
Abstract
Identifying the factors that contribute to ongoing intimate partner abuse (IPA) among survivors of childhood abuse is essential to developing appropriate interventions. The current study assessed prospectively whether childhood betrayal trauma (BT) history and women’s potential dependence on their perpetrators (unemployment, number of children below 13) increased women’s risk of ongoing victimization, while controlling for trauma-related symptoms (PTSD, depression, dissociation). Women survivors of IPA (N = 190) from an urban U.S. city were recruited based on an IPA incident reported to the police. At the initial interview, women reported on childhood betrayal trauma experiences, their employment status, number of children, and current trauma-related symptoms. Women returned 6 months later and reported on ongoing events of victimization (physical, sexual, psychological aggression, and injury) in their relationships with the initial IPA perpetrator. Results showed that higher levels of childhood BT were associated with ongoing victimization over the course of 6 months. Women’s unemployment status predicted greater physical and sexual aggression and injuries. Higher levels of depression and lower levels of PTSD symptoms were also associated with increases in physical, sexual, and psychological aggression, and bodily injury. The findings have important implications for interventions by demonstrating the need to process women’s betrayal trauma experiences, target depression symptoms, and increase women’s economic opportunities to prevent further victimization.
Intimate partner abuse (IPA) poses a serious public health challenge in the United States, contributing to mental and physical health consequences (Mechanic, Weaver, & Resick, 2008; Rennison & Welchans, 2000). IPA that involves ongoing victimization (OV)—that is, repeated victimization in a single relationship—can result in frequent and repeated exposure to abuse as well as severe injuries, hospitalizations, and even death threats (e.g., Platt, Barton, & Freyd, 2009). Unfortunately, researchers have yet to identify the factors that increase women’s exposure to OV in intimate relationships. Drawing on betrayal trauma theory (BTT; Freyd, 2004, 2006), the current study tested predictors of OV prospectively, including childhood betrayal trauma exposure and dependence on the IPA perpetrator, while controlling for trauma-related symptoms.
Childhood Betrayal Trauma and OV
Traumas vary in the degree of social betrayal involved, from no betrayal (e.g., a non-interpersonal natural disaster) to low (an assault by a stranger) or high betrayal (abuse by a caregiver; see Goldberg & Freyd, 2006). Traumas high in betrayal are characterized by violations of a social contract in which a person or institution on whom the victim depends perpetrates abuse (Freyd, 1994). According to BTT, victims of high betrayal traumas (BTs) may adapt to preserve attachments to abusive caregivers who are necessary for their survival and development. For example, dissociation (DePrince, & Freyd, 2007; Freyd, & DePrince, 2001), amnesia (DePrince et al., 2012; Freyd, DePrince, & Zurbriggen, 2001), or altered emotional processing (Reichmann-Decker, DePrince, & McIntosh, 2009) may help victims to maintain necessary, though abusive, attachments in childhood. Although it may be adaptive in terms of survival goals for victims to maintain attachments to abusive caregivers in childhood (Barlow, & Freyd, 2009; Freyd, 1994, 1996), experiences of high BT may also place victims at risk for subsequent abusive experiences in adulthood. Indeed, studies document links between childhood BT exposure and revictimization in adulthood (e.g., DePrince, 2005; Gobin, & Freyd, 2009); however, researchers have examined only the presence/absence of later intimate abuse, leaving unanswered questions about whether childhood BT increases risk of exposure to OV overall, and severe OV in particular. Extending previous research, then, we predicted that a history of childhood BT exposure would increase OV in a single relationship over a 6-month period, particularly for severe forms of IPA.
Dependence on One’s Perpetrator and OV
Originally framed around childhood abuse, researchers have increasingly extended the BTT framework to understand the dynamics of abusive intimate relationships in adulthood (DePrince, Chu, & Pineda, 2011; Gobin, & Freyd, 2009). For example, being unemployed and/or having young children may increase the degree to which women depend on (or are interdependent with) their abusive partners, fiscally as well as emotionally. Women’s dependence on their current abusive partners may, in turn, be linked with OV (e.g., via decreased awareness of the abuse; see DePrince et al., 2012). To date, only a handful of studies have examined links between OV and variables that may reflect women’s dependence on their perpetrators. For example, having children increased Norwegian women’s risk of sexual, psychological, and physical violence in their current relationships (Solveig & Bjorkly, 2010). Though unemployment may increase women’s financial dependence on their abusive partners, and previous research has found that IPA predicts employment instability over time (Kimberling et al., 2009; Rigger, Staggs, & Schewe, 2004; Staggs & Rigger, 2005); researchers have yet to examine whether unemployment actually predicts OV. Building on this burgeoning literature, we predicted that factors reflecting women’s potential dependence on their abusers (defined in terms of unemployment and number of child under age 13) would be linked to greater OV over the course of 6 months.
