
Abstract
Human trafficking is recognized as a major public health problem and a tragic transnational crime. Little is known about the health outcomes of victims of human trafficking. This study identifies the relationship of risk factors to physical, sexual, and mental health outcomes in three groups of women (N = 38) exploited for sex in the United States: international trafficking victims, domestic trafficking victims, and nontrafficked sex workers. To date this is the first study to examine the impact of risk factors on health outcomes using a sample of women trafficked for sex in the United States that includes both domestic and international victims. Overall, findings suggest that the experiences in sex work of domestic trafficking victims were dissimilar to those of international trafficking victims. Moreover, domestic trafficking victims displayed poorer health outcomes compared to international trafficking victims. In terms of risk factors, a higher percentage of women involved in street prostitution reported sexual health problems, co-occurring health issues, and addiction. Childhood physical/sexual victimization was related to poor physical health.
Keywords
Introduction
Human trafficking is recognized as a heinous crime and a public health issue. Its victims are disproportionately young women and children (Winterdyk & Reichel, 2010). Its health implications are severe, believed to affect hundreds of thousands annually (Siskin & Sun Wyler, 2010). Despite the growing recognition that human trafficking is an important national and global issue, little empirical research containing primary data has been published (Zhang, 2009). Zimmerman, Hossain, and Watts (2011) note, in their recent article outlining a conceptual model of human trafficking and health, that “health is a subject that has been largely neglected in anti-trafficking work” (p. 327). This article attempts to address this void through the identification and examination of risk factors associated with health outcomes of women sexually exploited in the United States. We review social science literature (including the fields of criminal justice/criminology and public health) to identify risk factors affecting the physical, sexual, and mental health outcomes of women exploited for sex, and analyze secondary data to advance our understanding of how three specific risk factors—early exposure to trauma, the nature of sex work, and the presence of coercion/deceit or entering sex work as a minor (e.g., being trafficked) shape health outcomes. To date this is the first study to examine the impact of risk factors on health outcomes using a sample of women trafficked for sex in the United States that includes both domestic and international victims.
Literature Review
According to the U.S. Department of State, human trafficking has been used as an umbrella term for the activities involved when one person obtains another in compelled service, often referred to as involuntary servitude, slavery, debt bondage, or forced labor (U.S. Department of State, 2011). In 2000 the U.S. Congress enacted the Victims of Trafficking and Violence Protection Act (TVPA), which defined sex trafficking as “the recruitment, harboring, transportation, provision or obtaining of a person for the purpose of a commercial sex act.” Commercial sex act is defined as “any sex act on account of which anything of value is given or received by any person.” The TVPA further delineated severe forms of trafficking to be those instances when a commercial sex act is “induced by force, fraud or coercion, or in which the person induced to perform such act has not attained 18 years of age” or “the recruitment, harboring, transportation, provision, or obtaining of a person for labor or services, through the use of force, fraud, or coercion for the purpose of subjection to involuntary servitude, peonage, debt bondage, or slavery.” According to the federal government, prostitution by willing adults is not human trafficking regardless of whether it is legalized, decriminalized, or criminalized, and child pornography per se is not sex trafficking, unless an actual child is induced to perform a commercial sex act for the purposes of producing the pornography. Some scholars, however, contend that all prostitution is a form of sexual exploitation, human trafficking, and a violation of human rights, arguing that the distinction based on the argument that some women volunteer and others do not volunteer in the sale of sex is artificial (Farley et al., 2003; Farr, 2005). A full discussion of this debate is beyond the scope of this article and readers are referred to others for additional information (Farley, 2009; McKinnon, 2011).
Estimates of the number of persons trafficked have varied widely and critics charge they are largely guesswork (Zhang, 2009). Only the U.S. government and the International Labour Organization (ILO) provide global estimates of human trafficking. The ILO (2005) estimated 2.5 million adults and children are in forced labor, bonded labor, or forced prostitution worldwide, and nearly half are below the age of 18. The U.S. State Department estimates roughly 800,000 persons are trafficked across borders each year (i.e., international trafficking); or between 2 and 4 million persons if trafficking within borders (i.e., domestic trafficking) is included (Siskin & Sun Wyler, 2010).
Sex Trafficking in the United States
Little research has been conducted on sex trafficking in the United States despite its attractiveness as a destination point (Phinney, 2001). The full extent of the trafficking of women into (and in) the United States is not known; the estimates are unreliable and difficult to obtain given the hidden nature of this crime (Laczko & Godziak, 2005). Sex trafficking primarily exploits women and children (Farr, 2005; Phinney, 2001). Early estimates from the federal government reported nearly 50,000 women and children are trafficked into the United States annually (O’Neill, 1999). More recent figures are more modest, estimating 14,500 to 17,000 individuals are trafficked annually into the United States, and 80% of these international victims are female and 70% are trafficked into the sex industry (Clawson, Dutch, Solomon, & Goldblatt Grace, 2009). According to the U.S. State Department (2010), more U.S. citizens are found in sex trafficking than labor trafficking, whereas more foreign victims are found in labor trafficking than sex trafficking.
Moving beyond estimates, information on suspected or known incidents of human trafficking, drawn from information provided by 45 human trafficking taskforces that operate throughout the United States, indicates that the number of victims may be even more modest. Between January 2008 and June 2010, 2,515 suspected incidents of human trafficking were investigated, and nearly 8 in 10 of the suspected incidents involved sex trafficking. The victims in confirmed sex trafficking cases (n = 389) were overwhelmingly female (94%), slightly less than half were under age 18, and four-fifths were U.S. citizens (Banks & Kyckelhahn, 2011).
The vast majority of our knowledge on human trafficking is drawn from international victims trafficked into the United States and less is known about domestic victims (Clawson et al., 2009). Furthermore, most current information on trafficking comes from case studies, the media, and law enforcement, government, and nongovernment organizations’ (NGO) reports. In their recent review of the literature, Clawson and colleagues (2009) note that much of the research published in peer-reviewed journals is limited to descriptions of the scope of the problem, whereas information on the needs and services provided to the trafficked population is found in the aforementioned case studies, the media, and law enforcement, government, and NGO reports.
Knowledge of Health Outcomes Among Persons Involved in Trafficking and Prostitution
While noting that prostitution and sex trafficking may differ in their legal definitions, researchers acknowledge that the lifestyle exposure and general health risk of prostitution can serve as an approximation of the general health risks of trafficked victims (Phinney, 2001). The literature is filled with statements that intuitively note that women in the sex industry, along with other marginalized populations (e.g., migrant women, exploited women laborers, women experiencing intimate partner violence) often suffer from poor nutrition, experience dangerous working conditions, and are at increased risk for exposure to infectious diseases (Gajic-Veljanoski & Stewart, 2007; Zimmerman et al., 2003). Indeed, a common precursor to sexual exploitation is physical or sexual abuse during childhood (Campbell, Ahrens, Sefl, & Clark, 2003; Wilson & Widom, 2010). However, while victimization may originate in childhood, it does not appear to end there. Victims of human trafficking report repeated and intrusive trauma (Briere & Spinazolla, 2005) that involves physical and sexual violence and psychological damage from restrictions on their movement and fear of reprisals. Research consistently shows that trafficking victims experience extensive violent victimizations across their lifetimes; 6 in 10 have been threatened with a weapon; 7 in 10 have been physically assaulted; 6 in 10 have been raped or sexually abused; 5 in 10 reported physical injury due to violence; and 7 in 10 reported having freedom of movement restricted (Farley et al., 2003; Zimmerman et al., 2008).
