifying specific exercises and activities aimed at helping them progress into the later stages of change. Some researchers have utilized TTM in their research finding encouraging results (Eckhardt, Babcock, & Homack, 2004; Scott & Wolfe, 2003), and other researchers have found weak or no evidence of effectiveness (Alexander & Morris, 2008; Brodeur, 2008)
Motivational interviewing (MI)
MI is a counseling strategy intended to help clients increase their readiness for change (Miller & Rollnick, 1991; Musser Semiatin, Taft, & Murphy, 2008). During MI, clients are assisted in utilizing and recognizing the aforementioned processes of change. The key components of MI include the use of empathy, development of discrepancy, avoidance of argumentation, utilization of resistance, and support of self-efficacy (Miller & Rollnick, 1991).
Research has shown that adding MI programming at intake can improve both treatment retention and lower recidivism rates among men attending programs for domestic violence (Taft et al., 2001) and sex offender intervention (Garland & Dougher, 1990). MI has additionally been shown to improve help-seeking behavior, reduce blaming, and encourage group participation and therapeutic homework completion with abusive men (Kistenmacher & Weiss, 2008; Musser et al., 2008).
The present study drew off from previous works conducted by Kistenmacher and Weiss (2008) and Musser et al. (2008) and published in the special issue of Violence and Victims, focusing on understanding and facilitating the change process in perpetrators and victims. Kistenmacher and Weiss examined the effects of MI on a group of men mandated to counseling as evidenced by a self-report test battery. This study utilized a randomized controlled trial design and took measures to ensure adherence to the MI model (Kistenmacher & Weiss, 2008). Musser et al. utilized a larger sample comprised of men who were both court mandated and self-referred. Results assessed group participation, homework completion, and partner reports of reabuse. The present study built on the findings of these two studies utilizing a substantially larger sample and restricting the participants to those who were court mandated. In addition, the present study utilized a statistical analysis method that allows for a greater understanding of the different trajectories for each stage of change, the MI condition, and the interaction between them.
The present study examined the global functioning of men who have been abusive in their intimate relationships. The three main research questions addressed were as follows:
Research Question 1: What is the influence of MI?
Research Question 2: What is the impact of stage of change?
Research Question 3: What is the effect of the interaction of MI and stage of change?
Predictions were that individuals at a later stage of change will reflect a greater recognition of distress in their lives and a desire to change, and the use of MI prior to the group therapy program will positively influence self-reported distress, reflecting a greater benefit from treatment.
Method
The present study utilized a quasi-experimental between-groups design to investigate the impact of MI and stage of change on participants’ self-reported global functioning. Data were collected at first contact with the agency, and again at the start and end of the group counseling program (pre- and post-test).
Participants
Data from 211 men were analyzed in this study. The respondents were selected from a group of 282 men who attended a domestic violence prevention program in a large Canadian city, between June 2007 and November 2008. Seventy-one individuals were excluded from the data because they were missing information on the stage-of-change variables; therefore, it was not possible to include them in the analysis.
Program participants from June 2007 to September 2008 (n = 106) did not receive MI prior to their referral to the Calgary Counseling Centre. Participants attending the program between September 2008 and November 2009 (n = 105) received two sessions of MI through Calgary Probation prior to their contact with the counseling centre. Participants in both groups were required to attend a minimum of one individual counseling session (mean = 4.43) with a therapist at the Calgary Counseling Centre prior to their enrolment in group. These sessions address the cessation of violence as well as working toward ensuring the safety of all members of the family (McGregor et al., 2002).
Demographic variables
The mean age of the participants was 34.6 years (10.77.); 87 were single, 40 were common-law, 41 were married, 31 were separated, and 11 were divorced. Two individuals reported less than high school–level education, 116 graduated from high school, 54 reported technical/vocational training, and 33 reported at least some university study. Table 1 provides a comparison of these and other characteristics that have been disaggregated by MI group.
Summary of Descriptive Statistics

Note: HR = high relapse; OQ = Outcome Questionnaire.