Current Study
The current study extends BTT research by testing the relative contributions of childhood BT exposure (no, low, or high) and dependence in women’s current abusive relationships (employment status and number of children below 13) to the chronicity and severity of OV in adult intimate relationships. Though prior research has investigated the relationship between child abuse and revictimization (defined in terms of a presence/absence) in adulthood, researchers have yet to examine OV and its severity longitudinally. We examined these relationships in a diverse sample of women who had incidents of IPA reported to the police. We hypothesized that higher levels of childhood BT as well as dependence on the partner perpetrating the IPA (defined as being unemployed and having young children) would each uniquely predict more chronic (i.e., more incidences) and more severe forms (i.e., more physical, sexual aggression and injury than psychological aggression) of OV over a 6-month period. Because trauma-related symptoms are common consequences of childhood BT and may be risk factors for revictimization (e.g., Classen et al., 2005), we controlled for symptom severity (depression, dissociation, and PTSD symptom severity) in our analyses. Furthermore, because women were recruited into the current study based on an incident of IPA reported to the police, we controlled for the severity of that initial IPA event.
Method
Participants
Women (N = 236) were recruited from cases of intimate partner abuse (IPA) reported to law enforcement in an urban city in the Rocky Mountain West if the case involved a heterosexual couple and a male defendant. Women were interviewed shortly after the IPA incident for Time 1 (T1) and again 6 months later for Time 2 (T2). Of the 236 participants enrolled at T1, 192 (81%) women returned for a T2 follow-up interview 6 months after T1. Women reported their ethnic/racial backgrounds to be 47% (n = 111) White, 33% (n = 77) Black or African American, 2% (n = 4) Asian, 1% (n = 3) Pacific Islander, 11% (n = 27) American Indian or Alaskan Native, 6% (n = 14) Other, and 40% (n = 94) Hispanic or Latina. Women reported the following in terms of highest level of education: 3% (n = 8) first to eighth grade, 27% (n = 64) some high school, 26% (n = 62) high school, 25% (n = 59) some college, 8% (n = 18) associate’s degrees, 7% (n = 16) 4-year college degree, 3% (n = 6) postgraduate education, and 1% (n = 3) other (e.g., trade school). A majority (n = 121, 63%) reported having at least one child; 48% (n = 113) were employed.
Measures
Childhood betrayal trauma
The Trauma History Questionnaire (THQ; Green, 1996) is a 24-item self-report questionnaire with good reliability and validity that measures the history of exposure to traumatic events. The THQ measures the lifetime occurrence of a range of potentially traumatic events, including interpersonal violence (e.g., physical or sexual abuse). The THQ also gathers information on the number of times and approximate age each traumatic event occurred. To collect data on whether participants witnessed family violence as a child, an additional item from the Brief Betrayal Trauma Survey (BBTS; Goldberg, & Freyd, 2006) was added to the THQ. Eight items tapping interpersonal traumas (e.g., physical abuse, sexual abuse, emotional/psychological abuse, and witnessing family violence) were used to classify childhood betrayal trauma level (BT; Goldberg, & Freyd, 2006). Examples of items for each type of interpersonal trauma included “Has anyone ever made you have intercourse, oral or anal sex against your will?” (sexual abuse); “Has anyone, including family members or friends, ever attacked you with a gun, knife, or some other weapon?” (physical abuse); “Has anyone emotionally or psychologically mistreated you over a significant period of time (e.g., put you down, called you names, prevented you from seeing friends or family)?” (psychological abuse); “As a child, did you ever witness an adult deliberately attack another adult family member so severely as to result in marks, bruises, blood, broken bones, or broken teeth?” (witnessing domestic violence). To collect data on the perpetrator/s for each interpersonal trauma item, the THQ was modified further to include the inquiry “Who did this to you?” The relationship between the participant and the perpetrator/s (e.g., father, aunt, teacher, etc.) was assessed in terms of closeness to the victim to distinguish between levels of BT for each type of abuse.