Whereas the trauma related to trafficking has been well documented, the health of trafficked victims has been largely neglected. Trafficking as a public health concern is in its “nascent stages” (Zimmerman et al., 2011, . 334). There is relatively little understanding of the health consequences for women trafficked, with exception of sexually transmitted infections (STIs) and HIV/AIDS, which has received extensive attention due to their transmission risk. Sex trafficking has been listed as a key factor in the heterosexual transmission of HIV/AIDS around the world, with men who buy sex the primary carriers of the disease (Spittal et al., 2003; World Health Organization, 2000).
In 2008 a U.S. Department of Health and Human Services national symposium provided an important venue to identify the serious and complex mental health needs of trafficking victims, including posttraumatic stress disorder, anxiety and mood disorders, dissociative disorders, and substance-related disorders (Williamson, Dutch, & Clawson, 2009). However, still few studies have examined physical or mental health outcomes of trafficked victims. Those that have are largely descriptive, based on convenience samples of women in treatment, detention, or brothels, and have been conducted outside of the United States. (Cwikel, Chudakov, Paikin, Agmon, & Belmaker, 2004; Decker, McCauley, Phuengsamran, Janyam, & Silverman, 2011). Findings of this scant research, generally speaking, report that sexually exploited women present increased levels of anxiety, depression, and posttraumatic stress disorder (PTSD; Farley et al., 2003; Tsutsumi et al., 2008; Zimmerman et al., 2008). Furthermore, reports of poor physical health were also common, with 6 in 10 reporting back pain, memory difficulty, stomach pain, pelvic pain, or gynecological infection, and 8 in 10 reporting headaches and fatigue (Zimmerman et al., 2008). In addition, studies note that trafficked women have limited access to health care or social services (Cwikel et al., 2004; Zimmerman et al., 2003). Such access is important to preventing the onset and exacerbation of negative health consequences among this vulnerable population (Beyrer & Stachowiak, 2003).
Comparatively speaking, far less is known about the health consequences for domestic or international women sex trafficked in and within the United States than in other nations. The limited research available suggests that the experiences of women sexually exploited in the United States parallel those in other countries (Aron, Zweig, & Newmark, 2006; Farley et al., 2003; Raymond & Hughes, 2001). As part of their larger nine nation study, Farley and colleagues examined chronic health problems for a subset of U.S. women (n = 21) no longer involved in prostitution and Canadian women (n = 100) still involved in prostitution, and found that the health risks of involvement in prostitution were indeed persistent, with the largest percentages of respondents in both groups reporting memory problems and physical injuries due to violence. Similarly, international trafficking survivors (n = 34) interviewed in three selected U.S. cities reported acute problems related to medical or dental care due to neglected health conditions (Aron et al., 2006). Raymond and Hughes (2001) interviewed 40 domestic and international sex trafficking victims in five regions of the United States and noted that women suffered multiple traumas due to violent sexual exploitation experienced. They found that the prevalence of injury (e.g., broken bones, sprains, stab wounds, bruises, head injuries, oral bleeding, and vaginal bleeding) as well as the contraction of major illnesses (e.g., hepatitis) and STIs was higher among U.S. women than international women. A larger percentage of U.S women reported no use of birth control, and if birth control was used, the primary form was condoms. Nearly half of both the U.S. and international women reported becoming pregnant as a result of sexual exploitation, but more U.S. women gave birth (42%) compared to international women (20%). Mental health consequences of exploitation also were measured, and here, with the exception of a higher percentage of U.S. women reporting suicidal thoughts/attempts and feelings of anger/rage, no differences were reported in rates of depression/sadness, inability to feel, difficulty sleeping, self-blame/guilt, and loss of appetite.
Risk Factors: The Pathway and Nature of Sex Work
Scholars agree that sex work, regardless of its form, poses potential and oftentimes life threatening risks (Dalla, Xia, & Kennedy, 2003). The International Organization for Migration (2007) noted a number of risk factors associated with trafficking that may influence health including physical, sexual, and psychological abuse; poor living and working conditions; exposure to wide range of diseases; social isolation and captivity, lack of access to health care, forced use of drugs/alcohol; limited or no access to health and social services; and poverty. For the purposes of this study, we will focus specifically on the effects of street prostitution, trauma exposure, and entry into sex work via trafficking on health outcomes among women in sex work.
Street prostitution
For those persons whose trafficking condition involves street prostitution, the risk of violent victimization at the hands of pimps and/or johns is ever present (Campbell et al., 2003; Silbert, 1982). Current consensus in the research suggests that the risk of violence victimizations is higher for women involved in street prostitution versus off-street venues, such as escort services, brothels, massage parlors, and exotic dancing (McElroy, 1998). However, scholars also correctly note that far fewer studies have examined the experiences of women whose prostitution occurs in indoor venues (Raphael & Shapiro, 2004). The few studies which have been done (Holsopple 1999; Maticka-Tyndale, Lewis, Clark, Zubick, & Young, 2000; Wesley, 2002) found significant amounts of violence, but relied on small samples, often did not measure the frequency of reported violence, and failed to consider whether women operate in indoor and outdoor venues simultaneously. In one of the few comparative studies done, Church, Henderson, Barnard, and Gran (2001) examined the degree to which violent victimization experiences varied dependent on whether prostitutes worked outdoors or indoors in three British cities and found that prostitutes working outdoors were younger, involved in prostitution at an earlier age, reported more illegal drug use, and experienced more violence from their clients than those working indoors. More recently, Raphael and Shapiro (2004) surveyed 222 women from Chicago currently or recently involved in prostitution asking about their type of prostitution activities and venues. Their findings indicated that a larger percentage of women in the streets, in drug houses, and in hotels experienced more types of violence than women in other venues. They also noted that in some instances, prostituted women indoors experienced more serious forms of violence than prostituted women outdoors, for example, high prevalence of being threatened with a weapon and threatened with rape.
Du Mont and McGregor (2004) in comparing the nature of police-reported sexual assaults experienced by sex workers compared to other sexual assault victims who sought emergency services in Vancouver, Canada, reported that sex workers were significantly more likely to sustain a greater number of genital and extragenital injuries, such as bruises, lacerations, tenderness, bite marks, scratches, swellings, and to test positive for the presence of sperm or semen than other victims of sexual assault.
More recently, Cohan and colleagues (2005) used data from the Young Women’s Survey, a population based cross-sectional survey of 2,543 low income women in northern California, to examine the sexual and drug using behaviors and prevalence of infections (HIV, STI, and hepatitis A, B, and C) of those involved in prostitution (n = 226) and those not (n = 2,317). Their findings suggest, not surprisingly, that those involved in prostitution were more likely to report previous infections for Chlamydia, gonorrhea, and syphilis; had more lifetime male sexual partners; were more likely to have sex with a man who also had sex with men and IV drug users; and had an HIV-infected partner. A history of sexual coercion also was more prevalent among those involved in prostitution.