Responsible Choices for Men (RCM)
The RCM group is a 14-week group therapy program specifically designed for individuals who use violence and control in their intimate relationships (McGregor et al., 2002). It is part of a coordinated community response to address male domestic violence based on feminist perspectives using narrative methods (Jenkins, 1991) that focuses on changing belief systems related to the use of violence (Tutty et al., 2009). The RCM program uses a primarily process-oriented approach, whereby the most important component of the group is allowing members opportunity to discuss new ideas with one another and increase their self-awareness in a supportive environment (McGregor et al., 2002; Saunders, 1996). Within group process, RCM utilizes cognitive behavioral principles to challenge the belief systems and self-perceptions that support the use of abusive behavior (McGregor et al., 2002). Each group is comprised of 6 to 12 men, cofacilitated by a male and female therapeutic team to model a positive male–female partnership. The major objectives of the group are to decrease all forms of abusive behavior, promote acceptance and responsibility for personal behavior, increase self-esteem and assertiveness, improve family relationships, decrease stress, and increase empathy to those who have been affected by the violence (McGregor et al., 2002). The current study only considered data from the men who had been court mandated to attend treatment.
Measures
Outcome Questionnaire (OQ)
The OQ-45.2, is a 45-item self-report instrument designed for the repeated measurement of client progress and overall global functioning through the course of therapy (Lambert et al., 1996). Areas covered include symptoms, interpersonal relationships, and social role performance. Items are evaluated on a 5-point Likert-type scale with response options ranging from never, rarely, sometimes, frequently, or almost always true. Examples of questions include “I get along well with others,” “I feel irritated,” and “I’m not working/studying as well as I used to” (Lambert et al., 1996). Scores are compared to a clinical cutoff of 63, with higher scores reflecting individuals with more distress than the normative population, and lower scores reflecting less distress (Lambert et al., 1996). The repeated measurement is intended to capture change over time, as participants are requested to answer the questions based on the past week (Lambert et al., 1996). The OQ is psychometrically robust with adequate 3-week test–retest reliability (.84) and high internal consistency reliability coefficients (.93; Lambert et al., 1996). A 14-point change in score is considered to be a reliable change (Jacobs & Trux, 1991). Data from the OQ reflect the participant’s benefits from treatment at the first individual session and at first and final group sessions. The OQ was administered by the primary therapist at the first counseling session and by the group facilitators during the first and final group counseling sessions. Individuals who were missing data from any of the three time points were not included in the analysis.
University of Rhode Island Change Assessment (URICA)
The URICA is a 32-item scale with 8 items measuring each of 4 stages of stage: precontemplation, contemplation, action, and maintenance (McConnaughy et al., 1983, 1989). Participants respond to each statement on a continuum from 1 (strongly disagree), 2 (disagree), 3 (undecided), 4 (agree), and 5 (strongly agree). Data from the URICA were collected at the client’s initial counseling session.
University of Rhode Island Change Assessment—Domestic Violence (URICA-DV)
The URICA-DV is a 20-item scale based on the URICA and adapted specifically for use with an abusive male population (Levesque et al., 2000). The URICA-DV makes specific mention of violence in its questions and focuses only on men’s readiness to change their physical forms of abuse. Violence is defined in the scale as “physical aggression toward your partner” and lists a number of abusive behaviors that may cause physical pain or injury. The characteristics of each stage of change are the same as the original URICA; however, wording of the questions has been modified. Stages of change were grouped into five clusters, adapted from those described in Levesque et al. and Brodeur et al. (2008).
Analytic strategy
Repeated measurements of the global outcome variables were obtained from individuals who were categorized into different groups of interest. The individual person-level measurements were collected at three different time points: first counseling session, first session of group, and final session of group. A two-level hierarchical linear model (HLM) was employed to measure the group average change over time (Raudenbush, Bryk, Cheong, & Congdon, 2004; Singer & Willett, 2004). Level 1 measures the individual responses at time t and Level 2 represents an individual’s membership in each of the respective groups.
A series of indicator variables were used at Level 2 to indentify an individual’s group membership. Through this approach we were able to identify the average rate of individual change for each group. The results for each group were examined to determine whether there were statistically significant changes between groups at the intercept and in the slope.
Repeated-measurement studies such as this require special treatment of individual-level responses because the measurement of an individual’s score on the same test over time violates the assumption of independence in the standard ordinary least squares (OLS) regression model. In HLM, trajectories for each individual are measured at Level 1 and group averages are measured at Level 2. That is to say, Level 1 measures change within individuals and Level 2 measures the differences between groups.