The BT scheme, similar to that utilized by DePrince et al. (2011), was as follows: High BT = abuse perpetrated by someone who was very close like a caregiver (e.g., father, mother, or legal guardian), immediate family member (e.g., stepparents or siblings), or dating partner (e.g., spouse, significant other); Low BT = abuse perpetrated by extended family members (e.g., aunt, uncle, cousin, grandparent), other individuals who were somewhat close (e.g., friend, neighbor, teacher, babysitter, casual dating partner, etc.), or abuse perpetrated by someone who was not close like an acquaintance or stranger; No BT = the participant marked “no” for all interpersonal items on the THQ, and/or abusive experiences occurred only when the participant was age 18 or older. If the victim indicated that she was abused by more than one person, the perpetrator that the victim had the closest relationship with was used to classify the level of childhood BT. If the level of betrayal varied across different types of abuse (e.g., high BT physical abuse, but low BT sexual abuse) the highest level of BT across all eight items was used to classify the overall level of childhood BT. Age of the victim at the time of the abuse was used to determine whether the victim was a child (under the age of 18) or adult when the abuse occurred/began. Only events that occurred when the survivor was a child were classified as childhood BT. Weights for childhood BT levels were assigned as follows: no BT = −1, low BT = 0, high BT = 1.
Employment status and number of children
Background demographic information was obtained at T1 using a Demographics Questionnaire, which included questions regarding employment status (i.e., “Are you employed?” yes/no) and number of children under age 13.
Posttraumatic stress
The 28-item Posttraumatic Diagnostic Scale (PDS; Foa, Cashman, Jaycox, & Perry, 1997) was administered at T1 to assess PTSD symptom severity. The PDS is widely used and has high diagnostic agreement with structured clinical interviews assessing PTSD (Foa et al., 1997), including use with samples of female domestic violence survivors (DePrince et al., 2011). Cronbach’s alpha for this sample was .82.
Depression
Depression symptoms were assessed at T1 using the Beck Depression Inventory–II (BDI-II; Beck, Steer, & Brown, 1996), one of the most widely used self-report depression measures with good validity and reliability. This 21-item measure assesses depression symptoms based on DSM-IV criteria (APA, 1994). Cronbach’s alpha for this sample was .90.
Dissociation
The Dissociative Experiences Scale (DES; Bernstein & Putnam, 1986), a 28-item self-report measure that assesses dissociative experiences, was administered at T1 to assess dissociation symptoms. The DES has been shown to have good validity and reliability. Cronbach’s alpha for this sample was .94.
Ongoing victimization and incident severity
The Conflict Tactics Scale (CTS; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) is a widely used instrument that assesses conflict in intimate partner relationships. The CTS has been found to have excellent validity and reliability (Straus et al., 1996). The CTS has four scales: psychological aggression, physical aggression, sexual coercion, and injury. The CTS gathers information on the number of times each aggressive tactic on the four scales was used against the victim by an intimate partner. Cronbach’s alphas for this sample were as follows: psychological aggression .90; physical aggression .93; sexual coercion .92; injury .87. Participants were asked whether each of the items on the four CTS subscales occurred during the target IPA incident. Examples of items on the physical aggression subscale included “Did he slap you?” “Did he strangle you?”; Items on the sexual coercion subscale: “Did he use threats for sex?” “Did he force you to have sex?”; Items on the injury subscale: “Did he cause sprains or bruises?” “Did he knock you unconscious?”; And, items on the psychological aggression subscale: “Did he insult you or swear?” “Did he destroy your property?”
The CTS was used to assess IPA severity for the target incident at T1 as well as ongoing victimization occurring between T1 and T2. To determine IPA incident severity, items endorsed for each CTS subscale were summed to obtain a tally of events for each subscale, with more endorsed items indicative of higher incident severity. The incident tallies were summed to produce an overall IPA incident severity score: psychological aggression tally + physical aggression tally + sexual coercion + injury tally = total IPA incident severity. For ongoing victimization, the total number of occurrences for each aggressive tactic between T1 and T2 were summed for each of the four CTS subscales to determine the rate of OV during the last 6 months since survivors’ initial entry into the study. The subscales of the CTS were then divided into two categories, “high severity” and “low severity” to account for the severity of victimization experiences: high severity CTS = physical aggression + sexual coercion + injury; low severity CTS = psychological aggression. Both high severity and low severity scores were used to assess ongoing victimization over the course of 6 months with the same intimate partner. Note: the term “severity” refers only to the likelihood that each type of abuse could have resulted in medical hospitalization or physical threat to a woman’s life, not to how detrimental an impact the type of abuse had on women’s emotional health or general well-being (in such a case psychological aggression could be more severe than physical or sexual aggression).