Trauma exposure
Early exposure to trauma, especially experiencing sexual coercion prior to adulthood, is an acknowledged risk factor for sexual exploitation later in life. However, given that sexual coercion may be persistent and reoccur, scholars have been interested in determining if the initial trauma, given its occurrence at an earlier yet arguably more vulnerable age, results in poorer health outcomes than more recent trauma. Research conducted in Israel with sex trafficked women in brothels and women awaiting deportation examined how early exposure to trauma (defined as experiencing homelessness, hunger, parental neglect, sexual abuse, physical abuse, or rape before age 18) and exposure to violence while involved in prostitution influenced current health outcomes (Chudakov, Ilan, Belmaker, & Cwikel, 2002; Cwikel et al., 2004). After controlling for age, findings suggest that early exposure to trauma was related to trauma while involved in prostitution and to poorer health outcomes, symptoms of depression, PTSD, and physical complaints. Furthermore, exposure to trauma during involvement in prostitution increased reporting of depression, PTSD, and physical symptoms.
In addition to examination of initial trauma, scholars have also studied the effects of sexual revictimization on health outcomes. Victims of multiple assaults often experience several negative health outcomes, compared to those with histories of childhood sexual abuse, such as unintended pregnancies and abortions (Wyatt, Guthrie, & Notgrass, 1992). Furthermore, West, Williams, and Seigel (2000) in their study of adult revictimization among Black women with histories of sexual abuse in childhood noted that sexually revictimized women were significantly more likely to engage in prostitution and reported higher rates of intimate partner violence.
Trafficking
While acknowledging that participation in sex work poses high risk of exposure to violence, sexual infections, and physical injury, a few scholars have more recently proposed that the health outcomes may be even worse for women who have been trafficked into sex work (coerced or deceived into sex work or entered prior to adulthood) than for women who enter into sex work by other means. Sarkar (2008) has argued that those entering sex work through conditions of coercion or deceit face greater levels of maltreatment and sexual risk. It is posited that due to compromised agency, women trafficked into sex work are less likely to refuse sex or to negotiate for use of condoms; their mobility and access to health care is more restricted; their knowledge of STIs or HIV may be limited due to their isolation and limited access to prevention messages. As sexual violence is often used to initiate women/girls into sex work, the risk of STIs and HIV is also increased (Decker et al., 2011). Furthermore, if trafficked into sex work at a young age, the risks for HIV are increased due to biological factors, such as greater areas of cervical ectopy. In sum, the argument is that even poorer health outcomes are expected, especially more intense and prolonged psychological reactions to abuse, in women who are trafficked into sex work than those not trafficked (Hossain et al., 2010).
However, additional research suggests that STD risk and noncondom use is not exclusively related to whether one is trafficked into prostitution. Vanwesenbeeck, van Zessen, de Graal, and Straver (1994) examined the protective behaviors of prostitutes and clients in the Netherlands, noting that the context and meaning of prostitution influenced such behaviors. Women identified as risk takers (e.g., those who selectively or regularly worked without condoms) compared to other women, were younger, started working at younger age, and had the highest financial need. They worked in streets and in windows, had the most clients, and the fastest work routine. In addition, reinforcing the importance of trauma history, they also had experienced the most severe abuse and violence in childhood and in adult life both on and off the job.
Current Study
While there has been a recent growth in research devoted to the study of human trafficking for the purpose of sexual exploitation (herein sex trafficking), little of it has included systematic primary data collection. Furthermore, minimal attention has been directed at examining the health outcomes of sex trafficking. The current study builds on the preliminary analysis of Raymond and Hughes (2001) to explore more fully the influence of risk factors on health outcomes for women sexually trafficked in the United States. Specifically, we integrate two questions emanating from public health research: (a) if the pathway into sex work (i.e., trafficked or not) produces different health outcomes; and (b) if the nature of sex work (i.e., street prostitution or not) produces different health outcomes. To the best of our knowledge, this is the first study to examine these questions using a sample of women sex trafficked in the United States that includes both domestic and international victims. While Raymond and Hughes (2001) and others have contributed important descriptions of the trauma experienced prior to and during trafficking and the health outcomes of sexually exploited women, this article delves deeper by examining what risk factors influence health outcomes of sexually exploited women, including whether women were trafficked (entered sex work through coercion/deceit or entered before age 18), the nature of the sex work (street prostitution or not), exposure to victimization/trauma before entry into sex work, victimization experiences while in sex work, age at entry into sex work, and length of time in sex work.
Method
The current study relies on data collected by Raymond and Hughes (2002) as part of examination into the international and domestic trafficking of women for the purposes of sexual exploitation in the United States. Semistructured qualitative interviews were centered around the themes of personal information, methods of recruitment, movement, initiation, control, coping, resistance, experience with others involved in the sex industry (e.g., pimps, recruiters, traffickers, buyers, and prostitutes), experiences with outside agencies (e.g., medical, law enforcement, and social services), and future goals and recommendations. The original data set contained 41 interviews that were conducted in 1999-2000 with international (n = 16) and domestic (n = 25) women who had been or were currently in the sex industry in the United States. For details on how respondents were recruited as well as general descriptive information on the total sample, see Raymond and Hughes (2002; 2001). After careful review of the data set, 3 cases were removed because of extensive missing information. As such, 38 cases (n = 16 international and n = 22 domestic women) were retained for the current study. Whereas all women in the original data set were or had been in the sex industry in the United States, for purposes of this study, women were differentiated by whether or not they had been trafficked for sex (i.e., entered sex work through coercion/deceit or entered before age of 18). This group of 30 women who were trafficked for sex were further distinguished by whether or not they were an international trafficking victim (n = 12) or a domestic trafficking victim (n = 18). The remaining 8 domestic and international women were included in a category herein referred to as nontrafficked sex workers.
Variables constructed from the interview narratives collected by Raymond and Hughes (2002) include demographic background (i.e., age, race, nationality, hometown description, educational level, and abuse history) and general experiences in sex work (i.e., age of entry into sex work, length of time in sex work, participation in street prostitution, exposure to violence [physical, sexual, and/or psychological], injuries, and abuse by pimp and/or john). Variables pertaining to health outcomes affiliated with sex work were also examined, including physical health problems (i.e., overall poor health, pneumonia, mononucleosis, hemorrhoids, stomach aches, and/or skin problems), mental health problems (i.e., depression, anger, hopelessness, guilt, difficulty sleeping, lack of energy, startled easily, homicidal, panic disorder, neuroses, disassociation, and/or paranoia), sexually transmitted infections (i.e., HIV, gonorrhea, hepatitis, syphilis, trichomoniasis, pubic lice, pelvic inflammatory disease, and/or herpes), suicidal ideations, and substance abuse (i.e., alcohol and/or drug addiction). Finally, because health problems may be ameliorated or exacerbated by access to health care services, variables pertaining to health care deprivation (i.e., not being allowed to seek medical care when needed) were examined.
Given the small number of cases available, parameter-free methods of statistical analyses were used (One-way ANOVA with Fisher’s Least Significant Difference test). Such tests are appropriate due to our limited knowledge of the parameters of each variable of interest in the population (StatSoft, 2012). In addition, results of statistical analyses will include Bayesian confidence intervals, rather than post hoc power calculations, to estimate the magnitude of the effects and better inform readers about the possibility of an inadequate sample size (Levine & Ensom, 2001). Finally, because it is easier to make Type I errors with a small sample size and the significance level used in this study is set at the conventional .05 level, it should be noted that the findings presented are exploratory. Future research should involve, when possible, larger sample sizes.
Results
This study provides a closer examination of the health outcomes (i.e., physical, sexual, and mental) attributable to sex trafficking in the United States among a sample of sexually exploited women. For a descriptive account of the health outcomes of the women in this sample, see Raymond and Hughes (2001). Utilizing post hoc subgroup tests, comparisons were made between international women trafficked into the United States (n = 12), domestic women trafficked within the United States (n = 18), and nontrafficked women participating in sex work in the United States (n = 8). These findings suggested several differences across the three groups. Results are presented below.