Results
Table 1 provides the sample characteristics for group and aggregated samples. The table presents counts for categorical data and means and standard deviations for continuous data. In addition to the descriptive findings, we also conducted statistical analysis to determine whether the groups were statistically significant. We used the chi-square test for categorical data and the one-way ANOVA (analysis of variance) for continuous variables.
The findings of the chi-square and one-way ANOVA indicate there are no statistically significant findings between the MI and non-MI groups, indicating that they were equivalent groups. The number of group sessions attended was higher among the MI group, and the difference approached statistical significance at the .05 level. This nonsignificant finding has the potential to become significant if the sample size was increased.
Two-level hierarchical models for change
A null model was conducted to determine the mean intercept and slope for the full population. The intercept was 35.95 (SE = 1.83, p < .00). The model was centered at Time 2; therefore, the mean OQ score for the full sample at the pretreatment stage was 35.95. The mean slope was −8.86 (SE = 0.82, p < .00). This finding indicates that the average OQ score for the population sample at Time 1 was 44.81 and 27.09 at Time 3.
Stages of change
Table 2 compares differences in Level 2 (or group) averages for the intercepts and slopes. The reference group was the precontemplation group. The model indicates the preparation (β = 19.60, SE = 5.33, p < .001) and action-high-relapse (β = 14.50, SE = 5.72, p < .05) groups had statistically significant and higher OQ scores at the intercept when compared to the precontemplation group. An examination of the average slopes for the five groups demonstrates that the rate of change over time is not statistically significant between the five groups. This suggests that the average rate of change is the same for participants regardless of their stage of change; however, men in the preparation and action-high-relapse categories have higher-than-group-average OQ scores at the onset and these initial differences remain stable over time. More important, the model indicates all of the men demonstrate positive change in the form of decreased OQ scores as a result of their participation in the program and the rate of change is similar for all men.
Level 2 Analysis: Stages of Change π0 (Intercept) and π1 (Slope)

These findings are clearly demonstrated in Figure 1. Note that the preparation and action-high-relapse groups have higher scores when compared to the other groups. The slopes for the three groups are relatively similar to each other, and the model indicates there are no statistically significant differences between the slopes of the five groups.

Stage of change mean OQ scores at Times 1, 2, and 3
Motivational interviewing (MI)
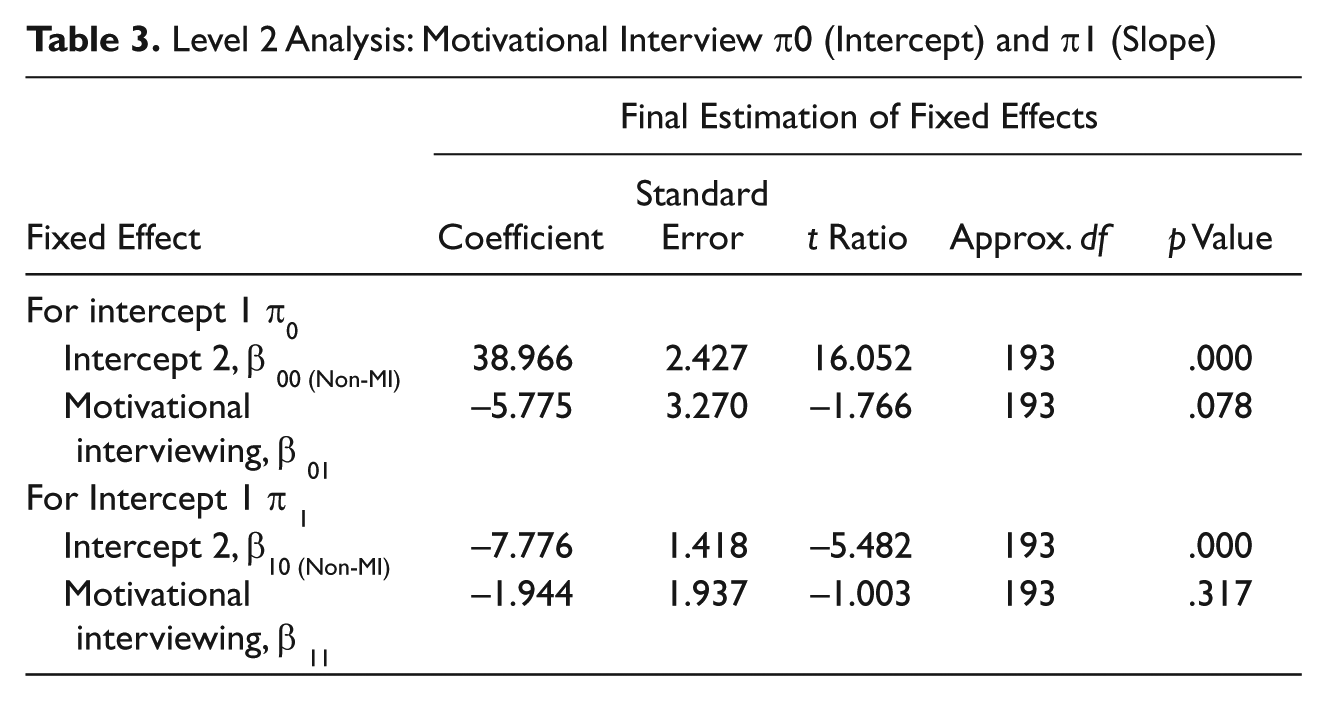
Table 3 provides the model statistics that test for differences in the slope and intercept between men who had two sessions of MI through Calgary probation prior to referral for counseling and those who did not. The results show that men who did not receive the MI (reference group) had higher OQ scores at the intercept. Their average score was 38.97 (SE = 2.43) compared to a score of 33.21 (SE = 3.27) for men who received the MI. This finding was approaching statistical significance at .05 but failed to meet the threshold (p = .078). It is important to note, however, that these are real differences in OQ scores for this sample. An examination of the standard error for the MI group shows a score of 3.27 with an effect size of −5.78. Thus, the effect of the MI intervention was not stable among men in this group. The findings also indicate no statistically significant differences between groups in the slope.