Procedure
As part of a larger study, researchers contacted women by phone to invite them to participate in a “Women’s Health Study.” Participants were identified through publically accessible records of domestic violence reports in a large metro area in the Rocky Mountain West (see DePrince, Labus, Belknap, Buckingham, & Gover, 2012, and DePrince, Belknap, Labus, Buckingham, & Gover, 2012, for details about the larger study and sample representativeness). Of the 827 women we attempted to recruit, 29% (n = 239) of women scheduled and attended the first interview. Only 9% (n = 78) declined to participate when reached by phone, while 8% (n = 64) said they would call back, but did not; 15% (n = 125) canceled/no-showed to the first scheduled interview and could not be rescheduled; 39% (n = 321) were never reached by phone. The women who agreed to participate were scheduled for a 3-hr interview at a research office. Women were informed that their names were accessed using public records and that the research was about IPA during the informed consent process. Consent information was provided both verbally by research personnel and on written forms. A consent quiz was administered to ensure that all women understood the consent information. Women were asked to complete questionnaire items and answer interview questions that were part of this larger study. Part of this interview included demographic questions, the THQ, BDI, PDS, DES, and CTS. Participants were debriefed and compensated US$50 for their time. Six months after their initial interview, participants were asked to return for follow-up interviews that were very similar to the first interview. When answering the questions on the CTS, women were asked to report events that occurred since the last interview with their partner who was the perpetrator in the initial IPA incident. Participants were debriefed and compensated US$55 for their time. This study and all of its procedures were approved by a University’s Institutional Review Board.
Data Analysis
Imputation
Of the 236 participants in the study, 192 (81%) returned for Time 2 six months later. Of the 192 participants who returned for Time 2, 159 (83%) had complete data for all key variables. Exploratory analyses comparing participants who returned for follow-up (n = 192) and those who did not return (n = 44) on all key study variables were not significant; therefore the two OV outcome variables (high severity CTS score and low severity CTS score) were not imputed. To evaluate whether key study variables