Demographic Profile Differences
Overall, women who were trafficked for sex domestically were significantly different from international women trafficked for sex into the United States and nontrafficked sex workers on almost all demographic variables analyzed. Domestic trafficking victims were significantly older; 39.9 years (SD = 7.4; 95% CI [36.2, 43.6]) compared to international trafficking victims, who were 29.1 years old (SD = 6.1; 95% CI [25.2, 32.9]; p < .001), and nontrafficked sex workers, who were 30.1 years old (SD = 2.7; 95% CI [27.9, 32.4]; p < .001). A higher percentage of domestic trafficking victims were non-White; 66.7% (95% CI [0.4, 0.8]) compared to 25.0% of internationally trafficked victims (95% CI [0.1, 0.5]; p < .01) and 25.0% of nontrafficked sex workers (95% CI [0.1, 0.6]; p < .05). American women trafficked for sex domestically were, on average, better educated (12.7 years; SD = 2.27; 95% CI [11.4, 14.0]) compared to international women trafficked for sex (10.7 years; SD = 2.87; 95% CI [8.8, 12.5]; p < .05) and nontrafficked sex workers (11.9 years; SD = 3.72; 95% CI [8.4, 15.3]; p < .52). Significantly higher percentages of domestic trafficking victims (77.8%; 95% CI [0.5, 0.9]) and nontrafficked sex workers (87.5%; 95% CI [0.5, 1.0]) came from hometowns characterized as being urban compared to international trafficking victims (50.0%; 95% CI [0.3, 0.7]; p < .05). Finally, a greater percentage of domestic trafficking victims reported having experienced physical and/or sexual abuse as a child (87.5%; 95% CI [0.6, 1.0]) compared to international trafficking victims (40.0%; 95% CI [0.2, 0.7]; p < .01). However, no significant difference was found between domestic trafficking victims and nontrafficked sex workers (57.1%; 95% CI [0.2, 0.8]; p < .14).
Differences Regarding Experiences in Sex Work
Significant differences across the three groupings also were evident when experiences in sex work were examined (see Table 1). American women trafficked for sex within the United States entered the sex industry at a significantly younger age (19.3 years of age, SD = 6.1; 95% CI [16.8, 25.3]) than did nontrafficked sex workers (24.7 years of age, SD = 4.9; 95% CI [20.2, 29.3]; p < .05), but no significant difference in age of entry into sex work was found between domestic trafficked women and internationally trafficked women (21.0 years of age, SD = 6.7; 95% CI [16.8, 25.3]; p < .45). Domestic and international trafficking victims also were significantly less likely to report having entered sex work voluntarily (44.4%; 95% CI [0.2, 0.6] and 50.0%; 95% CI [0.3, 0.7] respectively) compared to nontrafficked sex workers (100%; 95% CI [0.7, 1.0]; p < .01). In terms of length in sex work, domestic trafficking victims remained almost 3 times longer (17.9 years, SD = 9.2; 95% CI [13.0, 22.8]) than international trafficking victims, who were, on average, in sex work for 6.3 years (SD = 3.4; 95% CI [4.1, 8.4]; p < .001) and four times longer than nontrafficked sex workers, who were in sex work on average for 4.6 years (SD = 2.4; 95% CI [2.3, 6.8]; p < .001). While in sex work, a greater percentage of domestic trafficking victims reported having been prostituted on the streets; 77.8% (95% CI [0.5, 0.9]) compared to 41.7% of international trafficking victims (95% CI [0.2, 0.7]; p < .05) and 62.5% of nontrafficked sex workers (95% CI [0.2, 0.6]; p < .45); however, international trafficking victims and nontrafficked sex workers did not differ significantly in this regard.
Demographic Profile: Post Hoc Subgroup Comparisons of International Trafficking Victims to Domestic Trafficking Victims and Nontrafficked Sex Workers.
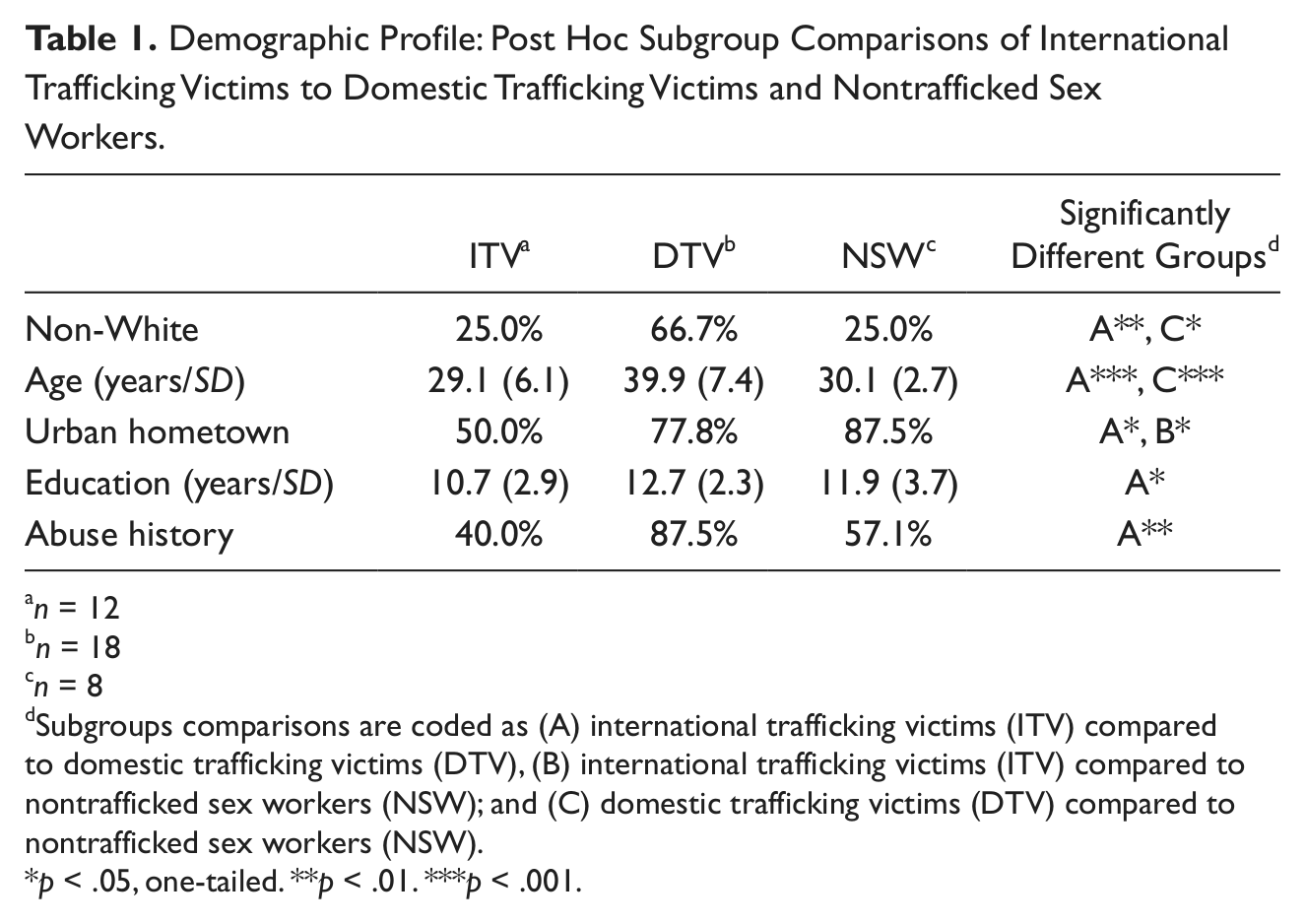
n = 12
n = 18
n = 8
Subgroups comparisons are coded as (A) international trafficking victims (ITV) compared to domestic trafficking victims (DTV), (B) international trafficking victims (ITV) compared to nontrafficked sex workers (NSW); and (C) domestic trafficking victims (DTV) compared to nontrafficked sex workers (NSW).
p < .05, one-tailed. **p < .01. ***p < .001.