Level 2 Analysis: Motivational Interview π0 (Intercept) and π1 (Slope)
In spite of the nonstatistically significant findings, Figure 2 demonstrates the relationship between the MI and non-MI groups. Note that there are real differences in the average OQ scores between the two groups.

Non-MI versus MI mean OQ scores at Times 1, 2, 3
A model incorporating the five stages-of-change groups by the MI groups was run, and no significant findings were identified. This result was not surprising given the potential for small categorical cell sizes.
Discussion
Relevance of stage of change
The results obtained in the present study are consistent with past research using the TTM. These results suggest that an individual’s readiness to change, as evidenced by their stage of change at the beginning of therapy, is related to their global treatment outcomes. Individuals in the later stages of change (specifically, preparation and action-high relapse) scored significantly higher on the OQ, suggesting they recognized areas in their lives that are related to their need for treatment. Individuals in the earlier stages of change (precontemplation and contemplation) scored significantly lower on the OQ, reflecting that they may not be recognizing the need to make changes in their lives. Individuals in the action-low-relapse stage also scored lower on the OQ. This may indicate that these individuals may have already begun to make changes in perceiving the role that violence plays in their life.
It is important to note however that all the participants scored below the cutoff score at all three time points, suggesting that they were not distressed to begin with. As all the participants were attending the counseling as a condition of their probation, it is important to consider the degree to which these men were attempting to present in a socially desirable way. Further research with this population could utilize a test of social desirability such as the Marlowe–Crowne Social desirability test to control for presentation bias (Reynolds, 1982; Saunders, 1991).
Impact of motivational interviewing (MI)
Though the MI condition did not make the cutoff for traditional statistical significance (p = .078), this result should be considered clinically relevant. The average difference on the OQ score was almost 6 points, which is a substantial difference on this assessment tool, and hence, the impact of MI should be considered clinically relevant although not statistically strong enough to reject the null hypothesis (α = .05; Moore & McCabe, 2006). In addition, it is important to consider the relatively large standard error measure of 3.27. This suggests that some men responded to the change and others did not. Clearly this is an important area for further research.
Relevance of stage of change and MI interaction
When the within-group differences were examined for each stage-of-change group in the MI condition, men who received MI scored lower than those who did not receive MI. This is consistent with the findings from the regression analysis of the MI condition alone, suggesting that MI sessions may help the individual address some of the distress in their lives prior to the commencement of group therapy specific to their proneness to violence as evidenced by the OQ. The regression analysis showed the preparation–no MI, preparation–MI, and action-high-relapse–no-MI groups to have the greatest difference in score. This too is consistent with the first regression analysis on stage of change alone, suggesting individuals in the later stages of change recognize the most distress in their lives.