aside from the outcome variables should be imputed, independent sample t tests were conducted to evaluate missing data only among the participants who did return for T2 (n = 192). Comparing participants with childhood BT data (n = 163) to participants without childhood BT data (n = 29) showed significant differences in CTS low severity scores, indicating that data for this key variable (i.e., childhood BT) were not missing at random. Therefore, based on recommendations by Acock (2005), the Expectation Maximum (EM) method was used to conduct a series of regression imputations for 17% of the data set using SOLAS for Missing Data Analysis© (Statistical Solutions, Inc.) software. The following key variables were imputed for all monotone data: posttraumatic stress (PDS scores), depression (BDI scores), dissociation (DES scores), childhood BT, number of children, and IPA incident severity (CTS score for T1). Two cases were excluded from the final data set because they were missing data for all of the key variables and were unable to be imputed, yielding a final total sample of 190. To maintain consistency across imputed and original scores, imputed childhood BT scores were converted into BT level weights (–1 = no BT, 0 = low BT; 1 = high BT) using conventional rounding techniques. Transformations of the imputed data did not alter the beta coefficient for the childhood BT variable. Notably, analyses conducted with complete cases only data (n = 159) yielded the same pattern of results.
Results
Before beginning analyses, distributions of all continuous variables were assessed for skew, kurtosis, and outliers. Skew and kurtosis were satisfactory for all variables. Outliers 2.5 SD above or below the mean were windsorized; however, because analyses performed with transformed variables did not produce different results, the original variables are reported here.
Descriptive Statistics and Correlations
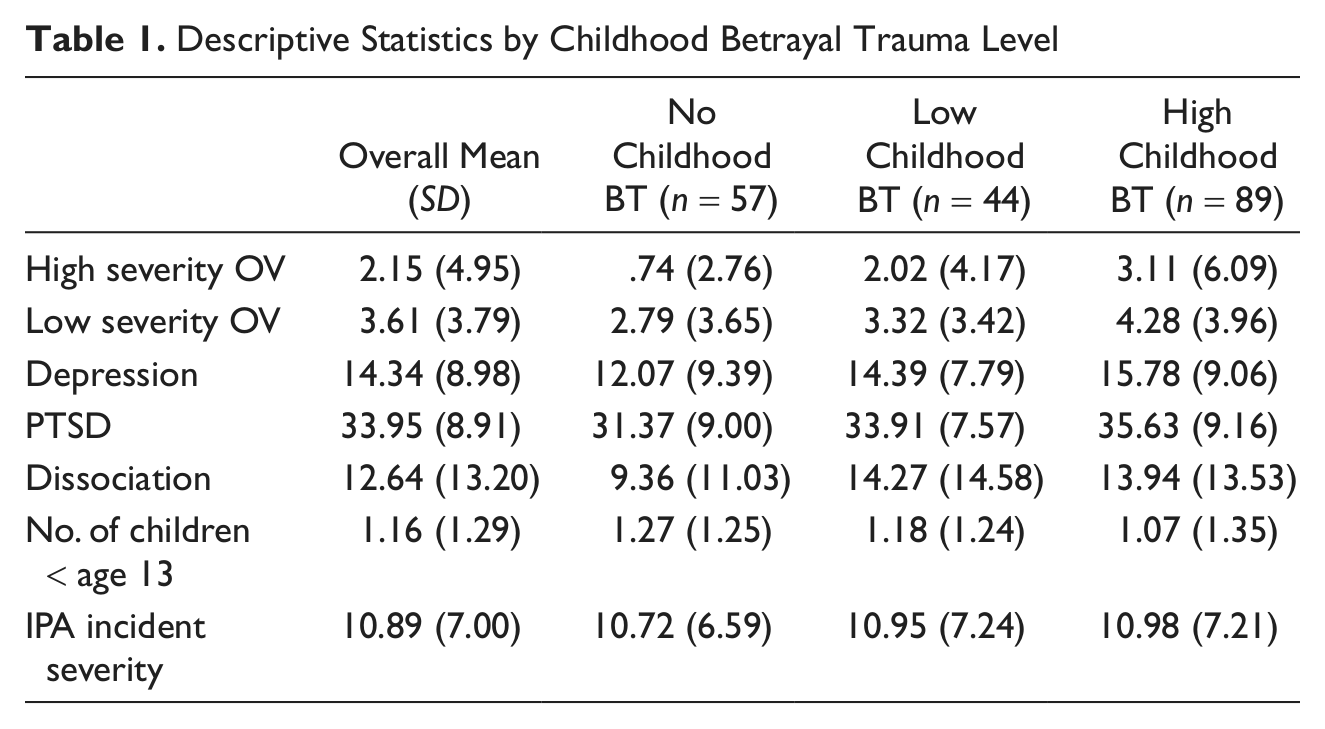
The results from the THQ showed that 47% of women reported experiencing trauma high in betrayal during childhood, 23% experienced low childhood betrayal trauma, and 30% had no childhood betrayal trauma. Table 1 provides descriptive statistics for all continuous variables used in the regression models: depression, PTSD, dissociation, IPA incident severity, number of children under 13, high severity OV and low severity OV. In addition to providing overall means, Table 1 describes these variables by level of childhood betrayal trauma (i.e., high, low, or no). Bivariate correlations