Somewhat unexpectedly, comparisons between the three groups of sexually exploited women indicated few significant differences regarding violent victimization. While domestic trafficking victims reported higher percentages of physical and sexual victimization and reported a higher incidence of injuries from such abuse, comparisons failed to produce statistically significant results (see Table 2). Significant differences, however, were found related to psychological victimization, with 100% of domestic trafficking victims (95% CI [0.7, 1.0]); having recounted being psychologically abused while in sex work compared to 81.8% of international trafficking victims (95% CI [0.4, 0.9]; p < .05) and 66.7% of nontrafficked sex workers (95% CI [0.2, 0.8]; p < .05).
Experiences in Sex Industry: Post Hoc Subgroup Comparisons of International Trafficking Victims to Domestic Trafficking Victims and Nontrafficked Sex Workers.
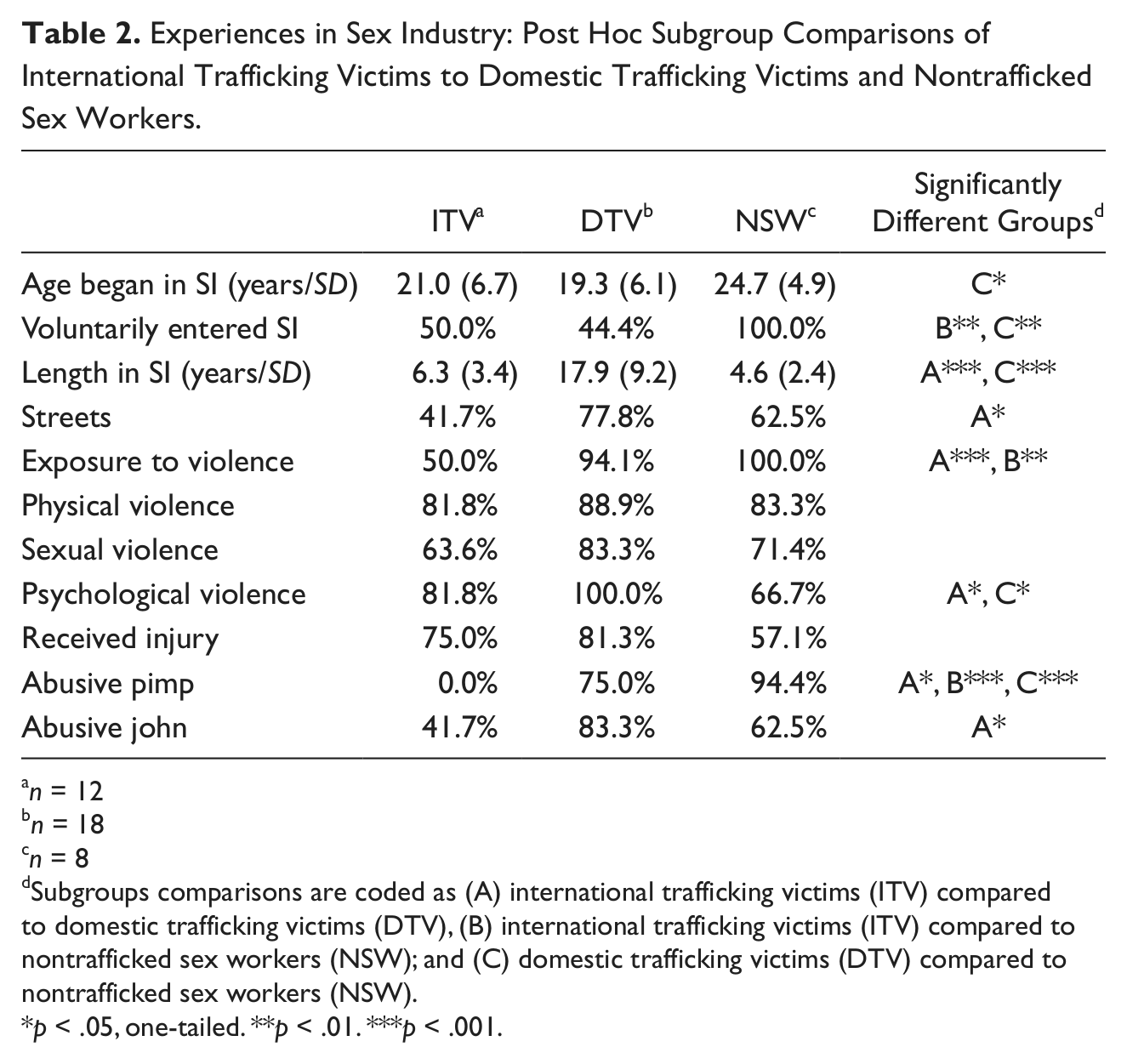
n = 12
n = 18
n = 8
Subgroups comparisons are coded as (A) international trafficking victims (ITV) compared to domestic trafficking victims (DTV), (B) international trafficking victims (ITV) compared to nontrafficked sex workers (NSW); and (C) domestic trafficking victims (DTV) compared to nontrafficked sex workers (NSW).
p < .05, one-tailed. **p < .01. ***p < .001.
A significantly lower percentage of international trafficking victims, on the other hand, reported exposure to violence; 50.0% (95% CI [0.3, 0.7]);compared to 94.1% of domestic trafficking victims (95% CI [0.7, 1.0]; p < .001) and 100.0% of nontrafficked sex workers (95% CI [0.7, 1.0]; p < .01). None of the international trafficking victims described being abused by a pimp; 0.0% (95% CI [0.0, 0.3]) compared to 75.0% of domestic trafficking victims (95% CI [0.4, 0.9]; p < .05) and 94.4% of nontrafficked sex workers (95% CI [0.7, 1.0]; p < .001) who described such abuse. A smaller percentage of international trafficking victims also reported having been abused by a john; 41.7% (95% CI [0.2, 0.7]) compared to 83.3% of domestic trafficking victims (95% CI [0.6, 0.9]; p < .05), but did not differ significantly in this regard compared to nontrafficked sex workers (62.5% (95% CI [0.3, 0.9]; p < .29).
Differences in Health Outcomes
As a whole, American women trafficked for sex within the United States exhibited the poorest health outcomes among the three groups (see Table 3). For instance, domestic trafficking victims reported significantly higher percentages of physical health problems; 64.7% (95% CI [0.4, 0.8]) compared to 25.0% of international trafficking victims (95% CI [0.1, 0.5]; p < .05) and 25.0% of nontrafficked sex workers (95% CI [0.1, 0.6]; p < .05). Most, if not all, of the women who had been trafficked for sex in the sample (100% of domestic trafficking victims; 95% CI [0.8, 1.0] and 91.7% of international trafficking victims; 95% CI [0.6, 1.0]) reported having at least one mental health problem compared to three quarters (75.0%) of nontrafficked sex workers (95% CI [0.4, 0.9]; p < .05). While relatively similar percentages of domestic trafficking victims 58.8%; 95% CI [0.4, 0.8]) and nontrafficked sex workers (57.1%; 95% CI [0.2, 0.8]; p < .94) indicated having at least one sexually transmitted infection while in sex work, a significantly smaller percentage of international trafficking victims (50.5%; 95% CI [0.3, 0.8]; p < .05) indicated an STI compared to domestic trafficking victims.