Implications for clinicians
Clinicians involved in this area of practice have a strong commitment toward increasing women’s safety (Gregory & Erez, 2002; McGregor et al., 2002). The present study identified that a man’s readiness and motivation to change affects his performance through the course of group therapy. This finding suggests that an assessment interview or a formal assessment with the URICA or URICA-DV gauging a man’s readiness and motivation to change could be beneficial to the group facilitator. Furthermore, this raises the question of whether men should be included in a group therapy program when they show only modest motivation or readiness to engage in therapy. It could be that improved outcomes could be achieved by providing individual counseling incorporating MI techniques as a pregroup treatment to individuals who are at a lower stage of change. Such interventions could improve the impact of the group intervention, resulting in an increased cessation of abusive behavior over time.
This study additionally identified that the men who engaged in MI sessions reported less distress on the OQ regardless of their stage of change. It may be that access to one-on-one counseling helped the men deal with some of the distress in their lives prior to engaging in the group therapy experience. Clinicians may want to consider the benefits of MI as a pregroup intervention for mandated men.
Mandated men represent a significant proportion of the population attending male domestic violence group therapy. They are likely to be resistant, defensive, and in denial of their problems (Scott & King, 2007; Scott & Wolfe, 2003) as well as attempting to present in a socially desirable way (Saunders, 1991). They may also be minimizing their role in the violence and remain at the point of victim blaming. Their motivation for attending the program may be extrinsic, as it represents their attempt to avoid jail time in putting their conviction for violence “behind them.” MI may assist this group in developing their own intrinsic motivations for doing the therapeutic work.
Considerations for Future Research
Multilevel growth modeling
The present study is among the first studies in the area of domestic violence that uses multilevel growth modeling in reflecting the extent of pretherapy conditions that can influence components of treatment outcomes. A valuable addition to the present study could have been the inclusion of a fourth time point, investigating self-reported distress at follow-up. Among the more important areas to be addressed include treatment attrition, future offending, and spouse-reported abuse.
The benchmark measure of whether a domestic violence intervention has been effective is reflected in the decline and ultimate cessation of violence following the intervention. The present study did not address this critical factor. The present study addressed within-treatment outcomes and whether or not therapy was helping the men identify and resolve distress in their own lives. Future research should investigate the extent to which TTM and MI enhanced treatment effectiveness as evidenced by subsequent abuse at follow-up.
Motivational interviewing (MI)
The high standard error seen in this study suggests that there may be factors separating men who benefit from MI from those who don’t. Future research can address this unknown factor.
Limitations
The present study drew on data collected in a clinical setting. As such, the methodology is limited as a result of the challenges and sensitivity associated with research in applied settings. Future research in this area should consider using a randomized control trial, assigning individuals to the MI or no-MI condition to ensure greater control of confounding variables.
The fact that the majority of participants in this study scored below the cutoff on the OQ suggests that something is influencing their scores. A test of social desirability could have explained this finding. Future research should include a measure of social desirability to investigate the impact of social desirability on participant’s willingness to respond in a forthright manner.
A final significant limitation to the present study is the assessment of the association between readiness to change and self-reported distress. This study drew on measures of the participants’ willingness to be accountable for behaviors that they had done, which was the basis for their engagement in the therapy work. It is not a measure of the extent to which they actually reduce or cease to commit subsequent acts of violence. From the results of this study, we can postulate that individuals who are accountable for their actions and ready to engage in the therapeutic process will make greater gains posttherapy. However, empirical evidence is still needed to further support this claim. Further research will be necessary to examine the degree to which MI and stages of change contributes to improving outcomes as reflected by a reduction of abusive behavior.
Summary and Conclusion
Notwithstanding the above limitations, the current study suggests MI may influence a man’s stage of change for self-reported outcomes in male domestic violence group therapy. The present study supports previous research findings that MI has the potential to improve treatment outcomes in male domestic violence group therapy. Results obtained showed that the presence of MI was linked to lower levels of reported personal distress. The results additionally suggest that TTM and the stages of change can be a useful predictor of those individuals who are most likely to report success from therapy. Thus, it is highly beneficial to assess individuals for their stage of change prior to the commencement of the group therapy program. The predictive utility of TTM suggests that effort should be taken to ensure that offenders are in a later stage of change prior to beginning group therapy in order to maximize their benefits from service.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Bios
![]() .
.