were performed to explore relationships between all variables included in the regression models. These variables included childhood betrayal trauma level (–1 = none, 0 = low, 1 = high), number of children under 13, employment status, depression, PTSD, dissociation, IPA incident severity, and ongoing victimization events tallied by severity. Table 2 presents the bivariate correlations.
Descriptive Statistics by Childhood Betrayal Trauma Level
Bivariate Correlations Among Variables Used in Multiple Regression Analyses
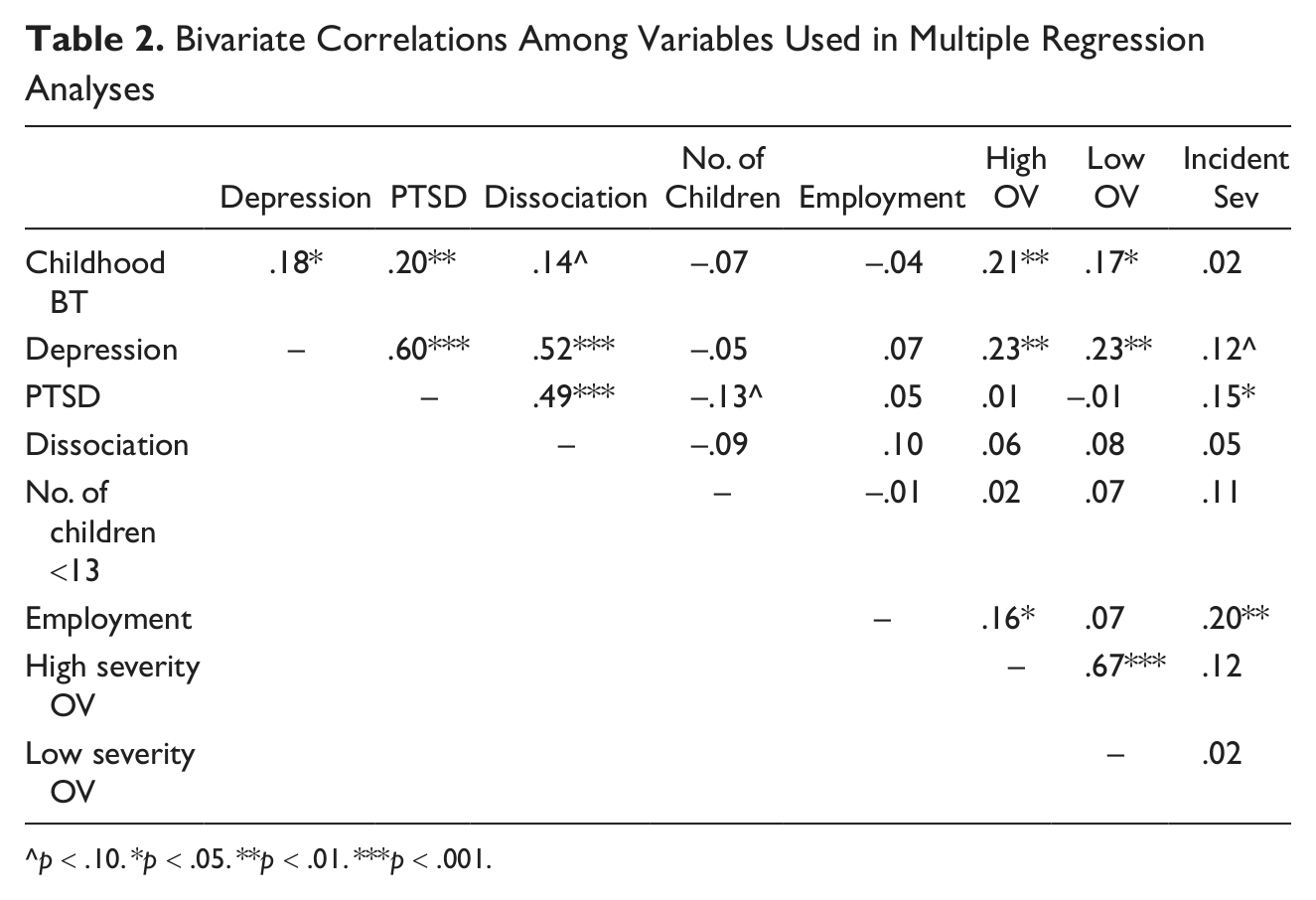
p < .10. *p < .05. **p < .01. ***p < .001.
Regression Models: Predictors of High and Low Severity OV
Two simultaneous regression analyses were conducted to assess whether childhood BT history and indicators of dependence on one’s perpetrator measured when women entered the study (T1) predict high or low severity ongoing victimization over the course of 6 months (T2) after controlling for trauma-related symptoms and IPA incident severity. The results of two simultaneous regression models are displayed in Table 3. Results show that both of the overall models were significant: high severity victimization, R2 = .14, F(6, 182) = 3.58, p < .01, and low severity victimization, R2 = .12, F(6, 182) = 3.02, p < .01. Regression coefficients for childhood BT were significant in both models, and the regression coefficient for employment was significant in the high severity model. Also, the regression coefficients for PTSD and depression were significant in both the high severity and low severity models. The regression coefficients were not significant for number of children under 13, dissociation, or IPA incident severity in either the high severity or low severity victimization models. Childhood BT and unemployment predicted high severity ongoing victimization at T2, even after controlling for trauma-related symptoms and IPA incident severity. In addition, increases in depression symptoms and decreases in posttraumatic stress symptoms predicted increases in both high and low severity ongoing victimization at T2.
Regression Coefficients of Simultaneous Regressions Assessing Predictors of Ongoing Victimization
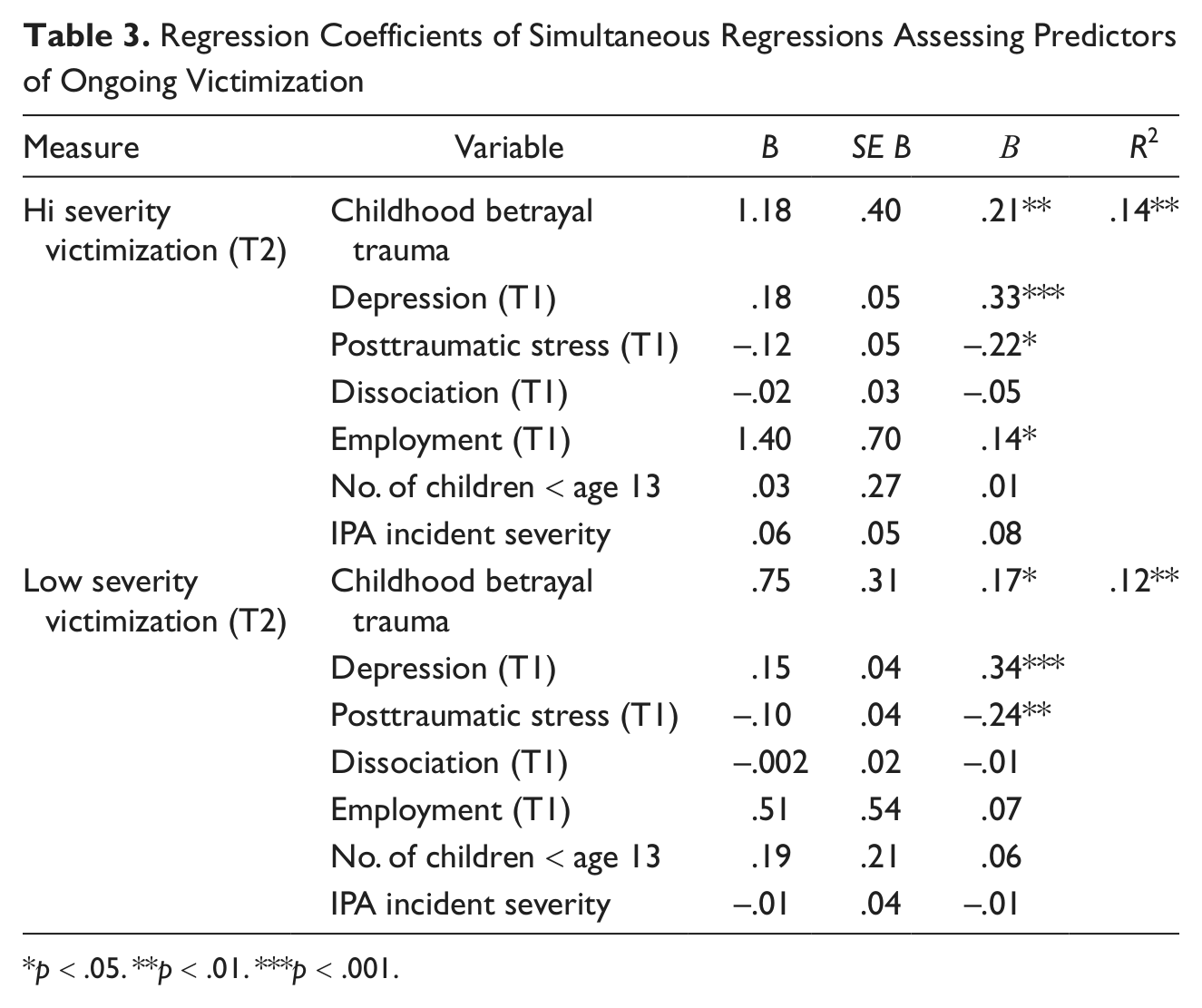
p < .05. **p < .01. ***p < .001.
Discussion