Health Outcomes: Post Hoc Subgroup Comparisons of International Trafficking Victims to Domestic Trafficking Victims and Nontrafficked Sex Workers.
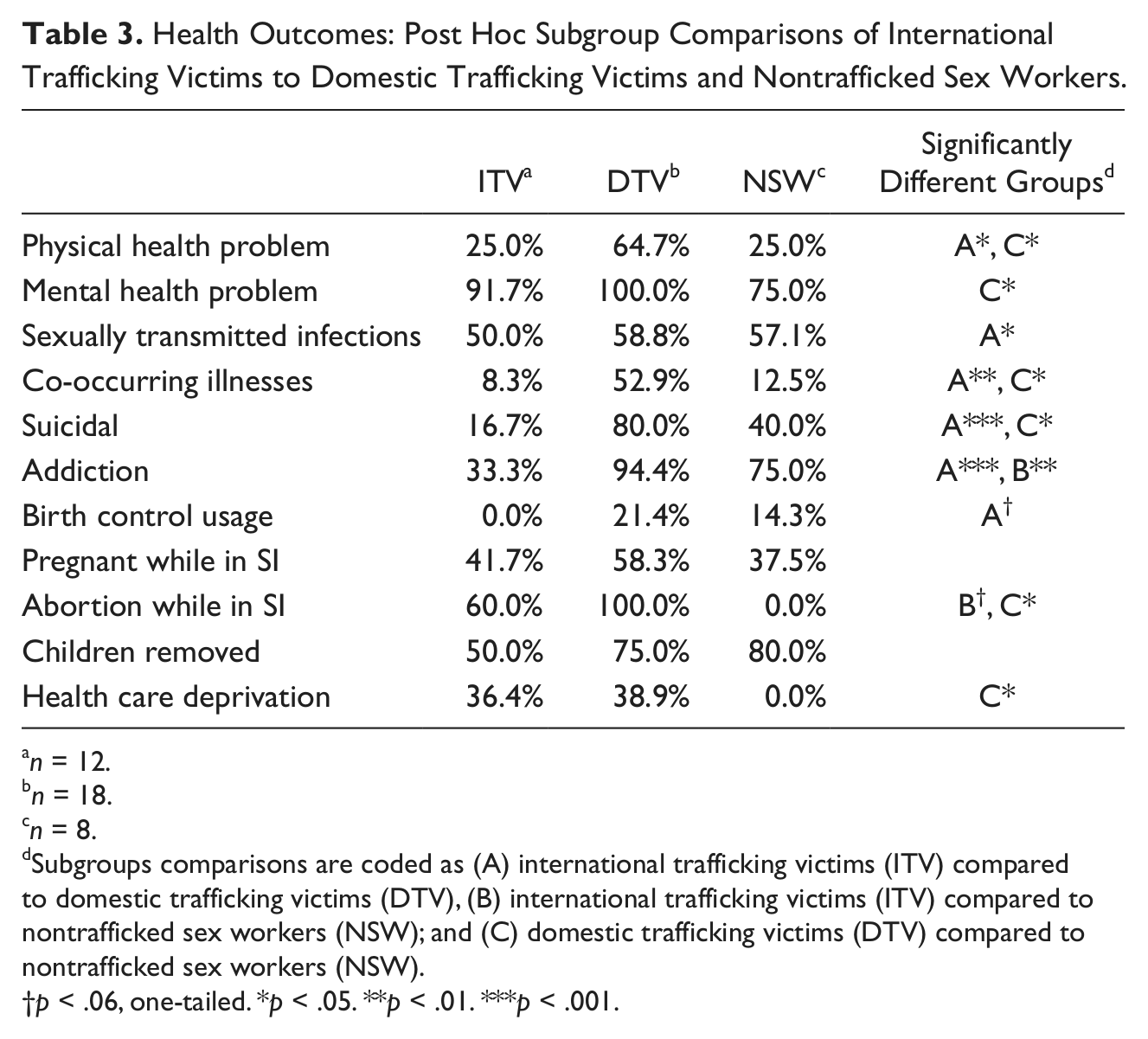
n = 12.
n = 18.
n = 8.
Subgroups comparisons are coded as (A) international trafficking victims (ITV) compared to domestic trafficking victims (DTV), (B) international trafficking victims (ITV) compared to nontrafficked sex workers (NSW); and (C) domestic trafficking victims (DTV) compared to nontrafficked sex workers (NSW).
p < .06, one-tailed. *p < .05. **p < .01. ***p < .001.
Several significant differences were apparent across the three groups in presence of suicidal ideation and addiction to drugs and/or alcohol. A significantly greater proportion of domestic trafficking victims (80.0%; 95% CI [0.5, 0.9]) stated they contemplated suicide while in sex work compared to 16.7% of international trafficking victims (95% CI [0.1, 0.5]; p < .001) and 40.0% of nontrafficked sex workers (95% CI [0.1, 0.8]; p < .05). There were significantly fewer international trafficking victims who were addicted to drugs and/or alcohol; 33.3% (95% CI [0.1, 0.6]) compared to 94.4% of domestic trafficking victims (95% CI [0.7, 1.0]; p < .001) and 75.0% of nontrafficked sex workers (95% CI [0.4, 0.9]; p < .01).
Women differed little in terms of experiences with family planning, pregnancy, and children. Very few women, regardless of grouping, reported using birth control (beyond sporadic condom use). Relatively large percentages of women reported becoming pregnant; 58.3% of domestic trafficking victims (95% CI [0.3, 0.8]), 41.7% of international trafficking victims (95% CI [0.2, 0.7]), and 37.5% of nontrafficked sex workers (95% CI [0.0, 0.7]). These differences, however, were not statistically significant (p < .86, p < .44, p < .38). Among the women who reported becoming pregnant, nontrafficked sex workers were significantly less likely to have had an abortion (0.0%; 95% CI [0.0, 0.7]) compared international trafficking victims (60.0%; 95% CI [0.2, 0.9]; p < .05). While not a statistically significant difference, nontrafficked sex workers were also less likely to have had an abortion compared to domestic trafficking victims (100%; 95% CI [0.4, 1.0]; p < .06), perhaps indicating the possibility of a trend. Among the mothers in the sample, 80% of nontrafficked sex workers (95% CI [0.2, 0.7]), 75% of domestic trafficking victims (95% CI [0.5, 0.9]), and 50% of international trafficked women (95% CI [0.2, 0.8]) reported that their children were no longer in their custody, having been removed by social services and/or adopted by a family member. These differences were not statistically significant across the three groups (p < .31, p < .31, p < .85).
Finally, women were asked about whether they had ever been prevented from obtaining health or medical treatment when they needed it while in sex work. Domestic trafficking victims (38.9%; 95% CI [0.2, 0.6]) were significantly more likely to report health care deprivation than nontrafficked sex workers (0.0%; 95% CI [0.0, 0.5]; p < .05), but not more likely than international trafficking victims (36.4%; 95% CI [0.2, 0.7]; p < .16) to report such an experience.
Risk Factors for Adverse Health Outcomes Among Sexually Exploited Women
A series of bivariate statistical analyses revealed several variables that were significantly related to adverse health outcomes among sexually exploited women (see Table 4). It worthwhile to mention the possibility that there may be overlap between the different factors examined (i.e., that they co-occur), making it difficult to disentangle which factor is the most relevant in terms of adverse health outcomes. The results from these analyses are presented below. Due to the number of chi-square and t tests conducted, the authors chose to interpret findings as significant using a lower probability value of .01.
Risk Factors for Adverse Health Outcomes Among Sexually Exploited Women.
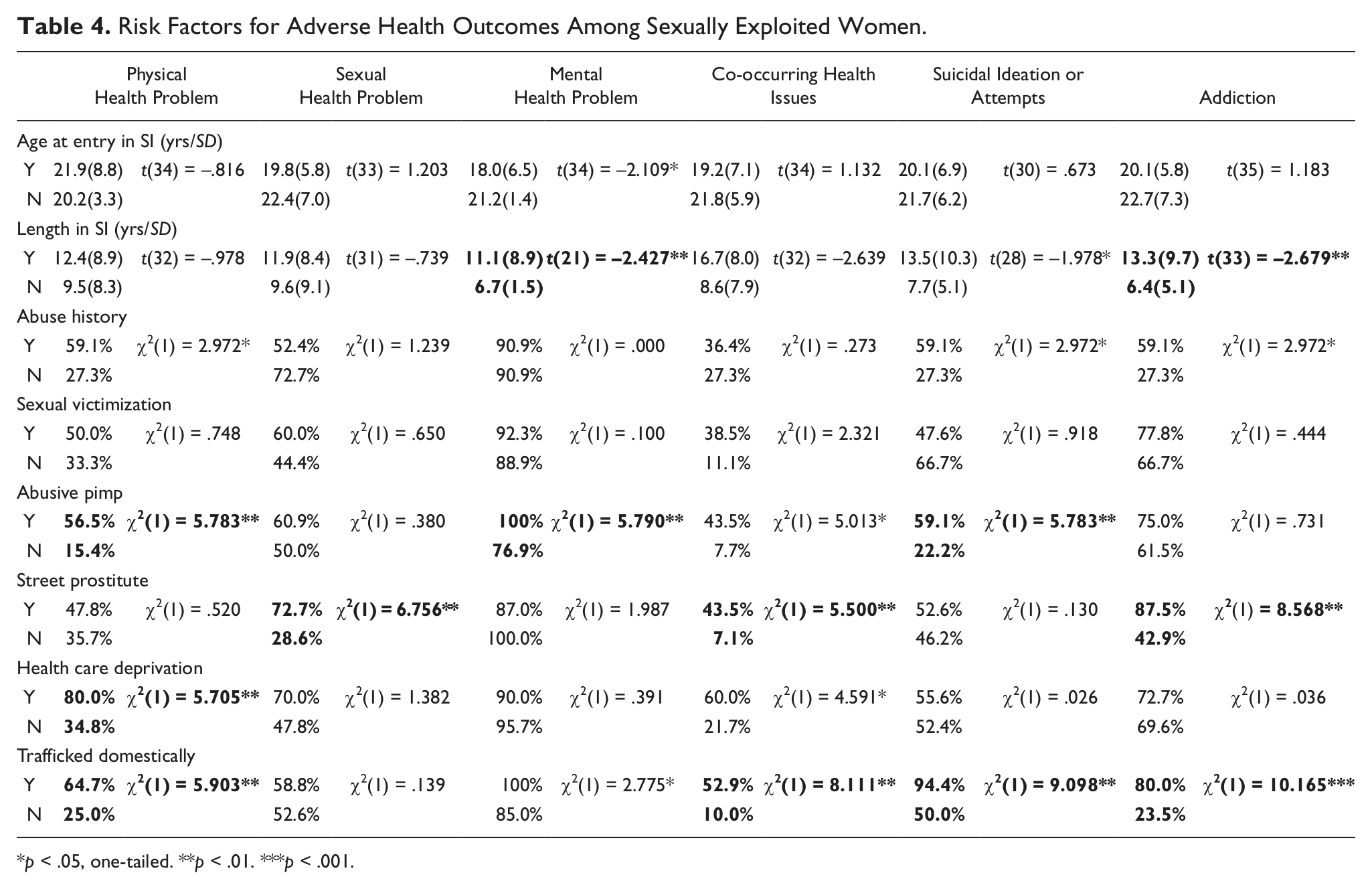
p < .05, one-tailed. **p < .01. ***p < .001.
In terms of physical health, half (50.0%, n = 19) of the women reported at least one physical ailment. A number of variables were found to be significantly associated with poor physical health, including having an abusive pimp, χ2(1) = 5.783, p < .01, health care deprivation, χ2(1) = 5.705, p < .01, and domestic sex trafficking, χ2(1) = 5.903, p < .01. Overall, women who had an abusive pimp were not allowed to seek necessary medical attention when needed, or were trafficked for sex domestically, and had poorer physical health than their counterparts who did not experience such phenomenon.
A nearly equal number of women (52.6%, n = 20) stated they had contracted at least one STI. Having participated in street prostitution was the only variable related to poor sexual health, χ2(1) = 6.756, p < .01. Women who engaged in prostitution on the streets reported a higher incidence of sexually transmitted infections than women who engaged in prostitution elsewhere (e.g., clubs, escort agencies, massage parlors).
The vast majority of the women interviewed (89.5%, n = 34) reported experiencing at least one mental health problem. Variables associated with poor mental health included length of time in sex work, t(21) = −2.427, p < .01, and having an abusive pimp, χ2(1) = 5.790, p < .016. In general, women who stayed longer in sex work and were sexually exploited by an abusive pimp had poorer mental health than their counterparts who did not experience such phenomena.
Slightly more than one quarter (28.9%, n = 11) of the women had co-occurring illnesses (having reported complaints in all three areas: physical, mental, and sexual). Variables associated with co-occurrence include involvement in street prostitution, χ2(1) = 5.500, p < .01, and domestic sex trafficking, χ2(1) = 8.111, p < .01. Overall, women who had been sexually exploited by an abusive pimp or were trafficked for sex domestically were more likely to have reported having co-occurring illnesses than other women.
Many of the women who had been sexually exploited (42.1%, n = 16) indicated they had contemplated suicide. Variables associated with suicidal ideation included having had an abusive pimp, χ2(1) = 3.476, p < .01, and having been trafficked domestically for sex, χ2(1) = 10.165, p < .001. In other words, suicidal ideation is greatest among women who were sexually exploited by an abusive pimp or trafficked for sex domestically.
Finally, a large percentage (71.1%, n=27) of women also reported being addicted to alcohol and/or drugs. Variables associated with addiction included length of time in sex work, t(33) = −2.679, p < .01, involvement in street prostitution, χ2(1) = 8.565, p < .01, and having been trafficked domestically for sex, χ2(1) = 9.098, p < .001. Overall, women who had been in the sex industry longer, prostituted on the street, or trafficked for sex domestically had higher rates of addiction than did their counterparts who did not experience such phenomenon.