Higher levels of childhood betrayal trauma among women IPA survivors predicted more OV events during a 6-month period following a police-reported IPA incident, even when controlling for current trauma-related symptoms and the severity of the initial IPA incident. In fact, women who experienced higher levels of childhood BT were significantly more likely than other women in the sample to report severe OV, including physical aggression, sexual coercion, or events resulting in serious bodily injury. Extending previous studies that document links between childhood BT and revictimization (Gobin, & Freyd, 2009; Platt et al., 2009), childhood BT was associated with chronic and severe OV during a 6-month period after an incident of police-reported IPA. These results highlight the deleterious long-term consequences childhood betrayal trauma can have on survivors’ well-being later in their life span, especially in terms of interpersonal relationships. If a child is abused by someone whom she is close to, trusts, or depends on for survival, this betrayal places the child at an increased risk of ongoing and severe IPA in adult relationships.
Just as childhood BT experiences increased women’s reports of severe OV in adulthood, so did factors related to women’s dependence on their current abusive partners. Specifically, we found that women who were unemployed when entering the study were more likely to experience severe OV involving physical aggression, sexual coercion, or bodily injury (but not more likely to experience psychological OV) than employed women, 6 months later. These findings are consistent with calls in the literature for interventions that target unemployment and other poverty-related factors to decrease women’s risk of further victimization (Klest, 2010; Sokoloff & Pratt, 2005). In their study assessing outcomes of the federally funded Job Readiness Program (JRP) operating in domestic violence shelters in Kentucky, Sokoloff and Pratt (2005) suggested that
a more effective way to reduce woman battering is to empower battered women by providing the underlying structural conditions for independent housing, job training and opportunities, affordable child care, and social services which allow women to break away from violent relationships. (p. 389)
These findings provide further support for the basic framework of Betrayal Trauma Theory (Freyd, 1994, 1996) in terms of identifying links between childhood betrayal and adult experiences of ongoing violence in intimate relationships as well as between variables that imply dependence in relationships (e.g., economic indicators) and abuse severity. This research points to the potential importance of extending the Betrayal Trauma Theory framework to research on the dynamics of adult intimate abuse, in addition to child abuse.