Discussion
To date, little research has examined the health outcomes of victims trafficked into or within the United States for sex work. No research has examined the influence of risk factors on the health outcomes of women trafficked for sex in the United States and no single study has compared the health outcomes of both domestic and internationally trafficked women. Relying on Hughes and Raymond’s (2002) original sample, women were categorized into three distinct subgroups (i.e., international women trafficked into the United States, domestic women trafficked in the United States, and nontrafficked women engaged in sex work in the United States) to examine the unique influences that type of entry into sex work (trafficked vs. nontrafficked) and the nature of sex work (street prostitute vs. other) had on their experiences and health outcomes. Prior research has predicted that the nature of street work (i.e., being exposed to street-level prostitution) increases women’s risks of exposure to victimization and such work will produce reduced health outcomes (Cohan et al., 2005; Church et al., 2001). In a closely related line of research, some scholars have examined stage of exposure to trauma/victimization (prior to entry into sex work or during sex work) to determine whether early or later exposure is more influential in shaping health outcomes (Chudakov et al., 2002; Cwikel et al., 2004; Hossain et al., 2010). Most recently, Decker and colleagues (2011) suggest that rather than the nature of the sex work engaged in or stage of exposure to trauma, it is the manner in which one enters sex work (i.e., trafficked or not) that has a more significant influence on health outcomes. Our research examined each of these three plausible explanations for how such risks affect health outcomes.
Overall, our findings suggest that the experiences in sex work of domestic trafficking victims and international trafficking victims were more dissimilar than they were similar. Domestic trafficking victims reported being in sex work for longer periods of time than the nontrafficked sex workers and the international trafficking victims, undoubtedly reflecting the combined effect of their earlier age of entry into sex work and their being older at the time of data collection. Compared to international trafficking victims, a larger proportion of domestic trafficking victims were involved in street prostitution, exposed to psychological violence, and experienced abuse at the hands of pimps and/or johns. However, despite the differences in the nature of sex work engaged in by the two groups, no differences in reports of sexual violence, physical violence, or injury were found. This is unexpected given that fewer international victims were involved in street prostitution, and hence their rates of such violence were expected to be lower than those of domestic trafficking victims or nontrafficked sex workers.
A larger proportion of domestic trafficking victims displayed poor health outcomes in areas of physical health, sexually transmitted infections, co-occurring illnesses, suicidal ideation, and addiction, compared to international trafficking victims. Furthermore, when compared to nontrafficked sex workers, a larger proportion of domestic trafficking victims reported problems with physical health, mental health, co-occurring illnesses, suicidal ideation, and having had an abortion. For only two health outcomes (i.e., experiences of pregnancy and removal of children from mother’s care) were similar portions of domestic trafficked victims, international trafficked victims, and nontrafficked sex workers affected. The higher proportion of domestic trafficked victims reporting health problems cannot be explained by their differential access to health care as high proportions of both domestic trafficking victims and international trafficking victims reported having been prevented from obtaining medical treatment when it was needed. It may be that length of time in prostitution is thus more predictive of adverse health outcomes than access to health care is among this population.
Finally, we examined the relationship of various risk factors identified in prior research to adverse health outcomes among the sample of sexually exploited women overall. Based on the work of Church et al. (2001), Du Mont and McGregor (2004), and Cohan et al. (2005) it was expected that the health outcomes of women involved in street prostitution would be poorer than those involved in other types of sex work. Overall, our findings support this conclusion as a higher percentage of those involved in street prostitution reported sexual health problems, co-occurring health issues, and addiction. Interestingly, being involved in street prostitution is the only risk factor associated with sexual health problems.
Furthermore, involvement of a pimp is common in street prostitution, and poses a potential risk to health and safety for women. Our findings suggest that a larger portion of women who reported having an abusive pimp reported physical health problems, mental health problems, co-occurring health issues, and suicidal ideations. Such findings bolster evidence that abusive behavior patterns displayed by pimps that includes psychological and verbal abuse, independent of physical or sexual violence, has an important and detrimental influence on health outcomes.
Our research also examined the influence of exposure to trauma/ violence before adulthood on health outcomes. While the work of Cwikel and colleagues (2004) found that such exposure was related to depression and PTSD, our findings suggest that women who reported physical and/or sexual abuse as a child were more likely to report physical health problems, suicidal ideations, and addiction, but not adverse mental health outcomes. However, our findings do suggest that the younger one experienced sexual exploitation (or entered into sex work), the poorer the mental health outcomes.
Last, how a person enters into sex work is posited to influence health outcomes. Hossain et al. (2010) and Decker et al. (2011) argue that persons who are forced or deceived into sex work or enter into sex work prior to maturity will evidence poorer health outcomes than those who enter at an older age or for whom coercion or deceit was not used initially. Entry via trafficking purportedly results in more negative health consequences because the person’s agency is compromised, access to health care and/or knowledge is more restricted, the risks of sexual violence are higher, and vulnerability to infection is greater. Our findings strongly suggest that this is indeed the case for domestic trafficked women. Being trafficked domestically was significantly related to five of the six adverse health outcomes examined, including physical health, mental health, co-occurring health issues, suicidal ideation, and addiction. However, international trafficked women did not report such negative health outcomes. It is plausible that differences in the domestic and international trafficking victims partially explain this effect. Recall that demographically the two subgroups differed on several attributes; the domestic trafficking group was predominately older (on average 10 years older), non-White, and had experienced physical or sexual abuse as a child, had been in sex work longer (nearly 3 times longer on average), and had been involved in street prostitution. Thus the combination of risk factors present in the lives of the domestic trafficked victims that are not evidenced in the lives of international trafficking victims may partially explain the differential effects that entry into sex work via trafficking has on health outcomes. For instance, it may be that factors associated with being a racial/ethnic minority in the United States contribute to poorer health outcomes experienced by domestic trafficking victims. The Centers for Disease Control and Prevention (2011) recently identified the extent of health disparities and inequalities experienced by racial/ethnic minorities in the United States noting that the overrepresentation of the poor, the uninsured, and the less educated among minority populations contributes to their living shorter and sicker lives.
Future research would benefit from examining the differential impact cumulative risk factors have on health outcomes among individuals involved in the sex trade. Particular attention should be directed toward the influence of time in prostitution. For instance, research by Vanwesenbeeck (1994) suggests that length of time in prostitution is strongly predictive of a range of harmful effects above and beyond whether or not the individual has been trafficked into the sex trade. The small number of cases available for analysis limits our ability to employ more sophisticated analysis of these interrelationships. However, future research with larger and more representative samples can use more advanced statistical analysis to explore this further.
This study has several limitations that must be identified to assure appropriate interpretation of its findings. First, while the study contributes to the existing literature in an important way by building on the original analysis of Raymond and Hughes (2001) to include examination of the relationship of identified risk factors to health outcomes, the analyses are based on a small number of nonrepresentative cases obtained using convenience sampling. Second, due to the manner in which the information on health outcomes was collected originally, their measurement is limited to determining whether or not an exploited woman experienced a particular health outcome of interest (its prevalence), rather than the number of times an exploited woman experienced a particular health outcome (its incidence) in the study period . Future research should attempt to avoid these weaknesses.
In conclusion, identification of risk factors is a common aim of both public health and criminological research. Information provided here, while preliminary, may help inform policy makers concerned with primary prevention strategies in the public health arena, and/or policies directed at addressing the complicated needs of trafficked victims assisting prosecution of their traffickers in the criminal justice process. The importance of engaging in research that better identifies the health outcomes of trafficking victims cannot be understated. Indeed, doing so may be central to the success of efforts to prevent harm when possible and to redress harm once it has occurred.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.