Originally included as control variables, results regarding trauma-related symptoms may have important implications for interventions with IPA survivors. Results showed that women with higher levels of depression, but also women with lower levels of PTSD were more likely to experience OV over the course of 6 months. These findings are contrary to previous research conducted with CSA survivors (Arata, 1999; Messman-Moore, Ward, & Brown, 2009) and sexual assault victims (Ullman, Najdowski, & Filipas, 2009) where PTSD predicted sexual revictimization. Perhaps in the face of OV with a single partner, PTSD symptoms serve an adaptive function of signaling to women (through fear, hypervigilance, etc.) the severity of abuse. In contrast, women with lower levels of PTSD symptoms may be less vigilant to their partner’s danger signs, placing them at greater risk for further victimization. Complementing this finding, Matlow and DePrince (2012) found that women who reported greater fear following IPA also reported greater readiness to leave the abusive relationship a year later. Given these complementary findings, more research is needed to understand the role that PTSD symptoms and related experiences (such as fear) may play in OV. The current findings also highlight the profound impact that depression—a frequently overlooked trauma-related problem—may have on women’s likelihood of experiencing OV. Primary symptoms of depression like negative self-attributions, sadness, worthlessness, or lack of motivation (Beck, Steer, & Brown, 1996) may disempower women, making them more vulnerable to OV or limiting their ability to leave abusive relationships.
Limitations and Conclusions
Though results of regression analyses predicting OV over the course of 6 months were significant, childhood betrayal trauma, employment, PTSD, and depression accounted for only a portion of the variance in OV. Future research is needed to identify additional factors that contribute to OV among women who have been previously abused to better understand and prevent further victimization in this population. This study interviewed women who experienced IPA by a male perpetrator that was reported to police. Given the high rates of IPA that is not reported to the police in the United States, future research will need to evaluate the extent to which these findings generalize to women who experienced IPA that was not reported to the police, or that was not perpetrated by a male partner. Moreover, the size of the sample in this study was modest, thus replication of results is needed. The current study also used a dichotomous variable (e.g., are you employed? yes/no) to examine the links between employment status and general types of OV (e.g., physical, psychological, sexual aggression, and injury). Future studies using continuous indicators of women’s income levels to predict specific categories of IPA (e.g., fights, coercive control, etc.) are necessary to provide a more detailed understanding of how women’s employment status predicts OV. Prospective studies are also needed to further advance our understanding of how experiences of childhood BT could potentially increase survivors’ risk of entering abusive, dependent relationships during adulthood.
This study assessed a diverse, community sample of women who experienced an IPA incident reported to the police in an urban U.S. city. Recruitment and retention of women IPA survivors in this study was very successful, and the design of the study allowed for a 6-month longitudinal assessment of OV in these women’s relationships. The current findings extend previous research (Gobin, & Freyd, 2009; Platt et al., 2009) by providing evidence that childhood BT increases women’s risk of experiencing severe OV in their chronically abusive relationships during a specific 6-month period. These findings also demonstrate how frequently overlooked factors of dependence (potentially linked to experiences of childhood BT), such as unemployment, increase women’s risk of OV. The fact that childhood BT and unemployment both uniquely predict OV, even after controlling for trauma-related symptoms and initial IPA severity, demonstrates the critical need for interventions to be tailored to address these factors. Higher levels of depression predicted OV, yet results also suggest that PTSD symptoms, though debilitating, may be protective by decreasing the likelihood of OV. Understanding how previous experiences like childhood betrayal trauma or proximal factors like dependence on one’s current perpetrator influence women’s risk of ongoing victimization in their intimate relationships is crucial to better inform intervention strategies for survivors.
Footnotes
Acknowledgements
Thank you to our study partners including Joanne Belknap, Susan Buckingham, Jennifer Labus, and Angela Gover; Denver District Attorney’s Office; City Attorney’s Office; Denver Police Department Victim Assistance Unit; Denver Domestic Violence Coordinating Council; SafeHouse Denver; Project Safeguard; AMEND; and the Triage Steering Committee. Thank you to the Traumatic Stress Studies Group, Stephen Shirk, and Daniel McIntosh. Finally, thank you to the women who participated in this study.
Authors’ Note
The opinions, findings, conclusions, or recommendations expressed in this report are those of the authors and do not necessarily reflect those of the Department of Justice or the National Institute of Justice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Award No. 2007-WG-BX-0002 awarded by the National Institute of Justice, Office of Justice Programs, U.S. Department of Justice.